
Ornithine Aspartate and Vitamin-E Combination Has Beneficial Effects on Cardiovascular Risk Factors in an Animal Model of Nonalcoholic Fatty Liver Disease in Rats
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
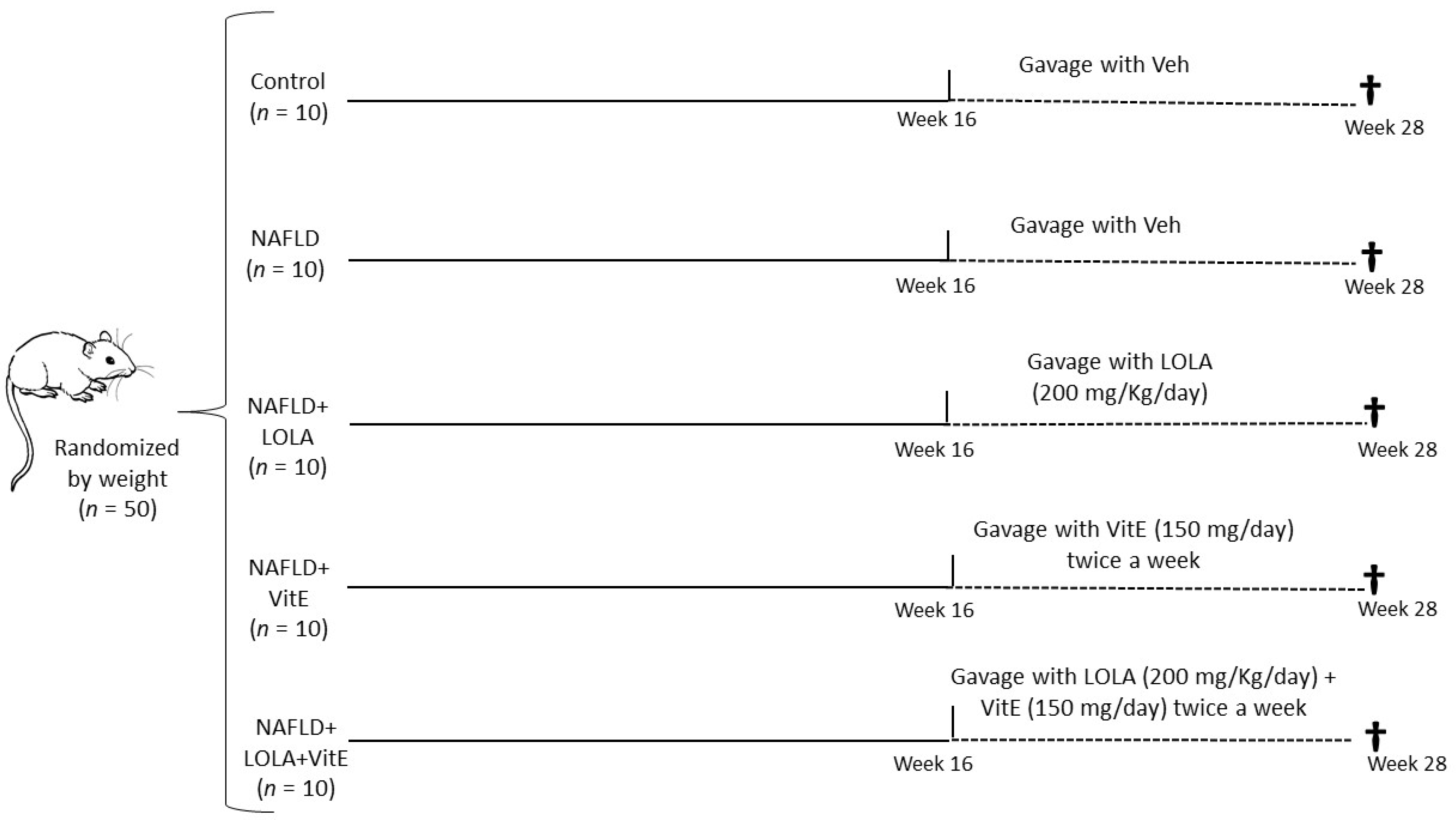
2.1. Animals and Study Design
2.2. Ornithine Aspartate and Vitamin E Treatment
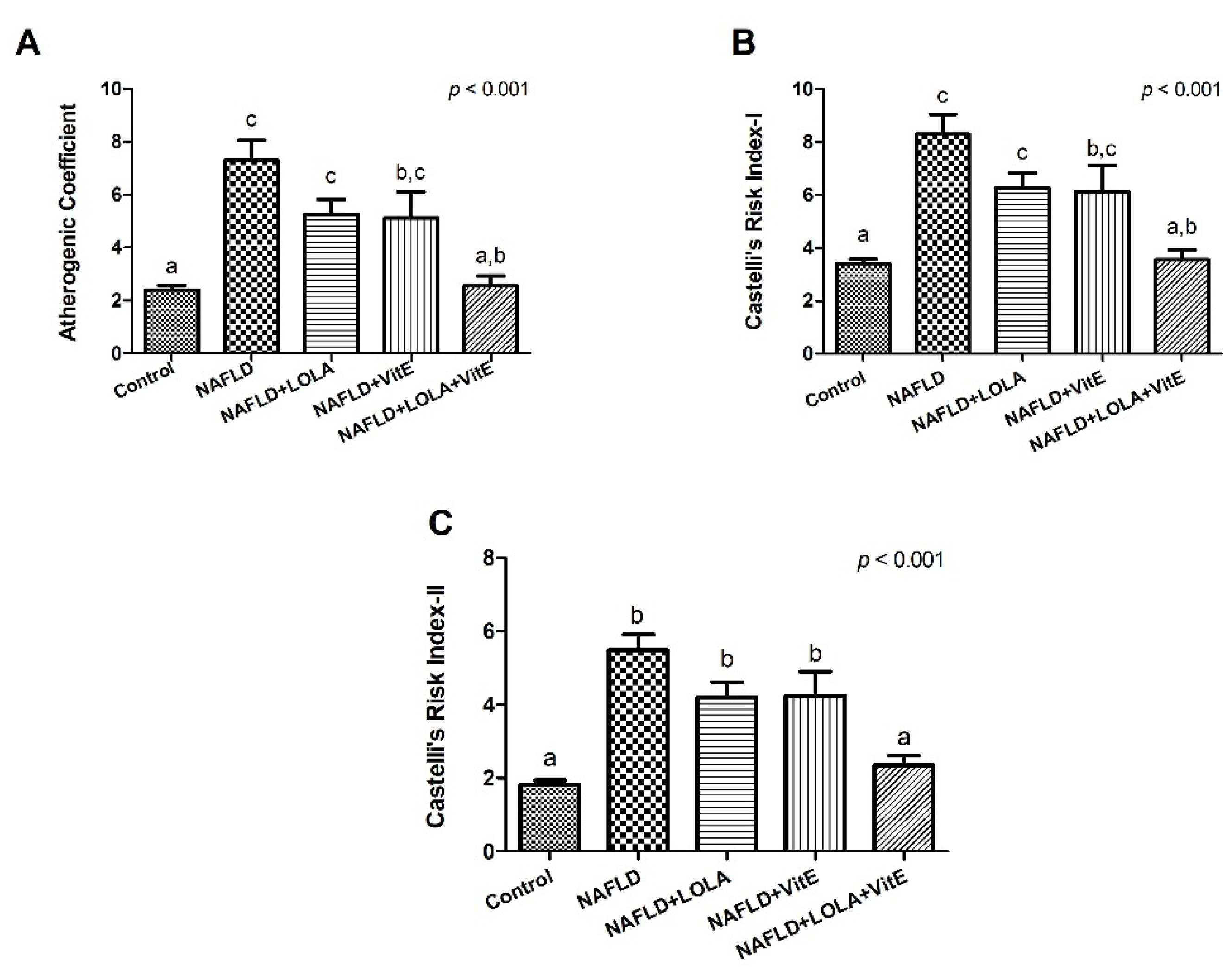
2.3. Atherogenic Ratios
2.4. Systemic Inflammation and Endothelial Dysfunction
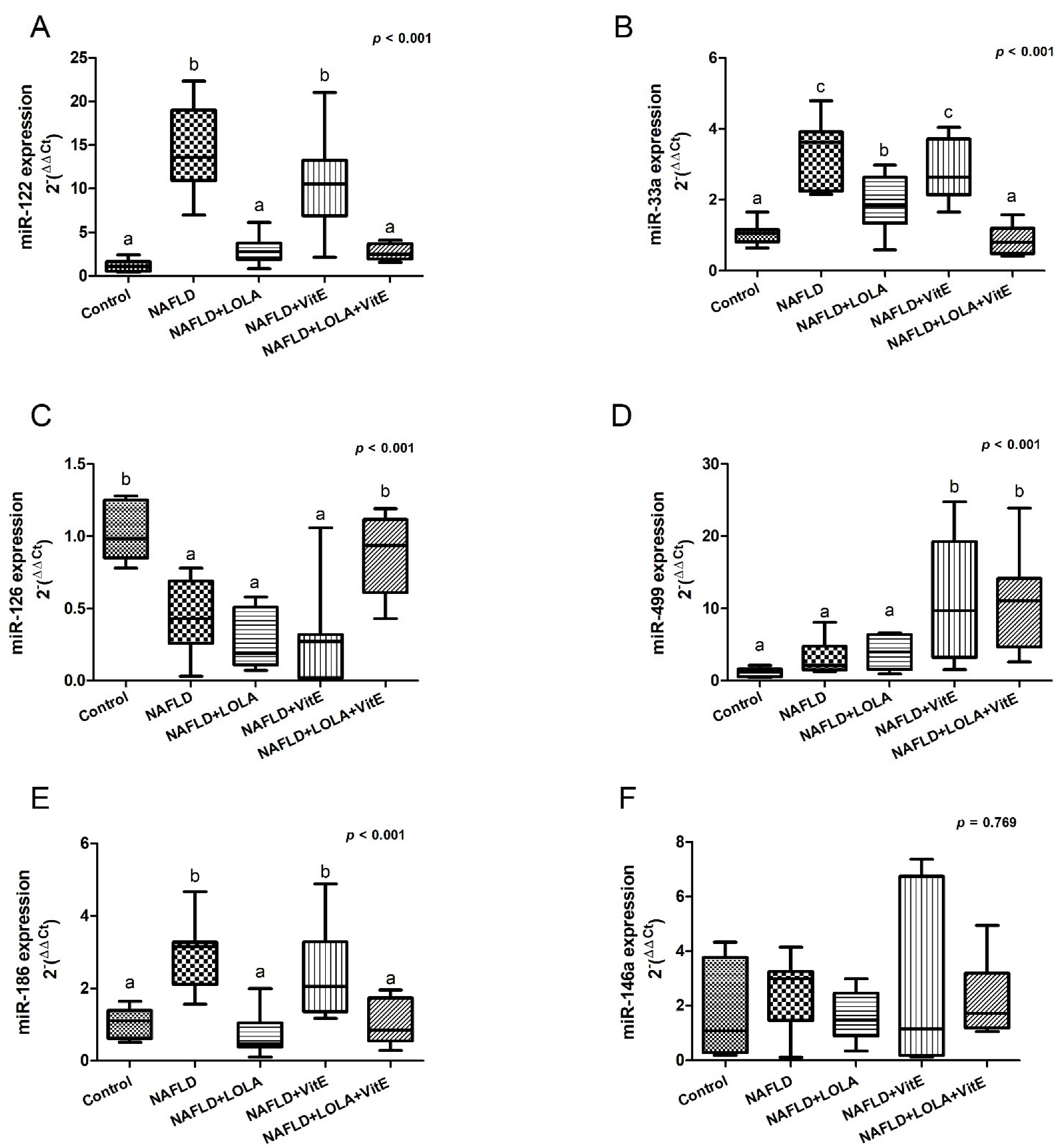
2.5. Analysis of the Circulating microRNAs
2.6. Liver Histopathological Analysis
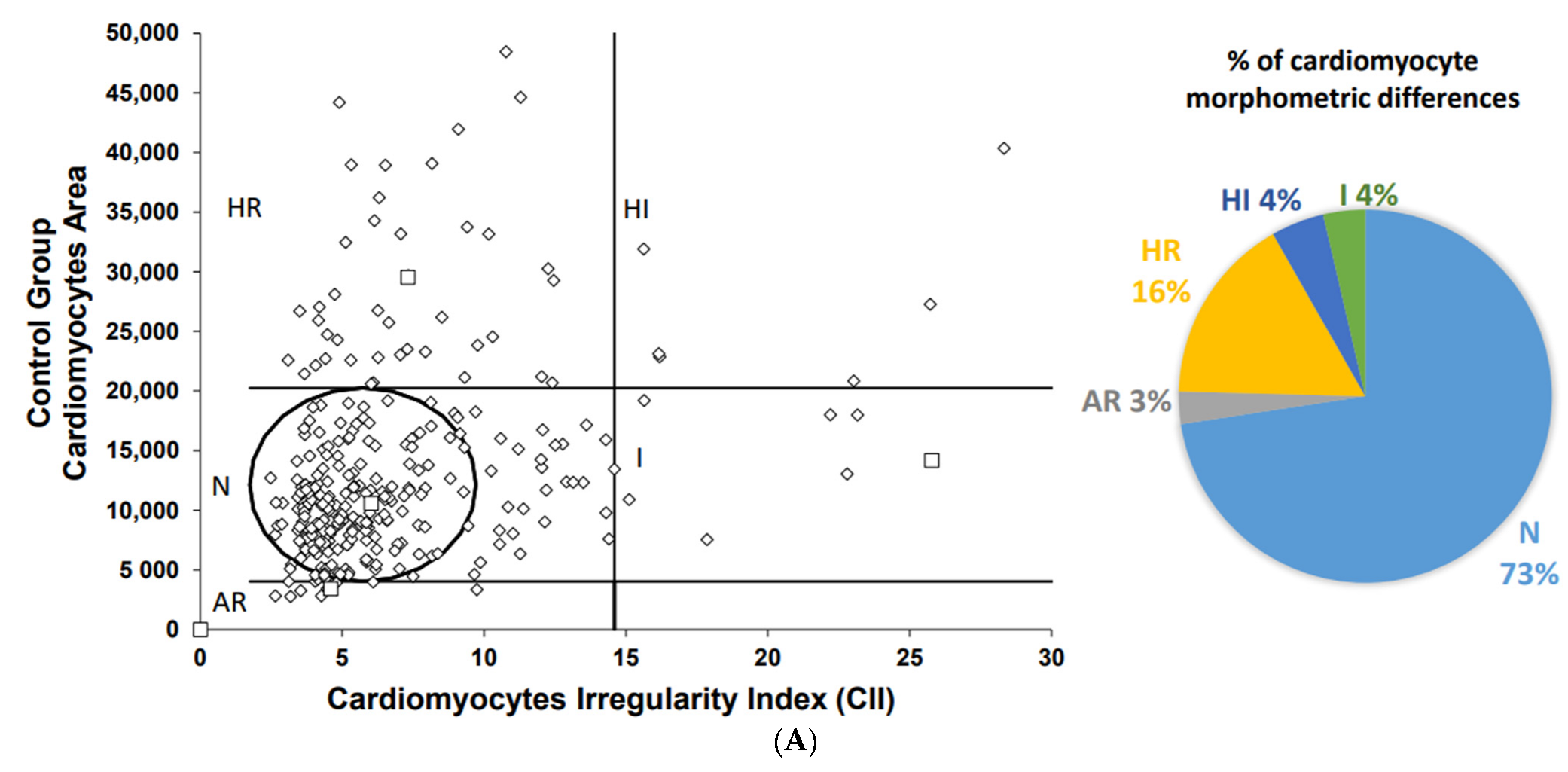
2.7. Cardiomyocytes Morphometric Analysis
2.8. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Atherogenic Ratios to Assess Cardiovascular Risk
3.3. Inflammation and Endothelial Dysfunction in the Assessment of Liver Damage and Cardiovascular Risk
3.4. Gene Expression of the Circulating microRNAs
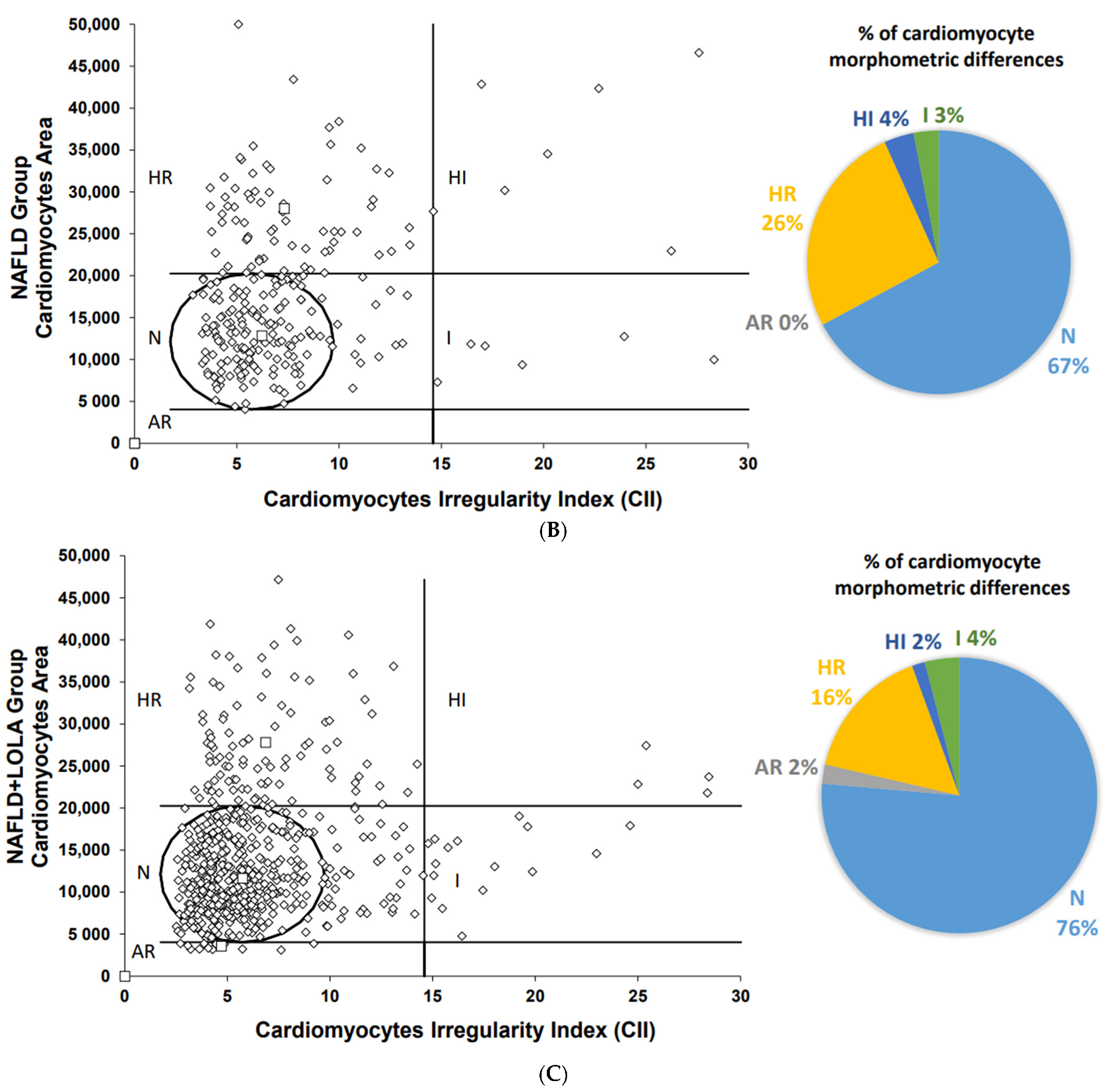
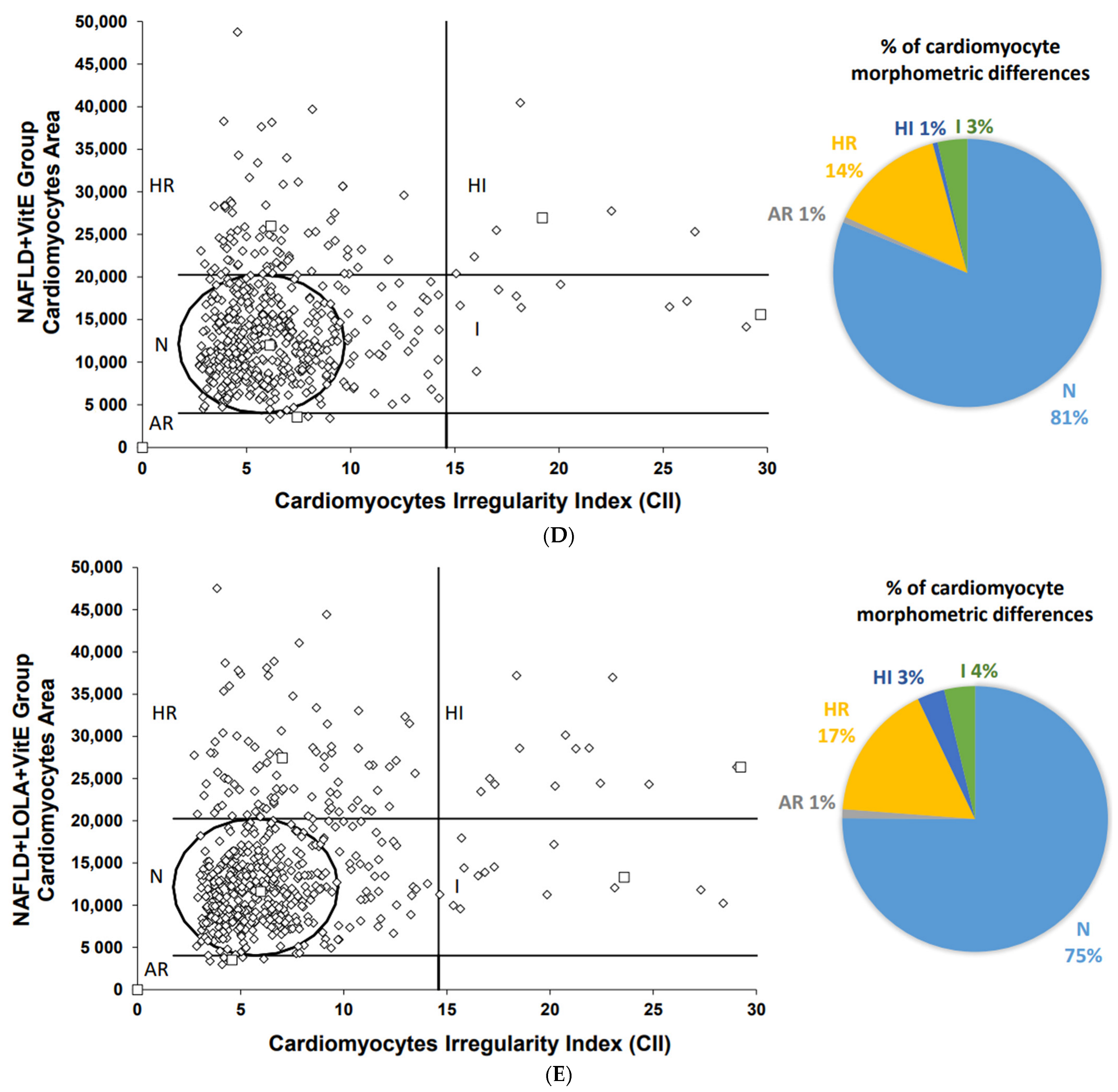
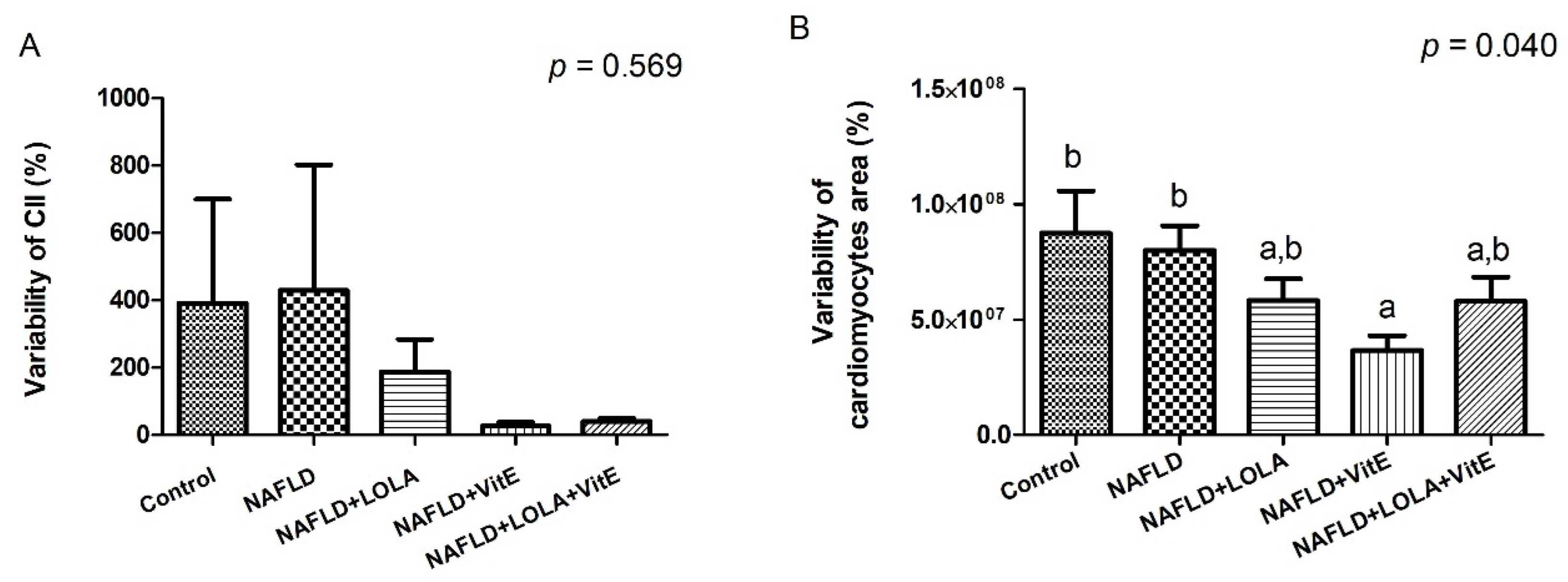
3.5. Morphometric and Histopathological Evaluation of Cardiomyocytes
3.6. Liver Histopathological Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AC | atherogenic coefficient |
| ALT | alanine aminotransferase |
| AST | aspartate aminotransferase |
| CRI | Castelli’s Risk Index |
| CVD | cardiovascular disease |
| HDLc | high density lipoprotein-cholesterol |
| H&E | hematoxylin & eosin |
| HFCD | high-fat and choline-deficient |
| LDLc | low-density lipoprotein-cholesterol |
| ICAM | intercellular adhesion molecule |
| IL | interleukin |
| LOLA | ornithine aspartate |
| MAFLD | metabolic-associated fatty liver disease |
| MCP | monocyte chemoattractant protein |
| NAFLD | nonalcoholic fatty liver disease |
| PAI | plasminogen activator inhibitor |
| TC | total cholesterol |
| TNF | tumor necrosis factor |
| Veh | vehicle |
| vitamin E | VitE |
References
- Eslam, M.; Sanyal, A.J.; George, J.; on behalf of the International Consensus Panel. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 1999–2014.e1. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wong, V.W.-S.; Dufour, J.-F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Kuchay, M.S.; Choudhary, N.S.; Mishra, S.K. Pathophysiological mechanisms underlying MAFLD. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1875–1887. [Google Scholar] [CrossRef]
- Maurice, J.; Manousou, P. Non-alcoholic fatty liver disease. Clin. Med. 2018, 18, 245–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazarus, J.V.; Mark, H.E.; Anstee, Q.M.; Arab, J.P.; Batterham, R.L.; Castera, L.; Cortez-Pinto, H.; Crespo, J.; Cusi, K.; Dirac, M.A.; et al. Advancing the global public health agenda for NAFLD: A consensus statement. Nat. Rev. Gastroenterol. Hepatol. 2022, 19, 60–78. [Google Scholar] [CrossRef]
- Younossi, Z.M. Non-alcoholic fatty liver disease—A global public health perspective. J. Hepatol. 2019, 70, 531–544. [Google Scholar] [CrossRef] [Green Version]
- Targher, G.; Corey, K.E.; Byrne, C.D. NAFLD, and cardiovascular and cardiac diseases: Factors influencing risk, prediction and treatment. Diabetes Metab. 2021, 47, 101215. [Google Scholar] [CrossRef]
- Estes, C.; Razavi, H.; Loomba, R.; Younossi, Z.; Sanyal, A.J. Modeling the epidemic of nonalcoholic fatty liver disease demonstrates an exponential increase in burden of disease. Hepatology 2018, 67, 123–133. [Google Scholar] [CrossRef] [Green Version]
- Targher, G.; Byrne, C.D.; Tilg, H. NAFLD and increased risk of cardiovascular disease: Clinical associations, pathophysiological mechanisms and pharmacological implications. Gut 2020, 69, 1691–1705. [Google Scholar] [CrossRef]
- Kasper, P.; Martin, A.; Lang, S.; Kütting, F.; Goeser, T.; Demir, M.; Steffen, H.-M. NAFLD and cardiovascular diseases: A clinical review. Clin. Res. Cardiol. 2021, 110, 921–937. [Google Scholar] [CrossRef]
- Longo, L.; Rampelotto, P.H.; Filippi-Chiela, E.; de Souza, V.E.G.; Salvati, F.; Cerski, C.T.; da Silveira, T.R.; Oliveira, C.P.; Uribe-Cruz, C.; Álvares-Da-Silva, M.R. Gut dysbiosis and systemic inflammation promote cardiomyocyte abnormalities in an experimental model of steatohepatitis. World J. Hepatol. 2021, 13, 2052–2070. [Google Scholar] [CrossRef] [PubMed]
- Pirola, C.J.; Fernandez Gianotti, T.; Castano, G.O.; Mallardi, P.; San Martino, J.; Mora Gonzalez Lopez Ledesma, M.; Flichman, D.; Mirshahi, F.; Sanyal, A.J.; Sookoian, S. Circulating microRNA signature in non-alcoholic fatty liver disease: From serum non-coding RNAs to liver histology and disease pathogenesis. Gut 2015, 64, 800–812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lombardi, R.; Iuculano, F.; Pallini, G.; Fargion, S.; Fracanzani, A.L. Nutrients, Genetic Factors, and Their Interaction in Non-Alcoholic Fatty Liver Disease and Cardiovascular Disease. Int. J. Mol. Sci. 2020, 21, 8761. [Google Scholar] [CrossRef] [PubMed]
- Longo, L.; Tonin Ferrari, J.; Rampelotto, P.H.; Hirata Dellavia, G.; Pasqualotto, A.; Oliveira, C.P.; Schmidt Cerski, C.T.; da Silveira, T.R.; Uribe-Cruz, C.; Álvares-da-Silva, M.R. Gut Dysbiosis and Increased Intestinal Permeability Drive microRNAs, NLRP-3 Inflammasome and Liver Fibrosis in a Nutritional Model of Non-Alcoholic Steatohepatitis in Adult Male Sprague Dawley Rats. Clin. Exp. Gastroenterol. 2020, 13, 351–368. [Google Scholar] [CrossRef]
- Butterworth, R.F.; Canbay, A. Hepatoprotection by L-Ornithine L-Aspartate in Non-Alcoholic Fatty Liver Disease. Dig. Dis. 2019, 37, 63–68. [Google Scholar] [CrossRef]
- Nagashimada, M.; Ota, T. Role of vitamin E in nonalcoholic fatty liver disease. IUBMB Life 2019, 71, 516–522. [Google Scholar] [CrossRef]
- Alcala, M.; Calderon-Dominguez, M.; Serra, D.; Herrero, L.; Ramos, M.P.; Viana, M. Short-term vitamin E treatment impairs reactive oxygen species signaling required for adipose tissue expansion, resulting in fatty liver and insulin resistance in obese mice. PLoS ONE 2017, 12, e0186579. [Google Scholar] [CrossRef] [Green Version]
- Sanyal, A.J.; Chalasani, N.; Kowdley, K.V.; McCullough, A.; Diehl, A.M.; Bass, N.M.; Neuschwander-Tetri, B.A.; Lavine, J.E.; Tonascia, J.; Unalp, A.; et al. Pioglitazone, Vitamin E, or Placebo for Nonalcoholic Steatohepatitis. N. Engl. J. Med. 2010, 362, 1675–1685. [Google Scholar] [CrossRef] [Green Version]
- Raab, W.P. Kaliopenic nephrosis: Protective action of L-ornithine-L-aspartate. Clin. Chim. Acta 1972, 39, 239–242. [Google Scholar] [CrossRef]
- Mailankot, M.; Jayalekshmi, H.; Chakrabarti, A.; Vasudevan, D.M. Effect of exogenous L-ornithine L-aspartate on ethanol induced testicular injury in Wistar rats. Indian J. Clin. Biochem. 2009, 24, 94–97. [Google Scholar] [CrossRef]
- Alcalá, M.; Sánchez-Vera, I.; Sevillano, J.; Herrero, L.; Serra, D.; Ramos, M.P.; Viana, M. Vitamin E reduces adipose tissue fibrosis, inflammation, and oxidative stress and improves metabolic profile in obesity. Obesity 2015, 23, 1598–1606. [Google Scholar] [CrossRef] [PubMed]
- Sujatha, R.; Kavitha, S. Atherogenic indices in stroke patients: A retrospective study. Iran. J. Neurol. 2017, 16, 78–82. [Google Scholar] [PubMed]
- Liang, W.; Menke, A.L.; Driessen, A.; Koek, G.H.; Lindeman, J.H.; Stoop, R.; Havekes, L.M.; Kleemann, R.; van den Hoek, A.M. Establishment of a General NAFLD Scoring System for Rodent Models and Comparison to Human Liver Pathology. PLoS ONE 2014, 9, e115922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiela, E.; Oliveira, M.M.; Jurkovski, B.; Jacques, S.M.C.; da Silva, V.D.; Lenz, G. Nuclear Morphometric Analysis (NMA): Screening of Senescence, Apoptosis and Nuclear Irregularities. PLoS ONE 2012, 7, e42522. [Google Scholar] [CrossRef] [Green Version]
- Nunes, T.W.; Filippi-Chiela, E.C.; Callegari-Jacques, S.M.; Da Silva, V.D.; Sansonowicz, T.; Lenz, G.; Roehe, A.V. Nuclear morphometric analysis in tissue as an objective tool with potential use to improve melanoma staging. Melanoma Res. 2019, 29, 474–482. [Google Scholar] [CrossRef]
- Walker, C.; Spinale, F.G. The structure and function of the cardiac myocyte: A review of fundamental concepts. J. Thorac. Cardiovasc. Surg. 1999, 118, 375–382. [Google Scholar] [CrossRef] [Green Version]
- Guerreiro, G.T.S.; Longo, L.; Fonseca, M.A.; de Souza, V.E.G.; Álvares-da-Silva, M.R. Does the risk of cardiovascular events differ between biopsy-proven NAFLD and MAFLD? Hepatol. Int. 2021, 15, 380–391. [Google Scholar] [CrossRef]
- Deprince, A.; Haas, J.T.; Staels, B. Dysregulated lipid metabolism links NAFLD to cardiovascular disease. Mol. Metab. 2020, 42, 101092. [Google Scholar] [CrossRef]
- Canbay, A.; Sowa, J.-P. l-Ornithine l-Aspartate (LOLA) as a Novel Approach for Therapy of Non-alcoholic Fatty Liver Disease. Drugs 2019, 79 (Suppl. 1), 39–44. [Google Scholar] [CrossRef] [Green Version]
- Gaedicke, S.; Zhang, X.; Schmelzer, C.; Lou, Y.; Doering, F.; Frank, J.; Rimbach, G. Vitamin E dependent microRNA regulation in rat liver. FEBS Lett. 2008, 582, 3542–3546. [Google Scholar] [CrossRef]
- Tian, L.-Y.; Lu, L.-G.; Tang, C.-W.; Xie, Y.; Luo, H.-S.; Tan, S.-Y.; Pang, Z.; Zhang, Y.-L.; Gong, L.-B.; Li, Y.-M.; et al. Aspartate-ornithine granules in the treatment of nonalcoholic steatohepatitis: A multiple-dose parallel controlled clinical trial. Zhonghua Gan Zang Bing Za Zhi 2013, 21, 528–532. [Google Scholar] [PubMed]
- Corey, K.E.; Vuppalanchi, R.; Wilson, L.A.; Cummings, O.W.; Chalasani, N.; Crn, T.N. NASH resolution is associated with improvements in HDL and triglyceride levels but not improvement in LDL or non-HDL-C levels. Aliment. Pharmacol. Ther. 2015, 41, 301–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dorairaj, V.; Sulaiman, S.A.; Abu, N.; Murad, N.A.A. Nonalcoholic Fatty Liver Disease (NAFLD): Pathogenesis and Noninvasive Diagnosis. Biomedicines 2021, 10, 15. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Song, J.; Wang, C.; Niu, D.; Li, H.; Liu, Y.; Ma, L.; Yu, R.; Chen, X.; Zen, K.; et al. Identification of serum microRNAs for cardiovascular risk stratification in dyslipidemia subjects. Int. J. Cardiol. 2014, 172, 232–234. [Google Scholar] [CrossRef] [PubMed]
- Moscoso, I.; Cebro-Márquez, M.; Martínez-Gómez, Á.; Abou-Jokh, C.; Martínez-Monzonís, M.A.; Martínez-Sande, J.L.; González-Melchor, L.; García-Seara, J.; Fernández-López, X.A.; Moraña-Fernández, S.; et al. Circulating miR-499a and miR-125b as Potential Predictors of Left Ventricular Ejection Fraction Improvement after Cardiac Resynchronization Therapy. Cells 2022, 11, 271. [Google Scholar] [CrossRef]
- Zhou, R.; Huang, W.; Fan, X.; Liu, F.; Luo, L.; Yuan, H.; Jiang, Y.; Xiao, H.; Zhou, Z.; Deng, C.; et al. miR-499 released during myocardial infarction causes endothelial injury by targeting α7-nAchR. J. Cell Mol. Med. 2019, 23, 6085–6097. [Google Scholar] [CrossRef] [Green Version]
- Pereira-Da-Silva, T.; Napoleão, P.; Costa, M.; Gabriel, A.; Selas, M.; Silva, F.; Enguita, F.; Ferreira, R.; Carmo, M. Circulating miRNAs Are Associated with the Systemic Extent of Atherosclerosis: Novel Observations for miR-27b and miR-146. Diagnostics 2021, 11, 318. [Google Scholar] [CrossRef]
- Pereira-Da-Silva, T.; Napoleão, P.; Costa, M.; Gabriel, A.; Selas, M.; Silva, F.; Enguita, F.; Ferreira, R.C.; Carmo, M.M. Association between miR-146a and Tumor Necrosis Factor Alpha (TNF-α) in Stable Coronary Artery Disease. Medicina 2021, 57, 575. [Google Scholar] [CrossRef]
- Alique, M.; Bodega, G.; Giannarelli, C.; Carracedo, J.; Ramírez, R. MicroRNA-126 regulates Hypoxia-Inducible Factor-1α which inhibited migration, proliferation, and angiogenesis in replicative endothelial senescence. Sci. Rep. 2019, 9, 7381. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.H.; Sangoi, A.R.; Leung, S.; Marinelli, R.J.; Nielsen, T.O.; van de Vijver, M.J.; West, R.B.; van de Rijn, M.; Koller, D. Systematic Analysis of Breast Cancer Morphology Uncovers Stromal Features Associated with Survival. Sci. Transl. Med. 2011, 3, 108ra113. [Google Scholar] [CrossRef]
- Bugrova, M.L.; Abrosimov, D.A.; Ermolin, I.L. Ultrastructural Morphological Characterization of Right Atrial and Left Ventricular Rat Cardiomyocytes during Postreperfusion Period. Bull. Exp. Biol. Med. 2017, 163, 805–808. [Google Scholar] [CrossRef]
- Mula, J.; Lee, J.D.; Liu, F.; Yang, L.; Peterson, C.A. Automated image analysis of skeletal muscle fiber cross-sectional area. J. Appl. Physiol. (1985) 2013, 114, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Walters, J. Muscle hypertrophy and pseudohypertrophy. Pract. Neurol. 2017, 17, 369–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pierantonelli, I.; Svegliati-Baroni, G. Nonalcoholic Fatty Liver Disease: Basic Pathogenetic Mechanisms in the Progression from NAFLD to NASH. Transplantation 2019, 103, e1–e13. [Google Scholar] [CrossRef] [PubMed]
- Tsuchida, T.; Lee, Y.A.; Fujiwara, N.; Ybanez, M.; Allen, B.; Martins, S.; Fiel, M.I.; Goossens, N.; Chou, H.-I.; Hoshida, Y.; et al. A simple diet- and chemical-induced murine NASH model with rapid progression of steatohepatitis, fibrosis and liver cancer. J. Hepatol. 2018, 69, 385–395. [Google Scholar] [CrossRef]
- Oseini, A.M.; Cole, B.K.; Issa, D.; Feaver, R.E.; Sanyal, A.J. Translating scientific discovery: The need for preclinical models of nonalcoholic steatohepatitis. Hepatol. Int. 2018, 12, 6–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butterworth, R.F.; Kircheis, G.; Hilger, N.; McPhail, M.J. Efficacy of l-Ornithine l-Aspartate for the Treatment of Hepatic Encephalopathy and Hyperammonemia in Cirrhosis: Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Exp. Hepatol. 2018, 8, 301–313. [Google Scholar] [CrossRef]
- Peng, C.; Stewart, A.G.; Woodman, O.L.; Ritchie, R.H.; Qin, C.X. Non-Alcoholic Steatohepatitis: A Review of Its Mechanism, Models and Medical Treatments. Front. Pharmacol. 2020, 11, 603926. [Google Scholar] [CrossRef]
- Fougerat, A.; Montagner, A.; Loiseau, N.; Guillou, H.; Wahli, W. Peroxisome Proliferator-Activated Receptors and Their Novel Ligands as Candidates for the Treatment of Non-Alcoholic Fatty Liver Disease. Cells 2020, 9, 1638. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables # | Control | NAFLD | NAFLD+LOLA | NAFLD+VitE | NAFLD+LOLA+VitE | p * |
|---|---|---|---|---|---|---|
| IL-1β (pg/mL) | 7.92 (0.69–15.16) | 5.50 (1.49–9.51) | 7.87 (2.0−13.73) | 9.04 (3.30–14.79) | 10.12 (1.17–19.06) | 0.843 |
| IL-6 (pg/mL) | 191.75 (36.93–994.25) | 116.15 (13.96–439.46) | 90.94 (25.47–149.70) | 113.67 (13.96–217.46) | 22.20 (1.96–994.25) | 0.165 |
| TNF-α (pg/mL) | 5.21 (1.44–8.99) | 3.49 (2.71–4.25) | 4.02 (2.58−5.46) | 4.56 (3.28–5.85) | 3.39 (1.90–4.87) | 0.580 |
| IL-10 (pg/mL) | 33.17 (19.93–49.62) | 56.07 (29.12–91.3) | 44.66 (24.88–76.66) | 53.55 (29.12–76.84) | 48.05 (27.53–66.41) | 0.062 |
| MCP-1 (pg/mL) | 317.39 (252.11–382.66) a | 433.32 (356.65–510.0) a,b | 395.64 (259.58–531.70) a,b | 523.19 (450.96–595.42) b | 453.10 (317.08–588.92) a,b | 0.037 |
| e-selectin (ng/mL) | 1.72 (1.42–2.03) a | 2.38 (1.95–2.80) a,b | 2.52 (2.22–2.82) b | 2.20 (1.76–2.65) a,b | 2.43 (2.0–2.87) b | 0.015 |
| ICAM-1 (ng/mL) | 0.14 (±0.03) a | 0.46 (±0.15) a,b | 0.67 (±0.15) b | 0.60 (±0.18) b | 1.06 (±0.40) b | <0.001 |
| PAI-1 (pg/mL) | 42.56 (18.24–66.88) | 46.28 (29.04–63.52) | 106.26 (29.57–182.94) | 89.25 (43.46–135.03) | 122.80 (19.78–225.80) | 0.170 |
| Insulin (pg/mL) | 381.52 (±74.72) a | 1750.39 (±498.76) b | 1170.23 (±264.63) a,b | 1023.09 (±204.90) a,b | 1880.82 (±326.98) b | <0.001 |
| Leptin (pg/mL) | 2227.51 (68.93–7502.01) a | 10119.70 (1203.67–25894.03) b | 7240.19 (3879.69–10600.70) a,b | 10807.54 (2779.80–18835.28) b | 11202.96 (7618.65–14787.270) a | 0.025 |
| Adiponectina (ng/mL) | 15.32 (11.36–19.28) a | 35.45 (26.87–44.03) b | 37.31 (29.59–45.04) b | 37.91 (22.91–52.92) b | 30.05 (26.10–35.25) a,b | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Freitas, L.B.R.; Longo, L.; Filippi-Chiela, E.; de Souza, V.E.G.; Behrens, L.; Pereira, M.H.M.; Leonhard, L.C.; Zanettini, G.; Pinzon, C.E.; Luchese, E.; et al. Ornithine Aspartate and Vitamin-E Combination Has Beneficial Effects on Cardiovascular Risk Factors in an Animal Model of Nonalcoholic Fatty Liver Disease in Rats. Biomolecules 2022, 12, 1773. https://doi.org/10.3390/biom12121773
de Freitas LBR, Longo L, Filippi-Chiela E, de Souza VEG, Behrens L, Pereira MHM, Leonhard LC, Zanettini G, Pinzon CE, Luchese E, et al. Ornithine Aspartate and Vitamin-E Combination Has Beneficial Effects on Cardiovascular Risk Factors in an Animal Model of Nonalcoholic Fatty Liver Disease in Rats. Biomolecules. 2022; 12(12):1773. https://doi.org/10.3390/biom12121773
Chicago/Turabian Stylede Freitas, Laura Bainy Rodrigues, Larisse Longo, Eduardo Filippi-Chiela, Valessa Emanoele Gabriel de Souza, Luiza Behrens, Matheus Henrique Mariano Pereira, Luiza Cecília Leonhard, Giulianna Zanettini, Carlos Eduardo Pinzon, Eduardo Luchese, and et al. 2022. "Ornithine Aspartate and Vitamin-E Combination Has Beneficial Effects on Cardiovascular Risk Factors in an Animal Model of Nonalcoholic Fatty Liver Disease in Rats" Biomolecules 12, no. 12: 1773. https://doi.org/10.3390/biom12121773