
Non-Uniform Bioaccumulation of Lead and Arsenic in Two Remote Regions of the Human Heart’s Left Ventricle: A Post-Mortem Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection
2.2. Inductively Coupled Plasma Mass Spectrometry (ICP-MS) Measurement
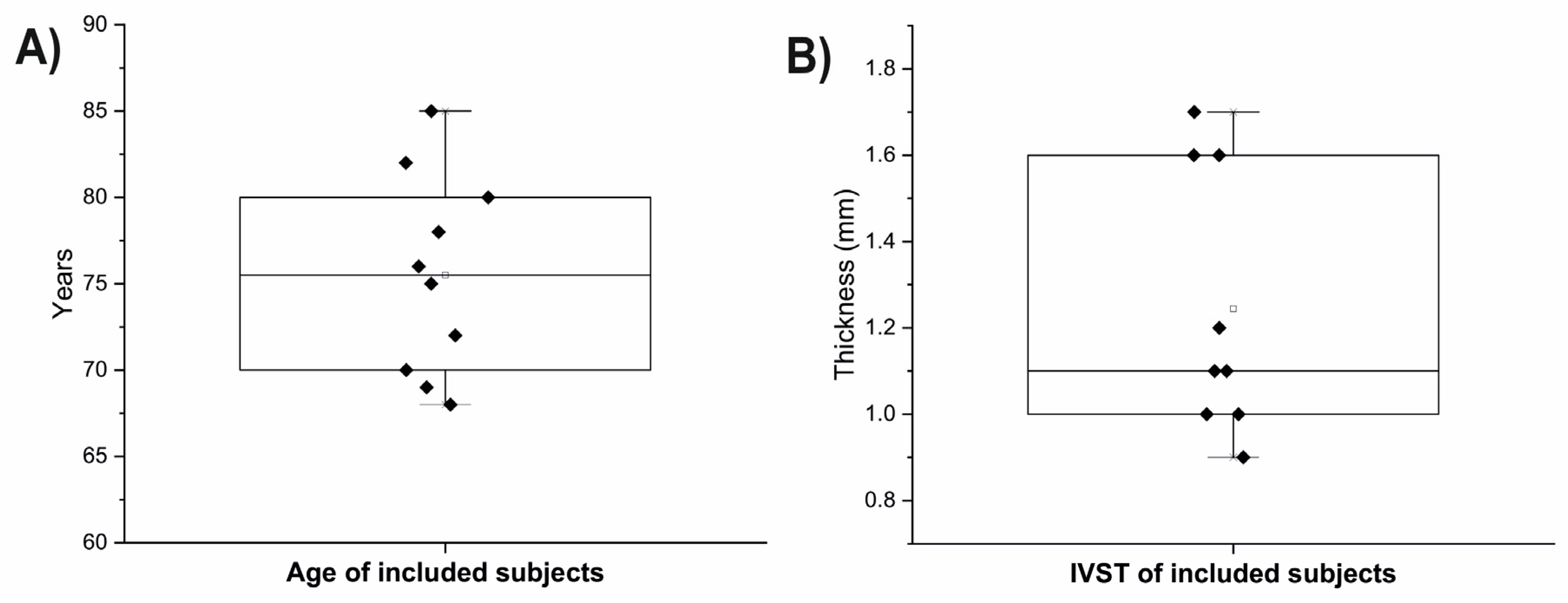
2.3. Measurement of LV Wall Thickness
2.4. Statistical Analysis
3. Results
Correlations between an Age and IVST with Metals Concentrations
4. Discussion
4.1. Arsenic and Lead-Induced Cardiotoxicity
4.2. Suggestions for a Future Measurements
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, C.; Shi, L.; Peng, C.; Yu, G.; Zhang, Y.; Du, Z. Lead-induced cardiomyocytes apoptosis by inhibiting gap junction intercellular communication via autophagy activation. Chem.-Biol. Interact. 2021, 337, 109331. [Google Scholar] [CrossRef]
- Wang, Q.; Ma, Y.; Li, Y.; He, Z.; Feng, B. Lead-induced cardiomyocytes apoptosis by inhibiting gap junction intercellular communication via modulating the PKCα/Cx43 signaling pathway. Chem. Biol. Interact. 2023, 376, 110451. [Google Scholar] [CrossRef] [PubMed]
- Barry, P.; Mossman, D. Lead concentrations in human tissues. Occup. Environ. Med. 1970, 27, 339–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egger, A.E.; Grabmann, G.; Gollmann-Tepeköylü, C.; Pechriggl, E.J.; Artner, C.; Türkcan, A.; Hartinger, C.G.; Fritsch, H.; Keppler, B.K.; Brenner, E. Chemical imaging and assessment of cadmium distribution in the human body. Metallomics 2019, 11, 2010–2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maduabuchi, J.-M.; Nzegwu, C.; Adigba, E.; Aloke, R.; Ezomike, C.; Okocha, C.; Obi, E.; Orisakwe, O. Lead and cadmium exposures from canned and non-canned beverages in Nigeria: A public health concern. Sci. Total Environ. 2006, 366, 621–626. [Google Scholar] [CrossRef]
- Huang, X.; Zhao, B.; Wu, Y.; Tan, M.; Shen, L.; Feng, G.; Yang, X.; Chen, S.; Xiong, Y.; Zhang, E. The lead and cadmium content in rice and risk to human health in China: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0278686. [Google Scholar] [CrossRef]
- Repić, A.; Bulat, P.; Antonijević, B.; Antunović, M.; Džudović, J.; Buha, A.; Bulat, Z. The influence of smoking habits on cadmium and lead blood levels in the Serbian adult people. Environ. Sci. Pollut. Res. 2020, 27, 751–760. [Google Scholar] [CrossRef]
- Shakeri, M.T.; Nezami, H.; Nakhaee, S.; Aaseth, J.; Mehrpour, O. Assessing heavy metal burden among cigarette smokers and non-smoking individuals in Iran: Cluster analysis and principal component analysis. Biol. Trace Elem. Res. 2021, 199, 4036–4044. [Google Scholar] [CrossRef]
- Borné, Y.; Barregard, L.; Persson, M.; Hedblad, B.; Fagerberg, B.; Engström, G. Cadmium exposure and incidence of heart failure and atrial fibrillation: A population-based prospective cohort study. BMJ Open 2015, 5, e007366. [Google Scholar] [CrossRef]
- Wade, T.J.; Xia, Y.; Mumford, J.; Wu, K.; Le, X.C.; Sams, E.; Sanders, W.E. Cardiovascular disease and arsenic exposure in Inner Mongolia, China: A case control study. Environ. Health 2015, 14, 35. [Google Scholar] [CrossRef] [Green Version]
- Ali, S.; Awan, Z.; Mumtaz, S.; Shakir, H.A.; Ahmad, F.; Ulhaq, M.; Tahir, H.M.; Awan, M.S.; Sharif, S.; Irfan, M. Cardiac toxicity of heavy metals (cadmium and mercury) and pharmacological intervention by vitamin C in rabbits. Environ. Sci. Pollut. Res. 2020, 27, 29266–29279. [Google Scholar] [CrossRef]
- Gammella, E.; Recalcati, S.; Rybinska, I.; Buratti, P.; Cairo, G. Iron-induced damage in cardiomyopathy: Oxidative-dependent and independent mechanisms. Oxid. Med. Cell. Longev. 2015, 2015, 230182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, M.; Cheng, Z.-W.; Huang, C.-G.; Ye, Z.-Q.; Sun, L.-J.; Chen, H.; Fu, B.-B.; Zhou, K.; Fang, Z.-R.; Wang, Z.-J. Long-term exposure to copper induces mitochondria-mediated apoptosis in mouse hearts. Ecotoxicol. Environ. Saf. 2022, 234, 113329. [Google Scholar] [CrossRef]
- Jarosz, M.; Olbert, M.; Wyszogrodzka, G.; Młyniec, K.; Librowski, T. Antioxidant and anti-inflammatory effects of zinc. Zinc-dependent NF-κB signaling. Inflammopharmacology 2017, 25, 11–24. [Google Scholar] [CrossRef] [Green Version]
- Pichler, G.; Grau-Perez, M.; Tellez-Plaza, M.; Umans, J.; Best, L.; Cole, S.; Goessler, W.; Francesconi, K.; Newman, J.; Redon, J.; et al. Association of Arsenic Exposure with Cardiac Geometry and Left Ventricular Function in Young Adults. Circ. Cardiovasc. Imaging 2019, 12, e009018. [Google Scholar] [CrossRef]
- Cirovic, A.; Denic, A.; Clarke, B.L.; Vassallo, R.; Cirovic, A.; Landry, G.M. A hypoxia-driven occurrence of chronic kidney disease and osteoporosis in COPD individuals: New insights into environmental cadmium exposure. Toxicology 2022, 482, 153355. [Google Scholar] [CrossRef]
- Qian, Z.M.; Mei Wu, X.; Fan, M.; Yang, L.; Du, F.; Yung, W.H.; Ke, Y. Divalent metal transporter 1 is a hypoxia-inducible gene. J. Cell. Physiol. 2011, 226, 1596–1603. [Google Scholar] [CrossRef]
- Bal, W.; Sokołowska, M.; Kurowska, E.; Faller, P. Binding of transition metal ions to albumin: Sites, affinities and rates. Biochim. Biophys. Acta 2013, 1830, 5444–5455. [Google Scholar] [CrossRef] [PubMed]
- Saljooghi, A.S.; Fatemi, S. Cadmium transport in blood serum. Toxicol. Ind. Health 2010, 26, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Limaye, D.A.; Shaikh, Z.A. Cytotoxicity of cadmium and characteristics of its transport in cardiomyocytes. Toxicol. Appl. Pharmacol. 1999, 154, 59–66. [Google Scholar] [CrossRef]
- He, S.; Zhuo, L.; Cao, Y.; Liu, G.; Zhao, H.; Song, R.; Liu, Z. Effect of cadmium on osteoclast differentiation during bone injury in female mice. Environ. Toxicol. 2020, 35, 487–494. [Google Scholar] [CrossRef]
- Makevic, V.; Milovanovich, I.D.; Popovac, N.; Janković, S.; Janković, V.; Stefanović, S.; Bukumiric, Z.; de Luka, S.R. Oligoelements in serum and intestinal tissue of pediatric IBD patients. J. Trace Elem. Med. Biol. 2023, 79, 127239. [Google Scholar] [CrossRef]
- Juloski, J.T.; Rakic, A.; Ćuk, V.V.; Ćuk, V.M.; Stefanović, S.; Nikolić, D.; Janković, S.; Trbovich, A.M.; De Luka, S.R. Colorectal cancer and trace elements alteration. J. Trace Elem. Med. Biol. 2020, 59, 126451. [Google Scholar] [CrossRef] [PubMed]
- Moon, K.; Guallar, E.; Navas-Acien, A. Arsenic exposure and cardiovascular disease: An updated systematic review. Curr. Atheroscler. Rep. 2012, 14, 542–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karachaliou, C.; Sgourou, A.; Kakkos, S.; Kalavrouziotis, I. Arsenic exposure promotes the emergence of cardiovascular diseases. Rev. Environ. Health 2022, 37, 467–486. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Li, A.; Mei, Y.; Zhou, Q.; Li, Y.; Li, K.; Xu, Q. The association of arsenic exposure with hypertension and blood pressure: A systematic review and dose-response meta-analysis. Environ. Pollut. 2021, 289, 117914. [Google Scholar] [CrossRef] [PubMed]
- Manna, P.; Sinha, M.; Sil, P.C. Arsenic-induced oxidative myocardial injury: Protective role of arjunolic acid. Arch. Toxicol. 2008, 82, 137–149. [Google Scholar] [CrossRef]
- Adil, M.; Kandhare, A.D.; Ghosh, P.; Bodhankar, S.L. Sodium arsenite-induced myocardial bruise in rats: Ameliorative effect of naringin via TGF-β/Smad and Nrf/HO pathways. Chem. Biol. Interact. 2016, 253, 66–77. [Google Scholar] [CrossRef]
- Zhao, Z.; Li, J.; Zheng, B.; Liang, Y.; Shi, J.; Zhang, J.; Han, X.; Chu, L.; Chu, X.; Gao, Y. Ameliorative effects and mechanism of crocetin in arsenic trioxide-induced cardiotoxicity in rats. Mol. Med. Rep. 2020, 22, 5271–5281. [Google Scholar] [CrossRef]
- Pamphlett, R. The prevalence of inorganic mercury in human cells increases during aging but decreases in the very old. Sci. Rep. 2021, 11, 16714. [Google Scholar] [CrossRef]
- Klinova, S.V.; Minigalieva, I.A.; Protsenko, Y.L.; Sutunkova, M.P.; Gurvich, V.B.; Ryabova, J.V.; Valamina, I.E.; Gerzen, O.P.; Nabiev, S.R.; Balakin, A.A. Changes in the Cardiotoxic Effects of Lead Intoxication in Rats Induced by Muscular Exercise. Int. J. Mol. Sci. 2022, 23, 4417. [Google Scholar] [CrossRef] [PubMed]
- Gerzen, O.P.; Nabiev, S.R.; Klinova, S.V.; Minigalieva, I.A.; Sutunkova, M.P.; Katsnelson, B.A.; Nikitina, L.V. Molecular mechanisms of mechanical function changes of the rat myocardium under subchronic lead exposure. Food Chem. Toxicol. 2022, 169, 113444. [Google Scholar] [CrossRef] [PubMed]
- Becker, J.S.; Breuer, U.; Hsieh, H.-F.; Osterholt, T.; Kumtabtim, U.; Wu, B.; Matusch, A.; Caruso, J.A.; Qin, Z. Bioimaging of metals and biomolecules in mouse heart by laser ablation inductively coupled plasma mass spectrometry and secondary ion mass spectrometry. Anal. Chem. 2010, 82, 9528–9533. [Google Scholar] [CrossRef] [PubMed]
- Sabine Becker, J. Imaging of metals in biological tissue by laser ablation inductively coupled plasma mass spectrometry (LA–ICP–MS): State of the art and future developments. J. Mass Spectrom. 2013, 48, 255–268. [Google Scholar] [CrossRef]
- Urgast, D.S.; Ou, O.; Gordon, M.-J.; Raab, A.; Nixon, G.F.; Kwun, I.-S.; Beattie, J.H.; Feldmann, J. Microanalytical isotope ratio measurements and elemental mapping using laser ablation ICP-MS for tissue thin sections: Zinc tracer studies in rats. Anal. Bioanal. Chem. 2012, 402, 287–297. [Google Scholar] [CrossRef]
- Saltzman, B.E.; Gross, S.B.; Yeager, D.W.; Meiners, B.G.; Gartside, P.S. Total body burdens and tissue concentrations of lead, cadmium, copper, zinc, and ash in 55 human cadavers. Environ. Res. 1990, 52, 126–145. [Google Scholar] [CrossRef]
- Mallah, E.; Rayyan, W.A.; Dayyih, W.A.; Al-Majali, I.S.; Qaralleh, H.; Al-Thunibat, O.Y. Analytical and Comparative Study about the Impact of Lead Homeostasis on Cardiovascular Disorders in Humans. Biomed. Pharmacol. J. 2018, 11, 277–284. [Google Scholar] [CrossRef]
- Rahil-Khazen, R.; Bolann, B.J.; Myking, A.; Ulvik, R.J. Multi-element analysis of trace element levels in human autopsy tissues by using inductively coupled atomic emission spectrometry technique (ICP-AES). J. Trace Elem. Med. Biol. 2002, 16, 15–25. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Elements | Range | LOD | LOQ | RSDr | Recovery |
|---|---|---|---|---|---|
| µg kg−1 | µg kg−1 | µg kg−1 | % | % | |
| 75As | 4–100 | 1.2 | 4 | 6.57 | 95.3 |
| 111Cd | 1–100 | 0.4 | 1 | 8.99 | 100.4 |
| 207Pb | 4–100 | 2 | 3.8 | 6.65 | 101.1 |
| 202Hg | 1–100 | 0.3 | 0.9 | 6.90 | 96.0 |
| mg kg−1 | mg kg−1 | mg kg−1 | % | % | |
| 63Cu | 1–50 | 0.022 | 0.066 | 6.26 | 101.7 |
| 57Fe | 5–300 | 0.08 | 0.23 | 4.71 | 96.6 |
| 66Zn | 2–100 | 0.124 | 0.372 | 10.52 | 95.6 |
| 55Mn | 0.1–5 | 0.004 | 0.011 | 4.47 | 102.0 |
| 60Ni | 0.1–5 | 0.050 | 0.145 | 9.19 | 102.4 |
| 44Ca | 10–500 | 3.08 | 9.24 | 3.64 | 99.6 |
| 24Mg | 10–500 | 0.13 | 0.40 | 3.03 | 98.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cirovic, A.; Orisakwe, O.E.; Cirovic, A.; Jevtic, J.; Tasic, D.; Tasic, N. Non-Uniform Bioaccumulation of Lead and Arsenic in Two Remote Regions of the Human Heart’s Left Ventricle: A Post-Mortem Study. Biomolecules 2023, 13, 1232. https://doi.org/10.3390/biom13081232
Cirovic A, Orisakwe OE, Cirovic A, Jevtic J, Tasic D, Tasic N. Non-Uniform Bioaccumulation of Lead and Arsenic in Two Remote Regions of the Human Heart’s Left Ventricle: A Post-Mortem Study. Biomolecules. 2023; 13(8):1232. https://doi.org/10.3390/biom13081232
Chicago/Turabian StyleCirovic, Ana, Orish E. Orisakwe, Aleksandar Cirovic, Jovan Jevtic, Danijela Tasic, and Nebojsa Tasic. 2023. "Non-Uniform Bioaccumulation of Lead and Arsenic in Two Remote Regions of the Human Heart’s Left Ventricle: A Post-Mortem Study" Biomolecules 13, no. 8: 1232. https://doi.org/10.3390/biom13081232