
Telephone versus In-Person Pharmacist-Led Medication Reviews in Home Dialysis Patients: Evaluating Quality of Care and Patient Satisfaction

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Pharmacist Medication Reviews
2.4. Data Collection
2.4.1. Quantitative Data
2.4.2. Qualitative Data
2.5. Data Analysis
2.5.1. Quantitative Data
Sample Size Estimation
2.5.2. Qualitative Data
3. Results
3.1. Demographics
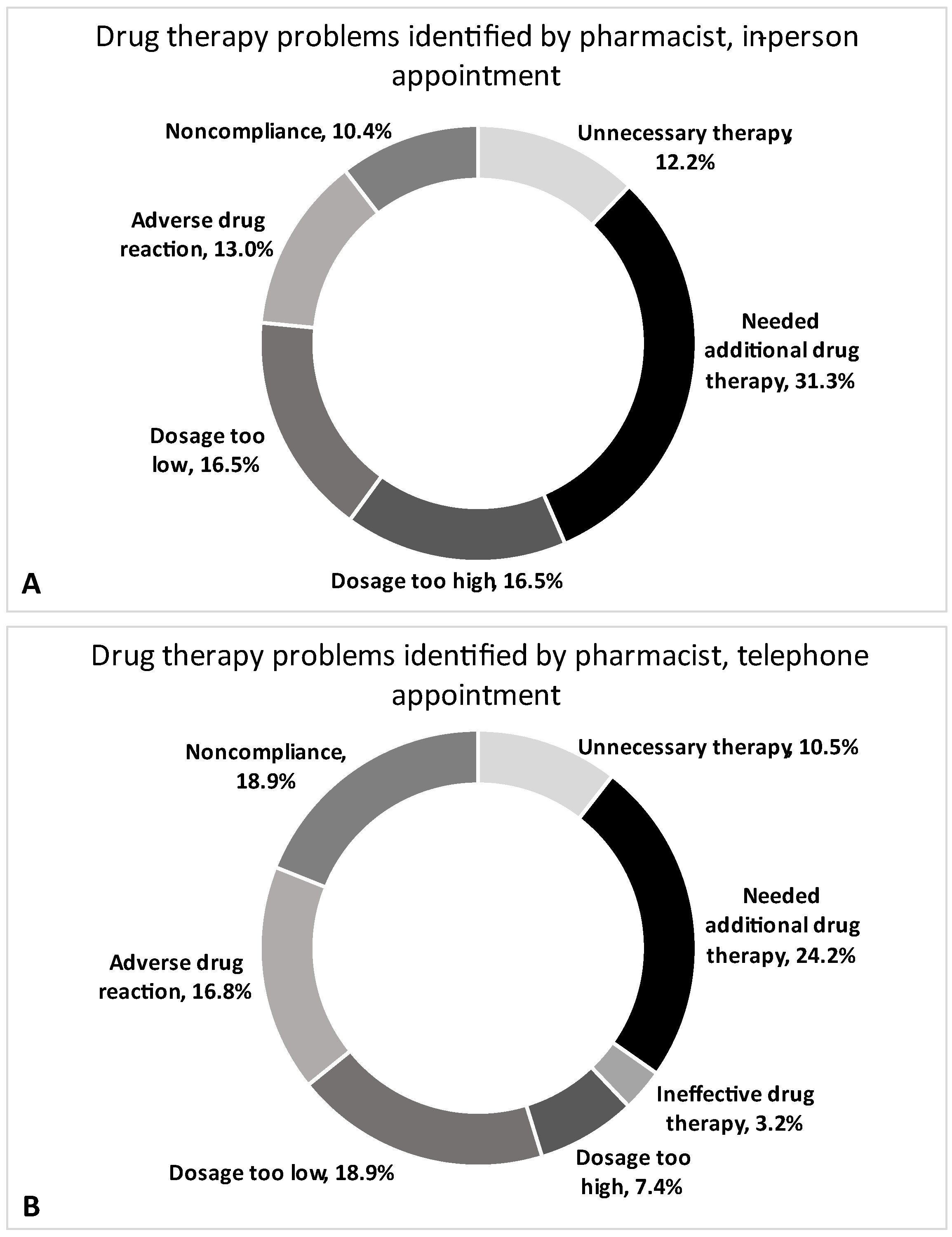
3.2. Pharmacist-Led Medication Review Outcomes
3.3. Patient Satisfaction Survey Outcomes
3.3.1. Quantitative Data
3.3.2. Qualitative Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Patient Survey
- (1)
- Have you had an in-person medication review with a pharmacist in the dialysis clinic?
Yes No - (2)
- Have you had a telephone medication review with a pharmacist from the dialysis clinic?
Please check the box that corresponds with your level of agreement to each of the following statements about medication reviews with the dialysis pharmacist completed over the telephone.Yes No - (3)
- I am satisfied with the care that I received from the dialysis pharmacist over the telephone.
Strongly disagree Disagree Neither agree or disagree Agree Strongly Agree - (4)
- I am able to communicate effectively with the pharmacist on the telephone.
Strongly disagree Disagree Neither agree or disagree Agree Strongly Agree - (5)
- My privacy and confidentiality were respected and protected during the medication review on the telephone.
Strongly disagree Disagree Neither agree or disagree Agree Strongly Agree - (6)
- The telephone medication reviews are just as good as in-person medication reviews.
Strongly disagree Disagree Neither agree or disagree Agree Strongly Agree - (7)
- How would you prefer to review your medications with the pharmacist in the future?
- I would prefer to review my medications with the pharmacist in person.
- I would prefer to review my medications with the pharmacist over the telephone.
- I would prefer to review my medications with the pharmacist in person once a year, and over the phone the rest of the time
- I don’t have a preference
- (8)
- What would you change about the telephone medication reviews with the pharmacist?_________________________________________________________________
- (9)
- What do you like best about the telephone medication reviews with the pharmacist?_________________________________________________________________
- (10)
- Please provide any additional comments:_________________________________________________________________
References
- Battistella, M.; Ng, P. Addressing polypharmacy in outpatient dialysis units. Clin. J. Am. Soc. Nephrol. 2021, 16, 144–146. [Google Scholar] [CrossRef] [PubMed]
- Chiu, Y.-W.; Teitelbaum, I.; Misra, M.; de Leon, E.M.; Adzize, T.; Mehrotra, R. Pill burden, adherence, hyperphosphatemia, and quality of life in maintenance dialysis patients. Clin. J. Am. Soc. Nephrol. 2009, 4, 1089–1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niriayo, Y.L.; Kumela, K.; Kassa, T.D.; Angamo, M.T. Drug therapy problems and contributing factors in the management of heart failure patients in Jimma University Specialized Hospital, Southwest Ethiopia. PLoS ONE 2018, 13, e0206120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinhandl, E.D.; Arneson, T.J.; St. Peter, W.L. Clinical outcomes associated with receipt of integrated pharmacy services by hemodialysis patients: A quality improvement report. Am. J. Kidney Dis. 2013, 62, 557–567. [Google Scholar] [CrossRef] [PubMed]
- Unni, E.J.; Patel, K.; Beazer, I.R.; Hung, M. Telepharmacy during COVID-19: A scoping review. Pharmacy 2021, 9, 183. [Google Scholar] [CrossRef] [PubMed]
- Niznik, J.D.; He, H.; Kane-Gill, S.L. Impact of clinical pharmacist services delivered via telemedicine in the outpatient or ambulatory care setting: A systematic review. Res. Social. Adm. Pharm. 2018, 14, 707–717. [Google Scholar] [CrossRef] [PubMed]
- Strnad, K.; Shoulders, B.R.; Smithburger, P.L.; Kane-Gill, S.L. A systematic review of ICU and non-ICU clinical pharmacy services using telepharmacy. Ann. Pharmacother. 2018, 52, 1250–1258. [Google Scholar] [CrossRef] [PubMed]
- Bruns, B.E.; Lorenzo-Castro, S.A.; Hale, G.M. Controlling blood pressure during a pandemic: The impact of telepharmacy for primary care patients. J. Pharm. Pract. 2022. [Google Scholar] [CrossRef] [PubMed]
- Cao, D.X.; Tran, R.J.C.; Yamzon, J.; Stewart, T.L.; Hernandez, E.A. Effectiveness of telepharmacy diabetes services: A systematic review and meta-analysis. Am. J. Health Syst. Pharm. 2022, 79, 860–872. [Google Scholar] [CrossRef] [PubMed]
- Iftinan, G.N.; Wathoni, N.; Lestari, K. Telepharmacy: A potential alternative approach for diabetic patients during the COVID-19 pandemic. J. Multidiscip. Healthc. 2021, 14, 2261–2273. [Google Scholar] [CrossRef] [PubMed]
- Al Ammari, M.; AlThiab, K.; AlJohani, M.; Sultana, K.; Maklhafi, N.; AlOnazi, H.; Maringa, A. Tele-pharmacy anticoagulation clinic during COVID-19 pandemic: Patient outcomes. Front. Pharmacol. 2021, 12, 652482. [Google Scholar] [CrossRef] [PubMed]
- Al Raiisi, F.; Stewart, D.; Fernandez-Llimos, F.; Salgado, T.M.; Mohamed, M.F.; Cunningham, S. Clinical pharmacy practice in the care of Chronic Kidney Disease patients: A systematic review. Int. J. Clin. Pharm. 2019, 41, 630–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Berlo-van de Laar, I.R.F.; Sluiter, H.E.; van’t Riet, E.; Taxis, K.; Jansman, F.G.A. Pharmacist-led medication reviews in pre-dialysis and dialysis patients. Res. Social. Adm. Pharm. 2020, 16, 1718–1723. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates, Publishers: Mahweh, NJ, USA, 1988. [Google Scholar]
- Dat, T.V.; Tu, V.L.; Quan, N.K.; Minh, N.H.; Trung, T.D.; Le, T.N.; Phuc-Vinh, D.; Trinh, D.-T.T.; Pham Dinh, L.; Nguyen-Thi, H.-Y.; et al. Telepharmacy: A systematic review of field application, benefits, limitations, and applicability during the COVID-19 pandemic. Telemed. e-Health 2022. ahead-of-print. [Google Scholar] [CrossRef]
- Park, L.; Kim, J.H.; Waldman, G.; Marks, C.R.; Clark, J.E. Impact analysis of virtual ambulatory transplant pharmacists during COVID-19. J. Am. Coll. Clin. Pharm. 2021, 4, 978–987. [Google Scholar] [CrossRef] [PubMed]
- Durand, A.; Gillibert, A.; Membre, S.; Mondet, L.; Lenglet, A.; Mary, A. Acceptance factors for in-hospital pharmacist interventions in daily practice: A retrospective study. Front. Pharmacol. 2022, 13, 811289. [Google Scholar] [CrossRef] [PubMed]
- McNamara, A.; Zhao, M.; Lee, S.Y. Evaluating the primary care clinical pharmacist visit transition to telehealth during the COVID-19 pandemic by comparing medication related problems from telehealth visits and in-person visits. J. Am. Coll. Clin. Pharm. 2021, 4, 914–923. [Google Scholar] [CrossRef] [PubMed]
- Heyck Lee, S.; Ramondino, S.; Gallo, K.; Moist, L.M. A quantitative and qualitative study on patient and physician perceptions of nephrology telephone consultation during COVID-19. Can. J. Kidney Health Dis. 2022, 9, 1–8. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Outcome |
|---|---|
| Demographics | |
| Male, N (%) | 20 (43.5) |
| Female, N (%) | 26 (56.5) |
| Age, years, mean (SD) | 59.3 (12.5) |
| Time on dialysis, years, mean (SD) | 3.6 (2.4) |
| Number of medications, mean (SD) | 11.3 (3.7) |
| Number of comorbidities, mean (SD) | 5.9 (2.3) |
| Comorbidities, N (%) | |
| Hypertension | 39 (84.8) |
| Diabetes | 25 (54.3) |
| Dyslipidemia | 16 (34.8) |
| Osteoarthritis | 8 (17.4) |
| Gout | 6 (13.0) |
| Atrial Fibrillation | 5 (10.9) |
| Polycystic Kidney Disease | 5 (10.9) |
| GERD | 4 (8.7) |
| COPD | 4 (8.7) |
| Peripheral Vascular Disease | 4 (8.7) |
| Measure | Median (IQR) | p-Value | ES |
|---|---|---|---|
| Number of recommendations, per visit | 0.200 | −0.13 | |
| In-person | 1.0 (0.5–1.5) | ||
| Telephone | 1.0 (0.38–1.5) | ||
| Acceptance of pharmacist intervention | 0.009 | −0.27 | |
| In-person | 1.0 (1.0–2.0) | ||
| Telephone | 0.0 (0.0–2.0) | ||
| No acceptance of pharmacist intervention | 0.057 | 0.20 | |
| In-person | 0.0 (0.0–1.0) | ||
| Telephone | 0.0 (0.0–1.0) | ||
| Acceptance of pharmacist intervention with change | 0.564 | −0.06 | |
| In-person | 0.0 (0.0–0.0) | ||
| Telephone | 0.0 (0.0–0.0) | ||
| Total drug therapy problems (DTPs) | 0.431 | −0.08 | |
| In-person | 2.0 (1.0–4.0) | ||
| Telephone | 2.0 (1.0–3.0) | ||
| Unnecessary drug therapy | 0.415 | −0.09 | |
| In-person | 0.0 (0.0–0.25) | ||
| Telephone | 0.0 (0.0–0.0) | ||
| Needed additional drug therapy | 0.094 | −0.17 | |
| In-person | 1.0 (0.0–1.0) | ||
| Telephone | 0.0 (0.0–1.0) | ||
| Ineffective drug therapy | 0.083 | 0.18 | |
| In-person | 0.0 (0.0–0.0) | ||
| Telephone | 0.0 (0.0–0.0) | ||
| Dosage too high | 0.089 | −0.18 | |
| In-person | 0.0 (0.0–1.0) | ||
| Telephone | 0.0 (0.0–0.0) | ||
| Dosage too low | 0.968 | −0.004 | |
| In-person | 0.0 (0.0–1.0) | ||
| Telephone | 0.0 (0.0–1.0) | ||
| Adverse drug reaction | 0.909 | 0.01 | |
| In-person | 0.0 (0.0–0.25) | ||
| Telephone | 0.0 (0.0–1.0) | ||
| Non-adherence | 0.186 | 0.14 | |
| In-person | 0.0 (0.0–0.0) | ||
| Telephone | 0.0 (0.0–1.0) |
| What Would You Change about the Telephone Medication Reviews with the Pharmacist? | ||
|---|---|---|
| Theme | # of Statements | Quotes |
| In-person visits only | 1 | “I don’t like virtual care” |
| Schedule appointment times in advance | 1 | “The one thing I would prefer would be a designated time and date, as opposed to getting an unexpected call. I like to have my med list in front of me, and have any questions I may have, prepared.” |
| Speak Louder | 1 | “If the pharmacist spoke a little louder.” |
| Change Nothing | 16 | “I wouldn’t change anything” |
| What do you Like Best about the Telephone Medication Reviews with the Pharmacist? | ||
| Theme | # of Statements | Quotes |
| Similar quality of care | 3 | “There is no difference between in person and telephone visits” |
| No travel required | 7 | “I live out of town, saves having to go for in person visit” “I don’t have to go to the hospital” |
| Efficient and patient-centered care | 5 | “The pharmacists are open and personable, effective and efficient during every visit.” “The professional yet personal experience” |
| Convenient for patient | 7 | “Quick, easy, and it saves time” “More convenient, I don’t have to be there” “It doesn’t take as much time” |
| Enjoy all of it | 1 | “All of it” |
| Please Provide any Additional Comments | ||
| Theme | # of Statements | Quotes |
| Patients are satisfied with the care they receive from pharmacists | 5 | “I am satisfied with the care I receive from the pharmacists” “I find the pharmacists to be very thorough, professional and informative.” |
| Better care is perceived to be obtained through in-person visits | 3 | “I feel if they see me they will do better, but you can’t do that on the phone. If you don’t tell them everything that’s going on they won’t know.” “I feel a disconnect with COVID and telephone visits.” |
| No issues | 2 | “No issues with pharmacy” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allen, K.; Flewelling, A.J.; Munro, L.; Naylor, H. Telephone versus In-Person Pharmacist-Led Medication Reviews in Home Dialysis Patients: Evaluating Quality of Care and Patient Satisfaction. Pharmacy 2023, 11, 1. https://doi.org/10.3390/pharmacy11010001
Allen K, Flewelling AJ, Munro L, Naylor H. Telephone versus In-Person Pharmacist-Led Medication Reviews in Home Dialysis Patients: Evaluating Quality of Care and Patient Satisfaction. Pharmacy. 2023; 11(1):1. https://doi.org/10.3390/pharmacy11010001
Chicago/Turabian StyleAllen, Kelsey, Andrew J. Flewelling, Lauren Munro, and Heather Naylor. 2023. "Telephone versus In-Person Pharmacist-Led Medication Reviews in Home Dialysis Patients: Evaluating Quality of Care and Patient Satisfaction" Pharmacy 11, no. 1: 1. https://doi.org/10.3390/pharmacy11010001