

Association of Long Noncoding RNA Expression Signatures with Stress-Induced Myocardial Perfusion Defects
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Dipyridamole-Thallium-201 Scintigraphy and SPECT Myocardial Perfusion Imaging
2.3. Coronary Angiography
2.4. RNA Extraction and Quantitative Real-Time Polymerase Chain Reaction
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Study Participants
3.2. Expression Profile of lncRNAs and Related Downstream Genes in Healthy Controls and Patients with Positive Thallium Stress Test but without Significant Coronary Artery Stenosis
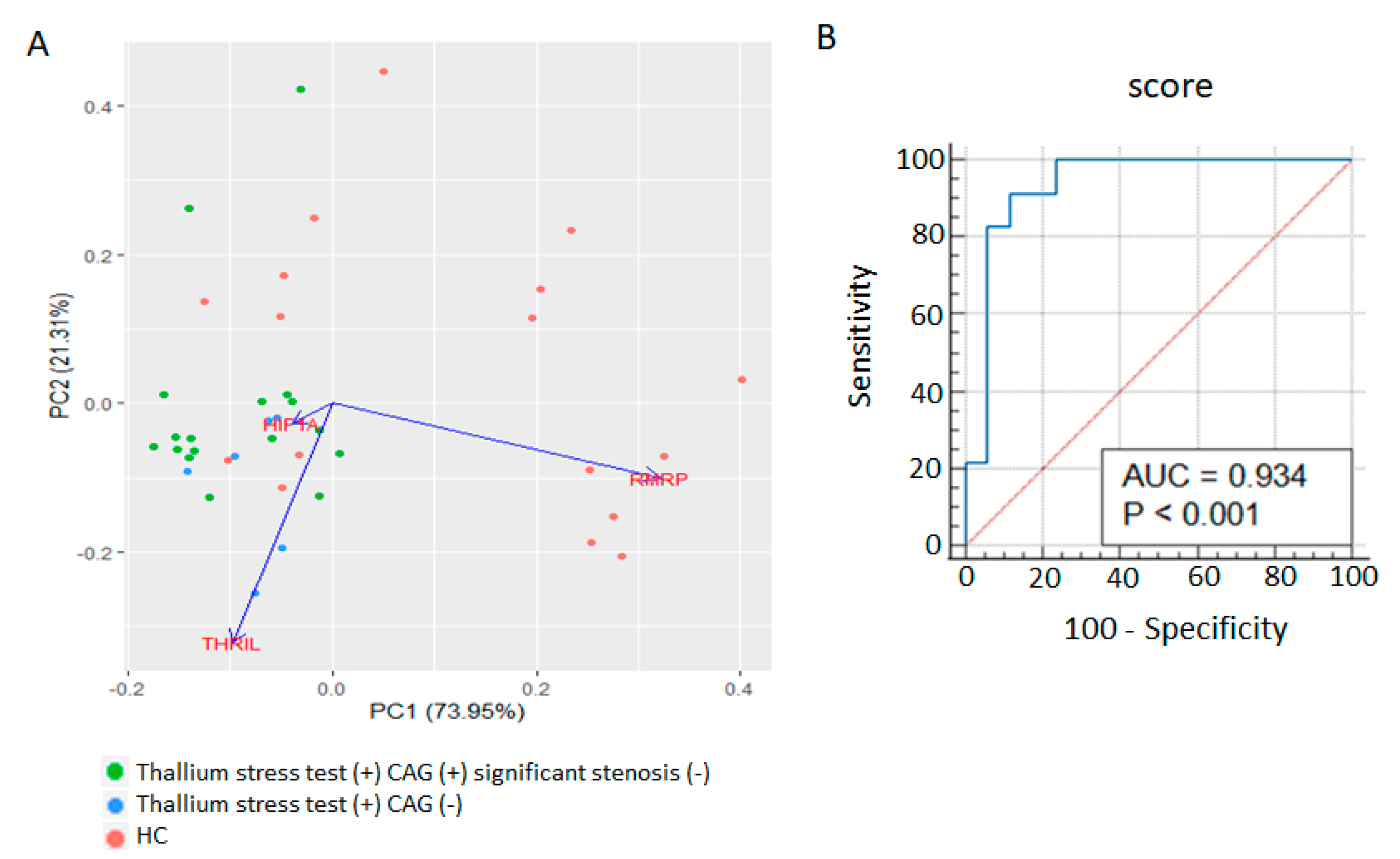
3.3. Whole Blood RMRP, THRIL, and HIF1A Expression Signatures as Diagnostic Markers for Positive Thallium Stress Test without Significant Coronary Artery Stenosis
3.4. Associations of Whole Blood RMRP, THRIL, and HIF1A Expression Levels with SSS and Cholesterol Ratio
3.5. Mixed lncRNA and mRNA Expression Scores for Predicting Further CAG in Patients with Significant Stress-Induced Myocardial Perfusion Defects
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Czaja, M.; Wygoda, Z.; Duszanska, A.; Szczerba, D.; Glowacki, J.; Gasior, M.; Wasilewski, J.P. Interpreting myocardial perfusion scintigraphy using single-photon emission computed tomography. Part 1. Kardiochir. Torakochirurgia Pol. 2017, 14, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Nakata, T.; Hashimoto, A.; Matsuki, T.; Yoshinaga, K.; Tsukamoto, K.; Tamaki, N. Prognostic value of automated SPECT scoring system for coronary artery disease in stress myocardial perfusion and fatty acid metabolism imaging. Int. J. Cardiovasc. Imaging 2013, 29, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Peix, A.; Batista, E.; Cabrera, L.O.; Rodriguez, L.; Padron, K.; Sainz, B.; Mendoza, V.; Carrillo, R.; Fernandez, Y.; Mena, E.; et al. Gated-SPECT myocardial perfusion imaging and coronary calcium score for evaluation of patients with acute chest pain and a normal or nondiagnostic electrocardiogram. Coron. Artery Dis. 2012, 23, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Trpkov, C.; Savtchenko, A.; Liang, Z.; Feng, P.; Southern, D.A.; Wilton, S.B.; James, M.T.; Feil, E.; Mylonas, I.; Miller, R.J.H. Visually estimated coronary artery calcium score improves SPECT-MPI risk stratification. Int. J. Cardiol. Heart Vasc. 2021, 35, 100827. [Google Scholar] [CrossRef]
- Wackers, F.J.; Lie, K.I.; Liem, K.L.; Sokole, E.B.; Samson, G.; van der Schoot, J.B.; Durrer, D. Thallium-201 scintigraphy in unstable angina pectoris. Circulation 1978, 57, 738–742. [Google Scholar] [CrossRef]
- Desmarais, R.L.; Kaul, S.; Watson, D.D.; Beller, G.A. Do false positive thallium-201 scans lead to unnecessary catheterization? Outcome of patients with perfusion defects on quantitative planar thallium-201 scintigraphy. J. Am. Coll. Cardiol. 1993, 21, 1058–1063. [Google Scholar] [CrossRef]
- Von Dohlen, T.W.; Prisant, L.M.; Frank, M.J. Significance of positive or negative thallium-201 scintigraphy in hypertrophic cardiomyopathy. Am. J. Cardiol. 1989, 64, 498–503. [Google Scholar] [CrossRef]
- Zerbo, S.; Lanzarone, A.; Raimondi, M.; Martino, L.; Malta, G.; Cappello, F.; Argo, A. Myocardial bridge pathology and preventable accidents during physical activity of healthy subjects: A case report and a literature review. Med. Leg. J. 2020, 88, 209–214. [Google Scholar] [CrossRef]
- Mehta, P.K.; Quesada, O.; Al-Badri, A.; Fleg, J.L.; Volgman, A.S.; Pepine, C.J.; Merz, C.N.B.; Shaw, L.J. Ischemia and no obstructive coronary arteries in patients with stable ischemic heart disease. Int. J. Cardiol. 2022, 348, 1–8. [Google Scholar] [CrossRef]
- Ang, D.T.Y.; Berry, C.; Kaski, J.C. Phenotype-based management of coronary microvascular dysfunction. J. Nucl. Cardiol. 2022, 29, 3332–3340. [Google Scholar] [CrossRef]
- Fredman, G.; MacNamara, K.C. Atherosclerosis is a major human killer and non-resolving inflammation is a prime suspect. Cardiovasc. Res. 2021, 117, 2563–2574. [Google Scholar] [CrossRef]
- Marin, W.; Marin, D.; Ao, X.; Liu, Y. Mitochondria as a therapeutic target for cardiac ischemia-reperfusion injury (Review). Int. J. Mol. Med. 2021, 47, 485–499. [Google Scholar] [CrossRef]
- Fuschi, P.; Maimone, B.; Gaetano, C.; Martelli, F. Noncoding RNAs in the Vascular System Response to Oxidative Stress. Antioxid. Redox Signal. 2019, 30, 992–1010. [Google Scholar] [CrossRef]
- Simion, V.; Haemmig, S.; Feinberg, M.W. LncRNAs in vascular biology and disease. Vascul. Pharmacol. 2019, 114, 145–156. [Google Scholar] [CrossRef]
- Chen, Y.G.; Satpathy, A.T.; Chang, H.Y. Gene regulation in the immune system by long noncoding RNAs. Nat. Immunol. 2017, 18, 962–972. [Google Scholar] [CrossRef]
- Michalik, K.M.; You, X.; Manavski, Y.; Doddaballapur, A.; Zornig, M.; Braun, T.; John, D.; Ponomareva, Y.; Chen, W.; Uchida, S.; et al. Long noncoding RNA MALAT1 regulates endothelial cell function and vessel growth. Circ. Res. 2014, 114, 1389–1397. [Google Scholar] [CrossRef]
- Zhu, Y.; Yang, T.; Duan, J.; Mu, N.; Zhang, T. MALAT1/miR-15b-5p/MAPK1 mediates endothelial progenitor cells autophagy and affects coronary atherosclerotic heart disease via mTOR signaling pathway. Aging 2019, 11, 1089–1109. [Google Scholar] [CrossRef]
- Fasolo, F.; Jin, H.; Winski, G.; Chernogubova, E.; Pauli, J.; Winter, H.; Li, D.Y.; Glukha, N.; Bauer, S.; Metschl, S.; et al. Long Noncoding RNA MIAT Controls Advanced Atherosclerotic Lesion Formation and Plaque Destabilization. Circulation 2021, 144, 1567–1583. [Google Scholar] [CrossRef]
- Teng, Y.; Ding, M.; Wang, X.; Li, H.; Guo, Q.; Yan, J.; Gao, L. LncRNA RMRP accelerates hypoxia-induced injury by targeting miR-214-5p in H9c2 cells. J. Pharmacol. Sci. 2020, 142, 69–78. [Google Scholar] [CrossRef]
- An, J.H.; Chen, Z.Y.; Ma, Q.L.; Li, Y.B.; Shi, F.W. Liraglutide improves atherosclerosis by regulating long non-coding RNA RMRP/miR-128-1-5P/Gadd45g axis. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 2725–2737. [Google Scholar] [CrossRef]
- Song, X.; Gao, F.; Li, H.; Qin, W.; Chai, C.; Shi, G.; Yang, H. Long noncoding RNA THRIL promotes foam cell formation and inflammation in macrophages. Cell. Biol. Int. 2023, 47, 156–166. [Google Scholar] [CrossRef] [PubMed]
- Qi, H.; Shen, J.; Zhou, W. Up-regulation of long non-coding RNA THRIL in coronary heart disease: Prediction for disease risk, correlation with inflammation, coronary artery stenosis, and major adverse cardiovascular events. J. Clin. Lab. Anal. 2020, 34, e23196. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.A.; Li, J.P.; Yen, J.C.; Lai, I.L.; Ho, Y.C.; Chen, Y.C.; Lan, J.L.; Chang, J.G. lncRNA NTT/PBOV1 Axis Promotes Monocyte Differentiation and Is Elevated in Rheumatoid Arthritis. Int. J. Mol. Sci. 2018, 19, 2806. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.A.; Bauer, S.; Ho, Y.C.; Sotzny, F.; Chang, J.G.; Scheibenbogen, C. The expression signature of very long non-coding RNA in myalgic encephalomyelitis/chronic fatigue syndrome. J. Transl. Med. 2018, 16, 231. [Google Scholar] [CrossRef]
- Yang, C.A.; Chen, P.K.; Lan, J.L.; Chang, C.K.; Chang, J.G.; Chang, S.H.; Lin, C.C.; Chen, D.Y. Expression signature of inflammation-associated long non-coding RNAs in adult-onset Still’s disease. Clin. Exp. Rheumatol. 2021, 39 (Suppl. S132), 67–74. [Google Scholar] [CrossRef]
- Farid, I.; Litaker, D.; Tetzlaff, J.E. Implementing ACC/AHA guidelines for the preoperative management of patients with coronary artery disease scheduled for noncardiac surgery: Effect on perioperative outcome. J. Clin. Anesth. 2002, 14, 126–128. [Google Scholar] [CrossRef]
- Varasteh, Z.; Weber, W.A.; Rischpler, C. Nuclear Molecular Imaging of Cardiac Remodeling after Myocardial Infarction. Pharmaceuticals 2022, 15, 183. [Google Scholar] [CrossRef]
- Gimelli, A.; Liga, R.; Clemente, A.; Marras, G.; Kusch, A.; Marzullo, P. Left ventricular eccentricity index measured with SPECT myocardial perfusion imaging: An additional parameter of adverse cardiac remodeling. J. Nucl. Cardiol. 2020, 27, 71–79. [Google Scholar] [CrossRef]
- Shirani, J.; Dilsizian, V. Molecular imaging targets of cardiac remodeling. Curr. Cardiol. Rep. 2009, 11, 148–154. [Google Scholar] [CrossRef]
- Zhou, H.; Wang, B.; Yang, Y.X.; Jia, Q.J.; Zhang, A.; Qi, Z.W.; Zhang, J.P. Long Noncoding RNAs in Pathological Cardiac Remodeling: A Review of the Update Literature. Biomed. Res. Int. 2019, 2019, 7159592. [Google Scholar] [CrossRef]
- Zheng, J.; Chen, P.; Zhong, J.; Cheng, Y.; Chen, H.; He, Y.; Chen, C. HIF-1alpha in myocardial ischemia-reperfusion injury (Review). Mol. Med. Rep. 2021, 23, 352. [Google Scholar] [CrossRef]
- Eckle, T.; Kohler, D.; Lehmann, R.; El Kasmi, K.; Eltzschig, H.K. Hypoxia-inducible factor-1 is central to cardioprotection: A new paradigm for ischemic preconditioning. Circulation 2008, 118, 166–175. [Google Scholar] [CrossRef]
- Han, Y.; Cai, Y.; Lai, X.; Wang, Z.; Wei, S.; Tan, K.; Xu, M.; Xie, H. lncRNA RMRP Prevents Mitochondrial Dysfunction and Cardiomyocyte Apoptosis via the miR-1-5p/hsp70 Axis in LPS-Induced Sepsis Mice. Inflammation 2020, 43, 605–618. [Google Scholar] [CrossRef]
- Xia, J.; Jiang, N.; Li, Y.; Wei, Y.; Zhang, X. The long noncoding RNA THRIL knockdown protects hypoxia-induced injuries of H9C2 cells through regulating miR-99a. Cardiol. J. 2019, 26, 564–574. [Google Scholar] [CrossRef]
- Jenei, Z.M.; Gombos, T.; Forhecz, Z.; Pozsonyi, Z.; Karadi, I.; Janoskuti, L.; Prohaszka, Z. Elevated extracellular HSP70 (HSPA1A) level as an independent prognostic marker of mortality in patients with heart failure. Cell Stress Chaperones 2013, 18, 809–813. [Google Scholar] [CrossRef]
- He, M.; Guo, H.; Yang, X.; Zhang, X.; Zhou, L.; Cheng, L.; Zeng, H.; Hu, F.B.; Tanguay, R.M.; Wu, T. Functional SNPs in HSPA1A gene predict risk of coronary heart disease. PLoS ONE 2009, 4, e4851. [Google Scholar] [CrossRef]
- Wang, S.; Yu, W.; Chen, J.; Yao, T.; Deng, F. LncRNA MALAT1 sponges miR-203 to promote inflammation in myocardial ischemia-reperfusion injury. Int. J. Cardiol. 2018, 268, 245. [Google Scholar] [CrossRef]
- Yang, C.A.; Chiang, B.L. Inflammasomes and Childhood Autoimmune Diseases: A Review of Current Knowledge. Clin. Rev. Allergy Immunol. 2021, 61, 156–170. [Google Scholar] [CrossRef]
- Toldo, S.; Mezzaroma, E.; Buckley, L.F.; Potere, N.; Di Nisio, M.; Biondi-Zoccai, G.; Van Tassell, B.W.; Abbate, A. Targeting the NLRP3 inflammasome in cardiovascular diseases. Pharmacol. Ther. 2022, 236, 108053. [Google Scholar] [CrossRef]
- Zhang, X.; Huang, Z.; Wang, Y.; Wang, T.; Li, J.; Xi, P. Long Non-Coding RNA RMRP Contributes to Sepsis-Induced Acute Kidney Injury. Yonsei Med. J. 2021, 62, 262–273. [Google Scholar] [CrossRef]
- Wang, Z.; Kun, Y.; Lei, Z.; Dawei, W.; Lin, P.; Jibo, W. LncRNA MIAT downregulates IL-1beta, TNF-a to suppress macrophage inflammation but is suppressed by ATP-induced NLRP3 inflammasome activation. Cell Cycle 2021, 20, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Tsilimigras, D.I.; Bibli, S.I.; Siasos, G.; Oikonomou, E.; Perrea, D.N.; Filis, K.; Tousoulis, D.; Sigala, F. Regulation of Long Non-Coding RNAs by Statins in Atherosclerosis. Biomolecules 2021, 11, 623. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Chen, L.; Li, H.; Yang, J.; Gong, Z.; Wang, B.; Zhao, X. Clopidogrel reduces apoptosis and promotes proliferation of human vascular endothelial cells induced by palmitic acid via suppression of the long non-coding RNA HIF1A-AS1 in vitro. Mol. Cell. Biochem. 2015, 404, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Bai, W.; Huo, T.; Chen, X.; Song, X.; Meng, C.; Dang, Y.; Rong, C.; Dou, L.; Qi, X. Sacubitril/valsartan inhibits ox-LDL-induced MALAT1 expression, inflammation and apoptosis by suppressing the TLR4/NF-kappaB signaling pathway in HUVECs. Mol. Med. Rep. 2021, 23, 402. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Thallium Stress Test (+) CAG (−) | Thallium Stress Test (+) CAG (+) | Healthy Control | p Value | |
|---|---|---|---|---|
| (n = 17) | (n = 10) | (n = 17) | ||
| Age (years) | 58.8 ± 9.3 (Range 40–77) | 56.7 ± 13.0 (Range 39–77) | 49.4 ± 12.5 (Range 33–74) | 0.088 † |
| Male | 5 (29.4%) | 8 (80%) | 7 (41.2%) | 0.035 # |
| Female | 12 (70.6%) | 2 (20%) | 10 (58.8%) | |
| Cholesterol ratio | 3.6 ± 1.1 | 3.6 ± 1.3 | NA | 0.83 †† |
| Summed stress score (SSS) | 8.4 ± 2.8 | 13.9 ± 3.1 | NA | 0.0002 †† |
| Treatments | ||||
| Statins | 6 (35.3%) | 7 (70%) | 0 | 0.12 ## |
| Antiplatelet agents | 4 (23.5%) | 5 (50%) | 0 | 0.219 ## |
| Calcium channel blocker | 5 (29.4%) | 3 (30%) | 0 | >0.99 ## |
| Angiotensin-receptor blocker | 3 (17.6%) | 1 (10%) | 0 | >0.99 ## |
| Antidiabetic treatment | 2 (11.8%) | 1 (10%) | 0 | >0.99 ## |
| Stenting for significant coronary artery stenosis (>50%) within 6 months after thallium scan | NA | 4 (40%) | NA | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, Y.-C.; Liou, J.-T.; Peng, Y.-M.; Chen, G.-J.; Lin, C.-Y.; Yang, C.-A. Association of Long Noncoding RNA Expression Signatures with Stress-Induced Myocardial Perfusion Defects. Biomolecules 2023, 13, 849. https://doi.org/10.3390/biom13050849
Chang Y-C, Liou J-T, Peng Y-M, Chen G-J, Lin C-Y, Yang C-A. Association of Long Noncoding RNA Expression Signatures with Stress-Induced Myocardial Perfusion Defects. Biomolecules. 2023; 13(5):849. https://doi.org/10.3390/biom13050849
Chicago/Turabian StyleChang, Yu-Chieh, Jun-Ting Liou, Yu-Min Peng, Guan-Jun Chen, Chien-Yu Lin, and Chin-An Yang. 2023. "Association of Long Noncoding RNA Expression Signatures with Stress-Induced Myocardial Perfusion Defects" Biomolecules 13, no. 5: 849. https://doi.org/10.3390/biom13050849