
Association of Asymmetric and Symmetric Dimethylarginine with Inflammation in the Population-Based Study of Health in Pomerania
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. General Characteristics of the Study Population
2.3. Quantification of Arginine, Asymmetric and Symmetric Dimethylarginine
2.4. Cytokine Measurements
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Böger, R.H. Live and let die: Asymmetric dimethylarginine and septic shock. Crit. Care 2006, 10, 169. [Google Scholar] [CrossRef]
- Bogdan, C. Nitric oxide synthase in innate and adaptive immunity: An update. Trends Immunol. 2015, 36, 161–178. [Google Scholar] [CrossRef]
- Winkler, M.S.; Nierhaus, A.; Rösler, G.; Lezius, S.; Harlandt, O.; Schwedhelm, E.; Böger, R.H.; Kluge, S. Symmetrical (SDMA) and asymmetrical dimethylarginine (ADMA) in sepsis: High plasma levels as combined risk markers for sepsis survival. Crit. Care 2018, 22, 216. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef] [PubMed]
- Denegri, A.; Boriani, G. High Sensitivity C-reactive Protein (hsCRP) and its Implications in Cardiovascular Outcomes. Curr. Pharm. Des. 2021, 27, 263–275. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.; Gerlach, H.; Vogelmann, T.; Preissing, F.; Stiefel, J.; Adam, D. Mortality in sepsis and septic shock in Europe, North America and Australia between 2009 and 2019- results from a systematic review and meta-analysis. Crit. Care 2020, 24, 239. [Google Scholar] [CrossRef]
- O’Dwyer, M.J.; Dempsey, F.; Crowley, V.; Kelleher, D.P.; McManus, R.; Ryan, T. Septic shock is correlated with asymmetrical dimethyl arginine levels, which may be influenced by a polymorphism in the dimethylarginine dimethylaminohydrolase II gene: A prospective observational study. Crit. Care 2006, 10, R139. [Google Scholar] [CrossRef]
- Mortensen, K.M.; Itenov, T.S.; Haase, N.; Müller, R.B.; Ostrowski, S.R.; Johansson, P.I.; Olsen, N.V.; Perner, A.; Søe-Jensen, P.; Bestle, M.H. High levels of methylarginines were associated with increased mortality in patients with severe sepsis. Shock 2016, 46, 365–372. [Google Scholar] [CrossRef] [PubMed]
- van Wijk, X.M.R.; Yun, C.; Lynch, K.L. Evaluation of biomarkers in sepsis: High dimethylarginine (ADMA and SDMA) concentrations are associated with mortality. J. Appl. Lab. Med. 2021, 6, 592–605. [Google Scholar] [CrossRef]
- Atzler, D.; Schwedhelm, E.; Nauck, M.; Ittermann, T.; Böger, R.H.; Friedrich, N. Serum reference intervals of homoarginine, ADMA, and SDMA in the study of health in Pomerania. Clin. Chem. Lab. Med. 2014, 52, 1835–1842. [Google Scholar] [CrossRef] [PubMed]
- Moritz, E.; Jedlitschky, G.; Negnal, J.; Tzvetkov, M.V.; Daum, G.; Dörr, M.; Felix, S.B.; Völzke, H.; Nauck, M.; Schwedhelm, E.; et al. Increased Sphingosine-1-Phosphate Serum Concentrations in Subjects with Periodontitis: A Matter of Inflammation. J. Inflamm. Res. 2021, 14, 2883–2896. [Google Scholar] [CrossRef] [PubMed]
- Rotheudt, L.; Moritz, E.; Markus, M.R.P.; Albrecht, D.; Völzke, H.; Friedrich, N.; Schwedhelm, E.; Daum, G.; Schminke, U.; Felix, S.B.; et al. Sphingosine-1-phosphate and vascular disease in the general population. Atherosclerosis 2022, 350, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Ponce-de-Leon, M.; Hannemann, A.; Linseisen, J.; Nauck, M.; Lerch, M.M.; Bülow, R.; Völzke, H.; Friedrich, N.; Kassubek, J.; Müller, H.P.; et al. Links between ectopic and abdominal fat and systemic inflammation: New insights from the SHIP-Trend study. Dig. Liver Dis. 2022, 54, 1030–1037. [Google Scholar] [CrossRef] [PubMed]
- Völzke, H.; Alte, D.; Schmidt, C.O.; Radke, D.; Lorbeer, R.; Friedrich, N.; Aumann, N.; Lau, K.; Piontek, M.; Born, G.; et al. Cohort Profile: The Study of Health in Pomerania. Int. J. Epidemiol. 2011, 40, 294–307. [Google Scholar] [CrossRef]
- Völzke, H.; Schössow, J.; Schmidt, C.O.; Jürgens, C.; Richter, A.; Werner, A.; Werner, N.; Radke, D.; Teumer, A.; Ittermann, T.; et al. Cohort Profile Update: The Study of Health in Pomerania (SHIP). Int. J. Epidemiol. 2022, 51, e372-83. [Google Scholar] [CrossRef]
- Völzke, H.; Ittermann, T.; Schmidt, C.O.; Baumeister, S.E.; Schipf, S.; Alte, D.; Biffar, R.; John, U.; Hoffmann, W. Prevalence trends in lifestyle—Related risk factors. Dtsch. Ärzteblatt Int. 2015, 112, 185–192. [Google Scholar] [CrossRef]
- Winter, T.; Friedrich, N.; Lamp, S.; Schäfer, C.; Schattschneider, M.; Bollmann, S.; Brümmer, D.; Riemann, K.; Petersmann, A.; Nauck, M. The Integrated Research Biobank of the University Medicine Greifswald. Open J. Bioresour. 2020, 7, 1–6. [Google Scholar] [CrossRef]
- Kuster, N.; Cristol, J.-P.; Cavalier, E.; Bargnoux, A.-S.; Halimi, J.-M.; Froissart, M.; Piéroni, L.; Delanaye, P. Enzymatic creatinine assays allow estimation of glomerular filtration rate in stages 1 and 2 chronic kidney disease using CKD-EPI equation. Clin. Chim. Acta 2014, 428, 89–95. [Google Scholar] [CrossRef]
- Schwedhelm, E.; Maas, R.; Tan-Andresen, J.; Schulze, F.; Riederer, U.; Böger, R.H. High-throughput liquid chromatographic-tandem mass spectrometric determination of arginine and dimethylated arginine derivatives in human and mouse plasma. J. Chromatogr. B 2007, 851, 211–219. [Google Scholar] [CrossRef]
- Stone, C.J.; Koo, C.Y. Additive splines in statistics. Proc. Stat. Comp. Sect. Am. Stat. Assoc. 1985, 27, 45–48. [Google Scholar]
- Pautz, A.; Li, H.; Kleinert, H. Regulation of NOS expression in vascular diseases. Front. Biosci. 2021, 26, 85–101. [Google Scholar]
- Feihl, F.; Waeber, B.; Liaudet, L. Is nitric oxide overproduction the target of choice for the management of septic shock? Pharmacol. Ther. 2001, 91, 179–213. [Google Scholar] [CrossRef]
- Schulman, S.P.; Becker, L.C.; Kass, D.A.; Champion, H.C.; Terrin, M.L.; Forman, S.; Ernst, K.V.; Kelemen, M.D.; Townsend, S.N.; Capriotti, A.; et al. L-arginine therapy in acute myocardial infarction: The Vascular Interaction with Age in Myocardial Infarction (VINTAGE MI) randomized clinical trial. JAMA 2006, 295, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Menzel, D.; Haller, H.; Wilhelm, M.; Robenek, H. L-Arginine and B vitamins improve endothelial function in subjects with mild to moderate blood pressure elevation. Eur. J. Nutr. 2018, 57, 557–568. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.; Wu, Y.; Mai, J.; Guo, G.; Meng, J.; Fang, X.; Chen, X.; Liu, C.; Zhong, S. Comprehensive Metabolic Profiling of Inflammation Indicated Key Roles of Glycerophospholipid and Arginine Metabolism in Coronary Artery Disease. Front. Immunol. 2022, 13, 829425. [Google Scholar] [CrossRef] [PubMed]
- Wierzchowska-McNew, R.A.; Engelen, M.P.K.J.; Thaden, J.J.; Ten Have, G.A.M.; Deutz, N.E.P. Obesity- and sex-related metabolism of arginine and nitric oxide in adults. Am. J. Clin. Nutr. 2022, 116, 1610–1620. [Google Scholar] [CrossRef] [PubMed]
- Baert, L.; Ahmed, M.C.; Manfroi, B.; Huard, B. The number 13 of the family: A proliferation inducing ligand. Curr. Opin. Immunol. 2021, 71, 132–137. [Google Scholar] [CrossRef]
- Tsiantoulas, D.; Eslami, M.; Obermayer, G.; Clement, M.; Smeets, D.; Mayer, F.J.; Kiss, M.G.; Enders, L.; Weißer, J.; Göderle, L.; et al. APRIL limits atherosclerosis by binding to heparan sulfate proteoglycans. Nature 2021, 597, 92–96. [Google Scholar] [CrossRef]
- Pontzen, D.L.; Bahls, M.; Albrecht, D.; Felix, S.B.; Dörr, M.; Ittermann, T.; Nauck, M.; Friedrich, N. Low-grade inflammation is associated with a heterogeneous lipoprotein subclass profile in an apparently healthy population sample. Lipids Health Dis. 2023, 22, 100. [Google Scholar] [CrossRef]
- Schepers, E.; Barreto, D.V.; Liabeuf, S.; Glorieux, G.; Eloot, S.; Barreto, F.C.; Massy, Z.; Vanholder, R. European Uremic Toxin Work Group (EUTox). Symmetric dimethylarginine as a proinflammatory agent in chronic kidney disease. Clin. J. Am. Soc. Nephrol. 2011, 6, 2374–2383. [Google Scholar] [CrossRef]
- Speer, T.; Rohrer, L.; Blyszczuk, P.; Shroff, R.; Kuschnerus, K.; Kränkel, N.; Kania, G.; Zewinger, S.; Akhmedov, A.; Shi, Y.; et al. Abnormal high-density lipoprotein induces endothelial dysfunction via activation of Toll-like receptor-2. Immunity 2013, 38, 754–768. [Google Scholar] [CrossRef] [PubMed]
- Dinarello, C.A. Interleukin-1 in the pathogenesis and treatment of inflammatory diseases. Blood 2011, 117, 3720–3732. [Google Scholar] [CrossRef]
- Monaco, C.; Gregan, S.M.; Navin, T.J.; Foxwell, B.M.; Davies, A.H.; Feldmann, M. Toll-like receptor-2 mediates inflammation and matrix degradation in human atherosclerosis. Circulation 2009, 120, 2462–2469. [Google Scholar] [CrossRef] [PubMed]
- Kanazawa, I.; Yano, S.; Yamaguchi, T.; Notsu, Y.; Nabika, T.; Sugimoto, T. Relationships between dimethylarginine and the presence of vertebral fractures in type 2 diabetes mellitus. Clin. Endocrinol. 2010, 73, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, N.; Kadono, Y.; Naito, A.; Matsumoto, K.; Yamamoto, T.; Tanaka, S.; Inoue, J. Segregation of TRAF6-mediated signaling pathways clarifies its role in osteoclastogenesis. EMBO J. 2001, 20, 1271–1280. [Google Scholar] [CrossRef]
- Tikhanovich, I.; Kuravi, S.; Artigues, A.; Villar, M.T.; Dorko, K.; Nawabi, A.; Roberts, B.; Weinman, S.A. Dynamic Arginine Methylation of Tumor Necrosis Factor (TNF) Receptor-associated Factor 6 Regulates Toll-like Receptor Signaling. J. Biol. Chem. 2015, 290, 22236–22249. [Google Scholar] [CrossRef]
- Dowsett, L.; Higgins, E.; Alanazi, S.; Alshuwayer, N.A.; Leiper, F.C.; Leiper, J. ADMA: A Key Player in the Relationship between Vascular Dysfunction and Inflammation in Atherosclerosis. J. Clin. Med. 2020, 9, 3026. [Google Scholar] [CrossRef]
- Iribarren, C.H.G.; Sydow, K.; Wang, B.Y.; Sidney, S.; Cooke, J.P. Asymmetric dimethyl-arginine and coronary artery calcification in young adults entering middle age: The CARDIA Study. Eur. J. Prev. Cardiol. 2007, 14, 222–229. [Google Scholar] [CrossRef]
- Chirinos, J.A.; David, R.; Bralley, J.A.; Zea-Díaz, H.; Muñoz-Atahualpa, E.; Corrales-Medina, F.; Cuba-Bustinza, C.; Chirinos-Pacheco, J.; Medina-Lezama, J. Endogenous nitric oxide synthase inhibitors, arterial hemodynamics, and subclinical vascular disease: The PREVENCION Study. Hypertension 2008, 52, 1051–1059. [Google Scholar] [CrossRef]
- Maas, R.; Xanthakis, V.; Polak, J.F.; Schwedhelm, E.; Sullivan, L.M.; Benndorf, R.; Schulze, F.; Vasan, R.S.; Wolf, P.A.; Böger, R.H.; et al. Association of the endogenous nitric oxide synthase inhibitor ADMA with carotid artery intimal media thickness in the Framingham Heart Study offspring cohort. Stroke 2009, 40, 2715–2719. [Google Scholar] [CrossRef] [PubMed]
- Bahls, M.; Friedrich, N.; Atzler, D.; Felix, S.B.; Nauck, M.A.; Böger, R.H.; Völzke, H.; Schwedhelm, E.; Dörr, M. L-Arginine and SDMA Serum Concentrations Are Associated with Subclinical Atherosclerosis in the Study of Health in Pomerania (SHIP). PLoS ONE 2015, 10, e0131293. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Whole Population n = 3556 | Subpopulation n = 456 | |
|---|---|---|
| Men, % | 50.7 | 46.7 |
| Age, years | 53 (40; 64) | 49 (40; 60) |
| Smoking, % | ||
| Never smoker | 36.0 | 42.3 |
| Ex-smoker | 37.2 | 34.2 |
| Current smoker | 26.8 | 23.5 |
| Diabetes, % | 12.2 | 3.3 |
| Hypertension, % | 47.8 | 37.3 |
| Waist circumference, cm | 91 (81; 101) | 88 (80; 97) |
| BMI, kg/m2 | 27.6 (24.6; 31.0) | 26.9 (24.2; 30.2) |
| Total cholesterol, mmol/L | 5.4 (4.6; 6.2) | 5.5 (4.8; 6.2) |
| HDL cholesterol, mmol/L | 1.39 (1.16; 1.66) | 1.42 (1.20; 1.67) |
| LDL cholesterol, mmol/L | 3.31 (2.67; 3.96) | 3.40 (2.78; 3.99) |
| Triglycerides, mmol/L | 1.40 (0.96; 2.01) | 1.25 (0.88; 1.72) |
| Creatinine, µmol/L | 70 (61; 80) | 70 (61; 78) |
| eGFR, mL/min/1.73 m2 | 97 (85; 108) | 98 (89; 108) |
| WBC, Gpt/L | 5.8 (4.9; 7.0) | 5.5 (4.7; 6.8) |
| Fibrinogen, g/L | 3.0 (2.5; 3.5) | 3.0 (2.4; 3.5) |
| hsCRP, mg/L | 1.29 (0.67; 2.90) | 1.18 (0.56; 3.22) |
| Arginine, µmol/L | 118 (105; 134) | 121 (107; 137) |
| ADMA, µmol/L | 0.70 (0.60; 0.81) | 0.70 (0.60; 0.81) |
| SDMA, µmol/L | 0.50 (0.42; 0.60) | 0.52 (0.44; 0.62) |
| White Blood Count | Fibrinogen | High-Sensitivity C-Reactive Protein | |||||||
|---|---|---|---|---|---|---|---|---|---|
| β | SE | p | β | SE | p | β | SE | p | |
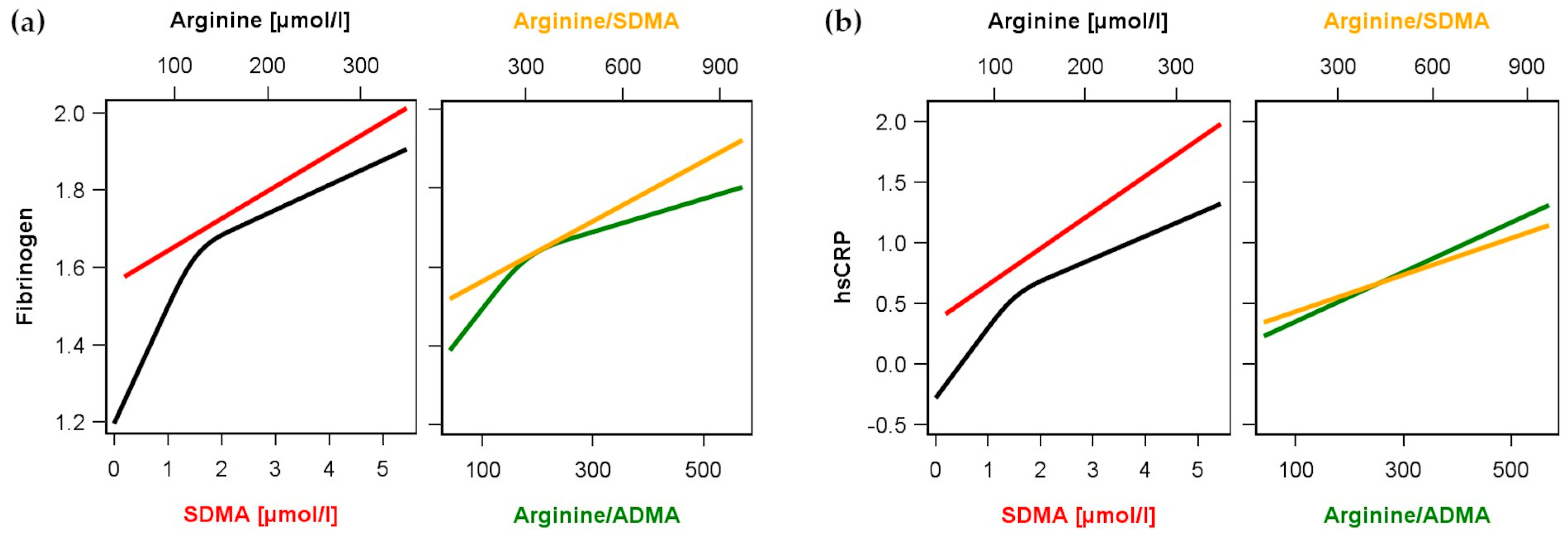
| Arginine Arginine’ | 2.44 × 10−4 | 2.44 × 10−4 | 0.32 | 5.23 × 10−3 | 4.75 × 10−4 | <0.01 | 0.010 | 0.002 | <0.01 |
| - | - | - | −5.64 × 10−7 | 9.59 × 10−8 | <0.01 | −9.29 × 10−7 | 4.32 × 10−7 | 0.03 | |
| ADMA | −0.010 | 0.028 | 0.71 | 0.008 | 0.022 | 0.71 | 0.060 | 0.098 | 0.54 |
| SDMA | −0.018 | 0.038 | 0.64 | 0.083 | 0.031 | 0.01 | 0.298 | 0.137 | 0.03 |
| Arginine/ADMA | 1.93 × 10−4 | 1.21 × 10−4 | 0.11 | 1.79 × 10−3 | 2.54 × 10−4 | <0.01 | 2.04 × 10−3 | 4.30 × 10−4 | <0.01 |
| Arginine/ADMA’ | - | - | - | −4.75 × 10−8 | 1.31 × 10−8 | <0.01 | - | - | - |
| Arginine/SDMA | 1.29 × 10−4 | 7.81 × 10−5 | 0.10 | 4.44 × 10−4 | 6.28 × 10−5 | <0.01 | 8.83 × 10−4 | 2.78 × 10−4 | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Winkler, M.S.; Bahls, M.; Böger, R.H.; Ittermann, T.; Dörr, M.; Friedrich, N.; Schwedhelm, E. Association of Asymmetric and Symmetric Dimethylarginine with Inflammation in the Population-Based Study of Health in Pomerania. Biomolecules 2023, 13, 1612. https://doi.org/10.3390/biom13111612
Winkler MS, Bahls M, Böger RH, Ittermann T, Dörr M, Friedrich N, Schwedhelm E. Association of Asymmetric and Symmetric Dimethylarginine with Inflammation in the Population-Based Study of Health in Pomerania. Biomolecules. 2023; 13(11):1612. https://doi.org/10.3390/biom13111612
Chicago/Turabian StyleWinkler, Martin Sebastian, Martin Bahls, Rainer H. Böger, Till Ittermann, Marcus Dörr, Nele Friedrich, and Edzard Schwedhelm. 2023. "Association of Asymmetric and Symmetric Dimethylarginine with Inflammation in the Population-Based Study of Health in Pomerania" Biomolecules 13, no. 11: 1612. https://doi.org/10.3390/biom13111612