
The Moderating Power of Impulsivity: A Systematic Literature Review Examining the Theory of Planned Behavior


(This article belongs to the Section Pharmacy Practice and Practice-Based Research)
Abstract
:1. Introduction
2. Methods
3. Results
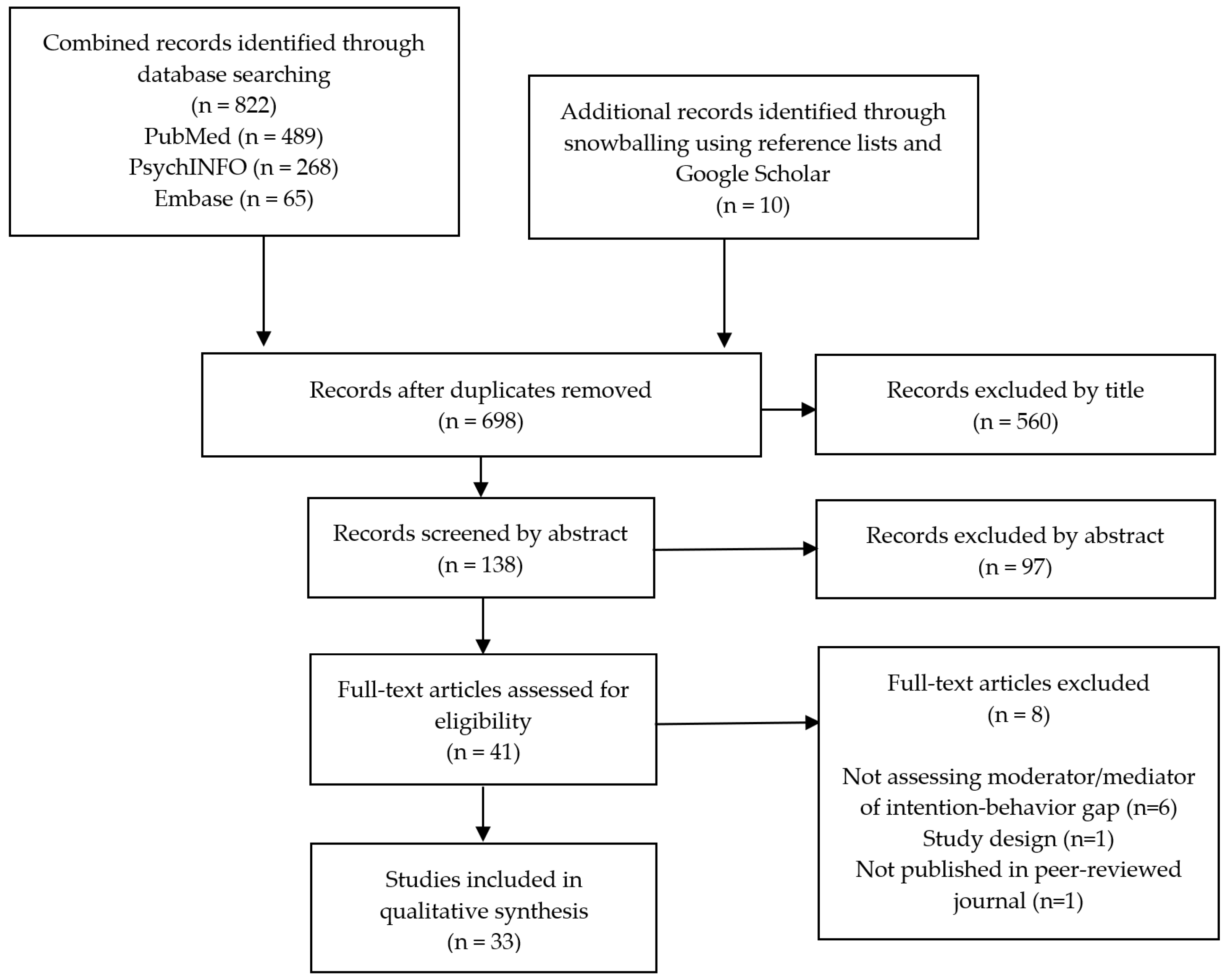
3.1. Database Hits
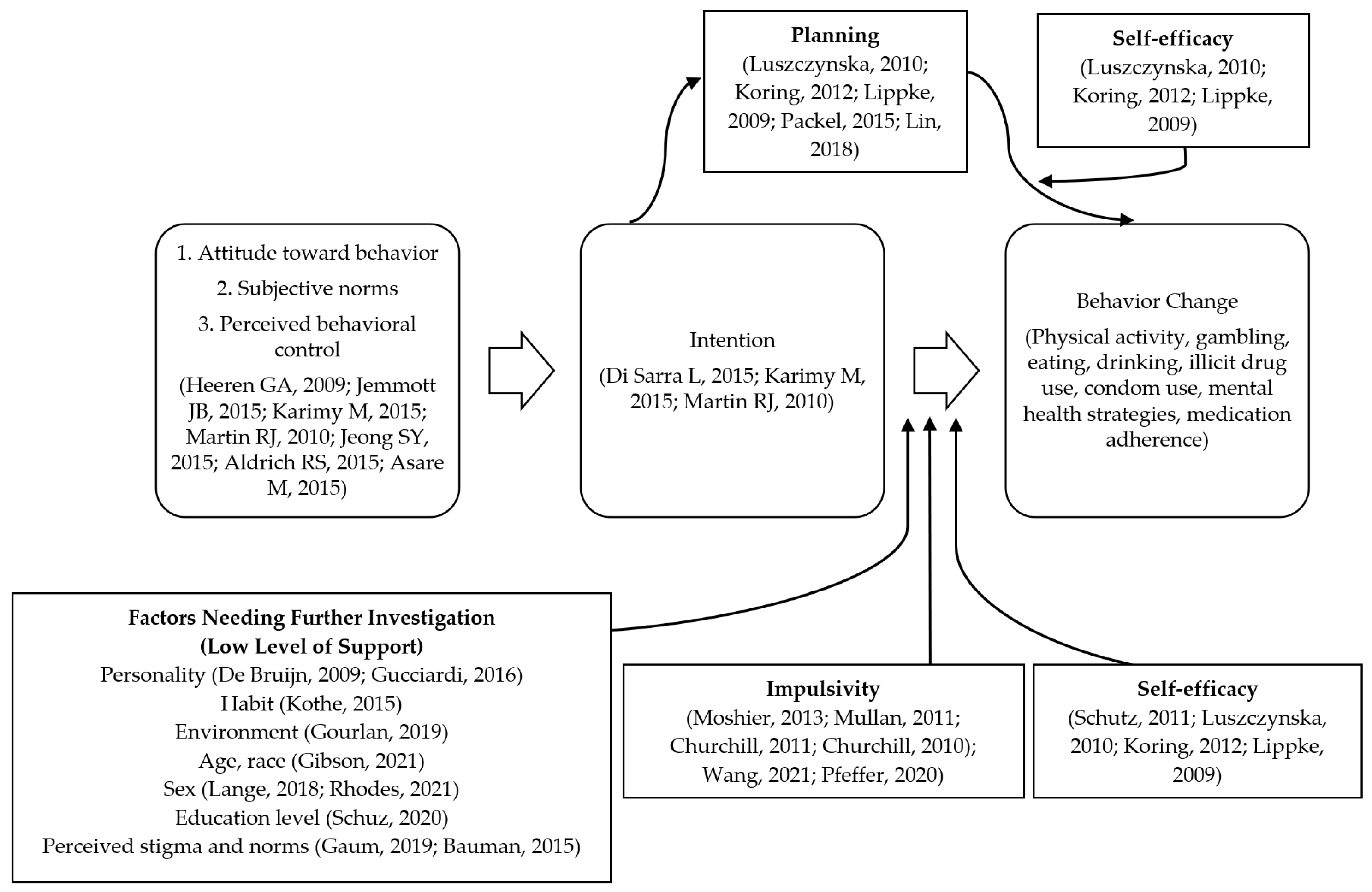
3.2. Moderators and Mediators with a High Level of Support
3.2.1. Impulsivity Moderates the Association between Intention and Behavior Change
3.2.2. Self-Efficacy Moderates the Association between Intention and Behavior Change
3.2.3. Planning Mediates the Association between Intention and Behavior Change
3.2.4. Planning and Self-Efficacy Contribute to Moderated Mediation
3.3. Moderators and Mediators with Less Support
3.3.1. Personality Moderates the Association between Intention and Behavior Change
3.3.2. Socioeconomic Factors Moderate the Association between Intention and Behavior Change
3.3.3. Perceptions and Beliefs Regarding Stigma and Norms Moderate the Association between Intention and Behavior Change
3.3.4. Environment Moderates the Association between Intention and Behavior Change
3.3.5. Habit Moderates the Association between Intention and Behavior Change
4. Discussion
4.1. Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ajzen, I. Theories of Cognitive Self-Regulation, the Theory of Planned Behavior. Organ. Behav. Hum. Decis. Processes 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Conner, M.; Armitage, C.J. Extending the theory of planned behavior: A review and avenues for further research. J. Appl. Soc. Psychol. 1998, 28, 1429–1464. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior: Frequently asked questions. Hum. Behav. Emerg. Technol. 2020, 2, 314–324. [Google Scholar] [CrossRef]
- Pearson, M.R.; Henson, J.M. Unplanned drinking and alcohol-related problems: A preliminary test of the model of unplanned drinking behavior. Psychol. Addict. Behav. 2013, 27, 584–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heeren, G.A.; Jemmott, J.B., 3rd; Mandeya, A.; Tyler, J.C. Sub-Saharan African university students’ beliefs about condoms, condom-use intention, and subsequent condom use: A prospective study. AIDS Behav. 2009, 13, 268–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jemmott, J.B., 3rd; Stephens-Shields, A.; O’Leary, A.; Jemmott, L.S.; Teitelman, A.; Ngwane, Z.; Mtose, X. Mediation of effects of a theory-based behavioral intervention on self-reported physical activity in South African men. Prev. Med. 2015, 72, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reyes Fernandez, B.; Warner, L.M.; Knoll, N.; Montenegro Montenegro, E.; Schwarzer, R. Synergistic effects of social support and self-efficacy on dietary motivation predicting fruit and vegetable intake. Appetite 2015, 87, 330–335. [Google Scholar] [CrossRef] [Green Version]
- McDermott, M.S.; Oliver, M.; Simnadis, T.; Beck, E.J.; Coltman, T.; Iverson, D.; Caputi, P.; Sharma, R. The Theory of Planned Behaviour and dietary patterns: A systematic review and meta-analysis. Prev. Med. 2015, 81, 150–156. [Google Scholar] [CrossRef] [Green Version]
- Di Sarra, L.; Ghezzi, V.; Eastland, T.Y.; Antonini, F.; Scialo, G.; Zega, M.; Alvaro, R. Applying the Theory of Planned Behavior to Explain Women’s Role in Prostate Cancer Screening. Res. Theory Nurs. Pract. 2015, 29, 200–213. [Google Scholar] [CrossRef]
- Karimy, M.; Zareban, I.; Araban, M.; Montazeri, A. An Extended Theory of Planned Behavior (TPB) Used to Predict Smoking Behavior Among a Sample of Iranian Medical Students. Int. J. High Risk Behav. Addict. 2015, 4, e24715. [Google Scholar] [CrossRef] [Green Version]
- Martin, R.J.; Usdan, S.; Nelson, S.; Umstattd, M.R.; Laplante, D.; Perko, M.; Shaffer, H. Using the theory of planned behavior to predict gambling behavior. Psychol. Addict. Behav. 2010, 24, 89–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, S.Y.; Kim, K.M. Influencing factors on hand hygiene behavior of nursing students based on theory of planned behavior: A descriptive survey study. Nurse Educ. Today 2016, 36, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Godin, G.; Gagnon, H.; Lambert, L.-D.; Conner, M. Determinants of condom use among a random sample of single heterosexual adults. Br. J. Health Psychol. 2005, 10, 85–100. [Google Scholar] [CrossRef] [PubMed]
- Aldrich, R.S. Using the Theory of Planned Behavior to Predict College Students’ Intention to Intervene with a Suicidal Individual. Crisis 2015, 36, 332–337. [Google Scholar] [CrossRef]
- Asare, M. Using the Theory of Planned Behavior to Determine the Condom Use Behavior Among College Students. Am. J. Health Stud. 2015, 30, 43–50. [Google Scholar] [CrossRef]
- Luszczynska, A.; Sheng Cao, D.; Mallach, N.; Pietron, K.; Mazurkiewicz, M.; Schwarzer, R. Intentions, planning, and self-efficacy predict physical activity in Chinese and Polish adolescents: Two moderated mediation analyses. Int. J. Clin. Health Psychol. 2010, 10, 265–278. [Google Scholar]
- Scribbr. Mediator vs. Moderator Variables. 2021. Available online: https://www.scribbr.com/methodology/mediator-vs-moderator/ (accessed on 10 June 2022).
- Rice, T. The Behavioral Economics of Health and Health Care. Annu. Rev. Public Health 2013, 34, 431–447. [Google Scholar] [CrossRef] [Green Version]
- Messina, B.G.; Silvestri, M.M.; Diulio, A.R.; Murphy, J.G.; Garza, K.B.; Correia, C.J. Alcohol use, impulsivity, and the non-medical use of prescription stimulants among college students. Addict. Behav. 2014, 39, 1798–1803. [Google Scholar] [CrossRef]
- Garza, K.B.; Harris, C.V.; Bolding, M.S. Examination of value of the future and health beliefs to explain dietary and physical activity behaviors. Res. Soc. Adm. Pharm. 2013, 9, 851–862. [Google Scholar] [CrossRef]
- Moshier, S.J.; Ewen, M.; Otto, M.W. Impulsivity as a moderator of the intention-behavior relationship for illicit drug use in patients undergoing treatment. Addict. Behav. 2013, 38, 1651–1655. [Google Scholar] [CrossRef] [Green Version]
- Chapman, G.B.; Elstein, A.S. Valuing the future: Temporal discounting of health and money. Med. Decis. Mak. Int. J. Soc. Med. Decis. Mak. 1995, 15, 373–386. [Google Scholar] [CrossRef]
- Price, M.; Higgs, S.; Lee, M. Self-reported eating traits: Underlying components of food responsivity and dietary restriction are positively related to BMI. Appetite 2015, 95, 203–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Lin, L. The moderating effects of impulsivity on Chinese rural young suicide. J. Clin. Psychol. 2014, 70, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Hohmann, N.S.; McDaniel, C.C.; Mason, S.W.; Cheung, W.Y.; Williams, M.S.; Salvador, C.; Graves, E.K.; Camp, C.N.; Chou, C. Healthcare providers’ perspectives on care coordination for adults with cancer and multiple chronic conditions: A systematic review. J. Pharm. Health Serv. Res. 2020, 11, 97–116. [Google Scholar] [CrossRef]
- Churchill, S.; Jessop, D. Spontaneous implementation intentions and impulsivity: Can impulsivity moderate the effectiveness of planning strategies? Br. J. Health Psychol. 2010, 15, 529–541. [Google Scholar] [CrossRef]
- Churchill, S.; Jessop, D.C. Too impulsive for implementation intentions? Evidence that impulsivity moderates the effectiveness of an implementation intention intervention. Psychol. Health 2011, 26, 517–530. [Google Scholar] [CrossRef]
- Mullan, B.; Wong, C.; Allom, V.; Pack, S.L. The role of executive function in bridging the intention-behaviour gap for binge-drinking in university students. Addict. Behav. 2011, 36, 1023–1026. [Google Scholar] [CrossRef] [Green Version]
- Pfeffer, I.; Strobach, T. Physical activity automaticity, intention, and trait self-control as predictors of physical activity behavior—A dual-process perspective. Psychol. Health Med. 2022, 27, 1021–1034. [Google Scholar] [CrossRef]
- Wang, X.; Won, D.; Jeon, H.S. Predictors of Sports Gambling among College Students: The Role of the Theory of Planned Behavior and Problem Gambling Severity. Int. J. Environ. Res. Public Health 2021, 18, 1803. [Google Scholar] [CrossRef]
- Chevance, G.; Stephan, Y.; Héraud, N.; Boiché, J. Interaction between self-regulation, intentions and implicit attitudes in the prediction of physical activity among persons with obesity. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2018, 37, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Crandall, A.; Cheung, A.; Young, A.; Hooper, A.P. Theory-Based Predictors of Mindfulness Meditation Mobile App Usage: A Survey and Cohort Study. JMIR Mhealth Uhealth 2019, 7, e10794. [Google Scholar] [CrossRef]
- Stevens, A.K.; Littlefield, A.K.; Talley, A.E.; Brown, J.L. Do individuals higher in impulsivity drink more impulsively? A pilot study within a high risk sample of young adults. Addict. Behav. 2017, 65, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Schutz, M.; Godin, G.; Kok, G.; Vézina-Im, L.-A.; Naccache, H.; Otis, J.; MAYA Study Group. Determinants of condom use among HIV-positive men who have sex with men. Int. J. STD AIDS 2011, 22, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Koring, M.; Richert, J.; Lippke, S.; Parschau, L.; Reuter, T.; Schwarzer, R. Synergistic effects of planning and self-efficacy on physical activity. Health Educ. Behav. Off. Publ. Soc. Public Health Educ. 2012, 39, 152–158. [Google Scholar] [CrossRef]
- Lippke, S.; Wiedemann, A.U.; Ziegelmann, J.P.; Reuter, T.; Schwarzer, R. Self-efficacy moderates the mediation of intentions into behavior via plans. Am. J. Health Behav. 2009, 33, 521–529. [Google Scholar] [CrossRef] [Green Version]
- Zhang, R.; Zhang, C.Q.; Gan, Y.; Li, D.; Rhodes, R.E. Predicting Transport-Related Walking in Chinese Employees by Integrating Worksite Neighbourhood Walkability and Social Cognition. Appl. Psychol. Health Well-Being 2019, 11, 484–498. [Google Scholar] [CrossRef]
- Kothe, E.J.; Sainsbury, K.; Smith, L.; Mullan, B.A. Explaining the intention–behaviour gap in gluten-free diet adherence: The moderating roles of habit and perceived behavioural control. J. Health Psychol. 2015, 20, 580–591. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.Q.; Fang, R.; Zhang, R.; Hagger, M.S.; Hamilton, K. Predicting Hand Washing and Sleep Hygiene Behaviors among College Students: Test of an Integrated Social-Cognition Model. Int. J. Environ. Res. Public Health 2020, 17, 1209. [Google Scholar] [CrossRef] [Green Version]
- Allom, V.; Mullan, B.; Cowie, E.; Hamilton, K. Physical Activity and Transitioning to College: The Importance of Intentions and Habits. Am. J. Health Behav. 2016, 40, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.Y.; Broström, A.; Nilsen, P.; Pakpour, A.H. Using extended theory of planned behavior to understand aspirin adherence in pregnant women. Pregnancy Hypertens. 2018, 12, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Packel, L.B.; Prehn, A.W.; Anderson, C.L.; Fisher, P.L. Factors influencing physical activity behaviors in colorectal cancer survivors. Am. J. Health Promot. AJHP 2015, 30, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Gucciardi, D.F. Mental toughness as a moderator of the intention-behaviour gap in the rehabilitation of knee pain. J. Sci. Med. Sport 2016, 19, 454–458. [Google Scholar] [CrossRef] [PubMed]
- de Bruijn, G.-J.; Brug, J.; Van Lenthe, F.J. Neuroticism, conscientiousness and fruit consumption: Exploring mediator and moderator effects in the theory of planned behaviour. Psychol. Health 2009, 24, 1051–1069. [Google Scholar] [CrossRef]
- MacCann, C.; Todd, J.; Mullan, B.A.; Roberts, R.D. Can personality bridge the intention-behavior gap to predict who will exercise? Am. J. Health Behav. 2015, 39, 140–147. [Google Scholar] [CrossRef]
- Monds, L.A.; MacCann, C.; Mullan, B.A.; Wong, C.; Todd, J.; Roberts, R.D. Can personality close the intention-behavior gap for healthy eating? An examination with the HEXACO personality traits. Psychol. Health Med. 2016, 21, 845–855. [Google Scholar] [CrossRef]
- Cao, Z.; Yang, Y.; Ding, W.; Huang, Z. From Physical Activity Intention to Behavior: The Moderation Role of Mental Toughness Among College Students and Wage Earners. Front. Psychol. 2021, 12, 584760. [Google Scholar] [CrossRef]
- Hannan, T.E.; Moffitt, R.L.; Neumann, D.L.; Thomas, P.R. Applying the Theory of Planned Behavior to Physical Activity: The Moderating Role of Mental Toughness. J. Sport Exerc. Psychol. 2015, 37, 514–522. [Google Scholar] [CrossRef]
- Hartson, K.R.; Avila, M.; Gance-Cleveland, B.; Harpin, S.B.; Tigges, B.; Cook, P.F. Predictors of Physical Activity in a Predominantly Hispanic Sample of Adolescents. West. J. Nurs. Res. 2020, 42, 514–523. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Beauchamp, M.R.; Quinlan, A.; Symons Downs, D.; Warburton, D.E.R.; Blanchard, C.M. Predicting the physical activity of new parents who participated in a physical activity intervention. Soc. Sci. Med. 2021, 284, 114221. [Google Scholar] [CrossRef] [PubMed]
- Gibson, L.P.; Magnan, R.E.; Kramer, E.B.; Bryan, A.D. Theory of Planned Behavior Analysis of Social Distancing During the COVID-19 Pandemic: Focusing on the Intention-Behavior Gap. Ann. Behav. Med. A Publ. Soc. Behav. Med. 2021, 55, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Schüz, B.; Brick, C.; Wilding, S.; Conner, M. Socioeconomic Status Moderates the Effects of Health Cognitions on Health Behaviors within Participants: Two Multibehavior Studies. Ann. Behav. Med. A Publ. Soc. Behav. Med. 2020, 54, 36–48. [Google Scholar] [CrossRef] [PubMed]
- Lange, D.; Barz, M.; Baldensperger, L.; Lippke, S.; Knoll, N.; Schwarzer, R. Sex differential mediation effects of planning within the health behavior change process. Soc. Sci. Med. 2018, 211, 137–146. [Google Scholar] [CrossRef]
- Gaum, P.M.; Brey, F.; Kraus, T.; Lang, J. Does stigmatization moderate the association between intention and implementation of learned prevention-strategies at work after a depressive episode?—A cross-sectional pilot study. J. Occup. Med. Toxicol. 2019, 14, 26. [Google Scholar] [CrossRef] [Green Version]
- Baumann, S.; Gaertner, B.; Schnuerer, I.; Haberecht, K.; John, U.; Freyer-Adam, J. Belief incongruence and the intention-behavior gap in persons with at-risk alcohol use. Addict. Behav. 2015, 48, 5–11. [Google Scholar] [CrossRef]
- Gourlan, M.; Bord, A.; Cousson-Gélie, F. From intentions formation to their translation into behavior: An extended model of theory of planned behavior in the exercise domain. Sport Exerc. Perform. Psychol. 2019, 8, 317–333. [Google Scholar] [CrossRef]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191. [Google Scholar] [CrossRef]
- St-Pierre, R.A.; Temcheff, C.E.; Derevensky, J.L.; Gupta, R. Theory of Planned Behavior in School-Based Adolescent Problem Gambling Prevention: A Conceptual Framework. J. Prim. Prev. 2015, 36, 361–385. [Google Scholar] [CrossRef]
- Norman, P.; Conner, M. Health Behavior. In Reference Module in Neuroscience and Biobehavioral Psychology; Elsevier: Amsterdam, The Netherlands, 2017. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Dickau, L. Moderators of the intention-behaviour relationship in the physical activity domain: A systematic review. Br. J. Sports Med. 2013, 47, 215–225. [Google Scholar] [CrossRef]
- Starfelt Sutton, L.C.; White, K.M. Predicting sun-protective intentions and behaviours using the theory of planned behaviour: A systematic review and meta-analysis. Psychol. Health 2016, 31, 1272–1292. [Google Scholar] [CrossRef] [PubMed]
- Verdoux, H.; Lengronne, J.; Liraud, F.; Gonzales, B.; Assens, F.; Abalan, F.; Os, J.V. Medication adherence in psychosis: Predictors and impact on outcome. A 2-year follow-up of first-admitted subjects. Acta Psychiatr. Scand. 2000, 102, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, M.; Golin, C.E.; Jones, C.D.; Ashok, M.; Blalock, S.J.; Wines, R.C.; Coker-Schwimmer, E.J.; Rosen, D.L.; Sista, P.; Lohr, K.N. Interventions to improve adherence to self-administered medications for chronic diseases in the United States: A systematic review. Ann. Intern. Med. 2012, 157, 785–795. [Google Scholar] [CrossRef] [PubMed]
- Halpern, S.D.; Asch, D.A.; Volpp, K.G. Commitment contracts as a way to health. BMJ 2012, 344, e522. [Google Scholar] [CrossRef] [Green Version]
- Reimann, M.; Bechara, A.; MacInnis, D. Leveraging the happy meal effect: Substituting food with modest nonfood incentives decreases portion size choice. J. Exp. Psychol. Appl. 2015, 21, 276–286. [Google Scholar] [CrossRef] [Green Version]
- Scholz, U.; Schuz, B.; Ziegelmann, J.P.; Lippke, S.; Schwarzer, R. Beyond behavioural intentions: Planning mediates between intentions and physical activity. Br. J. Health Psychol. 2008, 13, 479–494. [Google Scholar] [CrossRef] [Green Version]
- Caudroit, J.; Boiche, J.; Stephan, Y. The role of action and coping planning in the relationship between intention and physical activity: A moderated mediation analysis. Psychol. Health 2014, 29, 768–780. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Article Author, Year | Study Design | Intervention Population | Follow-Up Period | Behavior of Interest | Moderating or Mediating Variables (Scales) | Statistical Significance (p-Value) |
|---|---|---|---|---|---|---|
| Allom, 2016 [42] | Noncontrolled timeseries (pre-post)—T1, T2 | n = 101 Australian college students Mean age: 19.60 yrs Female: 81.40% | 1 week | Physical activity | Moderation | |
| No | |||||
| Baumann, 2015 [57] | Noncontrolled timeseries (pre-post)—T1, T2 | n = 433 German adult job agency clients Mean age: 30.6 yrs Female: 36% | 3 months | At-risk alcohol use | Moderation | |
| ||||||
| ○ Normative belief incongruence (4-item measure) | Yes (<0.05) | |||||
| ○ Behavioral belief incongruence (6-item measure) | No | |||||
| ○ Control belief incongruence (4-item measure) | No | |||||
| Cao, 2021 [49] | Noncontrolled timeseries (pre-post)—T1, T2 | n = 591 Chinese college students Mean age: not reported (range 19–24 yrs) Female: 57.53%; and n = 285 Chinese adult wage earners Mean age: not reported (range 27–58 yrs) Female: 44.56% | 1 week | Physical activity | Moderation | |
| ||||||
| ○ Among college students | Yes (<0.01) | |||||
| ○ Among wage earners | No | |||||
| Chevance, 2018 [33] | Noncontrolled timeseries (pre-post)—T1, T2 | n = 76 French adults Mean age: 56 yrs Female: not reported | 4 months | Physical activity | Moderation | |
| No | |||||
| ○ Lack of conscientiousness | No | |||||
| No | |||||
| Churchill, 2010 [28] | Noncontrolled timeseries (pre-post)—T1, T2 | n = 256 UK adults Mean age: 33.05 yrs Female: 79.36% | 2 weeks | Avoidance of snacking | Moderation | |
| ||||||
| ○ Urgency | Yes (<0.05) | |||||
| ○ Lack of premeditation | No | |||||
| ○ Lack of perseverance | No | |||||
| ○ Sensation seeking | No | |||||
| Churchill, 2011 [29] | Controlled timeseries—T1, T2, T3 | n = 323 UK adults Mean age: 32.8 yrs Female: 81.42% Students: 52.94% | 2 weeks (1-week intervals) | Fruit and vegetable consumption | Moderation | |
| ||||||
| ○ Urgency | Yes (<0.05) | |||||
| ○ Lack of premeditation | No | |||||
| ○ Lack of perseverance | No | |||||
| ○ Sensation seeking | No | |||||
| Crandall, 2019 [34] | Noncontrolled timeseries (pre-post)—T1, T2 | n = 85 Undergraduate college students in Utah, US Mean age: 21.81 yrs Female: 53% | 2 weeks | Mindfulness meditation mobile app use | Moderation | |
| No | |||||
| ○ Cognitive shifting (NIH-TB Dimensional Change Card-Sort Test) | No | |||||
| ○ Inhibitory control and attention (NIH-TB Flanker Inhibitory Control and Attention Test) | No | |||||
| ○ Working memory (NIH-TB List-Sorting Working Memory Test) | No | |||||
| De Bruijn, 2009 [46] | Cross-sectional interviewer-administered survey | n = 405 Dutch adults Mean age: 60.25 yrs Female: 57.53% | No follow-up | Fruit consumption | Moderation | |
| ||||||
| ○ Neuroticism (6-item measure) | Yes (<0.001) | |||||
| ○ Conscientiousness (6-item measure) | No | |||||
| Gaum, 2019 [56] | Cross-sectional survey | n = 112 German adults with history of depression Mean age: 42.3 yrs Female: 75% | No follow-up | Implementation of depression prevention strategies at work | Moderation | |
| Yes (0.003) | |||||
| No | |||||
| Gibson, 2021 [53] | Noncontrolled timeseries (pre-post)—T1, T2 | n = 507 US adults Mean age: 50.39 yrs Female: 50.9% | 3 months | Social distancing during COVID-19 | Moderation | |
| Yes (<0.001) | |||||
| Yes (0.002) | |||||
| Yes (<0.001) | |||||
| Gourlan, 2019 [58] | Noncontrolled timeseries (pre-post)—T1, T2 | n = 219 French adults Mean age: 41.28 Female: 52.51% | 3 months | Physical activity | Moderation | |
| No | |||||
| No | |||||
| Moderated Moderation | ||||||
| Yes (0.02) | |||||
| Gucciardi, 2016 [45] | Noncontrolled timeseries (pre-post)—T1, T2 | n = 193 Australian adults Mean age: 30.79 yrs Female: 55.44% | 2 weeks | Rehabilitation exercises for knee pain | Moderation | |
| Yes (0.013) | |||||
| Hannan, 2015 [50] | Noncontrolled timeseries (pre-post)—T1, T2 | n = 117 Australian adults and undergraduate students Mean age: 28.29 yrs Female: 73.50% | 1 week | Physical activity | Moderation | |
| No | |||||
| Hartson, 2020 [51] | Noncontrolled timeseries (pre-post)—T1, T2 | n = 232 US Hispanic adolescents Mean age: 15.23 yrs Female: 51.3% | 2 weeks | Physical activity | Moderation | |
| No | |||||
| Koring, 2012 [37] | Noncontrolled timeseries—T1, T2, T3 | n = 290 German adults Mean age: 41.9 yrs Female: 77% | 6 weeks | Physical activity | Moderation | |
| Yes (<0.05) | |||||
| Mediation | ||||||
| Yes (<0.05) | |||||
| Moderated Mediation | ||||||
| Yes (<0.05) | |||||
| Kothe, 2015 [40] | Cross-sectional survey | n = 228 Australian adults with Celiac disease Mean age: 45.2 yrs Female: 89.5% | No follow-up | Gluten-free diet adherence | Moderation | |
| No | |||||
| Yes (0.013) | |||||
| Moderated Moderation | ||||||
| Yes (<0.001) | |||||
| Lange, 2018 [55] | Study I. Noncontrolled timeseries—T1, T2, T3 | n = 461 German adults Mean age: 38.2 yrs Female: 81.6% | 4 months | Fruit and vegetable intake | Moderated Mediation | |
| Yes (0.040) | |||||
| Study II. Noncontrolled timeseries—T1, T2, T3 | n = 193 German university students Mean age: 24.5 yrs Female: 80.8% | 2 weeks | Physical activity |
| Yes (0.022) | |
| Study III. Noncontrolled timeseries (pre-post)—T1, T2 | n = 166 German adults Mean age: 37.6 yrs Female: 49.3% | 2 weeks | Sun protection |
| Yes (0.014) | |
| Lin, 2018 [43] | Noncontrolled timeseries (pre-post)—T1, T2 | n = 535 Iranian women with high-risk pregnancies Mean age: 32.29 yrs Female: 100% | 8 weeks | Medication adherence (aspirin) | Mediation | |
| ||||||
| ○ Action planning (4-item measure) | Yes (<0.01) | |||||
| ○ Coping planning (5-item measure) | Yes (<0.01) | |||||
| Lippke, 2009 [38] | Noncontrolled timeseries (pre-post)—T1, T2 | n = 812 German adults Mean age: 36.69 yrs Female: 74.4% | 4 weeks | Physical activity | Moderation | |
| Yes (<0.01) | |||||
| Mediation | ||||||
| Yes (<0.01) | |||||
| Moderated Mediation | ||||||
| Yes (<0.01) | |||||
| Luszczynska, 2010 [16] | Study I. Noncontrolled timeseries (pre-post)—T1, T2 | n = 534 Chinese adolescents, grades 7–12 Mean age: 13.8 yrs Female: 54% | 4 weeks | Physical activity | Moderation | |
| Yes (<0.01) | |||||
| Mediation | ||||||
| Yes (<0.01) | |||||
| Moderated Mediation | ||||||
| Yes (<0.01) | |||||
| Study II. Noncontrolled timeseries (pre-post)—T1, T2 | n = 620 Polish high school adolescents Mean age: 16.46 yrs Female: 62% | 10 weeks | Physical activity | Moderation | ||
| Yes (<0.05) | |||||
| Mediation | ||||||
| Yes (<0.05) | |||||
| Moderated Mediation | ||||||
| Yes (<0.05) | |||||
| MacCann, 2015 [47] | Cross-sectional survey | n = 1017 US college students Mean age: 23.1 yrs Female: 63.9% | No follow-up | Physical activity | Moderation | |
| ||||||
| ○ Honesty and humility (16 items) | No | |||||
| ○ Emotionality (16 items) | No | |||||
| ○ Extraversion (16 items) | No | |||||
| ○ Agreeableness (16 items) | No | |||||
| ○ Conscientiousness (16 items) | No | |||||
| ○ Openness to Experience (16 items) | No | |||||
| Monds, 2016 [48] | Cross-sectional survey | n = 1036 US college students Mean age: 23.08 yrs Female: 63.9% | No follow-up | Fruit and vegetable consumption | Moderation | |
| ||||||
| ○ Honesty and humility (16 items) | No | |||||
| ○ Emotionality (16 items) | No | |||||
| ○ Extraversion (16 items) | No | |||||
| ○ Agreeableness (16 items) | No | |||||
| ○ Conscientiousness (16 items) | No | |||||
| ○ Openness to Experience (16 items) | No | |||||
| Moshier, 2013 [21] | Cross-sectional survey | n = 84 Adults receiving methadone maintenance treatment from 2 outpatient clinics in Boston, US Mean age: 40 yrs Female: 56% | No follow-up | Illicit drug use | Moderation | |
| ||||||
| ○ Urgency | No | |||||
| ○ Lack of premeditation | Yes (0.015) | |||||
| ○ Lack of perseverance | No | |||||
| ○ Sensation seeking | Yes (0.007) | |||||
| Mullan, 2011 [30] | Noncontrolled timeseries (pre-post)—T1, T2 | n = 153 Australian university students Mean age: 20.1 yrs Female: 73.86% | 1 week | Binge drinking of alcohol | Moderation | |
| ||||||
| ○ Planning ability (the Tower of Hanoi task) | Yes (0.03) | |||||
| ○ Inhibitory control (the Stroop Task) | Yes (0.035) | |||||
| ○ Decision making (the Iowa Gambling Task) | No | |||||
| ○ Cognitive flexibility (the Wisconsin Card-Sorting Task) | No | |||||
| Packel, 2015 [44] | Cross-sectional survey | n = 96 Adults with colorectal cancer in Pennsylvania, US Mean age: 65.6 yrs Female: % not reported | No follow-up | Physical activity | Mediation | |
| ||||||
| ○ Action planning (4-item Action-Planning and Coping-Planning Scale—Physical Exercise) | Yes (0.007) | |||||
| ○ Coping planning (5-item Action-Planning and Coping-Planning Scale—Physical Exercise) | Yes (0.001) | |||||
| Pfeffer, 2020 [31] | Noncontrolled timeseries (pre-post)—T1, T2 | n = 118 University students Mean age: 24.74 yrs Female: 70.3% | 4 weeks | Physical activity | Moderation | |
| Yes (0.033) | |||||
| Rhodes, 2021 [52] | 2-arm parallel randomized trial (groups collapsed)—T1, T2, T3, T4 | n = 254 Canadian adults who were new parents Mean age: 31.94 yrs Female: 50% | Baseline, 6 weeks, 12 weeks, 6 months | Physical activity | Moderation | |
| Yes (<0.01) | |||||
| Moderated Moderation | ||||||
| ||||||
| ○ Gender*Affective attitude | No | |||||
| ○ Gender*Perceived opportunity | Yes (<0.05) | |||||
| ○ Gender*Planning | No | |||||
| ○ Gender*Habit | No | |||||
| ○ Gender*Identity | No | |||||
| Schutz, 2011 [36] | Noncontrolled timeseries (pre-post)—T1, T2 | n = 237 HIV-positive men who have sex with men in Montreal, Canada Mean age: 42.5 yrs | 6 months | Condom use | Moderation | |
| Yes a | |||||
| No | |||||
| No | |||||
| No | |||||
| No | |||||
| No | |||||
| No | |||||
| No | |||||
| No | |||||
| Schüz, 2020 [54] | Study I. Cross-sectional survey | n = 1005 US adults Mean age: 33.6 yrs Female: 47.1% | No follow-up | 1. Fruit and vegetable consumption 2. Physical activity 3. Low-fat diet 4. Alcohol consumption 5. Flossing daily 6. Testicular or breast self-exams | Moderation | |
| ||||||
| ○ Education level (categorical multiple choice based on the US Census Current Population Survey and International Standard Classification of Education (ISCED)) | Yes (<0.05) | |||||
| ○ Income (categorical multiple choice) | No | |||||
| ○ Occupation status (percentage unemployment level matched to zip code based on American Community Survey; area-level SES measure) | No | |||||
| ○ Zip code (text entry; area-level SES measure) | No | |||||
| ○ Subjective SES (10-point ladder subjective SES scale) | No | |||||
| Study II. Noncontrolled timeseries (pre-post)—T1, T2 | n = 1273 International adults Mean age: 31.57 yrs Female: 50.5% | 4 weeks | 1. Fruit and vegetable consumption 2. Physical activity 3. Alcohol consumption 4. Flossing daily 5. Not sitting for extended periods 6. Healthy snack consumption | Moderation | ||
| ||||||
| ○ Education level (categorical multiple choice based on the US Census Current Population Survey and International Standard Classification of Education (ISCED)) | Yes (<0.01) | |||||
| ○ Income (categorical multiple choice) | No | |||||
| ○ Occupation status (personal employment) | No | |||||
| ○ Subjective SES (10-point ladder subjective SES scale) | Yes (<0.05) | |||||
| Stevens, 2017 [35] | Noncontrolled timeseries (pre-post)—T1, T2 | n = 77 US young adults Mean age: 20.8 yrs Female: 60.5% | 10 days | Alcohol consumption | Moderation | |
| ||||||
| ○ Lack of planning (59-item UPPS-P Impulsive Behavior Scale) | No | |||||
| ○ Lack of perseverance (59-item UPPS-P) | No | |||||
| ○ Negative urgency (59-item UPPS-P) | No | |||||
| ○ Positive urgency (59-item UPPS-P) | No | |||||
| ○ Sensation seeking (59-item UPPS-P) | No | |||||
| ○ Response inhibition (Go–Stop Impulsivity Paradigm) | No | |||||
| ○ Response initiation (Immediate memory Task (IMT)) | No | |||||
| ○ Delay discounting (27-item Monetary Choice Questionnaire (MCQ) and Two-Choice Impulsivity Paradigm (TCIP)) | No | |||||
| Wang, 2021 [32] | Cross-sectional survey | n = 334 US college students. Mean age: 21 yrs Female: 32.3% | No follow-up | Sports gambling | Moderation | |
| Yes (0.003) | |||||
| Zhang C.Q., 2020 [41] | Noncontrolled timeseries—T1, T2, T3 | n = 297 College students in China Mean age: not reported (range: 18-35 yrs) Female: 82.49% | 2 months | Hand washing and sleep hygiene | Moderation (intention—hand washing) | |
| Yes (<0.001) | |||||
| No | |||||
| No | |||||
| No | |||||
| Moderation (intention—sleep hygiene) | ||||||
| No | |||||
| No | |||||
| No | |||||
| No | |||||
| Zhang R., 2019 [39] | Noncontrolled timeseries (pre-post)—T1, T2 | n = 157 Office employees in China Mean age: 33.26 yrs Female: 64.97% | 1 month | Transport-related walking | Moderation | |
| No |
| (a) | ||||
|---|---|---|---|---|
| Behavior Category | Specific Behaviors Included in Category | n | ||
| Physical Activity | General physical activity, transport-related walking, and knee pain rehabilitation exercises | 17 | ||
| Diet | Fruit and vegetable consumption, snacking, low-fat diet, and gluten-free diet | 9 | ||
| Preventive Health Behaviors | Flossing, hand washing, social distancing, limited sitting, condom use, breast or testicular self-exam, and sun protection | 7 | ||
| Addiction | Alcohol use, illicit drug use, and sports gambling | 6 | ||
| Mental Health | Mindfulness meditation app, depression prevention strategies, and sleep hygiene | 3 | ||
| Medication Adherence | Aspirin adherence | 1 | ||
| (b) | ||||
| Type of Analysis | n | |||
| Statistically Significant | Not Statistically Significant | Total | ||
| Moderation | 19 | 11 | 30 | |
| Mediation | 5 | 0 | 5 | |
| Moderated Mediation | 4 | 0 | 4 | |
| Moderated Moderation | 3 | 0 | 3 | |
| (c) | ||||
| Moderator or Mediator Category | Moderator and Mediator Variables | n | ||
| Statistically Significant | Not Statistically Significant | Total | ||
| More Support | Impulsivity Moderation | 6 | 3 | 9 |
| Self-Efficacy Moderation | 4 | 1 | 5 | |
| Planning Mediation | 5 | 0 | 5 | |
| Planning*Self-Efficacy-Moderated Mediation | 3 | 0 | 3 | |
| Less Support | Personality Moderation | 2 | 5 | 7 |
| Socioeconomics Moderation | 4 | 0 | 4 | |
| Perceptions and Beliefs Moderation | 2 | 0 | 2 | |
| Environment Moderation | 1 | 1 | 2 | |
| Habit Moderation | 1 | 1 | 2 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hohmann, L.A.; Garza, K.B. The Moderating Power of Impulsivity: A Systematic Literature Review Examining the Theory of Planned Behavior. Pharmacy 2022, 10, 85. https://doi.org/10.3390/pharmacy10040085
Hohmann LA, Garza KB. The Moderating Power of Impulsivity: A Systematic Literature Review Examining the Theory of Planned Behavior. Pharmacy. 2022; 10(4):85. https://doi.org/10.3390/pharmacy10040085
Chicago/Turabian StyleHohmann, Lindsey A., and Kimberly B. Garza. 2022. "The Moderating Power of Impulsivity: A Systematic Literature Review Examining the Theory of Planned Behavior" Pharmacy 10, no. 4: 85. https://doi.org/10.3390/pharmacy10040085