
Prepubertal Periodontitis in a Patient with Combined Classical and Periodontal Ehlers–Danlos Syndrome

 and
and
Abstract
:1. Introduction
2. Case Report
2.1. Medical History and Physical Examination of the Index Patient
2.2. Family History
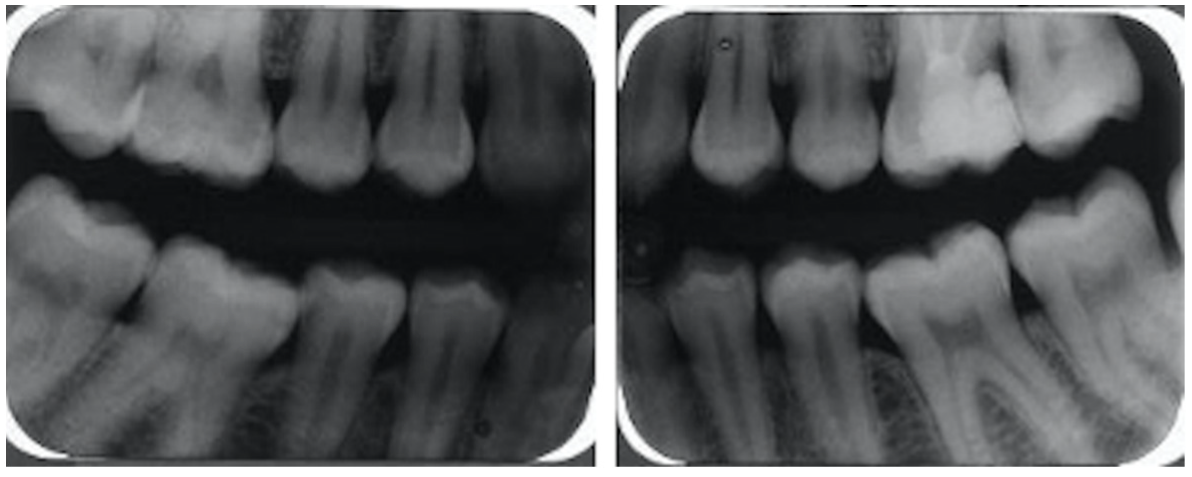
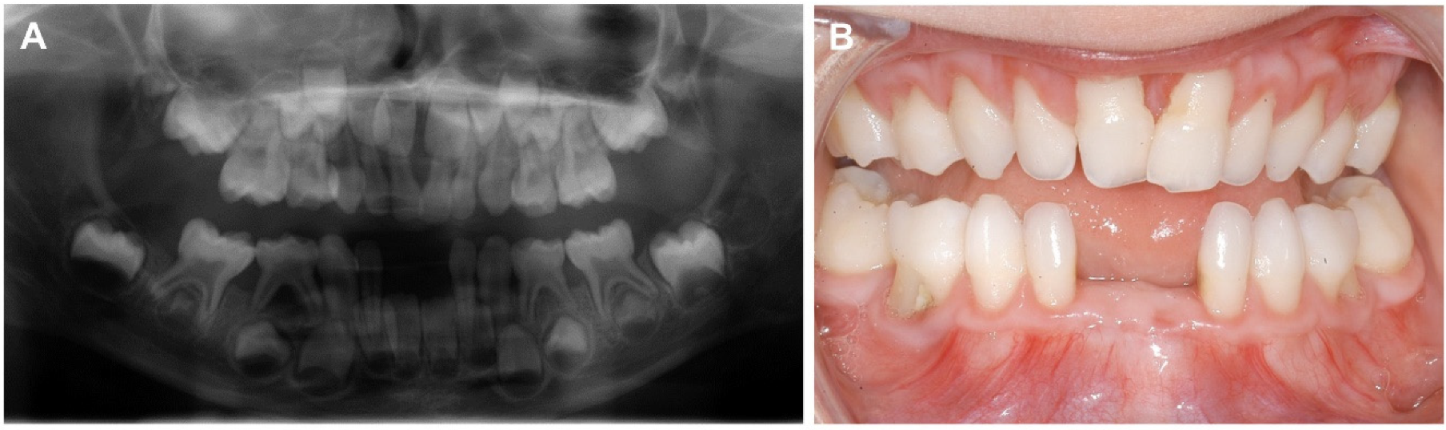
2.3. Oral Examination
2.4. Molecular Analysis and Findings
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malfait, F.; Francomano, C.; Byers, P.; Belmont, J.; Berglund, B.; Black, J.; Bloom, L.; Bowen, J.M.; Brady, A.F.; Burrows, N.P.; et al. The 2017 international classification of the Ehlers-Danlos syndromes. Am. J. Med. Genet. C Semin. Med. Genet. 2017, 175, 8–26. [Google Scholar] [CrossRef] [Green Version]
- Morlino, S.; Micale, L.; Ritelli, M.; Rohrbach, M.; Zoppi, N.; Vandersteen, A.; Mackay, S.; Agolini, E.; Cocciadiferro, D.; Sasaki, E.; et al. COL1-related overlap disorder: A novel connective tissue disorder incorporating the osteogenesis imperfecta/Ehlers-Danlos syndrome overlap. Clin. Genet. 2020, 97, 396–406. [Google Scholar] [CrossRef]
- Blackburn, P.R.; Xu, Z.; Tumelty, K.E.; Zhao, R.W.; Monis, W.J.; Harris, K.G.; Gass, J.M.; Cousin, M.A.; Boczek, N.J.; Mitkov, M.V.; et al. Bi-allelic Alterations in AEBP1 Lead to Defective Collagen Assembly and Connective Tissue Structure Resulting in a Variant of Ehlers-Danlos Syndrome. Am. J. Hum. Genet. 2018, 102, 696–705. [Google Scholar] [CrossRef] [Green Version]
- Beighton, P.; de Paepe, A.; Danks, D.; Finidori, G.; Gedde-Dahl, T.; Goodman, R.; Hall, J.G.; Hollister, D.W.; Horton, W.; McKusick, V.A.; et al. International Nosology of Heritable Disorders of Connective Tissue, Berlin, 1986. Am. J. Med. Genet. 1988, 29, 581–594. [Google Scholar] [CrossRef]
- Beighton, P.; De Paepe, A.; Steinmann, B.; Tsipouras, P.; Wenstrup, R.J. Ehlers-Danlos syndromes: Revised nosology, Villefranche, 1997. Ehlers-Danlos National Foundation (USA) and Ehlers-Danlos Support Group (UK). Am. J. Med. Genet. 1998, 77, 31–37. [Google Scholar] [CrossRef]
- Kapferer-Seebacher, I.; Pepin, M.; Werner, R.; Aitman, T.J.; Nordgren, A.; Stoiber, H.; Thielens, N.; Gaboriaud, C.; Amberger, A.; Schossig, A.; et al. Periodontal Ehlers-Danlos Syndrome Is Caused by Mutations in C1R and C1S, which Encode Subcomponents C1r and C1s of Complement. Am. J. Hum. Genet. 2016, 99, 1005–1014. [Google Scholar] [CrossRef] [Green Version]
- Kapferer-Seebacher, I.; Oakley-Hannibal, E.; Lepperdinger, U.; Johnson, D.; Ghali, N.; Brady, A.F.; Sobey, G.J.; Zschocke, J.; Van Dijk, F.S. Prospective clinical investigations of children with periodontal Ehlers–Danlos syndrome identify generalized lack of attached gingiva as a pathognomonic feature. Genet. Med. 2020. [Google Scholar] [CrossRef]
- Gröbner, R.; Kapferer-Seebacher, I.; Amberger, A.; Redolfi, R.; Dalonneau, F.; Björck, E.; Milnes, D.; Bally, I.; Rossi, V.; Thielens, N.; et al. C1R Mutations Trigger Constitutive Complement 1 Activation in Periodontal Ehlers-Danlos Syndrome. Front. Immunol. 2019, 5, 2537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajishengallis, G. Role of complement in host-microbe homeostasis of the periodontium. Semin. Immunol. 2013, 25, 65–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isola, G.; Polizzi, A.; Patini, R.; Ferlito, S.; Alibrandi, A.; Palazzo, G. Association among serum and salivary A. actinomycetemcomitans specific immunoglobulin antibodies and periodontitis. BMC Oral Health 2020, 20, 283. [Google Scholar] [CrossRef]
- Chen, M.; Ding, M.; Li, Y.; Zhong, X.; Liu, S.; Guo, Z.; Yin, X.; Fu, S.; Ye, J. The complement component 1 q (C1q) in Nile tilapia (Oreochromis niloticus): Functional characterization in host defense against bacterial infection and effect on cytokine response in macrophages. Dev. Comp. Immunol. 2018, 87, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Lo Giudice, A.; Polizzi, A.; Alibrandi, A.; Murabito, P.; Indelicato, F. Identification of the different salivary Interleukin-6 profiles in patients with periodontitis: A cross-sectional study. Arch. Oral Biol. 2020, 122, 104997. [Google Scholar] [CrossRef] [PubMed]
- Albandar, J.M.; Susin, C.; Hughes, F.J. Manifestations of systemic diseases and conditions that affect the periodontal attachment apparatus: Case definitions and diagnostic considerations. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S171–S189. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Yang, J.; Zhao, J.; Wu, J.R.; Zhang, X.; Leung, W.K.; Sun, W.B. A Chinese family with periodontal Ehlers-Danlos syndrome associated with missense mutation in the C1R gene. J. Clin. Periodontol. 2018, 45, 1311–1318. [Google Scholar] [CrossRef] [PubMed]
- Brinkmann, J.C.; Garcia-Gil, I.; Lobato-Pena, D.M.; Martinez-Mera, C.; Suarez-Garcia, M.J.; Martinez-Gonzalez, J.M.; Crespo, M.R. The key role of the dental practitioner in early diagnosis of periodontal Ehlers-Danlos syndromes: A rare case report of siblings. Quintessence Int. 2020, 51, 9. [Google Scholar] [CrossRef]
- Kapferer-Seebacher, I.; Waisfisz, Q.; Boesch, S.; Bronk, M.; van Tintelen, P.; Gizewski, E.R.; Groebner, R.; Zschocke, J.; van der Knaap, M.S. Periodontal Ehlers-Danlos syndrome is associated with leukoencephalopathy. Neurogenetics 2019, 20, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Kapferer-Seebacher, I.; Lundberg, P.; Malfait, F.; Zschocke, J. Periodontal manifestations of Ehlers-Danlos syndromes: A systematic review. J. Clin. Periodontol. 2017, 44, 1088–1100. [Google Scholar] [CrossRef]
- Pope, F.M.; Komorowska, A.; Lee, K.W.; Speight, P.; Zorawska, H.; Ranta, H.; Coonar, H.S.; MacKenzie, J.L. Ehlers Danlos syndrome type I with novel dental features. J. Oral Pathol. Med. 1992, 21, 418–421. [Google Scholar] [CrossRef]
- Cho, S.Y. Ehlers-Danlos syndrome (classic type): Report of a case presenting with an unusual dental anomaly. Prim. Dent. Care 2011, 18, 167–170. [Google Scholar] [CrossRef]
- Hakki, S.S.; Aktas, D.; Alanay, Y.; Avunduk, M.C.; Hakki, E.E. Dental Findings and Mutational Analysis of a Case with Ehlers-Danlos Syndrome. J. Dent. Oral Biol. 2017, 2, 5. [Google Scholar]
- Hanisch, M.; Hoffmann, T.; Bohner, L.; Hanisch, L.; Benz, K.; Kleinheinz, J.; Jackowski, J. Rare Diseases with Periodontal Manifestations. Int. J. Environ. Res. Public Health 2019, 16, 867. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, K.R.; Gui, J.; Dinulos, M.B.; Chou, R.C. Ehlers-Danlos syndrome hypermobility type is associated with rheumatic diseases. Sci. Rep. 2017, 7, 39636. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Proband IV:2 | Mother III:2 | Grandfather II:2 | |
|---|---|---|---|
| Major criteria of classical EDS | |||
| Joint hypermobility | + | + | + |
| Hyperelastic and soft skin | + | + | − |
| Atrophic scars | + | + | n.a. |
| Major criteria of periodontal EDS | |||
| Early severe periodontitis | + | − | − |
| Lack of attached gingiva | + | − | n.a. |
| Pretibial hyperpigmentation | + | − | − |
| Minor criteria of classical and / or periodontal EDS | |||
| Acrogeric face and hands | − | − | − |
| Myopia | − | + | − |
| Blue sclerae | + | − | |
| Ectopia lentis | − | − | − |
| epicanthic folds | − | + | |
| Arachnodactyly | − | − | − |
| multiple subcutaneous papules | + | + | |
| Easy bruising | + | + | + |
| Poor wound healing | + | + | + |
| dilatation of aorta | − | − | n.a. |
| Hernias | − | umbilical hernia | − |
| Organ rupture | − | − | − |
| Recurrent infections | + | + | + |
| Involvement of heart valves | hypermobile mitral valve (no prolapse) | n.a. | n.a. |
| Luxation of knee caps | + | + | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stock, F.; Hanisch, M.; Lechner, S.; Biskup, S.; Bohring, A.; Zschocke, J.; Kapferer-Seebacher, I. Prepubertal Periodontitis in a Patient with Combined Classical and Periodontal Ehlers–Danlos Syndrome. Biomolecules 2021, 11, 149. https://doi.org/10.3390/biom11020149
Stock F, Hanisch M, Lechner S, Biskup S, Bohring A, Zschocke J, Kapferer-Seebacher I. Prepubertal Periodontitis in a Patient with Combined Classical and Periodontal Ehlers–Danlos Syndrome. Biomolecules. 2021; 11(2):149. https://doi.org/10.3390/biom11020149
Chicago/Turabian StyleStock, Friedrich, Marcel Hanisch, Sarah Lechner, Saskia Biskup, Axel Bohring, Johannes Zschocke, and Ines Kapferer-Seebacher. 2021. "Prepubertal Periodontitis in a Patient with Combined Classical and Periodontal Ehlers–Danlos Syndrome" Biomolecules 11, no. 2: 149. https://doi.org/10.3390/biom11020149