
Update on Diabetic Kidney Disease (DKD): Focus on Non-Albuminuric DKD and Cardiovascular Risk
 ,
,  , , , , , , , ,
, , , , , , , , 
Abstract
:1. Introduction
2. Non-Albuminuric Phenotype: Clinical Presentation, Epidemiology and Risk Factors
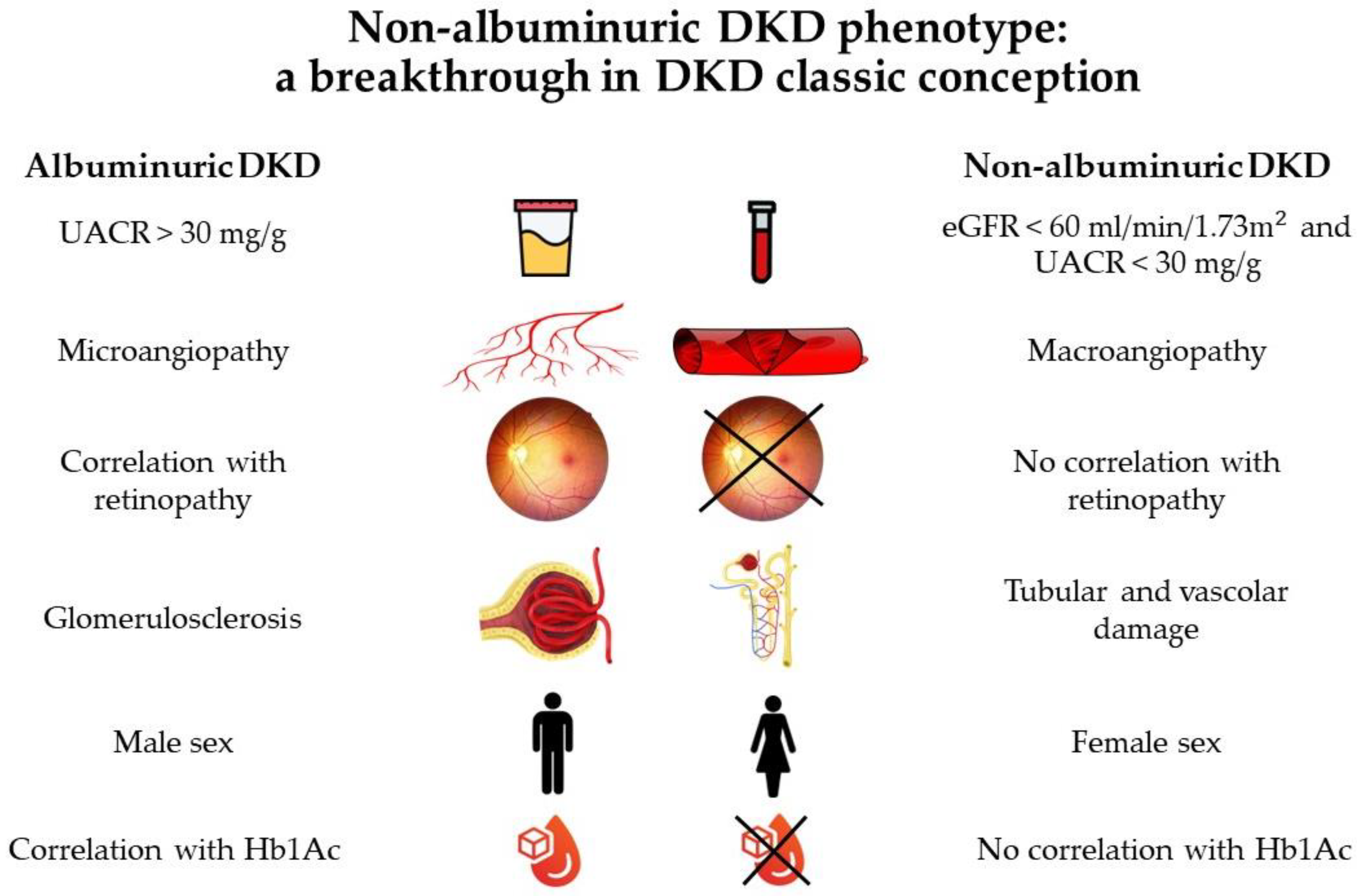
2.1. Clinical Presentation
2.2. Epidemiology
2.3. Risk Factors
3. Pathogenesis and Histopathology
3.1. Histopathology
3.2. Pathogenesis
4. Cardiovascular Risk Profile in DKD Phenotypes
5. Risk of Renal Progression in DKD Phenotypes
6. Therapy
6.1. Angiotensin-Converting Enzyme (ACE) Inhibitors or Angiotensin Receptor Blockers (ARBs)
6.2. Mineralocorticoid Receptor Antagonists (MRAs)
6.3. Glucose-Lowering Agents
6.3.1. DPP-4 Inhibitors
6.3.2. GLP1-RAs
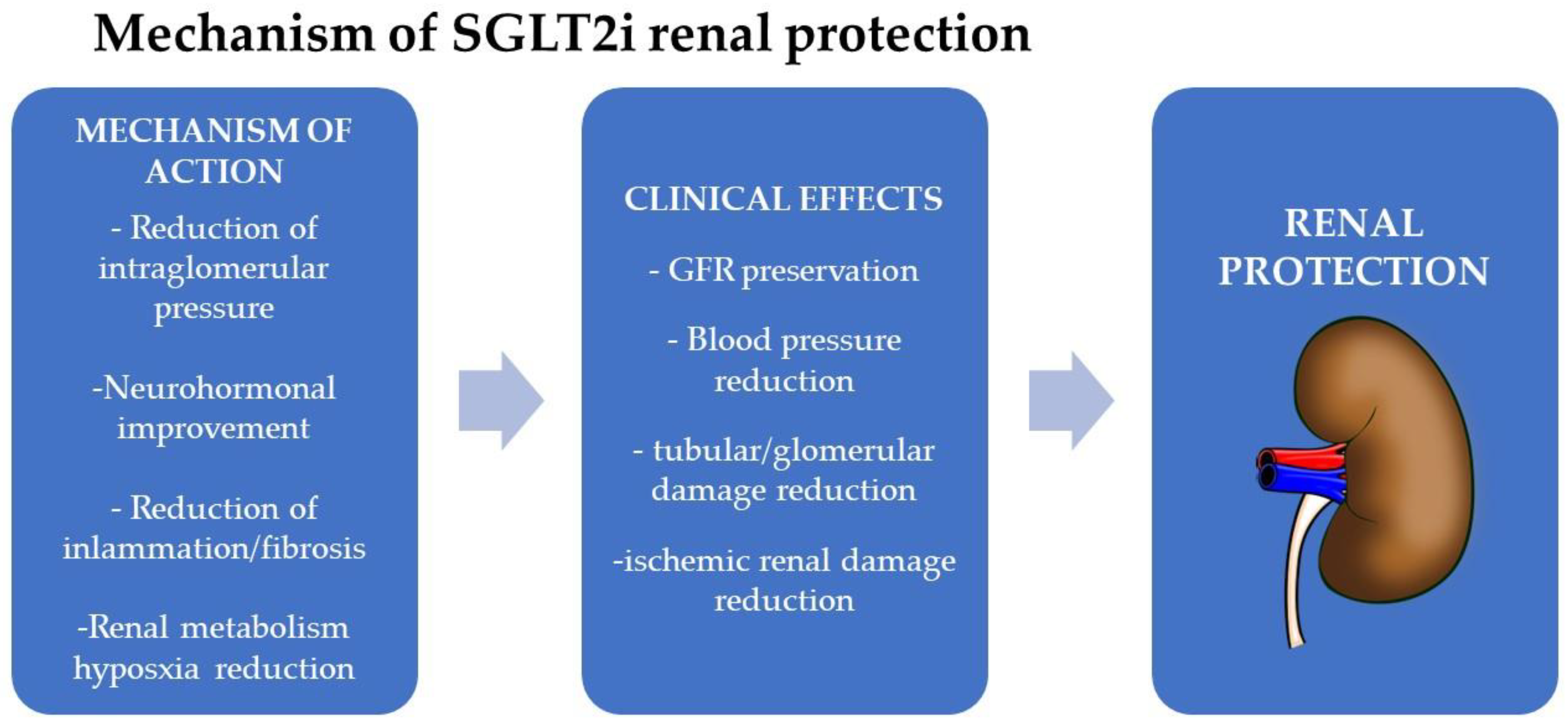
6.3.3. SGLT2 Inhibitors
6.4. Non-Albuminuric DKD Therapy
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roelofs, J.J.; Vogt, L. (Eds.) Diabetic Nephropathy: Pathophysiology and Clinical Aspects; Springer: Cham, Switzerland, 2019; ISBN 978-3-319-93521-8. [Google Scholar]
- Gregg, E.W.; Li, Y.; Wang, J.; Rios Burrows, N.; Ali, M.K.; Rolka, D.; Williams, D.E.; Geiss, L. Changes in Diabetes-Related Complications in the United States, 1990–2010. N. Engl. J. Med. 2014, 370, 1514–1523. [Google Scholar] [CrossRef] [PubMed]
- Coresh, J.; Heerspink, H.J.L.; Sang, Y.; Matsushita, K.; Arnlov, J.; Astor, B.C.; Black, C.; Brunskill, N.J.; Carrero, J.-J.; Feldman, H.I.; et al. Change in Albuminuria and Subsequent Risk of End-Stage Kidney Disease: An Individual Participant-Level Consortium Meta-Analysis of Observational Studies. Lancet Diabetes Endocrinol. 2019, 7, 115–127. [Google Scholar] [CrossRef] [PubMed]
- Di Pino, A.; Scicali, R.; Marchisello, S.; Zanoli, L.; Ferrara, V.; Urbano, F.; Filippello, A.; Di Mauro, S.; Scamporrino, A.; Piro, S.; et al. High Glomerular Filtration Rate Is Associated with Impaired Arterial Stiffness and Subendocardial Viability Ratio in Prediabetic Subjects. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 3393–3400. [Google Scholar] [CrossRef]
- Doshi, S.M.; Friedman, A.N. Diagnosis and Management of Type 2 Diabetic Kidney Disease. Clin. J. Am. Soc. Nephrol. 2017, 12, 1366–1373. [Google Scholar] [CrossRef] [PubMed]
- Kramer, H.J. Renal Insufficiency in the Absence of Albuminuria and Retinopathy Among Adults with Type 2 Diabetes Mellitus. JAMA 2003, 289, 3273. [Google Scholar] [CrossRef]
- Thomas, M.C.; MacIsaac, R.J.; Jerums, G.; Weekes, A.; Moran, J.; Shaw, J.E.; Atkins, R.C. Nonalbuminuric Renal Impairment in Type 2 Diabetic Patients and in the General Population (National Evaluation of the Frequency of Renal Impairment CO-Existing with NIDDM [NEFRON] 11). Diabetes Care 2009, 32, 1497–1502. [Google Scholar] [CrossRef]
- Shi, S.; Ni, L.; Gao, L.; Wu, X. Comparison of Nonalbuminuric and Albuminuric Diabetic Kidney Disease Among Patients With Type 2 Diabetes: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2022, 13, 871272. [Google Scholar] [CrossRef]
- Gaede, P. Remission to Normoalbuminuria during Multifactorial Treatment Preserves Kidney Function in Patients with Type 2 Diabetes and Microalbuminuria. Nephrol. Dial. Transplant. 2004, 19, 2784–2788. [Google Scholar] [CrossRef]
- Oshima, M.; Shimizu, M.; Yamanouchi, M.; Toyama, T.; Hara, A.; Furuichi, K.; Wada, T. Trajectories of Kidney Function in Diabetes: A Clinicopathological Update. Nat. Rev. Nephrol. 2021, 17, 740–750. [Google Scholar] [CrossRef]
- de Zeeuw, D.; Remuzzi, G.; Parving, H.-H.; Keane, W.F.; Zhang, Z.; Shahinfar, S.; Snapinn, S.; Cooper, M.E.; Mitch, W.E.; Brenner, B.M. Proteinuria, a Target for Renoprotection in Patients with Type 2 Diabetic Nephropathy: Lessons from RENAAL. Kidney Int. 2004, 65, 2309–2320. [Google Scholar] [CrossRef]
- Afghahi, H.; Miftaraj, M.; Svensson, A.-M.; Hadimeri, H.; Gudbjörnsdottir, S.; Eliasson, B.; Svensson, M.K. Swedish National Diabetes Register Ongoing Treatment with Renin-Angiotensin-Aldosterone-Blocking Agents Does Not Predict Normoalbuminuric Renal Impairment in a General Type 2 Diabetes Population. J. Diabetes Complicat. 2013, 27, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Penno, G.; Solini, A.; Bonora, E.; Fondelli, C.; Orsi, E.; Zerbini, G.; Trevisan, R.; Vedovato, M.; Gruden, G.; Cavalot, F.; et al. Clinical Significance of Nonalbuminuric Renal Impairment in Type 2 Diabetes. J. Hypertens. 2011, 29, 1802–1809. [Google Scholar] [CrossRef] [PubMed]
- An, J.H.; Cho, Y.M.; Yu, H.G.; Jang, H.C.; Park, K.S.; Kim, S.Y.; Lee, H.K. The Clinical Characteristics of Normoalbuminuric Renal Insufficiency in Korean Type 2 Diabetic Patients: A Possible Early Stage Renal Complication. J. Korean Med. Sci. 2009, 24, S75–S81. [Google Scholar] [CrossRef]
- Kramer, C.K.; Leitão, C.B.; Pinto, L.C.; Silveiro, S.P.; Gross, J.L.; Canani, L.H. Clinical and Laboratory Profile of Patients with Type 2 Diabetes with Low Glomerular Filtration Rate and Normoalbuminuria. Diabetes Care 2007, 30, 1998–2000. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, G. Updating the Natural History of Diabetic Nephropathy. Acta Diabetol. 2014, 51, 905–915. [Google Scholar] [CrossRef]
- Vallon, V.; Komers, R. Pathophysiology of the Diabetic Kidney. In Comprehensive Physiology; Terjung, R., Ed.; Wiley: Hoboken, NJ, USA, 2011; pp. 1175–1232. ISBN 978-0-470-65071-4. [Google Scholar]
- Toth-Manikowski, S.; Atta, M.G. Diabetic Kidney Disease: Pathophysiology and Therapeutic Targets. J. Diabetes Res. 2015, 2015, 1–16. [Google Scholar] [CrossRef]
- Noh, H.; King, G.L. The Role of Protein Kinase C Activation in Diabetic Nephropathy. Kidney Int. 2007, 72, S49–S53. [Google Scholar] [CrossRef]
- García-García, P.M. Inflammation in Diabetic Kidney Disease. World J. Diabetes 2014, 5, 431. [Google Scholar] [CrossRef]
- Brownlee, M. Biochemistry and Molecular Cell Biology of Diabetic Complications. Nature 2001, 414, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Di Mauro, S.; Scamporrino, A.; Filippello, A.; Di Marco, M.; Di Martino, M.T.; Scionti, F.; Di Pino, A.; Scicali, R.; Malaguarnera, R.; Purrello, F.; et al. Mitochondrial RNAs as Potential Biomarkers of Functional Impairment in Diabetic Kidney Disease. Int. J. Mol. Sci. 2022, 23, 8198. [Google Scholar] [CrossRef] [PubMed]
- Tervaert, T.W.C.; Mooyaart, A.L.; Amann, K.; Cohen, A.H.; Cook, H.T.; Drachenberg, C.B.; Ferrario, F.; Fogo, A.B.; Haas, M.; de Heer, E.; et al. Pathologic Classification of Diabetic Nephropathy. J. Am. Soc. Nephrol. 2010, 21, 556–563. [Google Scholar] [CrossRef] [PubMed]
- Dische, F.E. Measurement of Glomerular Basement Membrane Thickness and Its Application to the Diagnosis of Thin-Membrane Nephropathy. Arch. Pathol. Lab. Med. 1992, 116, 43–49. [Google Scholar] [PubMed]
- Mauer, S.M.; Steffes, M.W.; Ellis, E.N.; Sutherland, D.E.; Brown, D.M.; Goetz, F.C. Structural-Functional Relationships in Diabetic Nephropathy. J. Clin. Investig. 1984, 74, 1143–1155. [Google Scholar] [CrossRef] [PubMed]
- Allen, A. So-Called Intercapillary Glomerulosclerosis: A Lesion Associated with Diabetes Mellitus. Morphogenesis and Significance. Arch. Path 1941, 32, 33–51. [Google Scholar]
- Kimmelstiel, P.; Wilson, C. Intercapillary Lesions in the Glomeruli of the Kidney. Am. J. Pathol. 1936, 12, 83–98. [Google Scholar]
- Qian, Y.; Feldman, E.; Pennathur, S.; Kretzler, M.; Brosius, F.C. From Fibrosis to Sclerosis: Mechanisms of Glomerulosclerosis in Diabetic Nephropathy. Diabetes 2008, 57, 1439–1445. [Google Scholar] [CrossRef]
- Yamanouchi, M.; Furuichi, K.; Hoshino, J.; Toyama, T.; Hara, A.; Shimizu, M.; Kinowaki, K.; Fujii, T.; Ohashi, K.; Yuzawa, Y.; et al. Nonproteinuric Versus Proteinuric Phenotypes in Diabetic Kidney Disease: A Propensity Score–Matched Analysis of a Nationwide, Biopsy-Based Cohort Study. Diabetes Care 2019, 42, 891–902. [Google Scholar] [CrossRef]
- Ekinci, E.I.; Jerums, G.; Skene, A.; Crammer, P.; Power, D.; Cheong, K.Y.; Panagiotopoulos, S.; McNeil, K.; Baker, S.T.; Fioretto, P.; et al. Renal Structure in Normoalbuminuric and Albuminuric Patients with Type 2 Diabetes and Impaired Renal Function. Diabetes Care 2013, 36, 3620–3626. [Google Scholar] [CrossRef]
- Nosadini, R.; Velussi, M.; Brocco, E.; Bruseghin, M.; Abaterusso, C.; Saller, A.; Dalla Vestra, M.; Carraro, A.; Bortoloso, E.; Sambataro, M.; et al. Course of Renal Function in Type 2 Diabetic Patients with Abnormalities of Albumin Excretion Rate. Diabetes 2000, 49, 476–484. [Google Scholar] [CrossRef]
- Takaori, K.; Yanagita, M. Insights into the Mechanisms of the Acute Kidney Injury-to-Chronic Kidney Disease Continuum. Nephron 2016, 134, 172–176. [Google Scholar] [CrossRef]
- Rolland, A.-L.; Garnier, A.-S.; Meunier, K.; Drablier, G.; Briet, M. Drug-Induced Acute Kidney Injury: A Study from the French Medical Administrative and the French National Pharmacovigilance Databases Using Capture-Recapture Method. J. Clin. Med. 2021, 10, 168. [Google Scholar] [CrossRef] [PubMed]
- Infante, B.; Conserva, F.; Pontrelli, P.; Leo, S.; Stasi, A.; Fiorentino, M.; Troise, D.; Dello Strologo, A.; Alfieri, C.; Gesualdo, L.; et al. Recent Advances in Molecular Mechanisms of Acute Kidney Injury in Patients with Diabetes Mellitus. Front. Endocrinol. 2022, 13, 903970. [Google Scholar] [CrossRef] [PubMed]
- Venkatachalam, M.A.; Weinberg, J.M.; Kriz, W.; Bidani, A.K. Failed Tubule Recovery, AKI-CKD Transition, and Kidney Disease Progression. J. Am. Soc. Nephrol. 2015, 26, 1765–1776. [Google Scholar] [CrossRef]
- Lee, K.; He, J.C. AKI-to-CKD Transition Is a Potential Mechanism for Non-Albuminuric Diabetic Kidney Disease. Fac. Rev. 2022, 11, 21. [Google Scholar] [CrossRef] [PubMed]
- Porrini, E.; Ruggenenti, P.; Mogensen, C.E.; Barlovic, D.P.; Praga, M.; Cruzado, J.M.; Hojs, R.; Abbate, M.; de Vries, A.P.J. ERA-EDTA diabesity working group Non-Proteinuric Pathways in Loss of Renal Function in Patients with Type 2 Diabetes. Lancet Diabetes Endocrinol. 2015, 3, 382–391. [Google Scholar] [CrossRef] [PubMed]
- Ninomiya, T.; Perkovic, V.; de Galan, B.E.; Zoungas, S.; Pillai, A.; Jardine, M.; Patel, A.; Cass, A.; Neal, B.; Poulter, N.; et al. Albuminuria and Kidney Function Independently Predict Cardiovascular and Renal Outcomes in Diabetes. J. Am. Soc. Nephrol. 2009, 20, 1813–1821. [Google Scholar] [CrossRef]
- Di Marco, M.; Urbano, F.; Filippello, A.; Di Mauro, S.; Scamporrino, A.; Miano, N.; Coppolino, G.; L’Episcopo, G.; Leggio, S.; Scicali, R.; et al. Increased Platelet Reactivity and Proinflammatory Profile Are Associated with Intima-Media Thickness and Arterial Stiffness in Prediabetes. J. Clin. Med. 2022, 11, 2870. [Google Scholar] [CrossRef]
- Hallan, S. Association of Kidney Function and Albuminuria with Cardiovascular Mortality in Older vs Younger Individuals: The HUNT II Study. Arch. Intern. Med. 2007, 167, 2490. [Google Scholar] [CrossRef]
- Svensson, M.K.; Cederholm, J.; Eliasson, B.; Zethelius, B.; Gudbjörnsdottir, S. Albuminuria and Renal Function as Predictors of Cardiovascular Events and Mortality in a General Population of Patients with Type 2 Diabetes: A Nationwide Observational Study from the Swedish National Diabetes Register. Diabetes Vasc. Dis. Res. 2013, 10, 520–529. [Google Scholar] [CrossRef]
- Garofolo, M.; Russo, E.; Miccoli, R.; Lucchesi, D.; Giusti, L.; Sancho-Bornez, V.; Daniele, G.; Del Prato, S.; Penno, G. Albuminuric and Non-Albuminuric Chronic Kidney Disease in Type 1 Diabetes: Association with Major Vascular Outcomes Risk and All-Cause Mortality. J. Diabetes Complicat. 2018, 32, 550–557. [Google Scholar] [CrossRef]
- Drury, P.L.; Ting, R.; Zannino, D.; Ehnholm, C.; Flack, J.; Whiting, M.; Fassett, R.; Ansquer, J.-C.; Dixon, P.; Davis, T.M.E.; et al. Estimated Glomerular Filtration Rate and Albuminuria Are Independent Predictors of Cardiovascular Events and Death in Type 2 Diabetes Mellitus: The Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) Study. Diabetologia 2011, 54, 32–43. [Google Scholar] [CrossRef] [PubMed]
- For the Renal Insufficiency and Cardiovascular Events (RIACE) Study Group; Penno, G.; Solini, A.; Orsi, E.; Bonora, E.; Fondelli, C.; Trevisan, R.; Vedovato, M.; Cavalot, F.; Lamacchia, O.; et al. Non-Albuminuric Renal Impairment Is a Strong Predictor of Mortality in Individuals with Type 2 Diabetes: The Renal Insufficiency and Cardiovascular Events (RIACE) Italian Multicentre Study. Diabetologia 2018, 61, 2277–2289. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, H.; Araki, S.-I.; Kawai, K.; Yamazaki, K.; Shirabe, S.-I.; Sugimoto, H.; Minami, M.; Miyazawa, I.; Maegawa, H. JDDM Study Group the Prognosis of Patients with Type 2 Diabetes and Nonalbuminuric Diabetic Kidney Disease Is Not Always Poor: Implication of the Effects of Coexisting Macrovascular Complications (JDDM 54). Diabetes Care 2020, 43, 1102–1110. [Google Scholar] [CrossRef] [PubMed]
- Jin, Q.; Luk, A.O.; Lau, E.S.H.; Tam, C.H.T.; Ozaki, R.; Lim, C.K.P.; Wu, H.; Jiang, G.; Chow, E.Y.K.; Ng, J.K.; et al. Nonalbuminuric Diabetic Kidney Disease and Risk of All-Cause Mortality and Cardiovascular and Kidney Outcomes in Type 2 Diabetes: Findings from the Hong Kong Diabetes Biobank. Am. J. Kidney Dis. 2022, 80, 196–206.e1. [Google Scholar] [CrossRef]
- Stehouwer, C.D.A.; Smulders, Y.M. Microalbuminuria and Risk for Cardiovascular Disease: Analysis of Potential Mechanisms. J. Am. Soc. Nephrol. 2006, 17, 2106–2111. [Google Scholar] [CrossRef]
- Bigazzi, R.; Bianchi, S.; Nenci, R.; Baldari, D.; Baldari, G.; Campese, V.M. Increased Thickness of the Carotid Artery in Patients with Essential Hypertension and Microalbuminuria. J. Hum. Hypertens. 1995, 9, 827–833. [Google Scholar]
- Diamond, J.R. Analogous Pathobiologic Mechanisms in Glomerulosclerosis and Atherosclerosis. Kidney Int. Suppl. 1991, 31, S29–S34. [Google Scholar]
- Koye, D.N.; Magliano, D.J.; Reid, C.M.; Jepson, C.; Feldman, H.I.; Herman, W.H.; Shaw, J.E. Risk of Progression of Nonalbuminuric CKD to End-Stage Kidney Disease in People with Diabetes: The CRIC (Chronic Renal Insufficiency Cohort) Study. Am. J. Kidney Dis. 2018, 72, 653–661. [Google Scholar] [CrossRef]
- Buyadaa, O.; Magliano, D.J.; Salim, A.; Koye, D.N.; Shaw, J.E. Risk of Rapid Kidney Function Decline, All-Cause Mortality, and Major Cardiovascular Events in Nonalbuminuric Chronic Kidney Disease in Type 2 Diabetes. Diabetes Care 2020, 43, 122–129. [Google Scholar] [CrossRef]
- Wanner, C.; Tonelli, M.; The Kidney Disease: Improving Global Outcomes Lipid Guideline Development Work Group Members. KDIGO Clinical Practice Guideline for Lipid Management in CKD: Summary of Recommendation Statements and Clinical Approach to the Patient. Kidney Int. 2014, 85, 1303–1309. [Google Scholar] [CrossRef]
- King, P.; Peacock, I.; Donnelly, R. The UK Prospective Diabetes Study (UKPDS): Clinical and Therapeutic Implications for Type 2 Diabetes: Therapeutic Implications of the UKPDS. Br. J. Clin. Pharmacol. 1999, 48, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Praga, M.; Hernández, E.; Montoyo, C.; Andrés, A.; Ruilope, L.M.; Rodicio, J.L. Long-Term Beneficial Effects of Angiotensin-Converting Enzyme Inhibition in Patients with Nephrotic Proteinuria. Am. J. Kidney Dis. 1992, 20, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Lewis, E.J.; Hunsicker, L.G.; Bain, R.P.; Rohde, R.D. The Effect of Angiotensin-Converting-Enzyme Inhibition on Diabetic Nephropathy. The Collaborative Study Group. N. Engl. J. Med. 1993, 329, 1456–1462. [Google Scholar] [CrossRef] [PubMed]
- Kasiske, B.L.; Kalil, R.S.; Ma, J.Z.; Liao, M.; Keane, W.F. Effect of Antihypertensive Therapy on the Kidney in Patients with Diabetes: A Meta-Regression Analysis. Ann. Intern. Med. 1993, 118, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Keane, W.F.; Brenner, B.M.; de Zeeuw, D.; Grunfeld, J.-P.; McGill, J.; Mitch, W.E.; Ribeiro, A.B.; Shahinfar, S.; Simpson, R.L.; Snapinn, S.M.; et al. The Risk of Developing End-Stage Renal Disease in Patients with Type 2 Diabetes and Nephropathy: The RENAAL Study. Kidney Int. 2003, 63, 1499–1507. [Google Scholar] [CrossRef]
- Brenner, B.M.; Cooper, M.E.; de Zeeuw, D.; Keane, W.F.; Mitch, W.E.; Parving, H.H.; Remuzzi, G.; Snapinn, S.M.; Zhang, Z.; Shahinfar, S.; et al. Effects of Losartan on Renal and Cardiovascular Outcomes in Patients with Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2001, 345, 861–869. [Google Scholar] [CrossRef]
- de Boer, I.H.; Khunti, K.; Sadusky, T.; Tuttle, K.R.; Neumiller, J.J.; Rhee, C.M.; Rosas, S.E.; Rossing, P.; Bakris, G. Diabetes Management in Chronic Kidney Disease: A Consensus Report by the American Diabetes Association (ADA) and Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2022, 102, 974–989. [Google Scholar] [CrossRef]
- Bomback, A.S.; Kshirsagar, A.V.; Amamoo, M.A.; Klemmer, P.J. Change in Proteinuria After Adding Aldosterone Blockers to ACE Inhibitors or Angiotensin Receptor Blockers in CKD: A Systematic Review. Am. J. Kidney Dis. 2008, 51, 199–211. [Google Scholar] [CrossRef]
- Bakris, G.L.; Agarwal, R.; Chan, J.C.; Cooper, M.E.; Gansevoort, R.T.; Haller, H.; Remuzzi, G.; Rossing, P.; Schmieder, R.E.; Nowack, C.; et al. Effect of Finerenone on Albuminuria in Patients with Diabetic Nephropathy: A Randomized Clinical Trial. JAMA 2015, 314, 884–894. [Google Scholar] [CrossRef]
- Bakris, G.L.; Agarwal, R.; Anker, S.D.; Pitt, B.; Ruilope, L.M.; Rossing, P.; Kolkhof, P.; Nowack, C.; Schloemer, P.; Joseph, A.; et al. Effect of Finerenone on Chronic Kidney Disease Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2020, 383, 2219–2229. [Google Scholar] [CrossRef]
- Pitt, B.; Filippatos, G.; Agarwal, R.; Anker, S.D.; Bakris, G.L.; Rossing, P.; Joseph, A.; Kolkhof, P.; Nowack, C.; Schloemer, P.; et al. Cardiovascular Events with Finerenone in Kidney Disease and Type 2 Diabetes. N. Engl. J. Med. 2021, 385, 2252–2263. [Google Scholar] [CrossRef] [PubMed]
- Filippatos, G.; Anker, S.D.; Pitt, B.; Rossing, P.; Joseph, A.; Kolkhof, P.; Lambelet, M.; Lawatscheck, R.; Bakris, G.L.; Ruilope, L.M.; et al. Finerenone and Heart Failure Outcomes by Kidney Function/Albuminuria in Chronic Kidney Disease and Diabetes. JACC Heart Fail 2022, 10, 860–870. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Lin, H.; Tao, Y.; Xu, Y.; Chen, J.; Jia, Y.; Zheng, Z. Network Meta-Analysis of Mineralocorticoid Receptor Antagonists for Diabetic Kidney Disease. Front. Pharmacol. 2022, 13, 967317. [Google Scholar] [CrossRef] [PubMed]
- For the VADT Study Group; Agrawal, L.; Azad, N.; Bahn, G.D.; Ge, L.; Reaven, P.D.; Hayward, R.A.; Reda, D.J.; Emanuele, N.V. Long-Term Follow-up of Intensive Glycaemic Control on Renal Outcomes in the Veterans Affairs Diabetes Trial (VADT). Diabetologia 2018, 61, 295–299. [Google Scholar] [CrossRef]
- Groop, P.-H.; Cooper, M.E.; Perkovic, V.; Emser, A.; Woerle, H.-J.; von Eynatten, M. Linagliptin Lowers Albuminuria on Top of Recommended Standard Treatment in Patients with Type 2 Diabetes and Renal Dysfunction. Diabetes Care 2013, 36, 3460–3468. [Google Scholar] [CrossRef]
- Tanaka, T.; Higashijima, Y.; Wada, T.; Nangaku, M. The Potential for Renoprotection with Incretin-Based Drugs. Kidney Int. 2014, 86, 701–711. [Google Scholar] [CrossRef]
- Sarafidis, P.A.; Stafylas, P.C.; Georgianos, P.I.; Saratzis, A.N.; Lasaridis, A.N. Effect of Thiazolidinediones on Albuminuria and Proteinuria in Diabetes: A Meta-Analysis. Am. J. Kidney Dis. 2010, 55, 835–847. [Google Scholar] [CrossRef]
- Schernthaner, G.; Mogensen, C.E.; Schernthaner, G.-H. The Effects of GLP-1 Analogues, DPP-4 Inhibitors and SGLT2 Inhibitors on the Renal System. Diabetes Vasc. Dis. Res. 2014, 11, 306–323. [Google Scholar] [CrossRef]
- Elnaem, M.H.; Mansour, N.O.; Nahas, A.F.; Baraka, M.A.; Elkalmi, R.; Cheema, E. Renal Outcomes Associated with the Use of Non-Insulin Antidiabetic Pharmacotherapy: A Review of Current Evidence and Recommendations. Int. J. Gen. Med. 2020, 13, 1395–1409. [Google Scholar] [CrossRef]
- Christiansen, C.F.; Ehrenstein, V.; Heide-Jørgensen, U.; Skovbo, S.; Nørrelund, H.; Sørensen, H.T.; Li, L.; Jick, S. Metformin Initiation and Renal Impairment: A Cohort Study in Denmark and the UK. BMJ Open 2015, 5, e008531. [Google Scholar] [CrossRef]
- Mariano, F.; Pozzato, M.; Inguaggiato, P.; Guarena, C.; Turello, E.; Manes, M.; David, P.; Berutti, S.; Consiglio, V.; Amore, A.; et al. Metformin-Associated Lactic Acidosis Undergoing Renal Replacement Therapy in Intensive Care Units: A Five-Million Population-Based Study in the North-West of Italy. Blood Purif. 2017, 44, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.; Farran, B.; McGurnaghan, S.; McCrimmon, R.J.; Leese, G.P.; Petrie, J.R.; McKeigue, P.; Sattar, N.; Wild, S.; McKnight, J.; et al. Risk of Acute Kidney Injury and Survival in Patients Treated with Metformin: An Observational Cohort Study. BMC Nephrol. 2017, 18, 163. [Google Scholar] [CrossRef] [PubMed]
- De Bhailís, Á.M.; Azmi, S.; Kalra, P.A. Diabetic Kidney Disease: Update on Clinical Management and Non-Glycaemic Effects of Newer Medications for Type 2 Diabetes. Ther. Adv. Endocrinol. Metab. 2021, 12, 20420188211020664. [Google Scholar] [CrossRef] [PubMed]
- Scirica, B.M.; Bhatt, D.L.; Braunwald, E.; Steg, P.G.; Davidson, J.; Hirshberg, B.; Ohman, P.; Frederich, R.; Wiviott, S.D.; Hoffman, E.B.; et al. Saxagliptin and Cardiovascular Outcomes in Patients with Type 2 Diabetes Mellitus. N. Engl. J. Med. 2013, 369, 1317–1326. [Google Scholar] [CrossRef]
- White, W.B.; Cannon, C.P.; Heller, S.R.; Nissen, S.E.; Bergenstal, R.M.; Bakris, G.L.; Perez, A.T.; Fleck, P.R.; Mehta, C.R.; Kupfer, S.; et al. Alogliptin after Acute Coronary Syndrome in Patients with Type 2 Diabetes. N. Engl. J. Med. 2013, 369, 1327–1335. [Google Scholar] [CrossRef]
- Green, J.B.; Bethel, M.A.; Armstrong, P.W.; Buse, J.B.; Engel, S.S.; Garg, J.; Josse, R.; Kaufman, K.D.; Koglin, J.; Korn, S.; et al. Effect of Sitagliptin on Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 232–242. [Google Scholar] [CrossRef]
- Rosenstock, J.; Perkovic, V.; Johansen, O.E.; Cooper, M.E.; Kahn, S.E.; Marx, N.; Alexander, J.H.; Pencina, M.; Toto, R.D.; Wanner, C.; et al. Effect of Linagliptin vs Placebo on Major Cardiovascular Events in Adults with Type 2 Diabetes and High Cardiovascular and Renal Risk: The CARMELINA Randomized Clinical Trial. JAMA 2019, 321, 69–79. [Google Scholar] [CrossRef]
- Mann, J.F.E.; Ørsted, D.D.; Brown-Frandsen, K.; Marso, S.P.; Poulter, N.R.; Rasmussen, S.; Tornøe, K.; Zinman, B.; Buse, J.B. Liraglutide and Renal Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 839–848. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Botros, F.T.; Riddle, M.C.; Rydén, L.; et al. Dulaglutide and Renal Outcomes in Type 2 Diabetes: An Exploratory Analysis of the REWIND Randomised, Placebo-Controlled Trial. Lancet 2019, 394, 131–138. [Google Scholar] [CrossRef]
- Tuttle, K.R.; Lakshmanan, M.C.; Rayner, B.; Busch, R.S.; Zimmermann, A.G.; Woodward, D.B.; Botros, F.T. Dulaglutide versus Insulin Glargine in Patients with Type 2 Diabetes and Moderate-to-Severe Chronic Kidney Disease (AWARD-7): A Multicentre, Open-Label, Randomised Trial. Lancet Diabetes Endocrinol. 2018, 6, 605–617. [Google Scholar] [CrossRef]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jódar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef] [PubMed]
- Bethel, M.A.; Mentz, R.J.; Merrill, P.; Buse, J.B.; Chan, J.C.; Goodman, S.G.; Iqbal, N.; Jakuboniene, N.; Katona, B.G.; Lokhnygina, Y.; et al. Renal Outcomes in the EXenatide Study of Cardiovascular Event Lowering (EXSCEL). Diabetes 2018, 67, 522-P. [Google Scholar] [CrossRef]
- Leoncini, G.; Russo, E.; Bussalino, E.; Barnini, C.; Viazzi, F.; Pontremoli, R. SGLT2is and Renal Protection: From Biological Mechanisms to Real-World Clinical Benefits. Int. J. Mol. Sci. 2021, 22, 4441. [Google Scholar] [CrossRef] [PubMed]
- Zaccardi, F.; Webb, D.R.; Htike, Z.Z.; Youssef, D.; Khunti, K.; Davies, M.J. Efficacy and Safety of Sodium-Glucose Co-Transporter-2 Inhibitors in Type 2 Diabetes Mellitus: Systematic Review and Network Meta-Analysis. Diabetes Obes. Metab. 2016, 18, 783–794. [Google Scholar] [CrossRef] [PubMed]
- Ohashi, N.; Aoki, T.; Matsuyama, T.; Ishigaki, S.; Isobe, S.; Fujikura, T.; Hashimoto, T.; Tsuriya, D.; Morita, H.; Kato, A.; et al. Sodium-Glucose Cotransporter-2 Inhibitor Immediately Decreases Serum Uric Acid Levels in Type 2 Diabetic Patients. Med. Sci. Monit. 2020, 26, e926086. [Google Scholar] [CrossRef]
- Kidokoro, K.; Cherney, D.Z.I.; Bozovic, A.; Nagasu, H.; Satoh, M.; Kanda, E.; Sasaki, T.; Kashihara, N. Evaluation of Glomerular Hemodynamic Function by Empagliflozin in Diabetic Mice Using In Vivo Imaging. Circulation 2019, 140, 303–315. [Google Scholar] [CrossRef]
- Margonato, D.; Galati, G.; Mazzetti, S.; Cannistraci, R.; Perseghin, G.; Margonato, A.; Mortara, A. Renal Protection: A Leading Mechanism for Cardiovascular Benefit in Patients Treated with SGLT2 Inhibitors. Heart Fail Rev. 2021, 26, 337–345. [Google Scholar] [CrossRef]
- Tsai, K.-F.; Chen, Y.-L.; Chiou, T.T.-Y.; Chu, T.-H.; Li, L.-C.; Ng, H.-Y.; Lee, W.-C.; Lee, C.-T. Emergence of SGLT2 Inhibitors as Powerful Antioxidants in Human Diseases. Antioxidants 2021, 10, 1166. [Google Scholar] [CrossRef]
- Neuen, B.L.; Young, T.; Heerspink, H.J.L.; Neal, B.; Perkovic, V.; Billot, L.; Mahaffey, K.W.; Charytan, D.M.; Wheeler, D.C.; Arnott, C.; et al. SGLT2 Inhibitors for the Prevention of Kidney Failure in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Lancet Diabetes Endocrinol. 2019, 7, 845–854. [Google Scholar] [CrossRef]
- Mosenzon, O.; Wiviott, S.D.; Cahn, A.; Rozenberg, A.; Yanuv, I.; Goodrich, E.L.; Murphy, S.A.; Heerspink, H.J.L.; Zelniker, T.A.; Dwyer, J.P.; et al. Effects of Dapagliflozin on Development and Progression of Kidney Disease in Patients with Type 2 Diabetes: An Analysis from the DECLARE-TIMI 58 Randomised Trial. Lancet Diabetes Endocrinol. 2019, 7, 606–617. [Google Scholar] [CrossRef]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef] [PubMed]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef]
- Perkovic, V.; de Zeeuw, D.; Mahaffey, K.W.; Fulcher, G.; Erondu, N.; Shaw, W.; Barrett, T.D.; Weidner-Wells, M.; Deng, H.; Matthews, D.R.; et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes: Results from the CANVAS Program Randomised Clinical Trials. Lancet Diabetes Endocrinol. 2018, 6, 691–704. [Google Scholar] [CrossRef]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef] [PubMed]
- Dwyer, J.P.; Lewis, J.B. Nonproteinuric Diabetic Nephropathy: When Diabetics Don’t Read the Textbook. Med. Clin. N. Am. 2013, 97, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Inzucchi, S.E.; Bergenstal, R.M.; Buse, J.B.; Diamant, M.; Ferrannini, E.; Nauck, M.; Peters, A.L.; Tsapas, A.; Wender, R.; Matthews, D.R. Management of Hyperglycaemia in Type 2 Diabetes, 2015: A Patient-Centred Approach. Update to a Position Statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia 2015, 58, 429–442. [Google Scholar] [CrossRef] [PubMed]
- Sarafidis, P.; Ferro, C.J.; Morales, E.; Ortiz, A.; Malyszko, J.; Hojs, R.; Khazim, K.; Ekart, R.; Valdivielso, J.; Fouque, D.; et al. SGLT-2 Inhibitors and GLP-1 Receptor Agonists for Nephroprotection and Cardioprotection in Patients with Diabetes Mellitus and Chronic Kidney Disease. A Consensus Statement by the EURECA-m and the DIABESITY Working Groups of the ERA-EDTA. Nephrol. Dial. Transplant. 2019, 34, 208–230. [Google Scholar] [CrossRef]
- Kawai, Y.; Uneda, K.; Yamada, T.; Kinguchi, S.; Kobayashi, K.; Azushima, K.; Kanaoka, T.; Toya, Y.; Wakui, H.; Tamura, K. Comparison of Effects of SGLT-2 Inhibitors and GLP-1 Receptor Agonists on Cardiovascular and Renal Outcomes in Type 2 Diabetes Mellitus Patients with/without Albuminuria: A Systematic Review and Network Meta-Analysis. Diabetes Res. Clin. Pract. 2022, 183, 109146. [Google Scholar] [CrossRef]
- The EMPA-KIDNEY Collaborative Group; Herrington, W.G.; Staplin, N.; Wanner, C.; Green, J.B.; Hauske, S.J.; Emberson, J.R.; Preiss, D.; Judge, P.; Mayne, K.J.; et al. Empagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2023, 388, 117–127. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Stefánsson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.-F.; Mann, J.F.E.; McMurray, J.J.V.; Lindberg, M.; Rossing, P.; et al. Dapagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Class | Description |
|---|---|
| I | Mild or nonspecific light microscopy changes and electron microscopy-proven GBM thickening [24] |
| IIa | Mild mesangial expansion (in >25% of the observed mesangium) [25] |
| IIb | Severe mesangial expansion (in >25% of the observed mesangium) |
| III | Nodular sclerosis (Kimmelstiel-Wilson lesion) [26,27] |
| IV | Advanced diabetic glomerulosclerosis (<50% of glomeruli) [28] |
| ADVANCE Post-Hoc Analysis (Ninomiya et al., 2009) [38] * | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cardiovascular events | ||||||||||||
| eGFR ≥ 90 | eGFR 60–89 | eGFR < 60 | ||||||||||
| Normoalbuminuria | 1.00 (reference) | 0.98 (0.78–1.22) | 1.33 (1.02–1.75) | |||||||||
| Microalbuminuria | 1.48 (1.09–2.01) | 1.54 (1.20–1.98) | 2.04 (1.54–2.69) | |||||||||
| Macroalbuminuria | 1.18 (0.52–2.69) | 1.67 (1.09–2.57) | 3.23 (2.20–4.73) | |||||||||
| Cardiovascular death | ||||||||||||
| eGFR ≥ 90 | eGFR 60–89 | eGFR < 60 | ||||||||||
| Normoalbuminura | 1.00 (reference) | 1.22 (0.81–1.84) | 1.85 (1.17–2.92) | |||||||||
| Microalbuminuria | 1.96 (1.16–3.32) | 2.52 (1.65–3.84) | 3.37 (2.15–5.30) | |||||||||
| Macroalbuminuria | 2.87 (1.01–8.18) | 3.61 (2.02–6.43) | 5.93 (3.45–10.20) | |||||||||
| FIELD posthoc Analysis (Drury et al., 2011) [43] # | ||||||||||||
| Cardiovascular events | ||||||||||||
| eGFR ≥ 90 | eGFR 60–89 | eGFR < 60 | ||||||||||
| Normoalbuminura | 1.00 (reference) | 1.11 (0.95–1.29) | 1.63 (1.20–2.20) | |||||||||
| Microalbuminuria | 1.25 (1.01–1.54) | 1.43 (1.18–1.72) | 1.94 (1.37–2.73) | |||||||||
| Macroalbuminuria | 1.19 (0.76–1.85) | 1.77 (1.33–2.36) | 2.30 (1.48–3.55) | |||||||||
| Cardiovascular death | ||||||||||||
| eGFR ≥ 90 | eGFR 60–89 | eGFR < 60 | ||||||||||
| Normoalbuminura | 1.00 (reference) | 1.17 (0.80–1.72) | 2.36 (1.29–4.31) | |||||||||
| Microalbuminuria | 1.73 (1.08–2.77) | 1.38 (0.88–2.15) | 2.96 (1.59–5.51) | |||||||||
| Macroalbuminuria | 1.89 (0.83–4.27) | 2.59 (1.49–4.50) | 5.26 (2.73–10.15) | |||||||||
| RIACE (Penno et al., 2018) [44] @ | ||||||||||||
| All-cause death | ||||||||||||
| eGFR ≥90 | eGFR 75–89 | eGFR 60–74 | eGFR 45–59 | eGFR 30–44 | eGFR <30 | |||||||
| UACR <10 | 1.00 (ref.) | 0.80 (0.67–0.96) | 1.10 (0.83–1.12) | 1.32 (1.97–1.62) | 1.85 (1.40–2.44) | 1.61 (0.88–2.97) | ||||||
| UACR 10–29 | 0.94 (0.78–1.12) | 1.05 (0.89–1.25) | 1.06 (0.88–1.27) | 1.39 (1.14–1.69) | 2.25 (1.79–2.82) | 2.25 (1.49–3.37) | ||||||
| UACR 30–299 | 1.31 (1.08–1.60) | 1.31 (1.09–1.58) | 1.39 (1.15–1.68) | 1.48 (1.22–1.80) | 2.09 (1.69–2.59) | 2.79 (2.09–3.70) | ||||||
| UACR ≥300 | 2.19 (1.55–3.11) | 2.48 (1.82–3.38) | 1.71 (1.23–2.36) | 2.26 (1.71–3.00) | 2.78 (2.14–3.63) | 4.66 (3.59–6.05) | ||||||
| JDDM 54 (Yokoyama et al., 2020) [45] $ | ||||||||||||
| Alb− eGFR− | Alb+ eGFR− | Alb− eGFR+ | Alb+ eGFR+ | |||||||||
| CVD | 1.00 (reference) | 1.75 (1.32–2.34) | 1.06 (0.63–1.79) | 2.30 (1.57–3.39) | ||||||||
| Death or CVD | 1.00 (reference) | 1.73 (1.35–2.21) | 1.02 (0.66–1.60) | 2.32 (1.67–3.24) | ||||||||
| Analysis from Hong Kong Diabetes Biobank (Jin et al., 2022) [46] ° | ||||||||||||
| Alb− GFR− | Alb+ GFR− | Alb− GFR+ | Alb+ GFR+ | |||||||||
| All-cause mortality | 1.00 (reference) | 2.00 (1.52–2.63) | 1.59 (1.04–2.44) | 3.26 (2.43–4.38) | ||||||||
| CVD | 1.00 (reference) | 1.19 (1.02–1.40) | 1.14 (0.88–1.48) | 1.47 (1.23–1.76) | ||||||||
| Hospitalization for HF | 1.00 (reference) | 3.14 (2.09–4.73) | 3.08 (1.82–5.21) | 5.50 (3.63–8.34) | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scilletta, S.; Di Marco, M.; Miano, N.; Filippello, A.; Di Mauro, S.; Scamporrino, A.; Musmeci, M.; Coppolino, G.; Di Giacomo Barbagallo, F.; Bosco, G.; et al. Update on Diabetic Kidney Disease (DKD): Focus on Non-Albuminuric DKD and Cardiovascular Risk. Biomolecules 2023, 13, 752. https://doi.org/10.3390/biom13050752
Scilletta S, Di Marco M, Miano N, Filippello A, Di Mauro S, Scamporrino A, Musmeci M, Coppolino G, Di Giacomo Barbagallo F, Bosco G, et al. Update on Diabetic Kidney Disease (DKD): Focus on Non-Albuminuric DKD and Cardiovascular Risk. Biomolecules. 2023; 13(5):752. https://doi.org/10.3390/biom13050752
Chicago/Turabian StyleScilletta, Sabrina, Maurizio Di Marco, Nicoletta Miano, Agnese Filippello, Stefania Di Mauro, Alessandra Scamporrino, Marco Musmeci, Giuseppe Coppolino, Francesco Di Giacomo Barbagallo, Giosiana Bosco, and et al. 2023. "Update on Diabetic Kidney Disease (DKD): Focus on Non-Albuminuric DKD and Cardiovascular Risk" Biomolecules 13, no. 5: 752. https://doi.org/10.3390/biom13050752