

The Association between Maternal Urinary Phthalate Concentrations and Blood Pressure in Pregnancy: A Systematic Review and Meta-Analysis
 and
and
Abstract
:1. Introduction
2. Materials and Methods
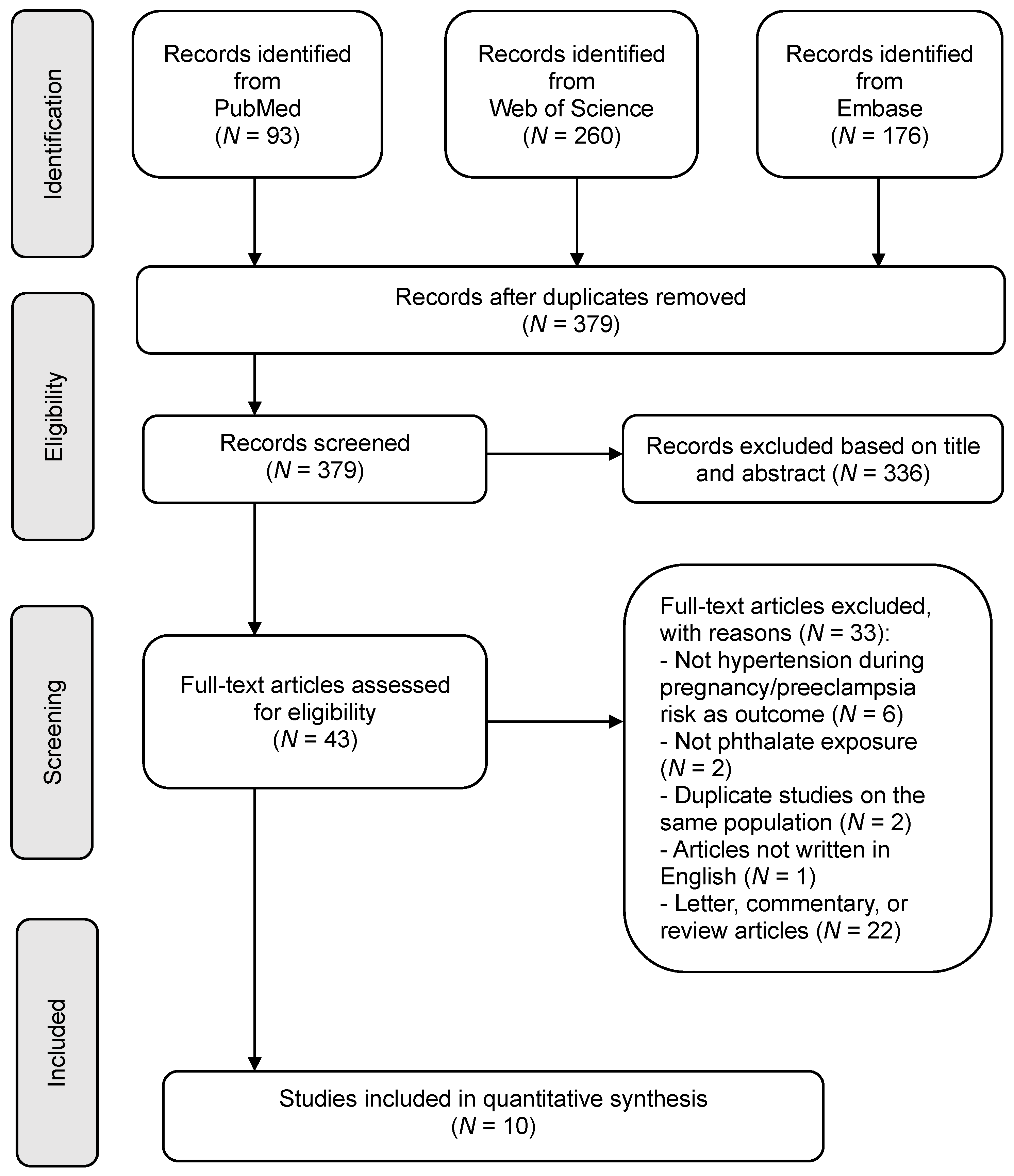
2.1. Search Strategy
2.2. Inclusion and Exclusion Criterion
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
3. Results
3.1. Study Characteristics
3.2. Main Meta-Analysis Findings
3.2.1. Phthalates Exposure during Pregnancy and BP
3.2.2. Phthalates Exposure during Pregnancy and Risk of HDP
3.3. Sensitivity Analysis and Publication Bias
4. Discussion
4.1. Strengths and Limitations
4.2. Recommendations for Future Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Roberts, C.L.; Ford, J.B.; Algert, C.S.; Antonsen, S.; Chalmers, J.; Cnattingius, S.; Gokhale, M.; Kotelchuck, M.; Melve, K.K.; Langridge, A.; et al. Population-based trends in pregnancy hypertension and pre-eclampsia: An international comparative study. BMJ Open 2011, 1, e000101. [Google Scholar] [CrossRef] [Green Version]
- Say, L.; Chou, D.; Gemmill, A.; Tuncalp, O.; Moller, A.B.; Daniels, J.; Gulmezoglu, A.M.; Temmerman, M.; Alkema, L. Global causes of maternal death: A WHO systematic analysis. Lancet Glob Health 2014, 2, e323–e333. [Google Scholar] [CrossRef] [Green Version]
- Bramham, K.; Parnell, B.; Nelson-Piercy, C.; Seed, P.T.; Poston, L.; Chappell, L.C. Chronic hypertension and pregnancy outcomes: Systematic review and meta-analysis. BMJ 2014, 348, g2301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umesawa, M.; Kobashi, G. Epidemiology of hypertensive disorders in pregnancy: Prevalence, risk factors, predictors and prognosis. Hypertens. Res. 2017, 40, 213–220. [Google Scholar] [CrossRef]
- Wei, J.; Liu, C.X.; Gong, T.T.; Wu, Q.J.; Wu, L. Cigarette smoking during pregnancy and preeclampsia risk: A systematic review and meta-analysis of prospective studies. Oncotarget 2015, 6, 43667–43678. [Google Scholar] [CrossRef] [PubMed]
- Ye, C.; Ruan, Y.; Zou, L.; Li, G.; Li, C.; Chen, Y.; Jia, C.; Megson, I.L.; Wei, J.; Zhang, W. The 2011 survey on hypertensive disorders of pregnancy (HDP) in China: Prevalence, risk factors, complications, pregnancy and perinatal outcomes. PLoS ONE 2014, 9, e100180. [Google Scholar] [CrossRef] [Green Version]
- Giovanoulis, G.; Bui, T.; Xu, F.; Papadopoulou, E.; Padilla-Sanchez, J.A.; Covaci, A.; Haug, L.S.; Cousins, A.P.; Magner, J.; Cousins, I.T.; et al. Multi-pathway human exposure assessment of phthalate esters and DINCH. Environ. Int. 2018, 112, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Zota, A.R.; Calafat, A.M.; Woodruff, T.J. Temporal trends in phthalate exposures: Findings from the National Health and Nutrition Examination Survey, 2001–2010. Environ. Health Perspect. 2014, 122, 235–241. [Google Scholar] [CrossRef] [Green Version]
- Cantonwine, D.E.; Meeker, J.D.; Ferguson, K.K.; Mukherjee, B.; Hauser, R.; McElrath, T.F. Urinary Concentrations of Bisphenol A and Phthalate Metabolites Measured during Pregnancy and Risk of Preeclampsia. Environ. Health Perspect. 2016, 124, 1651–1655. [Google Scholar] [CrossRef] [Green Version]
- Trasande, L.; Sathyanarayana, S.; Spanier, A.J.; Trachtman, H.; Attina, T.M.; Urbina, E.M. Urinary phthalates are associated with higher blood pressure in childhood. J. Pediatr. 2013, 163, 747–753.e741. [Google Scholar] [CrossRef] [Green Version]
- Varshavsky, J.R.; Morello-Frosch, R.; Woodruff, T.J.; Zota, A.R. Dietary sources of cumulative phthalates exposure among the U.S. general population in NHANES 2005–2014. Environ. Int. 2018, 115, 417–429. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.C.; Liao, K.W.; Chang, J.W.; Chan, S.H.; Lee, C.C. Characterization of phthalates exposure and risk for cosmetics and perfume sales clerks. Environ. Pollut. 2018, 233, 577–587. [Google Scholar] [CrossRef] [PubMed]
- Werner, E.F.; Braun, J.M.; Yolton, K.; Khoury, J.C.; Lanphear, B.P. The association between maternal urinary phthalate concentrations and blood pressure in pregnancy: The HOME Study. Environ. Health 2015, 14, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Philips, E.M.; Trasande, L.; Kahn, L.G.; Gaillard, R.; Steegers, E.A.P.; Jaddoe, V.W.V. Early pregnancy bisphenol and phthalate metabolite levels, maternal hemodynamics and gestational hypertensive disorders. Hum. Reprod. 2019, 34, 365–373. [Google Scholar] [CrossRef]
- Warembourg, C.; Basagana, X.; Seminati, C.; de Bont, J.; Granum, B.; Lyon-Caen, S.; Manzano-Salgado, C.B.; Pin, I.; Sakhi, A.K.; Siroux, V.; et al. Exposure to phthalate metabolites, phenols and organophosphate pesticide metabolites and blood pressure during pregnancy. Int. J. Hyg. Environ. Health 2019, 222, 446–454. [Google Scholar] [CrossRef]
- Gao, H.; Zhu, B.B.; Huang, K.; Zhu, Y.D.; Yan, S.Q.; Wu, X.Y.; Han, Y.; Sheng, J.; Cao, H.; Zhu, P.; et al. Effects of single and combined gestational phthalate exposure on blood pressure, blood glucose and gestational weight gain: A longitudinal analysis. Environ. Int. 2021, 155, 106677. [Google Scholar] [CrossRef]
- Han, X.; Li, J.; Wang, Y.; Xu, S.; Li, Y.; Liu, H.; Zhou, Y.; Zhao, H.; Fang, J.; Cai, Z.; et al. Association between phthalate exposure and blood pressure during pregnancy. Ecotoxicol. Environ. Saf. 2020, 189, 109944. [Google Scholar] [CrossRef]
- Morgan, R.L.; Whaley, P.; Thayer, K.A.; Schunemann, H.J. Identifying the PECO: A framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ. Int. 2018, 121, 1027–1031. [Google Scholar] [CrossRef]
- Wells, S.M.; Buford, M.C.; Migliaccio, C.T.; Holian, A. Elevated asymmetric dimethylarginine alters lung function and induces collagen deposition in mice. Am. J. Respir. Cell Mol. Biol. 2009, 40, 179–188. [Google Scholar] [CrossRef] [Green Version]
- Xing, Y.; Ma, Q.; Ma, X.; Wang, C.; Zhang, D.; Sun, Y. CHADS2 score has a better predictive value than CHA2DS2-VASc score in elderly patients with atrial fibrillation. Clin. Interv. Aging 2016, 11, 941–946. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harbord, R.M.; Egger, M.; Sterne, J.A. A modified test for small-study effects in meta-analyses of controlled trials with binary endpoints. Stat. Med. 2006, 25, 3443–3457. [Google Scholar] [CrossRef] [PubMed]
- Bedell, S.M.; Lyden, G.R.; Sathyanarayana, S.; Barrett, E.S.; Ferguson, K.K.; Santilli, A.; Bush, N.R.; Swan, S.H.; McElrath, T.F.; Nguyen, R.H.N. First- and Third-Trimester Urinary Phthalate Metabolites in the Development of Hypertensive Diseases of Pregnancy. Int. J. Environ. Res. Public Health 2021, 18, 10627. [Google Scholar] [CrossRef]
- Vuong, A.M.; Braun, J.M.; Sjodin, A.; Calafat, A.M.; Yolton, K.; Lanphear, B.P.; Chen, A. Exposure to endocrine disrupting chemicals (EDCs) and cardiometabolic indices during pregnancy: The HOME Study. Environ. Int. 2021, 156, 106747. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Kupsco, A.; Just, A.; Calafat, A.M.; Oken, E.; Braun, J.M.; Sanders, A.P.; Mercado-Garcia, A.; Cantoral, A.; Pantic, I.; et al. Maternal Phthalates Exposure and Blood Pressure during and after Pregnancy in the PROGRESS Study. Environ. Health Perspect. 2021, 129, 127007. [Google Scholar] [CrossRef]
- Soomro, M.H.; Maesano, C.N.; Heude, B.; Bornehag, C.G.; Annesi-Maesano, I. The association between maternal urinary phthalate metabolites concentrations and pregnancy induced hypertension: Results from the EDEN Mother-Child Cohort. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 102216. [Google Scholar] [CrossRef]
- Terrin, N.; Schmid, C.H.; Lau, J.; Olkin, I. Adjusting for publication bias in the presence of heterogeneity. Stat. Med. 2003, 22, 2113–2126. [Google Scholar] [CrossRef]
- Amin, M.M.; Ebrahimpour, K.; Parastar, S.; Shoshtari-Yeganeh, B.; Hashemi, M.; Mansourian, M.; Poursafa, P.; Fallah, Z.; Rafiei, N.; Kelishadi, R. Association of urinary concentrations of phthalate metabolites with cardiometabolic risk factors and obesity in children and adolescents. Chemosphere 2018, 211, 547–556. [Google Scholar] [CrossRef]
- Sol, C.M.; Santos, S.; Asimakopoulos, A.G.; Martinez-Moral, M.P.; Duijts, L.; Kannan, K.; Trasande, L.; Jaddoe, V.W.V. Associations of maternal phthalate and bisphenol urine concentrations during pregnancy with childhood blood pressure in a population-based prospective cohort study. Environ. Int. 2020, 138, 105677. [Google Scholar] [CrossRef]
- Vafeiadi, M.; Myridakis, A.; Roumeliotaki, T.; Margetaki, K.; Chalkiadaki, G.; Dermitzaki, E.; Venihaki, M.; Sarri, K.; Vassilaki, M.; Leventakou, V.; et al. Association of Early Life Exposure to Phthalates With Obesity and Cardiometabolic Traits in Childhood: Sex Specific Associations. Front. Public Health 2018, 6, 327. [Google Scholar] [CrossRef] [Green Version]
- Warembourg, C.; Maitre, L.; Tamayo-Uria, I.; Fossati, S.; Roumeliotaki, T.; Aasvang, G.M.; Andrusaityte, S.; Casas, M.; Cequier, E.; Chatzi, L.; et al. Early-Life Environmental Exposures and Blood Pressure in Children. J. Am. Coll. Cardiol. 2019, 74, 1317–1328. [Google Scholar] [CrossRef]
- Corrales, P.; Izquierdo-Lahuerta, A.; Medina-Gomez, G. Maintenance of Kidney Metabolic Homeostasis by PPAR Gamma. Int. J. Mol. Sci. 2018, 19, 2063. [Google Scholar] [CrossRef] [Green Version]
- Sugawara, A.; Uruno, A.; Matsuda, K.; Saito-Ito, T.; Funato, T.; Saito-Hakoda, A.; Kudo, M.; Ito, S. Effects of PPARgamma agonists against vascular and renal dysfunction. Curr. Mol. Pharmacol. 2012, 5, 248–254. [Google Scholar] [CrossRef]
- Ferguson, K.K.; McElrath, T.F.; Cantonwine, D.E.; Mukherjee, B.; Meeker, J.D. Phthalate metabolites and bisphenol-A in association with circulating angiogenic biomarkers across pregnancy. Placenta 2015, 36, 699–703. [Google Scholar] [CrossRef] [Green Version]
- Burton, G.J.; Yung, H.W.; Cindrova-Davies, T.; Charnock-Jones, D.S. Placental endoplasmic reticulum stress and oxidative stress in the pathophysiology of unexplained intrauterine growth restriction and early onset preeclampsia. Placenta 2009, 30 (Suppl. SA), S43–S48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, R.J.; Maynard, S.E.; Qian, C.; Lim, K.H.; England, L.J.; Yu, K.F.; Schisterman, E.F.; Thadhani, R.; Sachs, B.P.; Epstein, F.H.; et al. Circulating angiogenic factors and the risk of preeclampsia. N. Engl. J. Med. 2004, 350, 672–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Draganovic, D.; Lucic, N.; Jojic, D. Oxidative Stress Marker and Pregnancy Induced Hypertension. Med. Arch. 2016, 70, 437–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, H.Y.; Han, Y.; Gao, H.; Huang, K.; Ge, X.; Xu, Y.Y.; Xu, Y.Q.; Jin, Z.X.; Sheng, J.; Yan, S.Q.; et al. Maternal phthalate exposure during the first trimester and serum thyroid hormones in pregnant women and their newborns. Chemosphere 2016, 157, 42–48. [Google Scholar] [CrossRef]
- Zhang, Y.; Dai, X.; Yang, S.; Zhang, C.; Han, M.; Huang, H.F.; Fan, J. Maternal low thyroxin levels are associated with adverse pregnancy outcomes in a Chinese population. PLoS ONE 2017, 12, e0178100. [Google Scholar] [CrossRef] [Green Version]
- van’ t Erve, T.J.; Rosen, E.M.; Barrett, E.S.; Nguyen, R.H.N.; Sathyanarayana, S.; Milne, G.L.; Calafat, A.M.; Swan, S.H.; Ferguson, K.K. Phthalates and Phthalate Alternatives Have Diverse Associations with Oxidative Stress and Inflammation in Pregnant Women. Environ. Sci. Technol. 2019, 53, 3258–3267. [Google Scholar] [CrossRef]
- Harmon, A.C.; Cornelius, D.C.; Amaral, L.M.; Faulkner, J.L.; Cunningham, M.W., Jr.; Wallace, K.; LaMarca, B. The role of inflammation in the pathology of preeclampsia. Clin. Sci. 2016, 130, 409–419. [Google Scholar] [CrossRef] [Green Version]
- Benjamin, S.; Masai, E.; Kamimura, N.; Takahashi, K.; Anderson, R.C.; Faisal, P.A. Phthalates impact human health: Epidemiological evidences and plausible mechanism of action. J. Hazard. Mater. 2017, 340, 360–383. [Google Scholar] [CrossRef] [PubMed]
- Barrett, E.S.; Corsetti, M.; Day, D.; Thurston, S.W.; Loftus, C.T.; Karr, C.J.; Kannan, K.; LeWinn, K.Z.; Smith, A.K.; Smith, R.; et al. Prenatal phthalate exposure in relation to placental corticotropin releasing hormone (pCRH) in the CANDLE cohort. Environ. Int. 2022, 160, 107078. [Google Scholar] [CrossRef] [PubMed]
- Schoenaker, D.A.; Soedamah-Muthu, S.S.; Mishra, G.D. The association between dietary factors and gestational hypertension and pre-eclampsia: A systematic review and meta-analysis of observational studies. BMC Med. 2014, 12, 157. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Z.; Xie, H.; Liu, S.; Yang, R.; Yu, J.; Yan, Y.; Wang, X.; Zhang, Z.; Yan, W. Effects of physical exercise on blood pressure during pregnancy. BMC Public Health 2022, 22, 1733. [Google Scholar] [CrossRef]
- Cousins, I.T.; DeWitt, J.C.; Gluge, J.; Goldenman, G.; Herzke, D.; Lohmann, R.; Ng, C.A.; Scheringer, M.; Wang, Z. The high persistence of PFAS is sufficient for their management as a chemical class. Environ. Sci. Process. Impacts 2020, 22, 2307–2312. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowski, C.F.; Andrews, D.Q.; Birnbaum, L.S.; Bruton, T.A.; DeWitt, J.C.; Knappe, D.R.U.; Maffini, M.V.; Miller, M.F.; Pelch, K.E.; Reade, A.; et al. Scientific Basis for Managing PFAS as a Chemical Class. Environ. Sci. Technol. Lett. 2020, 7, 532–543. [Google Scholar] [CrossRef] [PubMed]
- Bobb, J.F.; Valeri, L.; Claus Henn, B.; Christiani, D.C.; Wright, R.O.; Mazumdar, M.; Godleski, J.J.; Coull, B.A. Bayesian kernel machine regression for estimating the health effects of multi-pollutant mixtures. Biostatistics 2015, 16, 493–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.K.; Tao, Y.; Meeker, J.D.; Harlow, S.D.; Mukherjee, B. Environmental risk score as a new tool to examine multi-pollutants in epidemiologic research: An example from the NHANES study using serum lipid levels. PLoS ONE 2014, 9, e98632. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Tao, Y.; Li, S.; Ferguson, K.K.; Meeker, J.D.; Park, S.K.; Batterman, S.A.; Mukherjee, B. Statistical strategies for constructing health risk models with multiple pollutants and their interactions: Possible choices and comparisons. Environ. Health 2013, 12, 85. [Google Scholar] [CrossRef] [Green Version]
- Billionnet, C.; Gay, E.; Kirchner, S.; Leynaert, B.; Annesi-Maesano, I. Quantitative assessments of indoor air pollution and respiratory health in a population-based sample of French dwellings. Environ. Res. 2011, 111, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Czarnota, J.; Gennings, C.; Wheeler, D.C. Assessment of weighted quantile sum regression for modeling chemical mixtures and cancer risk. Cancer Inform. 2015, 14, 159–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levin-Schwartz, Y.; Gennings, C.; Schnaas, L.; Del Carmen Hernandez Chavez, M.; Bellinger, D.C.; Tellez-Rojo, M.M.; Baccarelli, A.A.; Wright, R.O. Time-varying associations between prenatal metal mixtures and rapid visual processing in children. Environ. Health 2019, 18, 92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartell, S.M.; Calafat, A.M.; Lyu, C.; Kato, K.; Ryan, P.B.; Steenland, K. Rate of decline in serum PFOA concentrations after granular activated carbon filtration at two public water systems in Ohio and West Virginia. Environ. Health Perspect. 2010, 118, 222–228. [Google Scholar] [CrossRef] [Green Version]
- Olsen, G.W.; Burris, J.M.; Ehresman, D.J.; Froehlich, J.W.; Seacat, A.M.; Butenhoff, J.L.; Zobel, L.R. Half-life of serum elimination of perfluorooctanesulfonate, perfluorohexanesulfonate, and perfluorooctanoate in retired fluorochemical production workers. Environ. Health Perspect. 2007, 115, 1298–1305. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Source | Location | Study Period | Study Design | Sample Size | Phthalates Examined | Exposure Assessment | Exposure Period | Outcome(s) | Covariates Adjusted for | Main Findings |
|---|---|---|---|---|---|---|---|---|---|---|
| [9] | U.S. | 2011 | Cohort | 50 | MEHP; MEHHP; MEOHP; MECPP; MBzP; MBP; MiBP; MEP; MCPP; ΣDEHP | Maternal urine sample | 1st, 2nd and 3rd trimesters | PE | Age, race/ethnicity, prepregnancy BMI, health insurance category, education, smoking status during pregnancy, parity, gestational diabetes, prior history of PE | Several phthalate metabolites were significantly associated with increased risk of PE |
| [13] | U.S. | 2003–2006 | Cohort | 369 | MBzP; MMP; MEP; MiBP; MnBP; MEHP; MEOHP; MEHHP; MECPP; MBP; MCPP; ΣDEHP | Maternal urine sample | 2nd trimester | PIH (GH; PE; eclampsia; HELLP syndrome) | Race, age, house hold income, education, marital status, serum cotinine concentrations, parity, BMI at 16 weeks gestation, self-reported use of medications for high BP | Maternal urinary MBzP concentrations may be associated with increased diastolic BP and risk of pregnancy-induced hypertensive diseases |
| [14] | U.S. | 2004–2005 | Cohort | 1396 | Phthalic acid/LMW/HMW/DEHP/DNOP metabolite | Maternal urine sample | 1st trimester | Gestational hypertensive disorders (GH; PE) | Maternal age, maternal pre-pregnancy BMI, parity, ethnicity, education, maternal smoking, maternal alcohol, folic acid supplementation, gestational age at time of measurement and creatinine | Phthalate metabolite concentrations were not associated with gestational hypertensive disorders |
| [15] | Spain | 2014–2015 | Cross-sectional | 152 | MEP; MiBP; MnBP; MBzP; MEHP; MEHHP; MEOHP; MECPP; ΣDEHP; OH-MiNP; OXO-MiNP | Maternal urine sample | 2nd and 3rd trimesters | BP during pregnancy | Study center, age, ethnicity, marital status, pre-pregnancy BMI, BMI at examination, maternal height, education, working status, parity, physical activity, fruits and vegetables consumption, ultra-processed food consumption, gestational age, smoking status at examination | |
| [16] | China | - | Cohort | 3273 | DMP; DEP; DBP; MEHP; MEOHP; MBP; MMP; MEP; MBzP; MEHHP; BBzP; ∑DEHP | Maternal urine sample | 1st, 2nd and 3rd trimesters | HDOP (GH; PE; severe PE; eclampsia) | Age, pre-pregnancy BMI, education, residence, race, occupation type, monthly household income, drinking during pregnancy, smoking during pregnancy, primiparous | Exposure to a single phthalate metabolite or a specific diester during the first trimester of pregnancy elevated BP in the third trimester. However, inverse relationships were revealed for some phthalate metabolites, which were inconsistent with the results of their diesters |
| [17] | China | 2013–2015 | Cohort | 636 | MiBP; ΣDEHP; MMP; MEP; MnBP; MBzP; MEHP; MEOHP; MEHHP; MECPP; ΣLMW | Maternal urine sample | 1st, 2nd and 3rd trimesters | BP during pregnancy | Pre-pregnancy BMI, household income, GDM, fetus gender, age, parity | Exposure to phthalates was positively related to BP in pregnant women |
| [23] | U.S. | 2010–2012 | Cohort | 668 | MEP; MCPP; MiBP MBP; ∑DEHP; MBzP; MEHP; ∑DEHTP | Maternal urine sample | 1st and 3rd trimesters | PIH, GH; PE; eclampsia | Study center, race, age at delivery, household income, highest level of education, marital status, cigarette smoking in the first trimester, pre-pregnancy BMI, and parity | Several phthalate metabolite concentrations were significantly associated with PIH and greater increases in systolic BP across pregnancy |
| [24] | U.S. | 2003–2006 | Cohort | 388 | MEP; MBP; MiBP; MBzP; MCPP; ∑DEHP | Maternal urine sample | 2nd trimester | PIH, GH; PE; eclampsia | Age, race/ethnicity, annual household income, smoking status, marijuana use, pre-pregnancy BMI, parity, gestational week | No relationship was noted between any EDC compound and PIH disorders |
| [25] | Mexico | 2007–2011 | Cohort | 892 | ∑DEHP; MECPP; MBzP; ∑DBP; MCPP; MEP; MCNP; ∑DiNP; ∑DiBP | Maternal urine sample | 2nd and 3rd trimesters | BP during pregnancy | Age, SES, education, parity, second trimester BMI, second trimester height, second trimester BP, seasonality, and gestation age | Exposure to phthalates and phthalate biomarkers was associated with higher BP during late pregnancy |
| [26] | France | 2003–2006 | Cohort | 604 | MEP; MBP; MiBP; MECPP; MEHHP; MEOHP; MEHP; MBzP; MCOP; MCPP; MCNP; ΣDEHP | Maternal urine sample | 2nd trimester | PIH, GH; PE; eclampsia | Smoking, age, BMI, education level, gestational age, number of siblings | Prenatal exposure to some phthalates, including MEP and MBP, might play a role in pregnancy induced hypertension |
| Study Design | Reference | Selection | Comparability | Outcome/Exposure | Quality Score | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | |||
| Case-control | [9] | ★ | ★ | ★ | ★★ | ★ | ★ | ★ | 8/9 | |
| Cohort | [13] | ★ | ★ | ★ | ★ | ★ | ★ | ★ | 7/9 | |
| [14] | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | 8/9 | ||
| [15] | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ★ | 9/9 | |
| [16] | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | 8/9 | |
| [17] | ★ | ★ | ★ | ★ | ★ | ★ | ★ | 7/9 | ||
| [23] | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | 8/9 | ||
| [24] | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | 8/9 | ||
| [25] | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | 8/9 | ||
| [26] | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | 8/9 | ||
| Time of Outcome Measurement | Time of Exposure Measurement | Systolic Blood Pressure | Diastolic Blood Pressure | Hypertensive Disorders of Pregnancy | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Pooled Estimates (β) | I2 (%) | Tau2 | N | Pooled Estimates (β) | I2 (%) | Tau2 | N | Pooled Estimates(OR) | I2 (%) | Tau2 | ||
| MBP | |||||||||||||
| T1 | T1 | <3 | NA | <3 | NA | 4 | 1.07 (0.95, 1.20) | 0 | 0.0005 | ||||
| T2 + T3 | 3 | 1.05 (0.27, 1.83) * | 93 | 0.3780 | 3 | 0.40 (0.05, 0.74) * | 71 | 0.0514 | <3 | NA | |||
| T2 | T2 | <3 | NA | <3 | NA | <3 | NA | ||||||
| Average | <3 | NA | <3 | NA | 5 | 1.04 (0.92, 1.17) | 0 | 0.0018 | |||||
| MBzP | |||||||||||||
| T1 | T1 | <3 | NA | <3 | NA | 4 | 1.01 (0.94, 1.09) | 0 | 0.0009 | ||||
| T2 + T3 | 3 | 0.10 (−0.40, 0.59) | 32 | 0.1375 | 3 | 0.06 (−0.28, 0.40) | 41 | 0.0625 | <3 | NA | |||
| T2 | T2 | <3 | NA | <3 | NA | <3 | NA | ||||||
| T3 | 4 | 0.57 (0.01, 1.13) * | 0 | 0.0107 | 4 | 0.70 (0.27, 1.13) * | 0 | 0.0012 | <3 | NA | |||
| Average | <3 | NA | <3 | NA | 6 | 1.09 (0.99, 1.20) | 8 | 0.0109 | |||||
| MCPP | |||||||||||||
| T1 | T1 | <3 | NA | <3 | NA | 3 | 1.18 (0.99, 1.41) | 18 | 0.0117 | ||||
| T2 | T3 | 3 | 0.63 (–1.14, 2.40) | 72 | 1.7700 | 3 | 0.18 (−0.51, 0.86) | 0 | 0.0042 | <3 | NA | ||
| Average | <3 | NA | <3 | NA | 5 | 1.02 (0.86, 1.22) | 0 | 0.0066 | |||||
| MEHP | |||||||||||||
| T1 | T2 + T3 | 3 | −0.32 (−0.60, −0.05) * | 0 | 0.0163 | 3 | −0.38 (−0.61, −0.15) | 32 | 0.0139 | <3 | NA | ||
| MEHHP | |||||||||||||
| T1 | T1 | <3 | NA | <3 | NA | 3 | 1.02 (0.89, 1.17) | 0 | 0.0002 | ||||
| Average | <3 | NA | <3 | NA | 3 | 1.10 (0.96, 1.26) | 0 | <0.0001 | |||||
| MEP | |||||||||||||
| T1 | T1 | <3 | NA | <3 | NA | 4 | 1.12 (1.02, 1.23) | 26 | 0.0104 | ||||
| T2 + T3 | 3 | 0.14 (−0.14, 0.41) | 34 | 0.0200 | 3 | 0.06 (−0.20, 0.32) | 48 | 0.0292 | <3 | NA | |||
| T2 | T2 | 3 | −0.12 (−0.95, 0.72) | 44 | 0.3378 | 3 | −0.16 (−0.78, 0.45) | 36 | 0.1702 | <3 | NA | ||
| T3 | 5 | 0.21 (−0.61, 1.04) | 50 | 0.6418 | 5 | 0.22 (−0.27, 0.71) | 35 | 0.1897 | <3 | NA | |||
| Average | <3 | NA | <3 | NA | 6 | 1.06 (0.97, 1.15) | 0 | 0.0055 | |||||
| MIBP | |||||||||||||
| T1 | T1 | <3 | NA | <3 | NA | 3 | 1.14 (0.94, 1.39) | 32 | 0.0292 | ||||
| T2 | T3 | 3 | 0.04 (−0.91, 0.98) | 26 | 0.2691 | 3 | 0.17 (−0.38, 0.71) | 0 | 0.0652 | <3 | NA | ||
| Average | <3 | NA | <3 | NA | 4 | 1.11 (0.93, 1.33) | 48 | 0.0606 | |||||
| MMP | |||||||||||||
| T1 | T1 | <3 | NA | <3 | NA | 3 | 1.05 (0.93, 1.19) | 0 | 0.0004 | ||||
| Average | <3 | NA | <3 | NA | 3 | 1.02 (0.92, 1.14) | 0 | 0.0009 | |||||
| ΣDEHP | |||||||||||||
| T1 | T2 + T3 | 3 | 0.27 (−0.11, 0.66) | 0 | 0.0229 | 3 | −0.01 (−0.30, 0.28) | 0 | 0.0088 | <3 | NA | ||
| T2 | T2 | 3 | −0.02 (−0.58, 0.53) | 0 | 0.0041 | 3 | −0.22 (−0.63, 0.19) | 0 | 0.0007 | <3 | NA | ||
| T3 | 5 | 0.25 (−0.39, 0.90) | 15 | 0.1802 | 5 | −0.13 (−0.73, 0.47) | 22 | 0.2403 | <3 | NA | |||
| Average | <3 | NA | <3 | NA | 4 | 1.11 (0.96,1.28) | 0 | 0.0122 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, M.; Qiao, J.; Xie, P.; Li, Z.; Hu, C.; Li, F. The Association between Maternal Urinary Phthalate Concentrations and Blood Pressure in Pregnancy: A Systematic Review and Meta-Analysis. Metabolites 2023, 13, 812. https://doi.org/10.3390/metabo13070812
Zhang M, Qiao J, Xie P, Li Z, Hu C, Li F. The Association between Maternal Urinary Phthalate Concentrations and Blood Pressure in Pregnancy: A Systematic Review and Meta-Analysis. Metabolites. 2023; 13(7):812. https://doi.org/10.3390/metabo13070812
Chicago/Turabian StyleZhang, Mengyue, Jianchao Qiao, Pinpeng Xie, Zhuoyan Li, Chengyang Hu, and Fei Li. 2023. "The Association between Maternal Urinary Phthalate Concentrations and Blood Pressure in Pregnancy: A Systematic Review and Meta-Analysis" Metabolites 13, no. 7: 812. https://doi.org/10.3390/metabo13070812