
Identification of Prescribing Patterns in Hemodialysis Outpatients Taking Multiple Medications
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Objectives
2.2. Patient Population and Setting
2.3. Data Collection, Definitions and Outcomes
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
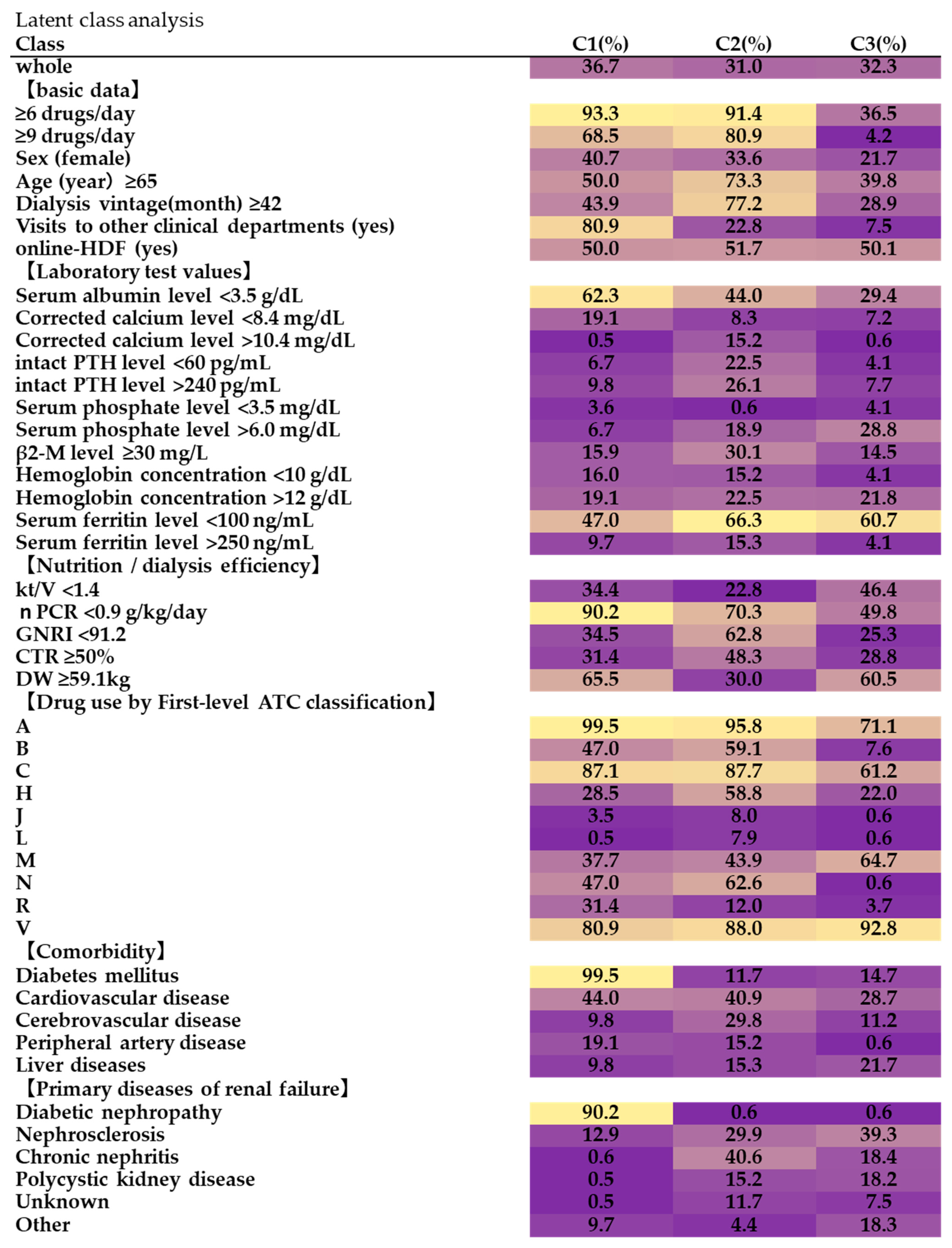
3.2. The LCA
3.3. Results of a Bivariate Analysis (Fisher’s Exact Test)
3.4. A Logistic Regression Analysis Using Stepwise Variable Selection
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fulton, M.M.; Allen, E.R. Polypharmacy in the elderly: A literature review. J. Am. Acad. Nurse Pract. 2005, 17, 123–132. [Google Scholar] [CrossRef]
- Gnjidic, D.; Hilmer, S.N.; Blyth, F.M.; Naganathan, V.; Cumming, R.G.; Handelsman, D.J.; McLachlan, A.J.; Abernethy, D.R.; Banks, E.; Le Couteur, D.G. High-risk prescribing and incidence of Frailty among older community-dwelling men. Clin. Pharmacol. Ther. 2012, 91, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Kojima, T.; Akishita, M.; Nakamura, T.; Nomura, K.; Ogawa, S.; Iijima, K.; Eto, M.; Ouchi, Y. Polypharmacy as a risk for fall occurrence in geriatric outpatients. Geriatr. Gerontol. Int. 2011, 12, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Kojima, T.; Akishita, M.; Kameyama, Y.; Yamaguchi, K.; Yamamoto, H.; Eto, M.; Ouchi, Y. High risk of adverse drug reactions in elderly patients taking six or more drugs: Analysis of inpatient database. Geriatr. Gerontol. Int. 2012, 12, 761–762. [Google Scholar] [CrossRef] [PubMed]
- Guidelines for Medical Treatment and Its Safety in the Elderly. The Japan Geriatrics Society. 2015. Available online: https://www.jpn-geriat-soc.or.jp/info/topics/pdf/20170808_01.pdf (accessed on 10 September 2021).
- Schmidt, I.M.; Hübner, S.; Nadal, J.; Titze, S.; Schmid, M.; Bärthlein, B.; Schlieper, G.; Dienemann, T.; Schultheiss, U.T.; Meiselbach, H.; et al. Patterns of medication use and the burden of polypharmacy in patients with chronic kidney disease: The German Chronic Kidney Disease study. Clin. Kidney J. 2019, 12, 663–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos-Díaz, G.; Pérez-Pico, A.; Suárez-Santisteban, M.; García-Bernalt, V.; Mayordomo, R.; Dorado, P. Prevalence of Potential Drug–Drug Interaction Risk among Chronic Kidney Disease Patients in a Spanish Hospital. Pharmaceutics 2020, 12, 713. [Google Scholar] [CrossRef] [PubMed]
- JSDT Renal Data Registry 2019. Japanese: The Japanese Society for Dialysis Therapy. Available online: https://docs.jsdt.or.jp/overview/index.html (accessed on 6 October 2020).
- Chapter 11: International Comparison, the 2018 USRDS Annual Data Report. Washington: United States Renal Data System. 2018. Available online: https://www.usrds.org/2018/view/v2_11.aspx (accessed on 10 September 2019).
- Imai, E.; Horio, M.; Iseki, K.; Yamagata, K.; Watanabe, T.; Hara, S.; Ura, N.; Kiyohara, Y.; Hirakata, H.; Moriyama, T.; et al. Prevalence of chronic kidney disease (CKD) in the Japanese general population predicted by the MDRD equation modified by a Japanese coefficient. Clin. Exp. Nephrol. 2007, 11, 156–163. [Google Scholar] [CrossRef]
- Chiu, Y.-W.; Teitelbaum, I.; Misra, M.; de Leon, E.M.; Adzize, T.; Mehrotra, R. Pill Burden, Adherence, Hyperphosphatemia, and Quality of Life in Maintenance Dialysis Patients. Clin. J. Am. Soc. Nephrol. 2009, 4, 1089–1096. [Google Scholar] [CrossRef] [Green Version]
- Nagano, N.; Ito, K.; Honda, M.; Sunaga, S.; Tagahara, A.; Nohara, T.; Nohara, A.; Hoshi, A.; Tamei, N.; Ando, T.; et al. The magnesium included as a pharmaceutical excipient in phosphate binders might affect the serum magnesium levels of dialysis patients. Nihon Toseki Igakkai Zasshi 2016, 49, 571–580. [Google Scholar] [CrossRef] [Green Version]
- Juul-Larsen, H.G.; Christensen, L.D.; Bandholm, T.; Andersen, O.; Kallemose, T.; Jørgensen, L.M.; Petersen, J. Patterns of Multimorbidity and Differences in Healthcare Utilization and Complexity among Acutely Hospitalized Medical Patients (≥65 Years)—A Latent Class Approach. Clin. Epidemiol. 2020, 12, 245–259. [Google Scholar] [CrossRef] [Green Version]
- Lanza, S.T.; Collins, L.M.; Lemmon, D.R.; Schafer, J.L. PROC LCA: A SAS Procedure for Latent Class Analysis. Struct. Equ. Model. Multidiscip. J. 2007, 14, 671–694. [Google Scholar] [CrossRef]
- Herr, M.; Robine, J.-M.; Pinot, J.; Arvieu, J.-J.; Ankri, J. Polypharmacy and frailty: Prevalence, relationship, and impact on mortality in a French sample of 2350 old people. Pharmacoepidemiol. Drug Saf. 2015, 24, 637–646. [Google Scholar] [CrossRef]
- Dosage Recommendations for Drugs That Require the Most Attention in Renal Impairment. The Japanese Society of Nephrology and Pharmacotherapy. Available online: https://www.jsnp.org/docs/%E8%85%8E%E6%A9%9F%E8%83%BD%E4%BD%8E%E4%B8%8B%E6%99%82%E3%81%AB%E6%9C%80%E3%82%82%E6%B3%A8%E6%84%8F%E3%81%AE%E5%BF%85%E8%A6%81%E3%81%AA%E8%96%AC%E5%89%A4%E6%8A%95%E4%B8%8E%E9%87%8F%E4%B8%80%E8%A6%A7_34.1%E7%89%88.pdf (accessed on 2 October 2021).
- Wasse, H.; Gillen, D.L.; Ball, A.M.; Kestenbaum, B.R.; Seliger, S.L.; Sherrard, D.; Stehman-Breen, C.O. Risk factors for upper gastrointes-tinal bleeding among end-stage renal disease patients. Kidney Int. 2003, 64, 1455–1461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, X.-H.; Lin, C.-C.; Wang, Y.-J.; Luo, J.-C.; Young, S.-H.; Chen, P.-H.; Hou, M.-C.; Lee, F.-Y. Risk factors of the peptic ulcer bleeding in aging uremia patients under regular hemodialysis. J. Chin. Med. Assoc. 2018, 81, 1027–1032. [Google Scholar] [CrossRef] [PubMed]
- Hosseininasab Nodoushan, S.A.; Nabavi, A. The Interaction of Helicobacter pylori Infection and Type 2 Diabetes Mellitus. Adv. Biomed. Res. 2019, 8, 15. [Google Scholar] [CrossRef] [PubMed]
- Nishihara, M.; Hirata, S.; Izumi, S.; Furukubo, T.; Ota, M.; Fujita, M.; Yamakawa, T.; Tanaka, K. A survey of constipation in dialysis patients. Nihon Toseki Igakkai Zasshi 2004, 37, 1887–1892. [Google Scholar] [CrossRef]
- Jong, I.-C.; Tsai, H.-B.; Lin, C.-H.; Ma, T.-L.; Guo, H.-R.; Hung, P.-H.; Hung, K.-Y. Close correlation between the ankle-brachial index and symptoms of depression in hemodialysis patients. Int. Urol. Nephrol. 2017, 49, 1463–1470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohtake, T.; Kobayashi, S.; Moriya, H.; Negishi, K.; Okamoto, K.; Maesato, K.; Saito, S. High Prevalence of Occult Coronary Artery Stenosis in Patients with Chronic Kidney Disease at the Initiation of Renal Replacement Therapy: An Angiographic Examination. J. Am. Soc. Nephrol. 2005, 16, 1141–1148. [Google Scholar] [CrossRef]
- Leskinen, Y.; Salenius, J.P.; Lehtimäki, T.; Huhtala, H.; Saha, H. The prevalence of peripheral arterial disease and medial arterial calcification in patients with chronic renal failure: Requirements for diagnostics. Am. J. Kidney Dis. 2002, 40, 472–479. [Google Scholar] [CrossRef]
- Takeuchi, H.; Uchida, H.A.; Kakio, Y.; Okuyama, Y.; Okuyama, M.; Umebayashi, R.; Wada, K.; Sugiyama, H.; Sugimoto, K.; Rakugi, H.; et al. The Prevalence of Frailty and its Associated Factors in Japanese Hemodialysis Patients. Aging Dis. 2018, 9, 192–207. [Google Scholar] [CrossRef] [Green Version]
- Ballew, S.H.; Chen, Y.; Daya, N.R.; Godino, J.G.; Windham, B.G.; McAdams-DeMarco, M.; Coresh, J.; Selvin, E.; Grams, M.E. Frailty, Kidney Function, and Polypharmacy: The Atherosclerosis Risk in Communities (ARIC) Study. Am. J. Kidney Dis. 2017, 69, 228–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, H.W.; Yoo, H.J.; Park, S.Y.; Kim, S.W.; Choi, J.Y.; Yoon, S.J.; Kim, C.H.; Kim, K.I. The Korean version of the FRAIL scale: Clinical fea-sibility and validity of assessing the frailty status of Korean elderly. Korean J. Intern. Med. 2016, 31, 594–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woo, J.; Leung, J. Multi-morbidity, dependency, and frailty singly or in combination have different impact on health outcomes. Age 2013, 36, 923–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamsen, K.M.; Bell, J.S.; Hilmer, S.N.; Kirkpatrick, C.M.J.; Ilomäki, J.; Le Couteur, D.; Blyth, F.M.; Handelsman, D.J.; Waite, L.; Naganathan, V.; et al. Effects of Changes in Number of Medications and Drug Burden Index Exposure on Transitions Between Frailty States and Death: The Concord Health and Ageing in Men Project Cohort Study. J. Am. Geriatr. Soc. 2016, 64, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Saum, K.-U.; Schöttker, B.; Meid, A.D.; Holleczek, B.; Haefeli, W.E.; Hauer, K.; Brenner, H. Is Polypharmacy Associated with Frailty in Older People? Results From the ESTHER Cohort Study. J. Am. Geriatr. Soc. 2016, 65, e27–e32. [Google Scholar] [CrossRef]


{kind=link}
| Number of Patients Analyzed | 98 |
|---|---|
| Number of drugs per day (median [IQR]) | 9 (5.8–11.0) |
| Number of patients receiving polypharmacy (≥6 drugs/day) (n [%]) | 74 (75.5) |
| Number of patients receiving polypharmacy (≥9 drugs/day) (n [%]) | 52 (53.1) |
| Age (years) (median [IQR]) | 65 (56.8–73.0) |
| ≥65 (n [%]) | 52 (53.1) |
| Dialysis vintage (month) (median [IQR]) | 42 (21.8–113.5) |
| ≥42 (n [%]) | 49 (50.0) |
| Sex (female) (n [%]) | 32 (32.7) |
| online-HDF (yes) (n [%]) | 46 (46.9) |
| Visits to other clinical departments (yes) (n [%]) | 41 (41.8) |
| Comorbidity | |
| Diabetes mellitus (n [%]) | 45 (45.9) |
| Cardiovascular disease (n [%]) | 36 (36.7) |
| Cerebrovascular disease (n [%]) | 15 (15.3) |
| Peripheral artery disease (n [%]) | 11 (11.2) |
| Liver diseases (n [%]) | 14 (14.3) |
| Primary diseases of renal failure | |
| Diabetic nephropathy (n [%]) | 34 (34.7) |
| Nephrosclerosis (n [%]) | 26 (26.5) |
| Chronic nephritis (n [%]) | 17 (17.3) |
| Polycystic kidney disease (n [%]) | 9 (9.2) |
| unknown (n [%]) | 6 (6.1) |
| Other (n [%]) | 10 (10.2) |
| Blood test values | |
| Serum albumin level, (g/dL) (median [IQR]) | 3.5 (3.2–3.7) |
| <3.5 g/dL (n [%]) | 48 (49.0) |
| Corrected calcium level (mg/dL) (median [IQR]) | 9 (8.7–9.4) |
| <8.4, >10.4 mg/dL (n [%]) | 15 (15.3) |
| <8.4 mg/dL (n [%]) | 11 (11.2) |
| >10.4 mg/dL (n [%]) | 4 (4.1) |
| Serum phosphate level (mg/dL) (median [IQR]) | 5.1 (4.5–5.8) |
| <3.5, >6.0 mg/dL (n [%]) | 20 (20.4) |
| <3.5 mg/dL (n [%]) | 2 (2.0) |
| >6.0 mg/dL (n [%]) | 18 (18.4) |
| intact PTH level (pg/mL) (median [IQR]) | 153.4 (102.2–212.6) |
| <60, >240 pg/mL (n [%]) | 24 (24.5) |
| <60 pg/mL (n [%]) | 10 (10.2) |
| >240 pg/mL (n [%]) | 14 (14.3) |
| β2-M level (mg/L) (median [IQR]) (n = 96) | 24.1 (20.0–29.0) |
| ≥30 mg/L (n [%]) | 21 (21.9) |
| Hemoglobin concentration (g/dL) (median [IQR]) (n = 97) | 11.3 (10.8–11.9) |
| <10, >12 g/dL (n [%]) | 30 (30.9) |
| <10 g/dL (n [%]) | 11 (11.3) |
| >12 g/dL (n [%]) | 19 (19.6) |
| Serum ferritin level (ng/mL) (median [IQR]) (n = 96) | 87.0 (53.3–150.5) |
| <100, >250 ng/mL (n [%]) | 64 (66.7) |
| <100 ng/mL (n [%]) | 54 (56.3) |
| >250 ng/mL (n [%]) | 10 (10.4) |
| Dialysis efficiency and nutritional effect | |
| kt/V (median [IQR]) (n = 97) | 1.52 (1.3–1.7) |
| <1.4 (n [%]) | 34 (35.1) |
| nPCR (g/kg/day) (median [IQR]) (n = 97) | 0.82 (0.7–0.9) |
| <0.9 g/kg/day (n [%]) | 67 (69.1) |
| GNRI (median [IQR]) (n = 93) | 92.33 (88.1–98.0) |
| <91.2 (n [%]) | 38 (40.9) |
| CTR (%) (median [IQR]) (n = 96) | 47 (44.3–52.0) |
| ≥50% (n [%]) | 35 (36.5) |
| Dry weight (kg) (median [IQR]) | 59.1 (49.5–70.0) |
| ≥59.1 kg (n [%]) | 48 (50.0) |
| First-level ATC classification (anatomical group) (n [%]) | |
| A-Alimentary Tract and Metabolism | 88 (89.8) |
| B-Blood and Blood Forming Organs | 35 (35.7) |
| C-Cardiovascular System | 79 (80.6) |
| H-Systemic Hormonal Preparations, Excl. Sex Hormones and Insulins | 33 (33.7) |
| J-Anti-infectives for Systemic Use | 4 (4.1) |
| L-Antineoplastic and Immunomodulating Agents | 2 (2.0) |
| M-Musculo-Skeletal System | 46 (46.9) |
| N-Nervous System | 38 (38.8) |
| R-Respiratory System | 17 (17.3) |
| V-Various | 86 (87.8) |
| Variable | <9 | ≥9 | Ratio (%) | p Value | ||
|---|---|---|---|---|---|---|
| A | Alimentary Tract and Metabolism | (−) | 10 | 0 | 0.0 | <0.001 |
| (+) | 36 | 52 | 59.1 | |||
| B | Blood and Blood-forming Organs | (−) | 38 | 25 | 39.7 | <0.001 |
| (+) | 8 | 27 | 77.1 | |||
| C | Cardiovascular System | (−) | 15 | 4 | 21.1 | <0.001 |
| (+) | 31 | 48 | 60.8 | |||
| H | Systemic Hormonal Preparations, excl. Sex Hormones and Insulins | (−) | 35 | 30 | 46.2 | 0.085 |
| (+) | 11 | 22 | 66.7 | |||
| J | Anti-infectives for Systemic Use | (−) | 46 | 48 | 51.1 | 0.120 |
| (+) | 0 | 4 | 100.0 | |||
| L | Antineoplastic and Immunomodulating Agents | (−) | 46 | 50 | 52.1 | 0.500 |
| (+) | 0 | 2 | 100.0 | |||
| M | Musculo-Skeletal System | (−) | 25 | 27 | 51.9 | 0.842 |
| (+) | 21 | 25 | 54.3 | |||
| N | Nervous System | (−) | 40 | 20 | 33.3 | <0.001 |
| (+) | 6 | 32 | 84.2 | |||
| R | Respiratory System | (−) | 42 | 39 | 48.1 | 0.059 |
| (+) | 4 | 13 | 76.5 | |||
| V | Various | (−) | 7 | 5 | 41.7 | 0.540 |
| (+) | 39 | 47 | 54.7 | |||
| Number of Patients Receiving Polypharmacy (≥9 Drugs/Day) | |||
|---|---|---|---|
| AOR | 95% Confidence Interval | ||
| Lower | Upper | ||
| A02 (Drugs for Acid-related Disorders) | 11.2 | 3.1 | 40.6 |
| A07 (Antidiarrheal agents, Intestinal Anti-inflammatory/Anti-infective Agents) | 4.9 | 1.1 | 22.3 |
| B01 (Antithrombotic Agents) | 6.8 | 1.8 | 25.4 |
| N05 (Psycholeptics) | 10.5 | 2.3 | 47.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagano, H.; Tomori, K.; Koiwa, M.; Kobayashi, S.; Takahashi, M.; Makabe, H.; Okada, H.; Kushiyama, A. Identification of Prescribing Patterns in Hemodialysis Outpatients Taking Multiple Medications. Pharmacy 2023, 11, 43. https://doi.org/10.3390/pharmacy11020043
Nagano H, Tomori K, Koiwa M, Kobayashi S, Takahashi M, Makabe H, Okada H, Kushiyama A. Identification of Prescribing Patterns in Hemodialysis Outpatients Taking Multiple Medications. Pharmacy. 2023; 11(2):43. https://doi.org/10.3390/pharmacy11020043
Chicago/Turabian StyleNagano, Hiroyuki, Koji Tomori, Mano Koiwa, Shotaro Kobayashi, Masahiro Takahashi, Hideki Makabe, Hirokazu Okada, and Akifumi Kushiyama. 2023. "Identification of Prescribing Patterns in Hemodialysis Outpatients Taking Multiple Medications" Pharmacy 11, no. 2: 43. https://doi.org/10.3390/pharmacy11020043