2.5.1. Concentrations of BBE Compounds in Rat Plasma
The measured concentrations of betulin in plasma samples are depicted in
Figure 4. The peak betulin concentrations in all tested groups occurred at the 2 h time point. The highest concentrations of betulin in the plasma were observed following oral oleogel administration. In this group, the betulin plasma concentration reached 344 ng/mL, surpassing the betulin concentrations in the hydrogel group by at least 3 times. When compared to the BBE suspension in oil, oleogel administration resulted in a 6 times higher betulin concentration. This difference is attributed to the fact that the oleogel contains smaller BBE particles than the oil suspension, resulting in a larger surface area and, consequently, improved bioavailability [
11,
23,
38,
39,
40,
46].
The lowest peak concentration of betulin was observed in rat plasma following the administration of the BBE suspension in water, a concentration that was as much as 5-fold lower than in the oil suspension group. The disparity in the betulin concentration between the oleogel and the hydrogel, as well as between the BBE suspensions in oil and water, indicates that an oil-containing system enhances betulin uptake. The solubility of BBE in water is very low (0.25 µg/mL), while in sunflower oil, it is 17,000 times higher (4.4 mg/mL) [
47]. This stark contrast accounts for the improved bioavailability in the oil phase. Betulin concentrations in the oleogel half-dose group reached a peak concentration approximately half that of the full-dose oleogel (
Figure 4). Thus, we demonstrate that the bioavailability of botulin from the oleogel is dose-dependent within the tested dose range. On the last day of the 7-day daily administration, the peak betulin concentration was lower, and the pharmacokinetic (PK) profile exhibited substantial differences.
A previous study by Jager et al. on the pharmacokinetics of betulin after the administration of a BBE suspension in sesame oil showed a dose-independent maximum betulin level of 130 ng/mL 4 h after administration [
52]. In our study, after the administration of BBE in the oleogel, betulin reached a 3 times higher concentration in blood plasma than in the Jager et al. study. However, after the administration of the BBE oil suspension, a 2.5 times lower betulin concentration was observed at the same time point than in Jager et al.’s study. It should be noted that the studies used different strains of rats, which may produce different results [
53]. In Pozharitskaya’s investigation, the use of betulin nanoparticles at a dose 3 times lower (25.2 mg/kg) demonstrated significantly higher bioavailability results (15.5 µg/mL) in blood plasma compared to the data observed in our study using the oleogel. It should be noted that in Pozharitskaya’s research, betulin was administered through the endotracheal route, which notably enhances the bioavailability indicators, and the studies are not comparable. This finding is further supported by Pozharitskaya’s data, where directly injected betulin powder reached 6.9 µg/mL in blood plasma, which is almost 1000 times higher than in the case of the aqueous suspension of BBE powder in our study. Additionally, it is important to mention that Pozharitskaya’s study employed a distinct rat species and administered pure betulin instead of a mixture of extracts. In Pozharitskaya’s study, betulin nanoparticles increased the bioavailability by 2.5 times compared to betulin powder, but in our study, the oleogel system increased the bioavailability by 42 times compared to the powder suspension in water [
54]. In Zhao et al.’s study, they orally administered betulin nanoparticles obtained by the antisolvent precipitation method, and the peak plasma concentration of betulin was 6 µg/mL, which indicates a 20 times greater bioavailability than in our study. It should be noted that in the study by Zhao et al., pure betulin nanoparticles were administered instead of a BBE mixture [
11].
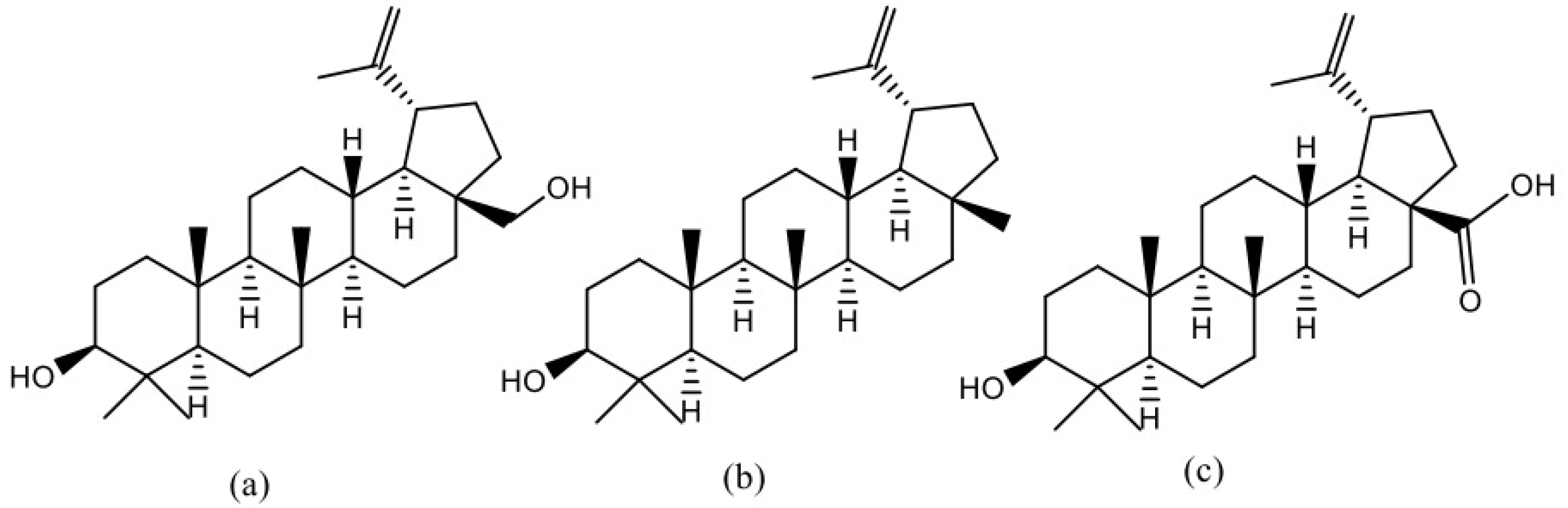
It is possible that, due to their structural similarity (
Figure 5), betulin, lupeol, and betulinic acid may compete among themselves for the absorption processes, similar to the case for the solubility balance [
43].
When comparing the total betulin exposure based on the AUC (area under the curve) across various BBE-containing dispersed systems, the highest betulin exposure was observed in the oleogel group rats, exceeding hydrogel exposure by 2.6-fold (
Figure 6). This discrepancy is attributed to the superior solubility of BBE in oil compared to water [
43,
47]. Furthermore, betulin exposure in the oleogel group was 5-fold higher than in the oil suspension, while its exposure in the hydrogel group was 16-fold higher than in the water suspension group. This can be explained by the smaller particle sizes in oleogel and hydrogel dispersion systems [
40]. The oleogel at a half dose reached 2.8-fold lower betulin exposure than the full-dose oleogel after a single administration (
Figure 6).
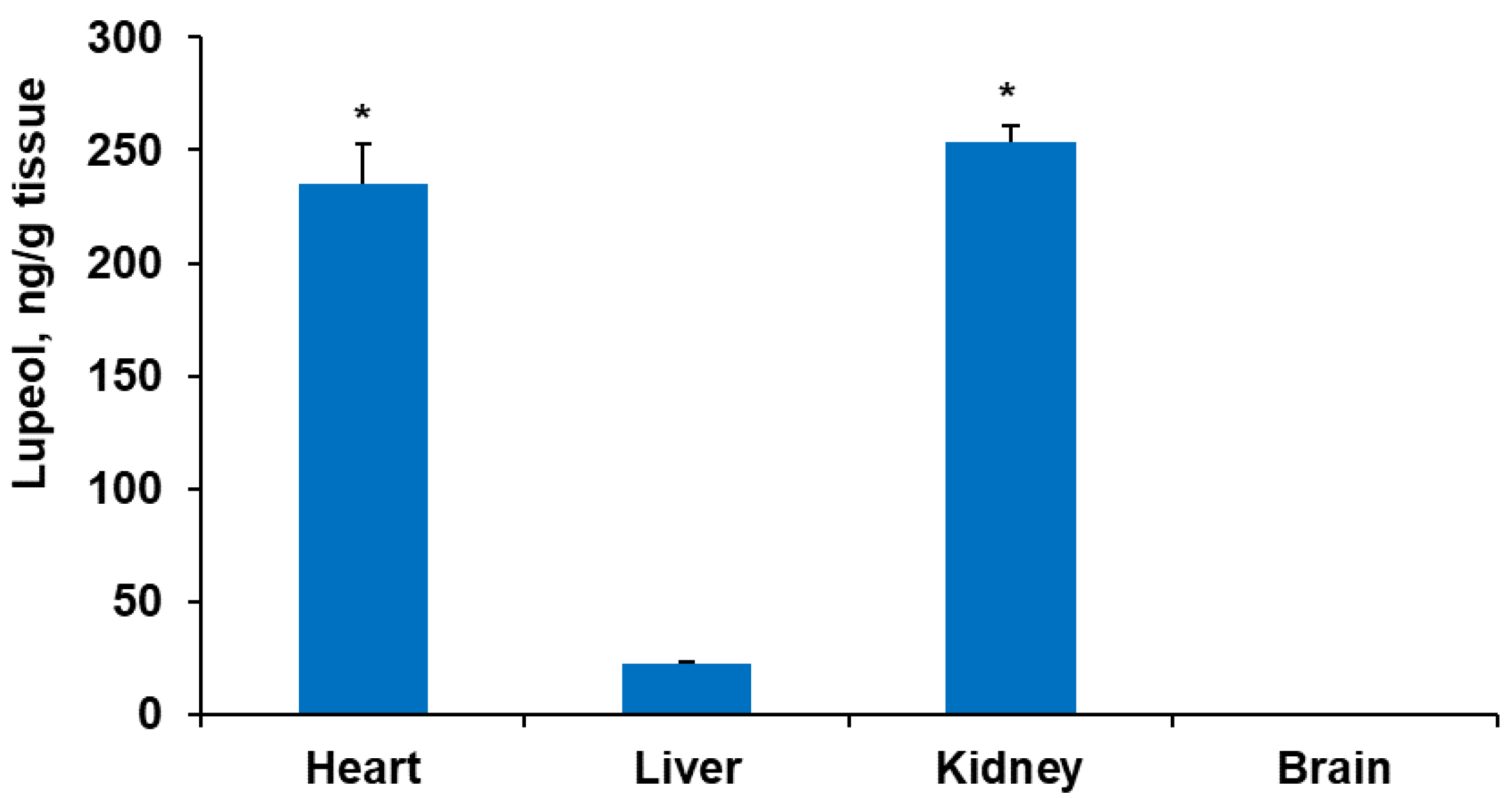
The measured concentrations of lupeol in plasma samples are shown in
Figure 7. The peak lupeol concentrations in all tested groups, except the water suspension, were at a 4 h time point. The highest plasma concentrations of lupeol were measured after oleogel administration. In this group, the lupeol plasma concentration reached 610 mg/mL, which exceeded the lupeol concentrations in all other groups but not by the same margin as betulin. Thus, the peak lupeol plasma concentration in the hydrogel group was only 20% lower than in the oleogel group. However, in comparison to the BBE suspension in oil, oleogel administration induced an 8 times higher lupeol concentration. Similar to betulin, the lowest peak concentration of lupeol was found in rat plasma after the administration of the BBE suspension in water, which was as much as 50-fold lower than in the oleogel group.
Peak lupeol concentrations in both measurements after the first and last administrations in the oleogel half-dose group were comparable, and approximately half of the lupeol plasma concentration was achieved after the administration of the oleogel at a full dose (
Figure 7). This implies that the bioavailability of lupeol is dose-dependent within the tested dose range. Nevertheless, on the last day of seven administrations, the peak lupeol concentration was slightly lower, and the PK profile exhibited differences. Similar to the betulin PK profile, the lupeol profile also indicates a slower but longer uptake of BBE compounds (
Figure 5 and
Figure 7).
Similar results were achieved in a study by Priyanka et al., where a 5 times higher dose of orally administered lupeol solid lipid nanoparticles reached 696 ng/mL of lupeol in the rat blood plasma [
46]. The results of our study demonstrate that the oleogel achieves a 4 times higher bioavailability of lupeol than what was observed in Priyanka et al.’s research. In the investigation conducted by Cháirez-Ramírez et al. [
45], lupeol was orally administered in olive oil at a concentration that was 20 times higher (200 mg/kg) than in our study. Nevertheless, our findings revealed only a 10-fold lower lupeol concentration in blood plasma (600 ng/mL) compared to the Cháirez-Ramírez study (6 ng/µL) [
45]. Hence, the oleogel formulation resulted in a two-fold increase in the bioavailability of lupeol, as compared to the findings of Cháirez-Ramírez et al.’s study [
45]. It is essential to note that the experimental protocol of Cháirez-Ramírez et al.’s research involved orally administering pure lupeol to mice, which may hinder direct comparisons with our study using rats [
45]. Considering the similarities between lupeol and betulin, it is possible that they may influence bioavailability, similar to the solubility balance. In general, lupeol demonstrates significantly better bioavailability than betulin, partly due to its superior solubility in both water and oil compared to betulin and betulinic acid [
43,
45,
47,
52].
The assessment of total lupeol exposure (AUC) in different dispersed BBE systems exhibited superior lupeol exposure in the oleogel group rats, registering 40% lower bioavailability results than in the study conducted by Priyanka et al [
46]. However, it should be noted that the Priyanka et al. study employed a 5 times higher dose of lupeol than was used in our study [
46]. This indicates that the oleogel can be considered the most effective formulation in terms of lupeol bioavailability. These data are summarized in
Figure 8. Oleogel exposure exceeded hydrogel exposure by 42%. Lupeol exposure in the oleogel group was 5- and 80-fold higher than exposure in the oil suspension and water suspension groups, respectively. The oleogel at a half dose after a single administration reached exactly 2-fold lower lupeol exposure than in the oleogel full-dose group. Exposure after seven administrations was 1.5-fold higher than after a single administration of half a dose.
Lupeol exposure was about 3 times higher than betulin exposure. Considering the lower dose of lupeol, its bioavailability from the oleogel is 20 times better than betulin bioavailability. Betulinic acid content in rat blood plasma was not detected or was below the limit of quantification for all BBE-containing dispersion systems at all time points. This indicates the low bioavailability of betulinic acid, but it should be noted that the administered dose of betulinic acid was 3 times lower than that of lupeol and 26 times lower than that of betulin. Taking into account that the dose of lupeol is only 3 times higher than that of betulinic acid, but the detection limit is 5 ng/mL for betulinic acid and 10 ng/mL for lupeol, it can be concluded that betulinic acid has the lowest bioavailability if the substances (betulin, lupeol, and betulinic acid) are administered at the same time; otherwise, even at such a low dose, we could assess betulinic acid in blood plasma. Veber et al.’s research supports that a decrease in polar surface area exhibits a positive correlation with an increase in the permeation rate, instead of lipophilicity, and that lower molecular weight is associated with higher oral bioavailability [
55].
Additionally, their study demonstrates that oral bioavailability is further linked to lower rotatable bond counts, lower hydrogen bond counts, and lower polar surface area. Based on this information, it is reasonable to conclude that the polar surface area of a compound plays a crucial role in determining its bioavailability [
55]. For instance, the polar surface areas of lupeol, betulin, and betulinic acid are approximately 20, 40, and 60 A
2, respectively, and their molecular weights are 426, 442, and 457, respectively. This likely influenced the bioavailability of lupeol in our tests and explains the low bioavailability of betulinic acid.


 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}