
Plasma Catestatin Levels and Advanced Glycation End Products in Patients on Hemodialysis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Considerations
2.2. Subjects
2.3. Blood Sampling and Laboratory Analysis
2.4. Blood Pressure Measurement
2.5. AGEs Measurement
2.6. Anthropometric Measurements and Clinical Examination
2.7. Malnutrition and Inflammation Assessment Scores
2.8. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Population
3.2. Laboratory Parameters of the Study Population
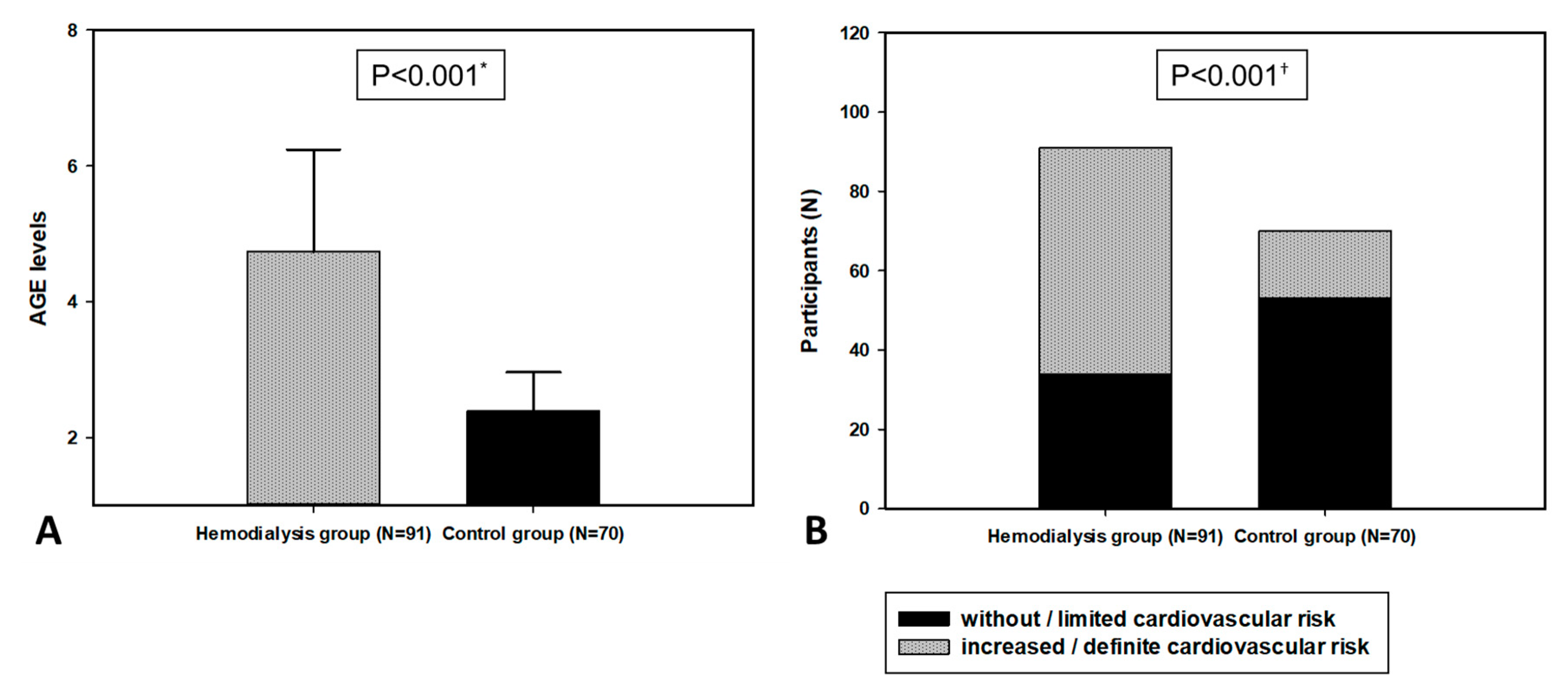
3.3. Skin Autofloruscence Level of AGEs in the Study Population
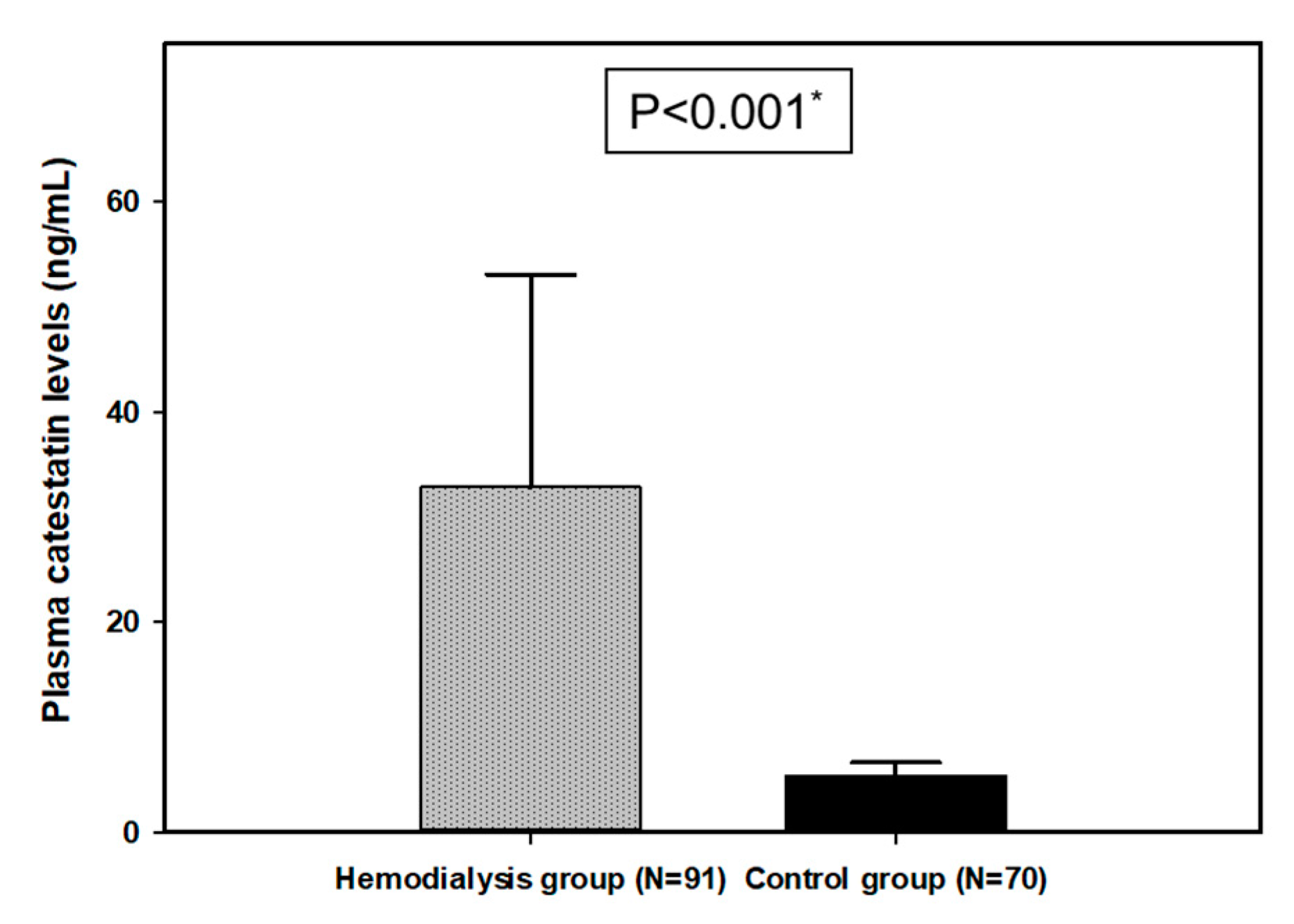
3.4. Plasma CST Levels in the Study Population
3.5. CST and AGEs Correlations with Anthropometric, Laboratory and Clinical Parameters in the HD Group
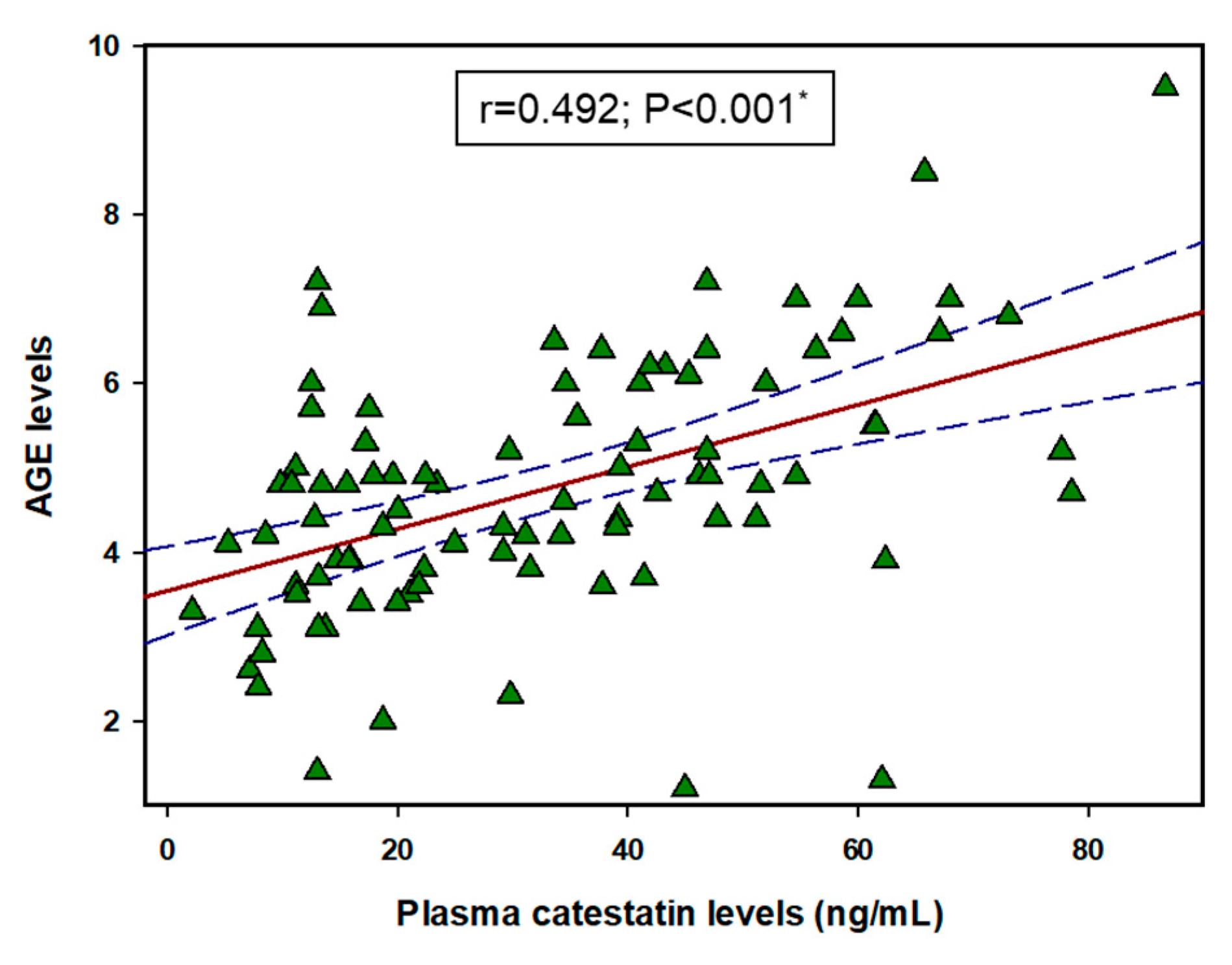
3.6. Correlation between CST and AGEs
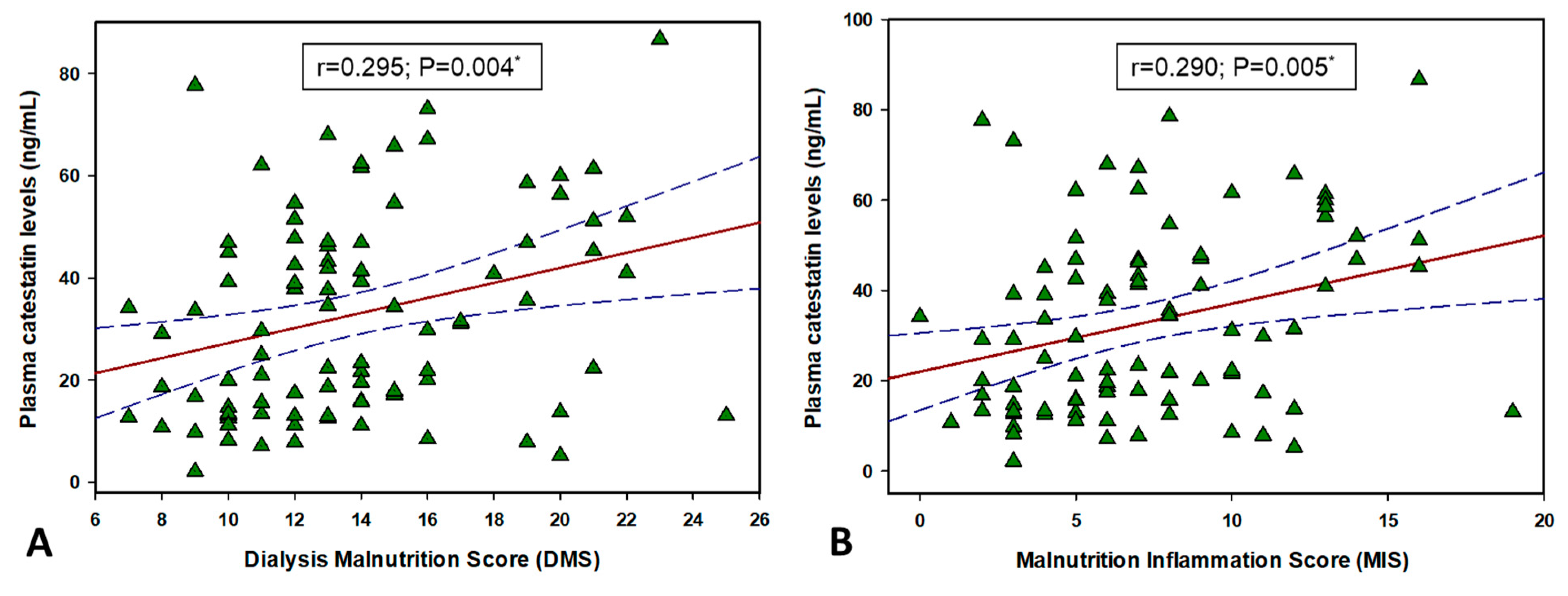
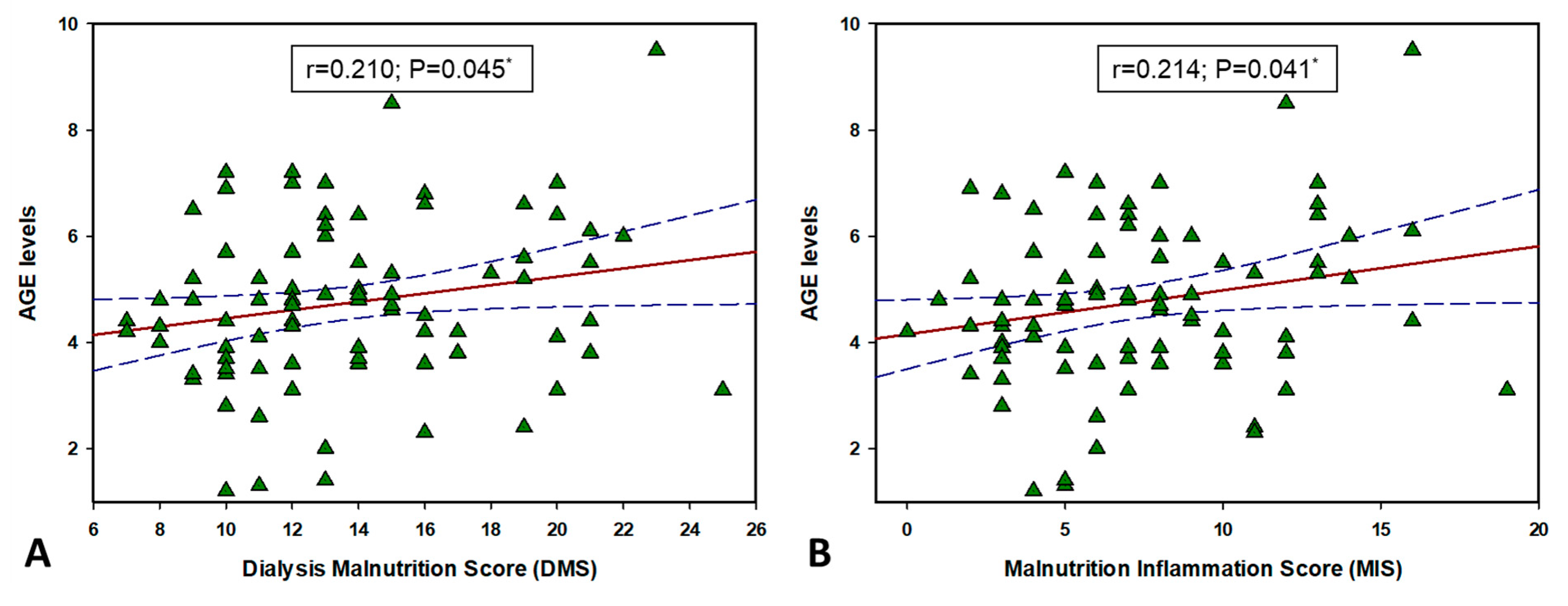
3.7. CST and AGEs Correlation with MIS and DMS
3.8. Multiple Linear Regression Model for Plasma CST Levels
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abbasi, M.A.; Chertow, G.M.; Hall, Y.N. End-stage renal disease. BMJ Clin. Evid. 2010, 2010, 2002. [Google Scholar]
- Hassanien, A.A.; Al-Shaikh, F.; Vamos, E.P.; Yadegarfar, G.; Majeed, A. Epidemiology of end-stage renal disease in the countries of the Gulf Cooperation Council: A systematic review. JRSM Short Rep. 2012, 3, 38. [Google Scholar] [CrossRef]
- El Nahas, A.M.; Bello, A.K. Chronic kidney disease: The global challenge. Lancet 2005, 365, 331–340. [Google Scholar] [CrossRef]
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D.R. Global prevalence of chronic kidney disease—A systematic review and meta-analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef] [PubMed]
- Ghaderian, S.B.; Hayati, F.; Shayanpour, S.; Beladi Mousavi, S.S. Diabetes and end-stage renal disease; a review article on new concepts. J. Renal Inj. Prev. 2015, 4, 28–33. [Google Scholar] [PubMed]
- Vadakedath, S.; Kandi, V. Dialysis: A review of the mechanisms underlying complications in the management of chronic renal failure. Cureus 2017, 9, e1603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mavrakanas, T.A.; Charytan, D.M. Cardiovascular complications in chronic dialysis patients. Curr. Opin. Nephrol. Hypertens. 2016, 25, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Yamagishi, S. Potential clinical utility of advanced glycation end product cross-link breakers in age- and diabetes-associated disorders. Rejuvenation Res. 2012, 15, 564–572. [Google Scholar] [CrossRef] [PubMed]
- Monnier, V.M. Nonenzymatic glycosylation, the Maillard reaction and the aging process. J. Gerontol. 1990, 45, B105–B111. [Google Scholar] [CrossRef] [PubMed]
- Fleming, T.H.; Humpert, P.M.; Nawroth, P.P.; Bierhaus, A. Reactive metabolites and AGE/RAGE-mediated cellular dysfunction affect the aging process: A mini-review. Gerontology 2011, 57, 435–443. [Google Scholar] [CrossRef]
- Fishman, S.L.; Sonmez, H.; Basman, C.; Singh, V.; Poretsky, L. The role of advanced glycation end-products in the development of coronary artery disease in patients with and without diabetes mellitus: A review. Mol. Med. 2018, 24, 59. [Google Scholar] [CrossRef] [PubMed]
- Beyan, H.; Riese, H.; Hawa, M.I.; Beretta, G.; Davidson, H.W.; Hutton, J.C.; Burger, H.; Schlosser, M.; Snieder, H.; Boehm, B.O.; et al. Glycotoxin and autoantibodies are additive environmentally determined predictors of type 1 diabetes: A twin and population study. Diabetes 2012, 61, 1192–1198. [Google Scholar] [CrossRef] [Green Version]
- Deluyker, D.; Evens, L.; Bito, V. Advanced glycation end products (AGEs) and cardiovascular dysfunction: Focus on high molecular weight AGEs. Amino Acids 2017, 49, 1535–1541. [Google Scholar] [CrossRef]
- Ribeiro, P.V.M.; Tavares, J.F.; Costa, M.A.C.; Matter, J.B.; Alfenas, R.C.G. Effect of reducing dietary advanced glycation end products on obesity-associated complications: A systematic review. Nutr. Rev. 2019, 77, 725–734. [Google Scholar] [CrossRef]
- Bohlender, J.M.; Franke, S.; Stein, G.; Wolf, G. Advanced glycation end products and the kidney. Am. J. Physiol. Renal Physiol. 2005, 289, F645–F659. [Google Scholar] [CrossRef]
- Fernando, D.H.; Forbes, J.M.; Angus, P.W.; Herath, C.B. Development and progression of non-alcoholic fatty liver disease: The role of advanced glycation end products. Int. J. Mol. Sci. 2019, 20, 5037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meerwaldt, R.; Zeebregts, C.J.; Navis, G.; Hillebrands, J.-L.; Lefrandt, J.D.; Smit, A.J. Accumulation of advanced glycation end products and chronic complications in ESRD treated by dialysis. Am. J. Kidney Dis. 2008, 53, 138–150. [Google Scholar] [CrossRef]
- Semba, R.D.; Fink, J.C.; Sun, K.; Windham, B.G.; Ferrucci, L. Plasma carboxymethyl-lysine, a dominant advanced glycation end product, is associated with chronic kidney disease: The Baltimore Longitudinal Study of Aging. J. Ren. Nutr. 2010, 20, 74–81. [Google Scholar] [CrossRef] [Green Version]
- Rabbani, N.; Thornalley, P.J. Advanced glycation end products in the pathogenesis of chronic kidney disease. Kidney Int. 2018, 93, 803–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liakopoulos, V.; Roumeliotis, S.; Gorny, X.; Eleftheriadis, T.; Mertens, P.R. Oxidative stress in patients undergoing peritoneal dialysis: A current review of the literature. Oxid. Med. Cell Longev. 2017, 2017, 3494867. [Google Scholar] [CrossRef] [Green Version]
- Roumeliotis, S.; Dounousi, E.; Salmas, M.; Eleftheriadis, T.; Liakopoulos, V. Unfavorable effects of peritoneal dialysis solutions on the peritoneal membrane: The role of oxidative stress. Biomolecules 2020, 10, 768. [Google Scholar] [CrossRef]
- Yamagishi, S.; Matsui, T. Advanced glycation end products, oxidative stress and diabetic nephropathy. Oxid. Med. Cell Longev. 2010, 3, 101–108. [Google Scholar] [CrossRef]
- Muntjewerff, E.M.; Dunkel, G.; Nicolasen, M.J.T.; Mahata, S.K.; van den Bogaart, G. Catestatin as a target for treatment of inflammatory diseases. Front. Immunol. 2018, 9, 2199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahata, S.K.; Mahata, M.; Fung, M.M.; O’Connor, D.T. Catestatin: A multifunctional peptide from chromogranin A. Regul. Pept. 2010, 162, 33–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahata, S.K.; Kiranmayi, M.; Mahapatra, N.R. Catestatin: A master regulator of cardiovascular functions. Curr. Med. Chem. 2018, 25, 1352–1374. [Google Scholar] [CrossRef] [PubMed]
- Avolio, E.; Mahata, S.K.; Mantuano, E.; Mele, M.; Alo, R.; Facciolo, R.M.; Talani, G.; Canonaco, M. Antihypertensive and neuroprotective effects of catestatin in spontaneously hypertensive rats: Interaction with GABAergic transmission in amygdala and brainstem. Neuroscience 2014, 270, 48–57. [Google Scholar] [CrossRef]
- Pei, Z.; Ma, D.; Ji, L.; Zhang, J.; Su, J.; Xue, W.; Chen, X.; Wang, W. Usefulness of catestatin to predict malignant arrhythmia in patients with acute myocardial infarction. Peptides 2014, 55, 131–135. [Google Scholar] [CrossRef]
- Liu, L.; Ding, W.; Li, R.; Ye, X.; Zhao, J.; Jiang, J.; Meng, L.; Wang, J.; Chu, S.; Han, X.; et al. Plasma levels and diagnostic value of catestatin in patients with heart failure. Peptides 2013, 46, 20–25. [Google Scholar] [CrossRef]
- Wang, X.; Xu, S.; Liang, Y.; Zhu, D.; Mi, L.; Wang, G.; Gao, W. Dramatic changes in catestatin are associated with hemodynamics in acute myocardial infarction. Biomarkers 2011, 16, 372–377. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, X.; Yang, C.; Su, X.; Yang, W.; Dai, Y.; Han, H.; Jiang, J.; Lu, L.; Wang, H.; et al. Decreased circulating catestatin levels are associated with coronary artery disease: The emerging anti-inflammatory role. Atherosclerosis 2019, 281, 78–88. [Google Scholar] [CrossRef]
- Xu, W.; Yu, H.; Wu, H.; Li, S.; Chen, B.; Gao, W. Plasma catestatin in patients with acute coronary syndrome. Cardiology 2017, 136, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Borovac, J.A.; D’Amario, D.; Bozic, J.; Glavas, D. Sympathetic nervous system activation and heart failure: Current state of evidence and the pathophysiology in the light of novel biomarkers. World J. Cardiol. 2020, 12, 373–408. [Google Scholar] [CrossRef]
- Zivkovic, P.M.; Matetic, A.; Tadin Hadjina, I.; Rusic, D.; Vilovic, M.; Supe-Domic, D.; Borovac, J.A.; Mudnic, I.; Tonkic, A.; Bozic, J. Plasma catestatin levels and arterial stiffness parameters are increased in patients with inflammatory bowel disease. J. Clin. Med. 2020, 9, 628. [Google Scholar] [CrossRef] [Green Version]
- Borovac, J.A.; Dogas, Z.; Supe-Domic, D.; Galic, T.; Bozic, J. Catestatin plasma levels are increased in male patients with obstructive sleep apnea. Sleep Breath. 2019, 23, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Rabbi, M.F.; Labis, B.; Metz-Boutigue, M.-H.; Bernstein, C.N.; Ghia, J.-E. Catestatin decreases macrophage function in two mouse models of experimental colitis. Biochem. Pharmacol. 2014, 89, 386–398. [Google Scholar] [CrossRef] [PubMed]
- Rabbi, M.F.; Eissa, N.; Munyaka, P.M.; Kermarrec, L.; Elgazzar, O.; Khafipour, E.; Bernstein, C.N.; Ghia, J.E. Reactivation of intestinal inflammation is suppressed by catestatin in a murine model of colitis via M1 macrophages and not the gut microbiota. Front. Immunol. 2017, 8, 985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, H.; Xian, W.; Geng, L.; Li, E.; Peng, Z.; Tian, J. Increased plasma level of catestatin might be associated with poor prognosis in hemodialysis patients. Int. Urol. Nephrol. 2017, 49, 1063–1069. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Kopple, J.D.; Block, G.; Humphreys, M.H. A malnutrition-inflammation score is correlated with morbidity and mortality in maintenance hemodialysis patients. Am. J. Kidney Dis. 2001, 38, 1251–1263. [Google Scholar] [CrossRef] [Green Version]
- Kalantar-Zadeh, K.; Kleiner, M.; Dunne, E.; Lee, G.H.; Luft, F.C. A modified quantitative subjective global assessment of nutrition for dialysis patients. Nephrol. Dial. Transplant. 1999, 14, 1732–1738. [Google Scholar] [CrossRef] [Green Version]
- Checheriţa, I.A.; Turcu, F.; Dragomirescu, R.F.; Ciocâlteu, A. Chronic complications in hemodialysis: Correlations with primary renal disease. Rom. J. Morphol. Embryol. 2010, 51, 21–26. [Google Scholar] [PubMed]
- Blagg, C.R. Long-term complications in hemodialysis. Saudi J. Kidney Dis. Transpl. 2001, 12, 487–493. [Google Scholar]
- Liakopoulos, V.; Roumeliotis, S.; Zarogiannis, S.; Eleftheriadis, T.; Mertens, P.R. Oxidative stress in hemodialysis: Causative mechanisms, clinical implications, and possible therapeutic interventions. Semin. Dial. 2019, 32, 58–71. [Google Scholar] [CrossRef]
- Rapa, S.F.; Di Iorio, B.R.; Campiglia, P.; Heidland, A.; Marzocco, S. Inflammation and oxidative stress in chronic kidney disease-potential therapeutic role of minerals, vitamins and plant-derived metabolites. Int. J. Mol. Sci. 2019, 21, 263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gluba-Brzozka, A.; Franczyk, B.; Olszewski, R.; Rysz, J. The influence of inflammation on anemia in CKD patients. Int. J. Mol. Sci. 2020, 21, 725. [Google Scholar] [CrossRef] [Green Version]
- Mohseni, S.; Emtenani, S.; Emtenani, S.; Asoodeh, A. Antioxidant properties of a human neuropeptide and its protective effect on free radical-induced DNA damage. J. Pept. Sci. 2014, 20, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Liao, F.; Zheng, Y.; Cai, J.; Fan, J.; Wang, J.; Yang, J.; Cui, Q.; Xu, G.; Tang, C.; Geng, B. Catestatin attenuates endoplasmic reticulum induced cell apoptosis by activation type 2 muscarinic acetylcholine receptor in cardiac ischemia/reperfusion. Sci. Rep. 2015, 5, 16590. [Google Scholar] [CrossRef] [Green Version]
- Perrelli, M.G.; Tullio, F.; Angotti, C.; Cerra, M.; Angelone, T.; Tota, B.; Alloatti, G.; Penna, C.; Pagliaro, P. Catestatin reduces myocardial ischaemia/reperfusion injury: Involvement of PI3K/Akt, PKCs, mitochondrial KATP channels and ROS signalling. Pflug. Arch.-Eur. J. Physiol. 2013, 465, 1031–1040. [Google Scholar] [CrossRef] [PubMed]
- Chu, S.Y.; Peng, F.; Wang, J.; Liu, L.; Meng, L.; Zhao, J.; Han, X.N.; Ding, W.H. Catestatin in defense of oxidative-stress-induced apoptosis: A novel mechanism by activating the beta2 adrenergic receptor and PKB/Akt pathway in ischemic-reperfused myocardium. Peptides 2020, 123, 170200. [Google Scholar] [CrossRef] [PubMed]
- Aung, G.; Niyonsaba, F.; Ushio, H.; Kajiwara, N.; Saito, H.; Ikeda, S.; Ogawa, H.; Okumura, K. Catestatin, a neuroendocrine antimicrobial peptide, induces human mast cell migration, degranulation and production of cytokines and chemokines. Immunology 2011, 132, 527–539. [Google Scholar] [CrossRef] [PubMed]
- Wolowiec, L.; Rogowicz, D.; Banach, J.; Gilewski, W.; Sinkiewicz, W.; Grzesk, G. Catestatin as a new prognostic marker in stable patients with heart failure with reduced ejection fraction in two-year follow-up. Dis. Markers 2020, 2020, 8847211. [Google Scholar] [CrossRef]
- Mahata, S.K.; O’Connor, D.T.; Mahata, M.; Yoo, S.H.; Taupenot, L.; Wu, H.; Gill, B.M.; Parmer, R.J. Novel autocrine feedback control of catecholamine release: A discrete chromogranin a fragment is a noncompetitive nicotinic cholinergic antagonist. J. Clin. Invest. 1997, 100, 1623–1633. [Google Scholar] [CrossRef] [Green Version]
- Taylor, C.V.; Taupenot, L.; Mahata, S.K.; Mahata, M.; Wu, H.; Yasothornsrikul, S.; Toneff, T.; Caporale, C.; Jiang, Q.; Parmer, R.J.; et al. Formation of the catecholamine release-inhibitory peptide catestatin from chromogranin A: Determination of proteolytic cleavage sites in hormone storage granules. J. Biol. Chem. 2000, 275, 22905–22915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.C.; Taylor, C.V.; Gaucher, S.P.; Toneff, T.; Taupenot, L.; Yasothornsrikul, S.; Mahata, S.K.; Sei, C.; Parmer, R.J.; Neveu, J.M.; et al. Primary sequence characterization of catestatin intermediates and peptides defines proteolytic cleavage sites utilized for converting chromogranin A into active catestatin secreted from neuroendocrine chromaffin cells. Biochemistry 2003, 42, 6938–6946. [Google Scholar] [CrossRef]
- Salem, R.M.; Cadman, P.E.; Chen, Y.; Rao, F.; Wen, G.; Hamilton, B.A.; Rana, B.K.; Smith, D.W.; Stridsberg, M.; Ward, H.J.; et al. Chromogranin A polymorphisms are associated with hypertensive renal disease. J. Am. Soc. Nephrol. 2008, 19, 600–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bech, P.R.; Ramachandran, R.; Dhillo, W.S.; Martin, N.M.; Bloom, S.R. Quantifying the effects of renal impairment on plasma concentrations of the neuroendocrine neoplasia biomarkers Chromogranin A, Chromogranin B, and Cocaine- and Amphetamine-regulated transcript. Clin. Chem. 2012, 58, 941–943. [Google Scholar] [CrossRef] [Green Version]
- Hsiao, R.J.; Mezger, M.S.; O’Connor, D.T. Chromogranin A in uremia: Progressive retention of immunoreactive fragments. Kidney Int. 1990, 37, 955–964. [Google Scholar] [CrossRef] [Green Version]
- Tramonti, G.; Ferdeghini, M.; Annichiarico, C.; Norpoth, M.; Donadio, C.; Bianchi, R.; Bianchi, C. Relationship between renal function and blood level of chromogranin A. Ren. Fail. 2001, 23, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Mahata, M.; Rao, F.; Khandrika, S.; Courel, M.; Fung, M.M.; Zhang, K.; Stridsberg, M.; Ziegler, M.G.; Hamilton, B.A.; et al. Chromogranin A regulates renal function by triggering Weibel-Palade body exocytosis. J. Am. Soc. Nephrol. 2009, 20, 1623–1632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stinghen, A.E.M.; Massy, Z.A.; Vlassara, H.; Striker, G.E.; Boullier, A. Uremic toxicity of advanced glycation end products in CKD. J. Am. Soc. Nephrol. 2016, 27, 354–370. [Google Scholar] [CrossRef] [Green Version]
- Meerwaldt, R.; Hartog, J.W.; Graaff, R.; Huisman, R.J.; Links, T.P.; den Hollander, N.C.; Thorpe, S.R.; Baynes, J.W.; Navis, G.; Gans, R.O.; et al. Skin autofluorescence, a measure of cumulative metabolic stress and advanced glycation end products, predicts mortality in hemodialysis patients. J. Am. Soc. Nephrol. 2005, 16, 3687–3693. [Google Scholar] [CrossRef]
- McIntyre, N.J.; Chesterton, L.J.; John, S.G.; Jefferies, H.J.; Burton, J.O.; Taal, M.W.; Fluck, R.J.; McIntyre, C.W. Tissue-advanced glycation end product concentration in dialysis patients. Clin. J. Am. Soc. Nephrol. 2010, 5, 51–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Turco, S.; Basta, G. An update on advanced glycation endproducts and atherosclerosis. Biofactors 2012, 38, 266–274. [Google Scholar] [CrossRef]
- Gao, S.; Liu, J. Association between circulating oxidized low-density lipoprotein and atherosclerotic cardiovascular disease. Chronic. Dis. Transl. Med. 2017, 3, 89–94. [Google Scholar] [CrossRef]
- Hegab, Z.; Gibbons, S.; Neyses, L.; Mamas, M.A. Role of advanced glycation end products in cardiovascular disease. World J. Cardiol. 2012, 4, 90–102. [Google Scholar] [CrossRef] [Green Version]
- Leonardis, D.; Basta, G.; Mallamaci, F.; Cutrupi, S.; Pizzini, P.; Tripepi, R.; Tripepi, G.; De Caterina, R.; Zoccali, C. Circulating soluble receptor for advanced glycation end product (sRAGE) and left ventricular hypertrophy in patients with chronic kidney disease (CKD). Nutr. Metab. Cardiovasc. Dis. 2012, 22, 748–755. [Google Scholar] [CrossRef] [PubMed]
- Falcone, C.; Bozzini, S.; D’Angelo, A.; Matrone, B.; Colonna, A.; Benzi, A.; Paganini, E.M.; Falcone, R.; Pelissero, G. Plasma levels of soluble receptor for advanced glycation end products and coronary atherosclerosis: Possible correlation with clinical presentation. Dis. Markers 2013, 35, 135–140. [Google Scholar] [CrossRef]
- Strozecki, P.; Kurowski, R.; Flisinski, M.; Stefanska, A.; Odrowaz-Sypniewska, G.; Manitius, J. Advanced glycation end products and arterial stiffness in patients with diabetic nephropathy and patients with chronic kidney disease without diabetes. Pol. Arch. Med. Wewn 2013, 123, 609–616. [Google Scholar] [CrossRef] [Green Version]
- Foley, R.N.; Parfrey, P.S.; Sarnak, M.J. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am. J. Kidney Dis. 1998, 32, S112–S119. [Google Scholar] [CrossRef] [PubMed]
- Liakopoulos, V.; Roumeliotis, S.; Gorny, X.; Dounousi, E.; Mertens, P.R. Oxidative stress in hemodialysis patients: A review of the literature. Oxid. Med. Cell. Longev. 2017, 2017, 3081856. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.F.; Chang, C.L.; Liou, S.Y. Increase in resting levels of superoxide anion in the whole blood of uremic patients on chronic hemodialysis. Blood Purif. 1998, 16, 290–300. [Google Scholar] [CrossRef]
- Nguyen, A.T.; Lethias, C.; Zingraff, J.; Herbelin, A.; Naret, C.; Descamps-Latscha, B. Hemodialysis membrane-induced activation of phagocyte oxidative metabolism detected in vivo and in vitro within microamounts of whole blood. Kidney Int. 1985, 28, 158–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duni, A.; Liakopoulos, V.; Roumeliotis, S.; Peschos, D.; Dounousi, E. Oxidative stress in the pathogenesis and evolution of chronic kidney disease: Untangling ariadne’s thread. Int. J. Mol. Sci. 2019, 20, 3711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalantar-Zadeh, K.; Ikizler, T.A.; Block, G.; Avram, M.M.; Kopple, J.D. Malnutrition-inflammation complex syndrome in dialysis patients: Causes and consequences. Am. J. Kidney Dis. 2003, 42, 864–881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibson, D.; Mehler, P.S. Anorexia Nervosa and the Immune System-A Narrative Review. J. Clin. Med. 2019, 8, 1915. [Google Scholar] [CrossRef] [Green Version]
- Kalantar-Zadeh, K. Recent advances in understanding the malnutrition-inflammation-cachexia syndrome in chronic kidney disease patients: What is next? Semin. Dial. 2005, 18, 365–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jonaidi, H.; Abbassi, L.; Yaghoobi, M.M.; Kaiya, H.; Denbow, D.M.; Kamali, Y.; Shojaei, B. The role of GABAergic system on the inhibitory effect of ghrelin on food intake in neonatal chicks. Neurosci. Lett. 2012, 520, 82–86. [Google Scholar] [CrossRef]
- Avolio, E.; Facciolo, R.M.; Alo, R.; Mele, M.; Carelli, A.; Canonaco, A.; Mosciaro, L.; Talani, G.; Biggio, G.; Sanna, E.; et al. Expression variations of Chromogranin A and α1,2,4 GABAAR in discrete limbic and brainstem areas rescue cardiovascular alterations. Neurosci. Res. 2013, 77, 8–15. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Hemodialysis Group (N = 91) | Control Group (N = 70) | p * |
|---|---|---|---|
| Male gender | 58 (63.7) | 34 (68.0) | 0.612 |
| Age (years) | 68.3 ± 12.6 | 67.2 ± 12.1 | 0.577 |
| Body weight (kg) | 74.9 ± 14.9 | 75.3 ± 14.7 | 0.865 |
| Body height (cm) | 174.1 ± 9.6 | 176.3 ± 8.1 | 0.125 |
| Body mass index (kg/m2) | 24.5 ± 4.8 | 23.9 ± 3.8 | 0.391 |
| Waist circumference (cm) | 98.7 ± 12.5 | 96.1 ± 11.1 | 0.171 |
| Hip circumference (cm) | 103.3 ± 10.7 | 100.6 ± 15.6 | 0.195 |
| Pre-dialysis systolic pressure (mmHg) | 135.1 ± 27.4 | − | − |
| Post-dialysis systolic pressure (mmHg) ‡ | 123.2 ± 27.5 | 118.5 ± 7.1 | 0.117 |
| Pre-dialysis diastolic pressure (mmHg) | 70.1 ± 16.1 | − | − |
| Post-dialysis diastolic pressure (mmHg) ‡ | 69.3 ± 14.7 | 72.1 ± 8.2 | 0.137 |
| Diabetes | 29 (31.9) | 14 (20.0) | 0.091 |
| Smoking | 28 (30.8) | 24 (34.3) | 0.636 |
| CKD duration (years) † | 11 (7.0–26.5) | − | − |
| Hemodialysis duration (years) | 4.0 (2.0–8.0) | − | − |
| Urine output (mL) | 200.0 (0–1075.0) | − | − |
| Erythropoietin therapy | 77 (84.6) | − | − |
| Arteriovenous fistula # | 48 (52.7) | − | − |
| Temporary CVC # | 27 (29.7) | − | − |
| Permanent CVC # | 16 (17.6) | − | − |
| Dialysis Malnutrition Score | 13.8 ± 4.0 | − | − |
| Malnutrition-Inflammation Score | 7.1 ± 3.8 | − | − |
| Parameter | Hemodialysis Group (N = 91) | Control Group (N = 70) | p * |
|---|---|---|---|
| Erythrocytes (×1012/L) | 3.7 ± 0.5 | 4.3 ± 0.6 | <0.001 |
| Hemoglobin (g/L) | 110.7 ± 10.6 | 137.5 ± 11.9 | <0.001 |
| Hematocrit | 0.34 ± 0.03 | 0.42 ± 0.05 | <0.001 |
| MCV (fL) | 91.9 ± 6.9 | 92.2 ± 6.2 | 0.776 |
| Plasma iron (µmol/L) | 11.4 ± 5.2 | 16.8 ± 4.8 | <0.001 |
| Total proteins (g/L) | 65.9 ± 5.2 | 71.5 ± 5.7 | <0.001 |
| Albumins (g/L) | 38.5 ± 3.0 | 43.1 ± 2.8 | <0.001 |
| Pre-dialysis creatinine (µmol/L) | 833.8 ± 186.1 | − | − |
| Post-dialysis creatinine (µmol/L)‡ | 335.5 ± 103.5 | 82.8 ± 16.8 † | <0.001 |
| Pre-dialysis urea (mmol/L) | 23.8 ± 6.2 | − | − |
| Post-dialysis urea (mmol/L) ‡ | 8.1 ± 3.5 | 6.2 ± 2.1 † | <0.001 |
| Pre-dialysis potassium (mmol/L) | 5.2 ± 0.8 | − | − |
| Post-dialysis potassium (mmol/L) ‡ | 3.5 ± 0.3 | 4.3 ± 0.4 † | <0.001 |
| Uric acid (µmol/L) | 345.2 ± 74.6 | 312.5 ± 68.4 | 0.005 |
| Sodium (mmol/L) | 138.4 ± 3.2 | 139.6 ± 3.4 | 0.024 |
| Calcium (mmol/L) | 2.27 ± 0.17 | 2.32 ± 0.12 | 0.038 |
| Phosphates (mmol/L) | 1.6 ± 0.5 | 1.1 ± 0.3 | <0.001 |
| Chlorides (mmol/L) | 101.9 ± 3.2 | 102.2 ± 3.3 | 0.566 |
| PTH (pmol/L) | 37.0 (17.0–56.0) | 5.0 (4.0–6.0) | <0.001 |
| Fasting glucose (mmol/L) | 6.7 ± 3.1 | 5.5 ± 0.7 | 0.003 |
| CRP (mg/L) | 4.5 (1.5–8.5) | 0.8 (0.4–1.8) | <0.001 |
| Total cholesterol (mmol/L) | 4.4 ± 3.1 | 4.6 ± 2.9 | 0.677 |
| HDL-cholesterol (mmol/L) | 1.08 ± 0.36 | 1.12 ± 0.24 | 0.424 |
| LDL-cholesterol (mmol/L) | 2.2 ± 1.0 | 2.4 ± 1.1 | 0.109 |
| Triglycerides (mmol/L) | 1.96 ± 1.04 | 1.84 ± 0.98 | 0.458 |
| Parameter | CST r (p *) | AGE r (p *) |
|---|---|---|
| Total proteins (g/L) | −0.083 (0.432) | −0.210 (0.045) |
| Albumins (g/L) | −0.159 (0.133) | −0.167 (0.113) |
| Pre-dialysis creatinine (µmol/L) | −0.245 (0.019) | −0.048 (0.651) |
| Post-dialysis creatinine (µmol/L) | −0.225 (0.032) | −0.112 (0.288) |
| Pre-dialysis urea (mmol/L) | −0.198 (0.060) | −0.216 (0.039) |
| Post-dialysis urea (mmol/L) | −0.143 (0.176) | −0.241 (0.021) |
| Pre-dialysis potassium (mmol/L) | −0.094 (0.373) | −0.002 (0.983) |
| Post-dialysis potassium (mmol/L) | −0.122 (0.250) | −0.205 (0.051) |
| CRP (mg/L) | −0.086 (0.419) | 0.033 (0.758) |
| Total cholesterol (mmol/L) | 0.170 (0.108) | 0.164 (0.121) |
| HDL-cholesterol (mmol/L) | 0.002 (0.988) | 0.098 (0.354) |
| LDL-cholesterol (mmol/L) | 0.040 (0.706) | −0.214 (0.041) |
| Triglycerides (mmol/L) | −0.106 (0.319) | −0.211 (0.045) |
| Pre-dialysis systolic pressure (mmHg) | −0.059 (0.577) | −0.069 (0.514) |
| Post-dialysis systolic pressure (mmHg) | −0.009 (0.931) | 0.112 (0.289) |
| Pre-dialysis diastolic pressure (mmHg) | 0.018 (0.865) | 0.021 (0.846) |
| Post-dialysis diastolic pressure (mmHg) | 0.084 (0.427) | 0.107 (0.311) |
| Age (years) | 0.290 (0.005) | 0.116 (0.272) |
| CKD duration (years)† | 0.089 (0.399) | 0.111 (0.296) |
| Hemodialysis duration (years) | 0.068 (0.524) | 0.060 (0.575) |
| Body mass index (kg/m2) | −0.172 (0.103) | −0.249 (0.017) |
| Waist circumference (cm) | 0.066 (0.531) | −0.084 (0.426) |
| Variable | β * | SE † | t-Value | p |
|---|---|---|---|---|
| Gender | −3.36 | 28.1 | −0.85 | 0.394 |
| Age (years) | 0.31 | 0.14 | 2.06 | 0.042 |
| Body mass index (kg/m2) | −0.97 | 0.65 | 0.14 | 0.139 |
| Waist circumference (cm) | 0.49 | 0.24 | 2.0 | 0.048 |
| Hemodialysis duration (years) | 0.25 | 0.24 | 1.04 | 0.299 |
| Malnutrition-Inflammation Score | 0.95 | 1.11 | 0.85 | 0.393 |
| Dialysis Malnutrition Score | −0.01 | 1.05 | −0.01 | 0.986 |
| AGE levels | 5.20 | 1.25 | 4.16 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luketin, M.; Mizdrak, M.; Boric-Skaro, D.; Martinovic, D.; Tokic, D.; Vilovic, M.; Supe-Domic, D.; Ticinovic Kurir, T.; Bozic, J. Plasma Catestatin Levels and Advanced Glycation End Products in Patients on Hemodialysis. Biomolecules 2021, 11, 456. https://doi.org/10.3390/biom11030456
Luketin M, Mizdrak M, Boric-Skaro D, Martinovic D, Tokic D, Vilovic M, Supe-Domic D, Ticinovic Kurir T, Bozic J. Plasma Catestatin Levels and Advanced Glycation End Products in Patients on Hemodialysis. Biomolecules. 2021; 11(3):456. https://doi.org/10.3390/biom11030456
Chicago/Turabian StyleLuketin, Mirko, Maja Mizdrak, Dijana Boric-Skaro, Dinko Martinovic, Daria Tokic, Marino Vilovic, Daniela Supe-Domic, Tina Ticinovic Kurir, and Josko Bozic. 2021. "Plasma Catestatin Levels and Advanced Glycation End Products in Patients on Hemodialysis" Biomolecules 11, no. 3: 456. https://doi.org/10.3390/biom11030456