
Potential Use of Thalidomide in Glioblastoma Treatment: An Updated Brief Overview
 , , ,
, , ,  , ,
, ,  ,
,  and
and
Abstract
:
1. Introduction
2. Genetic and Molecular Pathogenesis of GBM
3. Hypoxia, Endoplasmic Reticulum Stress, and Chemoresistance
4. Thalidomide Mechanism of Action
5. Thalidomide Efficacy
6. Thalidomide Safety
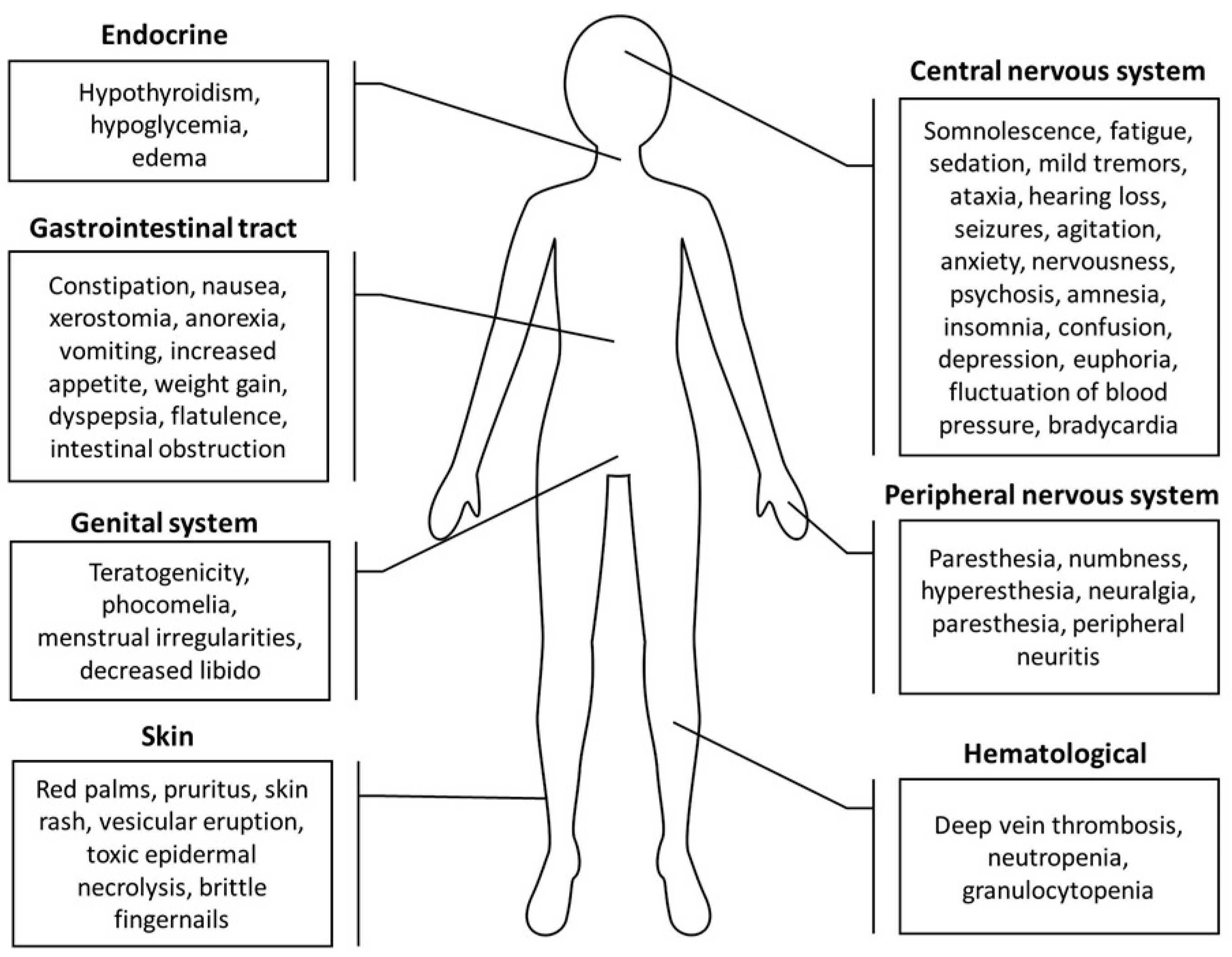
7. Thalidomide Toxicity
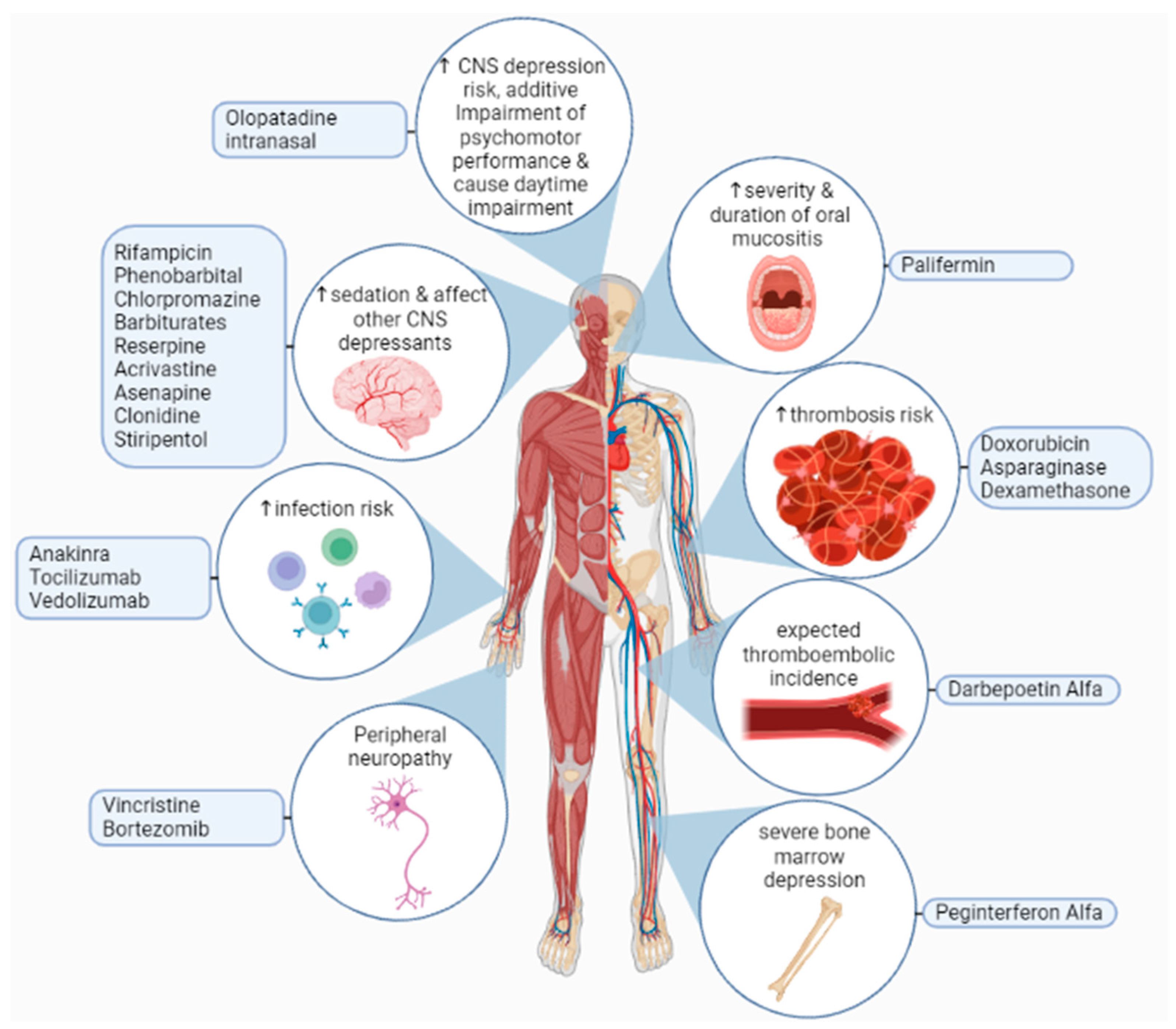
8. Thalidomide Drug Interactions
9. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| Abbreviation | Explanation |
| 5-ALA | 5-aminolaevulinic acid |
| ACVRL1 | activin A receptor like type 1 |
| ALA-PDT | 5-aminolevulinic acid photodynamic therapy |
| ALDH | aldehyde dehydrogenase 1 |
| AML | acute myeloid leukemia |
| ATRX | alpha-thalassemia/mental retardation, X-linked |
| AZA | 5-azacytidine |
| AZN | azathioprine |
| bFGF | basic fibroblast growth factors |
| BSA | body surface area |
| CD | cluster of differentiation |
| CIAP2 | cellular inhibitor of apoptosis protein 2 |
| CNS | central nervous system |
| Cox2 | cyclooxygenase 2 |
| CRBN | cereblon |
| DLE | discoid lupus erythematosus |
| DNA | deoxyribonucleic acid |
| DTH | delayed-type hypersensitivity |
| EGFR | epidermal growth factor receptor |
| ENG | endoglin |
| ENL | erythema nodosum leprosum |
| ER | endoplasmic reticulum |
| FCT | fludarabine, carboplatin, and topotecan |
| FGF | fibroblast growth factors |
| GBM | glioblastoma multiforme |
| GIB | gastrointestinal bleeding |
| GSCs | glioblastoma stem cells |
| HbF | fetal hemoglobin |
| HHT | hereditary hemorrhagic telangiectasia |
| HIF | hypoxia-inducible factors |
| HIMEC | human intestinal microvascular endothelial cells |
| HSA | hemangiosarcoma |
| IBD | inflammatory bowel disease |
| IDH | isocitrate dehydrogenases |
| IFN | interferon |
| IFNγ | interferon-gamma |
| IL | interleukin |
| IPF | idiopathic pulmonary fibrosis |
| KCNMA1 | calcium-activated potassium channel subunit alpha-1 |
| LVAD | left ventricular assist device |
| MDR1 | multidrug resistance mutation 1 |
| MDS | myelodysplastic syndrome |
| MDSCs | myeloid-derived suppressor cells |
| MGMT | O6-methylguanine-DNA methyltransferase |
| MMAC1 | mutated in multiple advanced cancers |
| MVD | marrow microvascular density |
| NF-κB | nuclear factor-kappa B |
| NKG2D | natural killer cell activation receptor |
| NSCLC | non-small-cell lung cancer |
| ORR | objective response rate |
| OS | overall survival |
| PASI | psoriasis area and severity index |
| PBMCs | peripheral blood mononuclear cells |
| PDAI | pemphigus disease area index |
| PDGFRA | platelet-derived growth factor receptor alpha |
| PDGFRβ | platelet-derived growth factor B |
| PNP | paraneoplastic pemphigus |
| POEMS | (polyneuropathy, organomegaly, endocrinopathy, monoclonal protein, skin changes) |
| PPD | purified protein derivative |
| PTEN | phosphatase and tensin homolog |
| PV | pemphigus vulgaris |
| RAS | recurrent aphthous stomatitis |
| RCC | renal cell carcinoma |
| RNA | ribonucleic acid |
| ROS | reactive oxygen species |
| TENM1 | teneurin transmembrane protein 1 |
| TERT | telomerase reverse transcriptase |
| TGF | transforming growth factor |
| TGFβ | transforming growth factor-beta |
| THD | thalidomide |
| TICs | tumor-initiating cells |
| TMZ | temozolomide |
| TNF | tumor necrosis factor |
| TNFα | tumor necrosis factor-alpha |
| Treg | regulatory T |
| VAD | vincristine, liposomal doxorubicin, and dexamethasone |
| VDT | Velcade, Doxil, and thalidomide |
| VEGF | vascular endothelial growth factor |
| VHL | von Hippel Lindau |
References
- Thakkar, J.P.; Dolecek, T.A.; Horbinski, C.; Ostrom, Q.T.; Lightner, D.D.; Barnholtz-Sloan, J.S.; Villano, J.L. Epidemiologic and Molecular Prognostic Review of Glioblastoma. Cancer Epidemiol. Biomark. Prev. 2014, 23, 1985–1996. [Google Scholar] [CrossRef] [Green Version]
- Tan, A.C.; Ashley, D.M.; López, G.Y.; Malinzak, M.; Friedman, H.S.; Khasraw, M. Management of glioblastoma: State of the art and future directions. CA Cancer J. Clin. 2020, 70, 299–312. [Google Scholar] [CrossRef]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [Green Version]
- Faria, J.; Romão, L.; Martins, S.; Alves, T.; Mendes, F.A.; de Faria, G.P.; Hollanda, R.; Takiya, C.; Chimelli, L.; Morandi, V.; et al. Interactive properties of human glioblastoma cells with brain neurons in culture and neuronal modulation of glial laminin organization. Differentiation 2006, 74, 562–572. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. The Hallmarks of Cancer. Cell 2000, 100, 57–70. [Google Scholar] [CrossRef] [Green Version]
- Field, K.M.; Jordan, J.T.; Wen, P.Y.; Rosenthal, M.A.; Reardon, D.A. Bevacizumab and glioblastoma: Scientific review, newly reported updates, and ongoing controversies. Cancer 2015, 121, 997–1007. [Google Scholar] [CrossRef]
- Plate, K.H.; Breier, G.; Weich, H.A.; Risau, W. Vascular endothelial growth factor is a potential tumour angiogenesis factor in human gliomas in vivo. Nature 1992, 359, 845–848. [Google Scholar] [CrossRef]
- Vredenburgh, J.J.; Desjardins, A.; Herndon, J.E.; Dowell, J.M.; Reardon, D.A.; Quinn, J.A.; Rich, J.N.; Sathornsumetee, S.; Gururangan, S.; Wagner, M.; et al. Phase II Trial of Bevacizumab and Irinotecan in Recurrent Malignant Glioma. Clin. Cancer Res. 2007, 13, 1253–1259. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.J.; Li, B.; Winer, J.; Armanini, M.; Gillett, N.; Phillips, H.S.; Ferrara, N. Inhibition of vascular endothelial growth factor-induced angiogenesis suppresses tumour growth in vivo. Nature 1993, 362, 841–844. [Google Scholar] [CrossRef]
- Jensen, R.L.; Ragel, B.T.; Whang, K.; Gillespie, D. Inhibition of hypoxia inducible factor-1α (HIF-1α) decreases vascular endothelial growth factor (VEGF) secretion and tumor growth in malignant gliomas. J. Neuro-Oncol. 2006, 78, 233–247. [Google Scholar] [CrossRef]
- Friedman, H.S.; Prados, M.D.; Wen, P.Y.; Mikkelsen, T.; Schiff, D.; Abrey, L.E.; Yung, W.K.A.; Paleologos, N.; Nicholas, M.K.; Jensen, R.; et al. Bevacizumab Alone and in Combination With Irinotecan in Recurrent Glioblastoma. J. Clin. Oncol. 2009, 27, 4733–4740. [Google Scholar] [CrossRef] [Green Version]
- Zhang, G.; Huang, S.; Wang, Z. A meta-analysis of bevacizumab alone and in combination with irinotecan in the treatment of patients with recurrent glioblastoma multiforme. J. Clin. Neurosci. 2012, 19, 1636–1640. [Google Scholar] [CrossRef]
- Vredenburgh, J.J.; Desjardins, A.; Herndon, J.E.; Marcello, J.; Reardon, D.A.; Quinn, J.A.; Rich, J.N.; Sathornsumetee, S.; Gururangan, S.; Sampson, J.; et al. Bevacizumab Plus Irinotecan in Recurrent Glioblastoma Multiforme. J. Clin. Oncol. 2007, 25, 4722–4729. [Google Scholar] [CrossRef] [Green Version]
- Smiley, S.B.; Zarrinmayeh, H.; Das, S.K.; Pollok, K.E.; Vannier, M.W.; Veronesi, M.C. Novel therapeutics and drug-delivery approaches in the modulation of glioblastoma stem cell resistance. Ther. Deliv. 2022, 13, 249–273. [Google Scholar] [CrossRef]
- Rodriguez, S.M.B.; Staicu, G.-A.; Sevastre, A.-S.; Baloi, C.; Ciubotaru, V.; Dricu, A.; Tataranu, L.G. Glioblastoma Stem Cells—Useful Tools in the Battle against Cancer. Int. J. Mol. Sci. 2022, 23, 4602. [Google Scholar] [CrossRef]
- Wang, Y.; Xing, D.; Zhao, M.; Wang, J.; Yang, Y. The Role of a Single Angiogenesis Inhibitor in the Treatment of Recurrent Glioblastoma Multiforme: A Meta-Analysis and Systematic Review. PLoS ONE 2016, 11, e0152170. [Google Scholar] [CrossRef] [Green Version]
- Taylor, O.G.; Brzozowski, J.S.; Skelding, K.A. Glioblastoma Multiforme: An Overview of Emerging Therapeutic Targets. Front. Oncol. 2019, 9, 963. [Google Scholar] [CrossRef] [Green Version]
- Ahmadiankia, N. In vitro and in vivo studies of cancer cell behavior under nutrient deprivation. Cell Biol. Int. 2020, 44, 1588–1597. [Google Scholar] [CrossRef]
- Rosa, R.; Monteleone, F.; Zambrano, N.; Bianco, R. In Vitro and In Vivo Models for Analysis of Resistance to Anticancer Molecular Therapies. Curr. Med. Chem. 2014, 21, 1595–1606. [Google Scholar] [CrossRef]
- Fujisawa, H.; Reis, R.M.; Nakamura, M.; Colella, S.; Yonekawa, Y.; Kleihues, P.; Ohgaki, H. Loss of Heterozygosity on Chromosome 10 Is More Extensive in Primary (De Novo) Than in Secondary Glioblastomas. Lab. Investig. 2000, 80, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Ohgaki, H.; Kleihues, P. Genetic Pathways to Primary and Secondary Glioblastoma. Am. J. Pathol. 2007, 170, 1445–1453. [Google Scholar] [CrossRef] [Green Version]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]
- Balss, J.; Meyer, J.; Mueller, W.; Korshunov, A.; Hartmann, C.; von Deimling, A. Analysis of the IDH1 codon 132 mutation in brain tumors. Acta Neuropathol. 2008, 116, 597–602. [Google Scholar] [CrossRef]
- Nobusawa, S.; Watanabe, T.; Kleihues, P.; Ohgaki, H. IDH1 Mutations as Molecular Signature and Predictive Factor of Secondary Glioblastomas. Clin. Cancer Res. 2009, 15, 6002–6007. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, T.; Nobusawa, S.; Kleihues, P.; Ohgaki, H. IDH1 Mutations Are Early Events in the Development of Astrocytomas and Oligodendrogliomas. Am. J. Pathol. 2009, 174, 1149–1153. [Google Scholar] [CrossRef] [Green Version]
- Yan, H.; Parsons, D.W.; Jin, G.; McLendon, R.; Rasheed, B.A.; Yuan, W.; Kos, I.; Batinic-Haberle, I.; Jones, S.; Riggins, G.J.; et al. IDH1andIDH2Mutations in Gliomas. N. Engl. J. Med. 2009, 360, 765–773. [Google Scholar] [CrossRef]
- Watanabe, K.; Tachibana, O.; Sato, K.; Yonekawa, Y.; Kleihues, P.; Ohgaki, H. Overexpression of the EGF Receptor and p53 Mutations are Mutually Exclusive in the Evolution of Primary and Secondary Glioblastomas. Brain Pathol. 1996, 6, 217–223. [Google Scholar] [CrossRef]
- Ohgaki, H.; Kleihues, P. The Definition of Primary and Secondary Glioblastoma. Clin. Cancer Res. 2013, 19, 764–772. [Google Scholar] [CrossRef] [Green Version]
- Hegi, M.E.; Diserens, A.-C.; Gorlia, T.; Hamou, M.-F.; de Tribolet, N.; Weller, M.; Kros, J.M.; Hainfellner, J.A.; Mason, W.; Mariani, L.; et al. MGMTGene Silencing and Benefit from Temozolomide in Glioblastoma. N. Engl. J. Med. 2005, 352, 997–1003. [Google Scholar] [CrossRef] [Green Version]
- Haile, L.A.; Greten, T.F.; Korangy, F. Immune Suppression: The Hallmark of Myeloid Derived Suppressor Cells. Immunol. Investig. 2012, 41, 581–594. [Google Scholar] [CrossRef]
- Li, H.; Han, Y.; Guo, Q.; Zhang, M.; Cao, X. Cancer-Expanded Myeloid-Derived Suppressor Cells Induce Anergy of NK Cells through Membrane-Bound TGF-β1. J. Immunol. 2009, 182, 240–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srivastava, M.K.; Sinha, P.; Clements, V.K.; Rodriguez, P.; Ostrand-Rosenberg, S. Myeloid-Derived Suppressor Cells Inhibit T-Cell Activation by Depleting Cystine and Cysteine. Cancer Res. 2010, 70, 68–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waldron, T.J.; Quatromoni, J.G.; Karakasheva, T.A.; Singhal, S.; Rustgi, A.K. Myeloid derived suppressor cells. OncoImmunology 2014, 2, e24117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tripodo, C.; Zhang, S.; Ma, X.; Zhu, C.; Liu, L.; Wang, G.; Yuan, X. The Role of Myeloid-Derived Suppressor Cells in Patients with Solid Tumors: A Meta-Analysis. PLoS ONE 2016, 11, e0164514. [Google Scholar] [CrossRef]
- Serocki, M.; Bartoszewska, S.; Janaszak-Jasiecka, A.; Ochocka, R.J.; Collawn, J.F.; Bartoszewski, R. miRNAs regulate the HIF switch during hypoxia: A novel therapeutic target. Angiogenesis 2018, 21, 183–202. [Google Scholar] [CrossRef] [Green Version]
- Shen, G.; Li, X.; Jia, Y.-f.; Piazza, G.A.; Xi, Y. Hypoxia-regulated microRNAs in human cancer. Acta Pharmacol. Sin. 2013, 34, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Balamurugan, K. HIF-1 at the crossroads of hypoxia, inflammation, and cancer. Int. J. Cancer 2016, 138, 1058–1066. [Google Scholar] [CrossRef] [Green Version]
- Masson, N.; Ratcliffe, P.J. Hypoxia signaling pathways in cancer metabolism: The importance of co-selecting interconnected physiological pathways. Cancer Metab. 2014, 2, 3. [Google Scholar] [CrossRef] [Green Version]
- Moldogazieva, N.T.; Mokhosoev, I.M.; Terentiev, A.A. Metabolic Heterogeneity of Cancer Cells: An Interplay between HIF-1, GLUTs, and AMPK. Cancers 2020, 12, 862. [Google Scholar] [CrossRef] [Green Version]
- Samanta, D.; Semenza, G.L. Metabolic adaptation of cancer and immune cells mediated by hypoxia-inducible factors. Biochim. Biophys. Acta (BBA)—Rev. Cancer 2018, 1870, 15–22. [Google Scholar] [CrossRef]
- Semenza, G.L. Hypoxia-Inducible Factors in Physiology and Medicine. Cell 2012, 148, 399–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaur, B.; Khwaja, F.W.; Severson, E.A.; Matheny, S.L.; Brat, D.J.; Van Meir, E.G. Hypoxia and the hypoxia-inducible-factor pathway in glioma growth and angiogenesis. Neuro-Oncology 2005, 7, 134–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, G.; Wang, J.-J.; Fu, X.-L.; Guang, R.; To, S.-S.T. Advances in the targeting of HIF-1α and future therapeutic strategies for glioblastoma multiforme. Oncol. Rep. 2017, 37, 657–670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiche, J.; Brahimi-Horn, M.C.; Pouysségur, J. Tumour hypoxia induces a metabolic shift causing acidosis: A common feature in cancer. J. Cell. Mol. Med. 2010, 14, 771–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gatenby, R.A.; Gillies, R.J. Why do cancers have high aerobic glycolysis? Nat. Rev. Cancer 2004, 4, 891–899. [Google Scholar] [CrossRef] [PubMed]
- Gerweck, L.E.; Seetharaman, K. Cellular pH gradient in tumor versus normal tissue: Potential exploitation for the treatment of cancer. Cancer Res. 1996, 56, 1194–1198. [Google Scholar] [PubMed]
- Kallinowski, F.; Vaupel, P. pH distributions in spontaneous and isotransplanted rat tumours. Br. J. Cancer 1988, 58, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Vaupel, P.; Kallinowski, F.; Okunieff, P. Blood flow, oxygen and nutrient supply, and metabolic microenvironment of human tumors: A review. Cancer Res. 1989, 49, 6449–6465. [Google Scholar] [PubMed]
- Hjelmeland, A.B.; Wu, Q.; Heddleston, J.M.; Choudhary, G.S.; MacSwords, J.; Lathia, J.D.; McLendon, R.; Lindner, D.; Sloan, A.; Rich, J.N. Acidic stress promotes a glioma stem cell phenotype. Cell Death Differ. 2010, 18, 829–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, L.; Fukumura, D.; Jain, R.K. Acidic Extracellular pH Induces Vascular Endothelial Growth Factor (VEGF) in Human Glioblastoma Cells via ERK1/2 MAPK Signaling Pathway. J. Biol. Chem. 2002, 277, 11368–11374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukumura, D.; Xu, L.; Chen, Y.; Gohongi, T.; Seed, B.; Jain, R.K. Hypoxia and acidosis independently up-regulate vascular endothelial growth factor transcription in brain tumors in vivo. Cancer Res. 2001, 61, 6020–6024. [Google Scholar] [PubMed]
- Mekhail, K.; Gunaratnam, L.; Bonicalzi, M.-E.; Lee, S. HIF activation by pH-dependent nucleolar sequestration of VHL. Nat. Cell Biol. 2004, 6, 642–647. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Bao, S.; Wu, Q.; Wang, H.; Eyler, C.; Sathornsumetee, S.; Shi, Q.; Cao, Y.; Lathia, J.; McLendon, R.E.; et al. Hypoxia-Inducible Factors Regulate Tumorigenic Capacity of Glioma Stem Cells. Cancer Cell 2009, 15, 501–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joseph, J.V.; Conroy, S.; Pavlov, K.; Sontakke, P.; Tomar, T.; Eggens-Meijer, E.; Balasubramaniyan, V.; Wagemakers, M.; den Dunnen, W.F.A.; Kruyt, F.A.E. Hypoxia enhances migration and invasion in glioblastoma by promoting a mesenchymal shift mediated by the HIF1α–ZEB1 axis. Cancer Lett. 2015, 359, 107–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peppino, G.; Ruiu, R.; Arigoni, M.; Riccardo, F.; Iacoviello, A.; Barutello, G.; Quaglino, E. Teneurins: Role in Cancer and Potential Role as Diagnostic Biomarkers and Targets for Therapy. Int. J. Mol. Sci. 2021, 22, 2321. [Google Scholar] [CrossRef]
- Ziegler, A.; Corvalán, A.; Roa, I.; Brañes, J.A.; Wollscheid, B. Teneurin protein family: An emerging role in human tumorigenesis and drug resistance. Cancer Lett. 2012, 326, 1–7. [Google Scholar] [CrossRef]
- Carcelen, M.; Velasquez, C.; Vidal, V.; Gutiérrez, O.; Fernández-Luna, J.L. Signaling Pathways Regulating the Expression of the Glioblastoma Invasion Factor TENM1. Biomedicines 2022, 10, 1104. [Google Scholar] [CrossRef]
- Heddleston, J.M.; Li, Z.; McLendon, R.E.; Hjelmeland, A.B.; Rich, J.N. The hypoxic microenvironment maintains glioblastoma stem cells and promotes reprogramming towards a cancer stem cell phenotype. Cell Cycle 2014, 8, 3274–3284. [Google Scholar] [CrossRef] [Green Version]
- Seidel, S.; Garvalov, B.K.; Wirta, V.; von Stechow, L.; Schänzer, A.; Meletis, K.; Wolter, M.; Sommerlad, D.; Henze, A.-T.; Nistér, M.; et al. A hypoxic niche regulates glioblastoma stem cells through hypoxia inducible factor 2α. Brain 2010, 133, 983–995. [Google Scholar] [CrossRef] [Green Version]
- Soeda, A.; Park, M.; Lee, D.; Mintz, A.; Androutsellis-Theotokis, A.; McKay, R.D.; Engh, J.; Iwama, T.; Kunisada, T.; Kassam, A.B.; et al. Hypoxia promotes expansion of the CD133-positive glioma stem cells through activation of HIF-1α. Oncogene 2009, 28, 3949–3959. [Google Scholar] [CrossRef] [Green Version]
- Chevet, E.; Hetz, C.; Samali, A. Endoplasmic Reticulum Stress—Activated Cell Reprogramming in Oncogenesis. Cancer Discov. 2015, 5, 586–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hetz, C.; Zhang, K.; Kaufman, R.J. Mechanisms, regulation and functions of the unfolded protein response. Nat. Rev. Mol. Cell Biol. 2020, 21, 421–438. [Google Scholar] [CrossRef] [PubMed]
- Oakes, S.A. Endoplasmic Reticulum Stress Signaling in Cancer Cells. Am. J. Pathol. 2020, 190, 934–946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madden, E.; Logue, S.E.; Healy, S.J.; Manie, S.; Samali, A. The role of the unfolded protein response in cancer progression: From oncogenesis to chemoresistance. Biol. Cell 2019, 111, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheloni, G.; Poteti, M.; Bono, S.; Masala, E.; Mazure, N.M.; Rovida, E.; Lulli, M.; Dello Sbarba, P. The Leukemic Stem Cell Niche: Adaptation to “Hypoxia” versus Oncogene Addiction. Stem Cells Int. 2017, 2017, 4979474. [Google Scholar] [CrossRef] [Green Version]
- Rovida, E.; Peppicelli, S.; Bono, S.; Bianchini, F.; Tusa, I.; Cheloni, G.; Marzi, I.; Cipolleschi, M.G.; Calorini, L.; Sbarba, P.D. The metabolically-modulated stem cell niche: A dynamic scenario regulating cancer cell phenotype and resistance to therapy. Cell Cycle 2014, 13, 3169–3175. [Google Scholar] [CrossRef] [PubMed]
- Comerford, K.M.; Wallace, T.J.; Karhausen, J.; Louis, N.A.; Montalto, M.C.; Colgan, S.P. Hypoxia-inducible factor-1-dependent regulation of the multidrug resistance (MDR1) gene. Cancer Res. 2002, 62, 3387–3394. [Google Scholar]
- Doublier, S.; Belisario, D.C.; Polimeni, M.; Annaratone, L.; Riganti, C.; Allia, E.; Ghigo, D.; Bosia, A.; Sapino, A. HIF-1 activation induces doxorubicin resistance in MCF7 3-D spheroids via P-glycoprotein expression: A potential model of the chemo-resistance of invasive micropapillary carcinoma of the breast. BMC Cancer 2012, 12, 4. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.; Yan, Q.; Liao, B.; Zhao, L.; Xiong, S.; Wang, J.; Zou, D.; Pan, J.; Wu, L.; Deng, Y.; et al. The HIF1α/HIF2α-miR210-3p network regulates glioblastoma cell proliferation, dedifferentiation and chemoresistance through EGF under hypoxic conditions. Cell Death Dis. 2020, 11, 992. [Google Scholar] [CrossRef]
- Tang, J.-H.; Ma, Z.-X.; Huang, G.-H.; Xu, Q.-F.; Xiang, Y.; Li, N.; Sidlauskas, K.; Zhang, E.E.; Lv, S.-Q. Downregulation of HIF-1a sensitizes U251 glioma cells to the temozolomide (TMZ) treatment. Exp. Cell Res. 2016, 343, 148–158. [Google Scholar] [CrossRef]
- Asatsuma-Okumura, T.; Ito, T.; Handa, H. Molecular Mechanisms of the Teratogenic Effects of Thalidomide. Pharmaceuticals 2020, 13, 95. [Google Scholar] [CrossRef] [PubMed]
- Faver, I.R.; Guerra, S.G.; Su, W.P.D.; el-Azhary, R. Thalidomide for dermatology: A review of clinical uses and adverse effects. Int. J. Dermatol. 2005, 44, 61–67. [Google Scholar] [CrossRef]
- Miyazato, K.; Tahara, H.; Hayakawa, Y. Antimetastatic effects of thalidomide by inducing the functional maturation of peripheral natural killer cells. Cancer Sci. 2020, 111, 2770–2778. [Google Scholar] [CrossRef] [PubMed]
- de Souza, C.M.; Araújo e Silva, A.C.; de Jesus Ferraciolli, C.; Moreira, G.V.; Campos, L.C.; dos Reis, D.C.; Lopes, M.T.P.; Ferreira, M.A.N.D.; Andrade, S.P.; Cassali, G.D. Combination therapy with carboplatin and thalidomide suppresses tumor growth and metastasis in 4T1 murine breast cancer model. Biomed. Pharmacother. 2014, 68, 51–57. [Google Scholar] [CrossRef]
- Abe, Y.; Ishida, T. Immunomodulatory drugs in the treatment of multiple myeloma. Jpn. J. Clin. Oncol. 2019, 49, 695–702. [Google Scholar] [CrossRef]
- Holstein, S.A.; McCarthy, P.L. Immunomodulatory Drugs in Multiple Myeloma: Mechanisms of Action and Clinical Experience. Drugs 2017, 77, 505–520. [Google Scholar] [CrossRef]
- Ito, T.; Handa, H. Molecular mechanisms of thalidomide and its derivatives. Proc. Jpn. Acad. Ser. B 2020, 96, 189–203. [Google Scholar] [CrossRef] [PubMed]
- Vargesson, N. Thalidomide-induced teratogenesis: History and mechanisms. Birth Defects Res. Part C Embryo Today Rev. 2015, 105, 140–156. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.J.; Pucilowska, J.; Lombardi, R.Q.; Rooney, J.P. A mutation in a novel ATP-dependent Lon protease gene in a kindred with mild mental retardation. Neurology 2004, 63, 1927–1931. [Google Scholar] [CrossRef] [Green Version]
- Angers, S.; Li, T.; Yi, X.; MacCoss, M.J.; Moon, R.T.; Zheng, N. Molecular architecture and assembly of the DDB1–CUL4A ubiquitin ligase machinery. Nature 2006, 443, 590–593. [Google Scholar] [CrossRef]
- Higgins, J.J.; Hao, J.; Kosofsky, B.E.; Rajadhyaksha, A.M. Dysregulation of large-conductance Ca2+-activated K+ channel expression in nonsyndromal mental retardation due to a cereblon p.R419X mutation. Neurogenetics 2008, 9, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Jo, S.; Lee, K.-H.; Song, S.; Jung, Y.-K.; Park, C.-S. Identification and functional characterization of cereblon as a binding protein for large-conductance calcium-activated potassium channel in rat brain. J. Neurochem. 2005, 94, 1212–1224. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Scialli, A.R. Thalidomide: The Tragedy of Birth Defects and the Effective Treatment of Disease. Toxicol. Sci. 2011, 122, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reske, T.; Fulciniti, M.; Munshi, N.C. Mechanism of action of immunomodulatory agents in multiple myeloma. Med. Oncol. 2010, 27, 7–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zervas, K.; Dimopoulos, M.A.; Hatzicharissi, E.; Anagnostopoulos, A.; Papaioannou, M.; Mitsouli, C.; Panagiotidis, P.; Korantzis, J.; Tzilianos, M.; Maniatis, A. Primary treatment of multiple myeloma with thalidomide, vincristine, liposomal doxorubicin and dexamethasone(T-VAD doxil): A phase II multicenter study. Ann. Oncol. 2004, 15, 134–138. [Google Scholar] [CrossRef]
- Raza, A.; Mehdi, M.; Mumtaz, M.; Ali, F.; Lascher, S.; Galili, N. Combination of 5-azacytidine and thalidomide for the treatment of myelodysplastic syndromes and acute myeloid leukemia. Cancer 2008, 113, 1596–1604. [Google Scholar] [CrossRef]
- Kesari, S.; Schiff, D.; Henson, J.W.; Muzikansky, A.; Gigas, D.C.; Doherty, L.; Batchelor, T.T.; Longtine, J.A.; Ligon, K.L.; Weaver, S.; et al. Phase II study of temozolomide, thalidomide, and celecoxib for newly diagnosed glioblastoma in adults. Neuro-Oncology 2008, 10, 300–308. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Giralt, S.; Delasalle, K.; Handy, B.; Alexanian, R. Bortezomib in combination with thalidomide-dexamethasone for previously untreated multiple myeloma. Hematology 2013, 12, 235–239. [Google Scholar] [CrossRef]
- Amato, R.J.; Morgan, M.; Rawat, A. Phase I/II study of thalidomide in combination with interleukin-2 in patients with metastatic renal cell carcinoma. Cancer 2006, 106, 1498–1506. [Google Scholar] [CrossRef]
- Barr, P.; Fu, P.; Lazarus, H.; Kane, D.; Meyerson, H.; Hartman, P.; Reyes, R.; Creger, R.; Stear, K.; Laughlin, M.; et al. Antiangiogenic activity of thalidomide in combination with fludarabine, carboplatin, and topotecan for high-risk acute myelogenous leukemia. Leuk. Lymphoma 2009, 48, 1940–1949. [Google Scholar] [CrossRef]
- Milanovic, D.; Sticht, C.; Röhrich, M.; Maier, P.; Grosu, A.-L.; Herskind, C. Inhibition of 13-cis retinoic acid-induced gene expression of reactive-resistance genes by thalidomide in glioblastoma tumoursin vivo. Oncotarget 2015, 6, 28938–28948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramírez-Flores, P.N.; Barraza-Reyna, P.J.; Aguirre-Vázquez, A.; Camacho-Moll, M.E.; Guerrero-Beltrán, C.E.; Resendez-Pérez, D.; González-Villasana, V.; Garza-González, J.N.; Silva-Ramírez, B.; Castorena-Torres, F.; et al. Isotretinoin and Thalidomide Down-Regulate c-MYC Gene Expression and Modify Proteins Associated with Cancer in Hepatic Cells. Molecules 2021, 26, 5742. [Google Scholar] [CrossRef] [PubMed]
- Austin, A.S.; Mahida, Y.R.; Clarke, D.; Ryder, S.D.; Freeman, J.G. A pilot study to investigate the use of oxpentifylline (pentoxifylline) and thalidomide in portal hypertension secondary to alcoholic cirrhosis. Aliment. Pharmacol. Ther. 2004, 19, 79–88. [Google Scholar] [CrossRef]
- Bekker, L.G.; Haslett, P.; Maartens, G.; Steyn, L.; Kaplan, G. Thalidomide-Induced Antigen-Specific Immune Stimulation in Patients with Human Immunodeficiency Virus Type 1 and Tuberculosis. J. Infect. Dis. 2000, 181, 954–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, J.P.; Orbell, G.; Cave, N.; Munday, J.S. Does thalidomide prolong survival in dogs with splenic haemangiosarcoma? J. Small Anim. Pract. 2018, 59, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Casseb, J.; Fonseca, L.A.M.; Veiga, A.P.R.; de Almeida, A.; Bueno, A.; Ferez, A.C.; Gonsalez, C.R.; Brigido, L.F.M.; Mendonça, M.; Rodrigues, R.; et al. AIDS Incidence and Mortality in a Hospital-Based Cohort of HIV-1–Seropositive Patients Receiving Highly Active Antiretroviral Therapy in São Paulo, Brazil. AIDS Patient Care STDs 2003, 17, 447–452. [Google Scholar] [CrossRef]
- Deng, Y.; Wei, W.; Wang, Y.; Pan, L.; Du, G.; Yao, H.; Tang, G. A Randomized controlled clinical trial on dose optimization of thalidomide in maintenance treatment for recurrent aphthous stomatitis. J. Oral Pathol. Med. 2021, 51, 106–112. [Google Scholar] [CrossRef]
- Domingo, S.; Solé, C.; Moliné, T.; Ferrer, B.; Ordi-Ros, J.; Cortés-Hernández, J. Efficacy of Thalidomide in Discoid Lupus Erythematosus: Insights into the Molecular Mechanisms. Dermatology 2020, 236, 467–476. [Google Scholar] [CrossRef]
- Fang, J.; Chen, X.; Zhu, B.; Ye, H.; Zhang, W.; Guan, J.; Su, K. Thalidomide for Epistaxis in Patients with Hereditary Hemorrhagic Telangiectasia: A Preliminary Study. Otolaryngol.—Head Neck Surg. 2017, 157, 217–221. [Google Scholar] [CrossRef]
- Gonçalves, F. Thalidomide for the Control of Severe Paraneoplastic Pruritus Associated With Hodgkin’s Disease. Am. J. Hosp. Palliat. Med. 2010, 27, 486–487. [Google Scholar] [CrossRef]
- Hammond, E.R.; Kaplin, A.I.; Kerr, D.A. Thalidomide for acute treatment of neurosarcoidosis. Spinal Cord 2007, 45, 802–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harte, M.C.; Saunsbury, T.A.; Hodgson, T.A. Thalidomide use in the management of oromucosal disease: A 10-year review of safety and efficacy in 12 patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 130, 398–401. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Mao, R.; Chen, F.; Xu, P.-P.; Chen, B.-L.; Wu, Y.; Qiu, Y.; Zhang, S.-H.; Feng, R.; Zeng, Z.-R.; et al. Thalidomide induces clinical remission and mucosal healing in adults with active Crohn’s disease: A prospective open-label study. Therap. Adv. Gastroenterol. 2017, 10, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Kropff, M.; Baylon, H.G.; Hillengass, J.; Robak, T.; Hajek, R.; Liebisch, P.; Goranov, S.; Hulin, C.; Blade, J.; Caravita, T.; et al. Thalidomide versus dexamethasone for the treatment of relapsed and/or refractory multiple myeloma: Results from OPTIMUM, a randomized trial. Haematologica 2011, 97, 784–791. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.J.; Kim, K.W.; Lee, H.M.; Nahm, F.S.; Lim, Y.J.; Park, J.H.; Kim, C.S. The effect of thalidomide on spinal cord ischemia/reperfusion injury in a rabbit model. Spinal Cord 2006, 45, 149–157. [Google Scholar] [CrossRef]
- Liu, Y.; Li, H.; Matsui, O. The antiangiogenic effect of thalidomide on occult liver metastases: Anin vivostudy in mice. J. Gastroenterol. Hepatol. 2009, 24, 1077–1081. [Google Scholar] [CrossRef]
- Misawa, S.; Sato, Y.; Katayama, K.; Nagashima, K.; Aoyagi, R.; Sekiguchi, Y.; Sobue, G.; Koike, H.; Yabe, I.; Sasaki, H.; et al. Safety and efficacy of thalidomide in patients with POEMS syndrome: A multicentre, randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2016, 15, 1129–1137. [Google Scholar] [CrossRef]
- Purev, U.; Chung, M.J.; Oh, D.-H. Individual differences on immunostimulatory activity of raw and black garlic extract in human primary immune cells. Immunopharmacol. Immunotoxicol. 2012, 34, 651–660. [Google Scholar] [CrossRef]
- Reid, J.; Mills, M.; Cantwell, M.M.; Cardwell, C.R.; Murray, L.J.; Donnelly, M. Thalidomide for managing cancer cachexia. Cochrane Database Syst. Rev. 2012, 2021, CD008664. [Google Scholar] [CrossRef]
- Seng, B.J.J.; Teo, L.L.Y.; Chan, L.L.; Sim, D.K.L.; Kerk, K.L.; Soon, J.L.; Tan, T.E.; Sivathasan, C.; Lim, C.P. Novel Use of Low-dose Thalidomide in Refractory Gastrointestinal Bleeding in Left Ventricular Assist Device Patients. Int. J. Artif. Organs 2017, 40, 636–640. [Google Scholar] [CrossRef]
- Singhal, S.; Mehta, J.; Desikan, R.; Ayers, D.; Roberson, P.; Eddlemon, P.; Munshi, N.; Anaissie, E.; Wilson, C.; Dhodapkar, M.; et al. Antitumor Activity of Thalidomide in Refractory Multiple Myeloma. N. Engl. J. Med. 1999, 341, 1565–1571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tramontana, J.M.; Utaipat, U.; Molloy, A.; Akarasewi, P.; Burroughs, M.; Makonkawkeyoon, S.; Johnson, B.; Klausner, J.D.; Rom, W.; Kaplan, G. Thalidomide Treatment Reduces Tumor Necrosis Factor α Production and Enhances Weight Gain in Patients with Pulmonary Tuberculosis. Mol. Med. 1995, 1, 384–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turan, E.; Ardic, N.; Sürücü, H.A.; Aksoy, M.; Satoskar, A.R.; Varikuti, S.; Doni, N.; Oghumu, S.; Yesilova, A.; Yeşilova, Y. A Comparison of Demographic and Clinical Characteristics of Syrian and Turkish Patients with Cutaneous Leishmaniasis. Am. J. Trop. Med. Hyg. 2015, 93, 559–563. [Google Scholar] [CrossRef] [Green Version]
- Tusa, M.G.; Pearce, D.; Camacho, F.; Willard, J.; McCarty, A.; Feldman, S.R. An Open-Label Trial of Thalidomide in the Treatment of Chronic Plaque Psoriasis. Psoriasis Forum 2018, 15a, 19–22. [Google Scholar] [CrossRef]
- Vergara, T.R.C.; Samer, S.; Santos-Oliveira, J.R.; Giron, L.B.; Arif, M.S.; Silva-Freitas, M.L.; Cherman, L.A.; Treitsman, M.S.; Chebabo, A.; Sucupira, M.C.A.; et al. Thalidomide is Associated With Increased T Cell Activation and Inflammation in Antiretroviral-naive HIV-infected Individuals in a Randomised Clinical Trial of Efficacy and Safety. EBioMedicine 2017, 23, 59–67. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Zhang, Y.; Pan, M. Thalidomide as a potential adjuvant treatment for paraneoplastic pemphigus: A single-center experience. Dermatol. Ther. 2020, 33, e14353. [Google Scholar] [CrossRef]
- Zhang, B.; Mao, X.; Zhao, W.; Jin, H.; Li, L. Successful treatment with thalidomide for pemphigus vulgaris. Ther. Adv. Chronic Dis. 2020, 11, 2040622320916023. [Google Scholar] [CrossRef]
- Kwon, H.Y.; Han, Y.J.; Im, J.H.; Baek, J.H.; Lee, J.S. Two cases of immune reconstitution inflammatory syndrome in HIV patients treated with thalidomide. Int. J. STD AIDS 2019, 30, 1131–1135. [Google Scholar] [CrossRef]
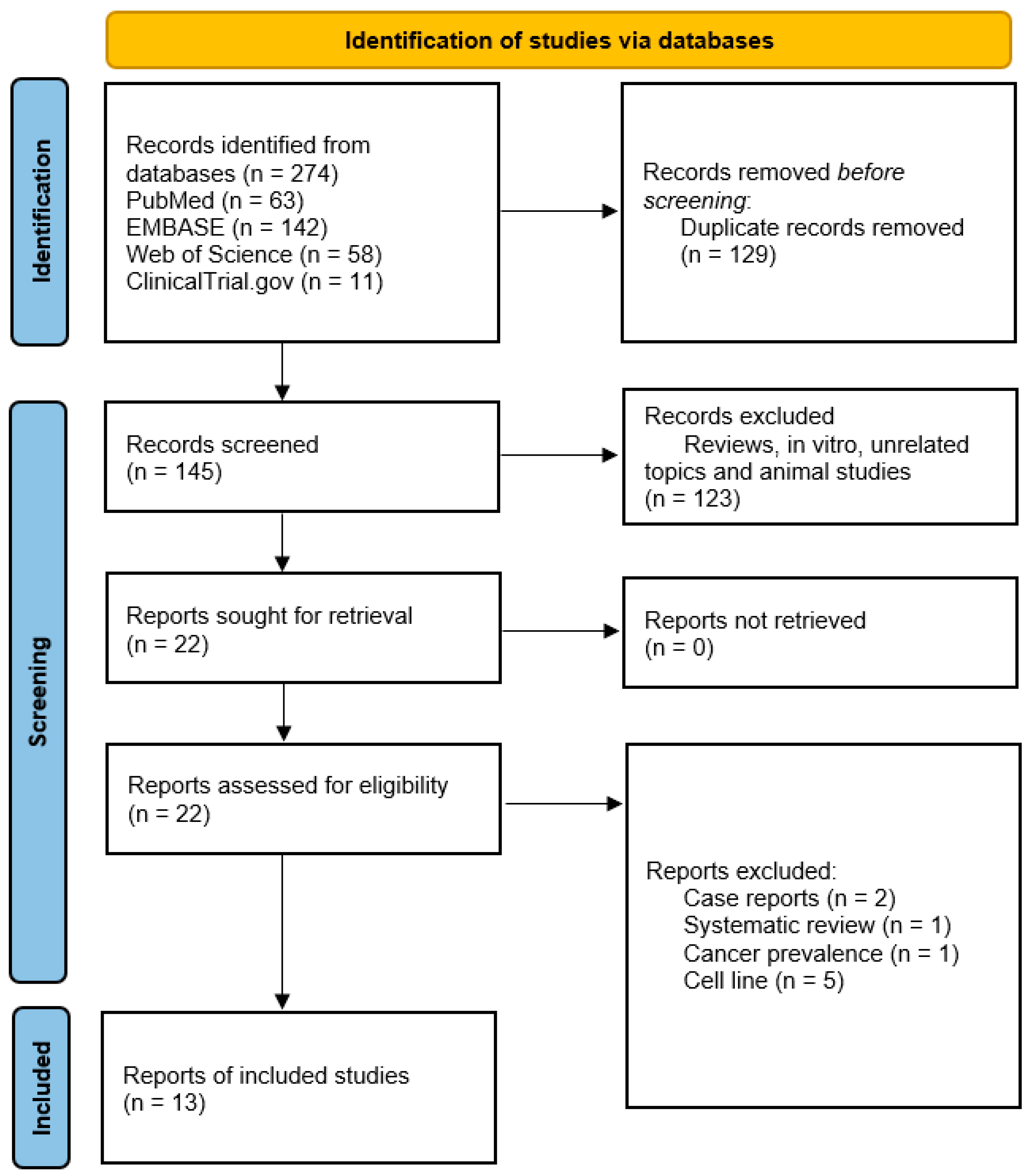
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Stewart, A.K. Medicine. How thalidomide works against cancer. Science 2014, 343, 256–257. [Google Scholar] [CrossRef] [Green Version]
- Eleutherakis-Papaiakovou, V.; Bamias, A.; Dimopoulos, M.A. Thalidomide in cancer medicine. Ann. Oncol. 2004, 15, 1151–1160. [Google Scholar] [CrossRef] [PubMed]
- Richardson, P.; Hideshima, T.; Anderson, K. Thalidomide: Emerging role in cancer medicine. Annu. Rev. Med. 2002, 53, 629–657. [Google Scholar] [CrossRef] [PubMed]
- Morabito, A.; Fanelli, M.; Carillio, G.; Gattuso, D.; Sarmiento, R.; Gasparini, G. Thalidomide prolongs disease stabilization after conventional therapy in patients with recurrent glioblastoma. Oncol. Rep. 2004, 11, 93–95. [Google Scholar] [CrossRef] [PubMed]
- Marx, G.M.; Pavlakis, N.; McCowatt, S.; Boyle, F.M.; Levi, J.A.; Bell, D.R.; Cook, R.; Biggs, M.; Little, N.; Wheeler, H.R. Phase II study of thalidomide in the treatment of recurrent glioblastoma multiforme (GBM). J. Neuro-Oncol. 2001, 54, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Fine, H.A.; Figg, W.D.; Jaeckle, K.; Wen, P.Y.; Kyritsis, A.P.; Loeffler, J.S.; Levin, V.A.; Black, P.M.; Kaplan, R.; Pluda, J.M.; et al. Phase II Trial of the Antiangiogenic Agent Thalidomide in Patients With Recurrent High-Grade Gliomas. J. Clin. Oncol. 2000, 18, 708. [Google Scholar] [CrossRef]
- Fadul, C.E.; Kingman, L.S.; Meyer, L.P.; Cole, B.F.; Eskey, C.J.; Rhodes, C.H.; Roberts, D.W.; Newton, H.B.; Pipas, J.M. A phase II study of thalidomide and irinotecan for treatment of glioblastoma multiforme. J. Neuro-Oncol. 2008, 90, 229–235. [Google Scholar] [CrossRef] [Green Version]
- Puduvalli, V.K.; Giglio, P.; Groves, M.D.; Hess, K.R.; Gilbert, M.R.; Mahankali, S.; Jackson, E.F.; Levin, V.A.; Conrad, C.A.; Hsu, S.H.; et al. Phase II trial of irinotecan and thalidomide in adults with recurrent glioblastoma multiforme. Neuro-Oncology 2008, 10, 216–222. [Google Scholar] [CrossRef] [Green Version]
- Alexander, B.M.; Wang, M.; Yung, W.K.A.; Fine, H.A.; Donahue, B.A.; Tremont, I.W.; Richards, R.S.; Kerlin, K.J.; Hartford, A.C.; Curran, W.J.; et al. A phase II study of conventional radiation therapy and thalidomide for supratentorial, newly-diagnosed glioblastoma (RTOG 9806). J. Neuro-Oncol. 2012, 111, 33–39. [Google Scholar] [CrossRef]
- Chang, S.M.; Lamborn, K.R.; Malec, M.; Larson, D.; Wara, W.; Sneed, P.; Rabbitt, J.; Page, M.; Nicholas, M.K.; Prados, M.D. Phase II study of temozolomide and thalidomide with radiation therapy for newly diagnosed glioblastoma multiforme. Int. J. Radiat. Oncol. Biol. Phys. 2004, 60, 353–357. [Google Scholar] [CrossRef]
- Iwamoto, F.M.; Lassman, A.B. Factorial clinical trials: A new approach to phase II neuro-oncology studies. Neuro-Oncology 2014, 17, 174–176. [Google Scholar] [CrossRef] [Green Version]
- Milanovic, D.; Maier, P.; Schanne, D.H.; Wenz, F.; Herskind, C. The influence of retinoic Acid and thalidomide on the radiosensitivity of u343 glioblastoma cells. Anticancer Res. 2014, 34, 1885–1891. [Google Scholar]
- Penas-Prado, M.; Hess, K.R.; Fisch, M.J.; Lagrone, L.W.; Groves, M.D.; Levin, V.A.; De Groot, J.F.; Puduvalli, V.K.; Colman, H.; Volas-Redd, G.; et al. Randomized phase II adjuvant factorial study of dose-dense temozolomide alone and in combination with isotretinoin, celecoxib, and/or thalidomide for glioblastoma. Neuro-Oncology 2015, 17, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Riva, M.; Imbesi, F.; Beghi, E.; Galli, C.; Citterio, A.; Trapani, P.; Sterzi, R.; Collice, M. Temozolomide and thalidomide in the treatment of glioblastoma multiforme. Anticancer Res. 2007, 27, 1067–1071. [Google Scholar] [PubMed]
- Hassler, M.R.; Sax, C.; Flechl, B.; Ackerl, M.; Preusser, M.; Hainfellner, J.A.; Woehrer, A.; Dieckmann, K.U.; Rössler, K.; Prayer, D.; et al. Thalidomide as Palliative Treatment in Patients with Advanced Secondary Glioblastoma. Oncology 2015, 88, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Ai, X.; Song, Z.; Jian, H.; Zhou, Z.; Chen, Z.; Yu, Y.; Li, Z.; Lu, S. Pyrotinib combined with thalidomide in advanced non-small-cell lung cancer patients harboring HER2 exon 20 insertions (PRIDE): Protocol of an open-label, single-arm phase II trial. BMC Cancer 2021, 21, 1033. [Google Scholar] [CrossRef]
- Chanan-Khan, A.; Miller, K.C. Velcade, Doxil and Thalidomide (VDT) is an effective salvage regimen for patients with relapsed and refractory multiple myeloma. Leuk. Lymphoma 2009, 46, 1103–1104. [Google Scholar] [CrossRef]
- Chen, C.; Qi, F.; Shi, K.; Li, Y.; Li, J.; Chen, Y.; Pan, J.; Zhou, T.; Lin, X.; Zhang, J.; et al. Thalidomide combined with low-dose short-term glucocorticoid in the treatment of critical Coronavirus Disease 2019. Clin. Transl. Med. 2020, 10, e35. [Google Scholar] [CrossRef]
- Clark, P.E.; Hall, M.C.; Miller, A.; Ridenhour, K.P.; Stindt, D.; Lovato, J.F.; Patton, S.E.; Brinkley, W.; Das, S.; Torti, F.M. Phase II trial of combination interferon-alpha and thalidomide as first-line therapy in metastatic renal cell carcinoma. Urology 2004, 63, 1061–1065. [Google Scholar] [CrossRef]
- Emre, S.; Sumrani, N.; Hong, J. Beneficial Effect of Thalidomide and Ciclosporin Combination in Heterotopic Cardiac Transplantation in Rats. Eur. Surg. Res. 1990, 22, 336–339. [Google Scholar] [CrossRef]
- Giglio, P.; Dhamne, M.; Hess, K.R.; Gilbert, M.R.; Groves, M.D.; Levin, V.A.; Kang, S.L.; Ictech, S.E.; Liu, V.; Colman, H.; et al. Phase 2 trial of irinotecan and thalidomide in adults with recurrent anaplastic glioma. Cancer 2012, 118, 3599–3606. [Google Scholar] [CrossRef]
- Hoang, T.; Dahlberg, S.E.; Schiller, J.H.; Mehta, M.P.; Fitzgerald, T.J.; Belinsky, S.A.; Johnson, D.H. Randomized Phase III Study of Thoracic Radiation in Combination With Paclitaxel and Carboplatin With or Without Thalidomide in Patients With Stage III Non–Small-Cell Lung Cancer: The ECOG 3598 Study. J. Clin. Oncol. 2012, 30, 616–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.M.; Rudd, R.; Woll, P.J.; Ottensmeier, C.; Gilligan, D.; Price, A.; Spiro, S.; Gower, N.; Jitlal, M.; Hackshaw, A. Randomized Double-Blind Placebo-Controlled Trial of Thalidomide in Combination With Gemcitabine and Carboplatin in Advanced Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2009, 27, 5248–5254. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Qiu, Y.; Li, X.; Zhuang, X.; Huang, S.; Li, M.; Feng, R.; Chen, B.; He, Y.; Zeng, Z.; et al. Thalidomide Combined With Azathioprine as Induction and Maintenance Therapy for Azathioprine-Refractory Crohn’s Disease Patients. Front. Med. 2020, 7, 557986. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Han, Z.; Wang, X.; Mo, Z.; Zhang, W.; Li, A.; Liu, S. Combination therapy of infliximab and thalidomide for refractory entero-Behcet’s disease: A case report. BMC Gastroenterol. 2013, 13, 167. [Google Scholar] [CrossRef] [Green Version]
- McCollum, A.D.; Wu, B.; Clark, J.W.; Kulke, M.H.; Enzinger, P.C.; Ryan, D.P.; Earle, C.C.; Michelini, A.; Fuchs, C.S. The Combination of Capecitabine and Thalidomide in Previously Treated, Refractory Metastatic Colorectal Cancer. Am. J. Clin. Oncol. 2006, 29, 40–44. [Google Scholar] [CrossRef]
- Mi, R.; Chen, L.; Yang, H.; Zhang, Y.; Liu, J.; Yin, Q.; Wei, X. Combined use of interferon alpha-1b, interleukin-2, and thalidomide to reverse the AML1-ETO fusion gene in acute myeloid leukemia. Ann. Hematol. 2021, 100, 2593–2601. [Google Scholar] [CrossRef]
- Mita, M.M.; Rowinsky, E.K.; Forero, L.; Eckhart, S.G.; Izbicka, E.; Weiss, G.R.; Beeram, M.; Mita, A.C.; de Bono, J.S.; Tolcher, A.W.; et al. A phase II, pharmacokinetic, and biologic study of semaxanib and thalidomide in patients with metastatic melanoma. Cancer Chemother. Pharmacol. 2006, 59, 165–174. [Google Scholar] [CrossRef]
- Ning, Y.-M.; Gulley, J.L.; Arlen, P.M.; Woo, S.; Steinberg, S.M.; Wright, J.J.; Parnes, H.L.; Trepel, J.B.; Lee, M.-J.; Kim, Y.S.; et al. Phase II Trial of Bevacizumab, Thalidomide, Docetaxel, and Prednisone in Patients With Metastatic Castration-Resistant Prostate Cancer. J. Clin. Oncol. 2010, 28, 2070–2076. [Google Scholar] [CrossRef] [Green Version]
- Palladini, G.; Perfetti, V.; Perlini, S.; Obici, L.; Lavatelli, F.; Caccialanza, R.; Invernizzi, R.; Comotti, B.; Merlini, G. The combination of thalidomide and intermediate-dose dexamethasone is an effective but toxic treatment for patients with primary amyloidosis (AL). Blood 2005, 105, 2949–2951. [Google Scholar] [CrossRef]
- Ruddy, J.M.; Majumdar, S.K. Antitumorigenic Evaluation of Thalidomide Alone and in Combination with Cisplatin in DBA2/J Mice. J. Biomed. Biotechnol. 2002, 2, 7–13. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.; Sheth, R.; Shah, K.; Patel, K. Safety and effectiveness of thalidomide and hydroxyurea combination in β-thalassaemia intermedia and major: A retrospective pilot study. Br. J. Haematol. 2019, 188, e18–e21. [Google Scholar] [CrossRef] [PubMed]
- Tsenova, L.; Sokol, K.; Victoria, H.F.; Kaplan, G. A Combination of Thalidomide plus Antibiotics Protects Rabbits from Mycobacterial Meningitis-Associated Death. J. Infect. Dis. 1998, 177, 1563–1572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vallet, S.; Palumbo, A.; Raje, N.; Boccadoro, M.; Anderson, K.C. Thalidomide and lenalidomide: Mechanism-based potential drug combinations. Leuk. Lymphoma 2009, 49, 1238–1245. [Google Scholar] [CrossRef]
- Zduniak, K.; Gdesz-Birula, K.; Woźniak, M.; Duś-Szachniewicz, K.; Ziółkowski, P. The Assessment of the Combined Treatment of 5-ALA Mediated Photodynamic Therapy and Thalidomide on 4T1 Breast Carcinoma and 2H11 Endothelial Cell Line. Molecules 2020, 25, 5184. [Google Scholar] [CrossRef]
- Zheng, W.; Fu, L. Effect of thalidomide combined with TP chemotherapy on serum VEGF and NRP-1 levels advanced esophageal cancer patients. Am. J. Transl. Res. 2021, 13, 10809–10815. [Google Scholar]
- Ghobrial, I.M.; Rajkumar, S.V. Management of thalidomide toxicity. J. Support. Oncol. 2003, 1, 194–205. [Google Scholar]
- Ruiz, J.; Case, D.; Enevold, G.; Rosdhal, R.; Tatter, S.B.; Ellis, T.L.; McQuellon, R.P.; McMullen, K.P.; Stieber, V.W.; Shaw, E.G.; et al. A phase II trial of thalidomide and procarbazine in adult patients with recurrent or progressive malignant gliomas. J. Neurooncol. 2012, 106, 611–617. [Google Scholar] [CrossRef] [Green Version]
- Dimopoulos, M.A.; Eleutherakis-Papaiakovou, V. Adverse effects of thalidomide administration in patients with neoplastic diseases. Am. J. Med. 2004, 117, 508–515. [Google Scholar] [CrossRef]
- Grover, J.K.; Uppal, G.; Raina, V. The adverse effects of thalidomide in relapsed and refractory patients of multiple myeloma. Ann. Oncol. 2002, 13, 1636–1640. [Google Scholar] [CrossRef]
- Eriksson, T.; Bjorkman, S.; Hoglund, P. Clinical pharmacology of thalidomide. Eur. J. Clin. Pharmacol. 2001, 57, 365–376. [Google Scholar] [CrossRef]
- Morival, C.; Oumari, S.; Lenglet, A.; Le Corre, P. Clinical pharmacokinetics of oral drugs in the treatment of multiple myeloma. Hematol. Oncol. 2017, 36, 505–518. [Google Scholar] [CrossRef] [PubMed]
- Sherbet, G.V. Therapeutic Potential of Thalidomide and Its Analogues in the Treatment of Cancer. Anticancer Res. 2015, 35, 5767–5772. [Google Scholar] [PubMed]
- Baxter, K.; Preston, C.L. (Eds.) Stockley’s Drug Interactions, 9th ed.; Pharmaceutical Press: London, UK, 2010. [Google Scholar]
- Thalidomide (Rx) Interactions. Available online: https://reference.medscape.com/drug/thalomid-thalidomide-343211#3 (accessed on 5 April 2023).
- Thalidomide Drug Interactions. Available online: https://www.drugs.com/drug-interactions/thalidomide-index.html?filter=3 (accessed on 5 April 2023).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | Sample Size/Design | Outcomes/Measures | MOA | Ref. |
|---|---|---|---|---|
| Patients | ||||
| Cancer cachexia | 416 adult patients with advanced cancer and weight loss or cachexia | Control weight loss in advanced malignancy | Inhibits TNFα and NF-κB, and then limits downstream gene expression, which controls pro-inflammatory cytokines, cells’ growth, and control. Such direct control of NF-κB may help illuminate why THD appears to control severe weight loss with advanced cancers | [109] |
| Active Crohn’s disease | 47 adult patients with active Crohn’s disease received 50 mg THD orally, and then the dose was elevated to 75 mg or 100 mg according to clinical symptoms and tolerance | -Clinical remission at week 8, defined by a CDAI score -Endoscopic efficacy and clinical response | Decreases intestinal inflammatory activity and inflammatory markers (ESR and CRP) and restores mucosal integrity | [117] |
| Chronic Plaque Psoriasis | 20 patients treated with THD at 200 mg/day for eight weeks | THD efficacy in the treatment of psoriasis and in managing the severity of the disease measured by PASI and BSA | Inhibits TNFα | [100] |
| DLE | 60 patients with cutaneous lupus erythematosus, including 25 patients diagnosed with refractory DLE | 98% of patients improved after therapy, and 85% attained complete remission over eight years of follow up | -DLE patients had high serum VEGF, THD can decrease IL-10 and TGFβ/Treg production through its immunomodulatory effects on T-cells -THD can inhibit macrophage activation cytokine inhibition, promoting NK cell-mediated cytotoxicity | [98] |
| ENL | -22 men with ENL received six capsules containing 100 mg of THD (group A, n = 12) Or 300 mg THD (group B, n = 10) daily for a week -Then, group A was given 50 mg/day THD in weeks 2 and 3, then placebo capsules from weeks 4 to 7 -Group B had gradual decrements every two weeks | Resolution of inflamed ENL nodules through the initial seven-day of treatment | Inhibits TNFα associated with ENL toxicity | [94] |
| HHT | 7 HHT patients with recurrent epistaxis were treated with 50 mg/d THD and increased every week by 25 mg/d if no response happened by the third week. The maximum dose was 100 mg/d | THD efficacy for epistaxis that usually occurs in hereditary hemorrhagic telangiectasia | THD could cause blood vessel maturation through increasing expression PDGFRβ in endothelial cells and stimulated activation of the mural cell | [103] |
| 7 subjects aged between 48 and 75 years had HHT with severe, recurrent epistaxis and mutations in ENG or ACVRL1–3 subjects were untreated controls | THD lowered the frequency of epistaxis in subjects with HHT and reduced blood transfusion requirements | -Antihemorrhagic action through direct inhibition of endothelial cells -THD modulates mural cells activation by increasing their proliferation and forming protrusions that can embrace blood vessels and lead to vessel stabilization | [105] | |
| HIV-1 and Tuberculosis | 30 patients were seropositive for HIV-1 infection, never received antiretroviral treatment, and were hospitalized with a recent pulmonary tuberculosis diagnosis | THD effect on HIV levels in vivo and in vitro. -Efficacy of THD on the production of TNFα and Th1-type cytokines (IL-12 and IFNγ) in HIV-infected patients with TB | -Stimulated antigen-specific T cell immunity, as indicated through enhancement of T cell proliferation as a response to PPD -Immunostimulatory effect was indicated by increased plasma levels of some of the Th1-type cytokines and cytokine receptors, including IL-12, IFN-g, TNFαR, and IL-2R -THD increases numbers of CD41 and CD81 T cells and plasma sCD8 levels and stimulates endogenous IL-12 production | [96] |
| HIV-1 | -30 adult antiretroviral naïve males with CD4 ≥ 350 cells/mm3 -16 had 200 mg of THD for three weeks; 14 patients in the control group; then, they were followed for 48 weeks | Investigated if THD would decrease HIV replication and the inflammations related to it via measuring CD4/CD8 ratio, CD4 cells count, the percentage of CD38+/HLA-DR+ CD8 cells and US-CRP | Amendment of inflammatory cytokines as IFNγ, TNFα, IL-12, IL-10, COX2, and NF-κB | |
| IBD | 248 patients, including 92 pediatric patients: 192 administered THD, and 56 with Crohn’s disease administered lenalidomide | Induction of remission in pediatric Crohn’s disease | Blocks NF-kB activation after the suppression of IkB kinase activity; THD blocks VEGF and cell adhesion molecule expression in HIMEC | [98] |
| LVAD patients with GIB | 78 patients with LVAD implantation for end-stage heart failure | -Evaluation of efficacy and safety of THD at low dose in the management of LVAD-related GIB | Suppresses VEGF, which implicates arteriovenous malformations | [99] |
| Multiple myeloma | -84 patients with myeloma, previously treated and progressed -All patients received oral THD for an average of 80 days -The dose started with 200 mg daily, then increased by 200 mg every two weeks until it reached 800 mg per day | Evaluate the efficacy of THD as an antiangiogenic agent in patients with resistant disease | -THD alters the adhesion molecules’ expression and suppresses TNFα production; it increases the production of IL-10 and average soluble IL-2 receptor plasma levels and the total number of lymphocytes, CD4+, and CD8+ T-cell counts -Enhances cell-mediated immunity through cytotoxic T cells’ direct stimulation -Interacts with type 1 and type 2 helper T cells and produces complex effects on levels of cytokines as IL-4, IL-5, and IFNγ | [112] |
| Multiple myeloma | -499 eighteen years or more patients -They already had received one to three lines of treatment “three different doses of THD (100, 200, or 400 mg/day)” and required additional therapy because of disease progression | -Primary outcome is to compare the time of progression and to know the ideal THD dose considering the time to progression and toxicity. -Secondary ones showed efficacy of THD in the following: -response rate -progression-free survival -overall survival | Unclear | [93] |
| Neurosarcoidosis | 42 years old African American male started THD orally at 400 mg daily for 30-day course | To assess improvement clinically and on MRI | THD is an immunomodulatory drug that inhibits the production of TNFα through enhancing TNFα mRNA degradation; it also produces inhibition of IL-6 upregulation and down-regulates the action of NF-kB, both of which are elevated and essential in CNS inflammation, as in neurosarcoidosis | [102] |
| Nodular sclerosis type II Hodgkin lymphoma | A 22-year-old woman on 200 mg at night | THD efficacy in controlling severe paraneoplastic pruritus | THD has antipruritic action that can be due to its inhibition of TNFα, or due to its central depressive action | [110] |
| Oro mucosal disease | -12 patients were given THD through a period of ulcerative oromucosal condition (recurrent aphthous stomatitis, HIV-related oral ulceration, and oral manifestation of Crohn’s disease) | THD had an excellent efficacy-to-safety ratio in managing oro-mucosal ulceration over a prolonged treatment period | Modulation of inflammatory cascade and interaction with various cytokines, such as TNFα, IL-6, and IL-10 | [116] |
| PNP | -12 patients after treatment from associated tumor administered THD (75–100 mg/day) -THD combined with or without low- to mild-dose oral prednisone | -THD could be a safe, effective, and economical treatment choice for PNP patients -The potential of THD in the treatment of PNP through scores of PDAI | -IL-10 and IL-6 were reported to be at raised levels in serum of PNP patients -THD inhibits TNFα, VEGF, IL-6, IL-12, IL-1, IL-10, and IFNγ, and maybe NF-кB -For associated tumors, THD may cause down-regulation of VEGF | [95] |
| POEMS syndrome | 24 adults aged 20 years or more with definite or probable POEMS. | A reduction rate in the concentration of serum VEGF | -THD reduces serum VEGF concentrations and can suppress monoclonal plasma cell proliferation -It causes modulation of up-regulated pro-inflammatory cytokines, such as TNFα, IL6, and IL12 | [114] |
| Portal hypertension secondary to alcoholic cirrhosis | 20 alcoholic cirrhosis and current or previously esophageal varices patients | Assessment of THD and oxpentifylline in liver cirrhosis and also their effects on hepatic venous pressure and creation of TNFα | THD reduced hepatic venous pressure gradient through the inhibition of TNFα production | [106] |
| Pulmonary Tuberculosis | -30 male cases of active TB with either negative or positive HIV1 -They received THD for single or multiple fourteen-day cycles or placebo | -THD did not adversely affect the response of DTH to PPD, differential cell counts, or total leukocytes -Daily intake of THD led to a significant enhancement in weight gain | THD suppresses TNFα production; it increases IFNγ secretion in vivo, in the patient’s serum, and in vitro by PBMCs stimulated by mycobacterium | [113] |
| PV | 6 cases aged between 38 and 67 | Appraisal of the safety and efficacy of THD with PV patients | THD inhibits inflammatory cytokines production, including IL-7 and TNFα, and may up-regulate the expression of desmoglein in epidermal keratinocytes as a compensatory mechanism; it also regulates local immunity in the epidermis that contributes to pemphigus pathogenesis | [115] |
| RAS | -113 patients aged between 18–75 with a history of RAS for about 12 months -The patient had occurrences of aphthae one or two times in one month before enrollment -Fresh minor ulcers presented within two days of eruption without systemic or topical medication treatment -Women refused to become pregnant and started menopause -Men decided to use birth control measures with their partners | -25 mg/d THD extended the recurrence interval of RAS, with better safety through its long-term effect -The primary outcomes were the recurrence interval and total of ulcer-free days -Secondary outcomes were the number of ulcers and the visual analog scale | Unclear | [107] |
| Animal | ||||
| Breast cancer | 15 six-week-old female mice | THD’s ability to inhibit the tumor cells and the ability to aggregate and create primary tumors at the injection site | -Delays the capability of a single cell suspension of 4T1 cells to aggregate and create primary tumors -Reduces the density of surface molecules of 4T1 cells implicated in adhesion which would delay the ability of these cells to assemble and create tumors | [111] |
| Hepatic metastases | 20 mice with induced hepatic metastases | Morphological changes in microvessels intratumorally next to THD management in occult hepatic metastases | THD has an antiangiogenic effect that discourages vascular formation, indirectly discouraging tumor progression during the early stages | [108] |
| HIV-1 | -30 adult antiretroviral naïve males with CD4 ≥ 350 cells/mm3 -16 have 200 mg of THD for three weeks and 14 patients in the control group; then, they were followed for 48 weeks | Investigated if THD would decrease HIV replication and the inflammations related to it via measuring CD4/CD8 ratio, CD4 cells count, the percentage of CD38+/HLA-DR+ CD8 cells and US-CRP | THD acts as an immunomodulatory, anti-inflammatory, and antiangiogenic drug; it causes the amendment of inflammatory cytokines such as IFNγ, TNFα, IL-12, IL-10, COX2, and NF-κB; THD’s anti-inflammatory effect is exerted by enhancing the degradation of TNFα mRNA | [104] |
| Spinal cord ischemia/reperfusion injury | 54 male rabbits | THD lowered the early-stage ischemia/reperfusion damage of the spinal cord in rabbits | -Inhibits TNFα by enhancing the degradation of TNFα mRNA -THD is a target cell-dependent drug which can target microglia cells; hence, THD can inhibit TNFα production by lipoarabinomannan- or lipopolysaccharide-aroused human microglial cells | [101] |
| Splenic HSA | 15 dogs with a histological diagnosis of HSA and recovery after splenectomy | -The HSA was the primary endpoint for the study -Investigation of the efficacy of THD as an adjuvant drug for canines that diseased by hemangiosarcoma | -THD cannot interrupt the progression of a macroscopic lesion longer -THD can suppress SDF1α, CXCR4, and NF-κB, which can influence the expression of several angiogenesis genes, such as VEGF, β-FGF, and HGF; it can also co-stimulate primary human T lymphocytes, which increases their anticancer activity | [97] |
| Combination | Mechanism of Action | Uses | Ref. |
|---|---|---|---|
| -5AZA and THD | Both drugs target the bone marrow microenvironment and cells via different mechanisms. THD has anti-cytokine and antiangiogenic activity, while AZA acts as a prodrug, binds to RNA, and inhibits protein synthesis, affecting the bone marrow microenvironment. After activation of AZA, it binds to DNA, causing cytotoxicity, hypomethylation, gene reactivation, suppression of enzyme methyltransferase, and cell differentiation of MDS | -Useful in treating all MDS types and AML patients with MDS history -In patients with high risks of AML and MDS (n = 40), the efficacy of the combined drug was at least as good as seven days of AZA alone -The survival after one year in continuous combined treatment of AZA and THD is comparable with continuous treatment with AZA | [86] |
| VDT | The development of therapeutic resistance and cell proliferation in multiple myeloma depends on the bone marrow’s microenvironment. The VDT combination has non-cross resistance, and non-overlapping toxicity as Doxil was a cytotoxic drug that targets the myeloma cells, and THD targets the microenvironment | -Well-tolerated in refractory cases of multiple myeloma (n = 6) | [136] |
| THD and AZN | In Crohn’s disease, TNFα is implicated in the inflammatory process. AZN has a synergistic impact with THD through its anti-TNFα activity by decreasing the responsiveness of biological treatment and boosting anti-TNFα levels. The synergistic effect of both drugs improves by modulation of T-cell immunity | -Achieving clinical remission (24 weeks, 70.5%) was well-tolerated in Crohn’s disease patients (n = 122) who did not respond to AZN monotherapy -Mucosal healing was achieved in 23.6% of the patients; 50.8% had adverse effects with a 63.6% endoscopic remission rate, and only 13 patients had to discontinue therapy intake | [143] |
| Capecitabine and THD | THD exerts its immunomodulatory effect, and capecitabine is a prodrug transformed to 5-fluorouracil in tissue via numerous enzymatic routes, and has the same effectiveness in colorectal cancer as 5-fluorouracil | -Treatment of refractory metastatic colorectal cancer (n = 34) revealed a low level of toxicity, such as thromboembolism, constipation, and hand-foot syndrome; however, 38% of the patients had stable disease, and the median progression-free survival rate was 2.6 months, while median overall survival was 7.1 months -There were no radiographic responses observed with therapy -No treatment response in cases treated previously from metastatic colorectal cancer | [145] |
| Interferon-α and THD | Interferon and THD are angiogenesis inhibitors that slow the progression of renal carcinoma | -The response of renal carcinoma is moderate to interferon and THD -In a study (n = 30) involving patients with renal cell carcinomas, the median follow-up time was 49.6 weeks, while the study’s median time of participation was 11.1 weeks -There were 29 patients with grade 2 toxicity -At 12 weeks, there was no complete response; there were 2 partial response patients, 8 with stable disease, and 11 patients showed disease progression -The median survival was 68 weeks The plasma concentration of THD has no connection to the dose -There was no link between medication level and treatment response or toxic effects | [138] |
| THD and FCT | Pathophysiology of acute leukemia depends on angiogenesis, contributes to the survival of leukemia cells, and resistance to chemotherapy-induced apoptosis The combination between THD and other chemotherapeutic drugs such as FCT may decrease the angiogenic process due to the ability of THD to block VEGF, thus inhibiting the formation of new vessels | -FCT is an effective therapy in recurrent leukemia patients (n = 42). Adding THD to this combination did not significantly increase efficacy or modify angiogenic markers such as VEGF or MVD -The total response rate in this trial with THD added to the FCT regimen is similar to the regimen seen in phase I when FCT was used alone (24% vs. 26%) -Adding THD results in thrombotic events and dermatological problems, which were not found in phase I using only FCT | [90] |
| Carboplatin and THD | Carboplatin is an antineoplastic agent that enhances the cell cycle, stimulates apoptosis, and inhibits cancer cell proliferation. Combining both drugs has an antiangiogenic effect through inhibiting cytokines VEGF, TNF, and Factor VIII expression in neoplastic cells | -THD and carboplatin combination effectively inhibit tumor proliferation and 4T1 murine breast cancer metastasis in the animal model -The treated group had a significantly increased animal survival rate compared with the control group (p = 0.0005) -Compared with the control group, there was a (62%) significant reduction in tumor growth after treatment (p < 0.05) -The number of lung metastases in the treated group was fewer than in the control group (p < 0.001) -There was a significant reduction in mitosis and an increase in apoptosis in the treated group compared with the control group (p < 0.05 and p < 0.001, respectively). -Immunohistochemical analysis of tumor vascularization revealed a higher reduction in the number of blood vessels in the intervention group than in the control (p < 0.001) | [74] |
| TMZ, THD, and celecoxib | TMZ is cytotoxic chemotherapy for the treatment of malignant gliomas. Malignant glioma cells’ secrets of angiogenic factors such as acidic FGF, bFGF, angiogenin, VEGF, platelets-derived growth factors, and IL 8 induce angiogenic process, increasing tumor proliferation. Combining TMZ with two angiogenic inhibitors such as THD and celecoxib inhibits these growth factors, inhibiting angiogenesis | The combination of TMZ, THD, and celecoxib is moderately well-tolerated but unlikely to significantly increase the survival of patients newly diagnosed with GBM (n = 50) | [87] |
| Bortezomib, THD-dexamethasone | Bortezomib causes inhibition of the action of proteasome, which results in cell apoptosis. Moreover, it inhibits the activation of NF-κB and regulatory protein toxic levels accumulation, but the mechanism leading to apoptosis of cells remains unclear. THD prevents angiogenesis. Finally, dexamethasone suppresses tumor growth and enhances the apoptosis of myeloma cells, but it does not release cytochrome C from mitochondria | -Bortezomib, THD, and dexamethasone combination were successful therapies for multiple myeloma patients (n = 38) -THD and dexamethasone increased induction remission in 66% of patients, but when adding bortezomib to the combination, remission occurred very fast in 87% of patients, including 16% with complete remission -Most side effects of the combination were mild | [88] |
| Thoracic radiation, paclitaxel, carboplatin, and THD | Inhibition of the angiogenesis process | Combining THD with chemoradiotherapy increased levels of toxicity (grade 3) such as fatigue, dizziness, thromboembolism, tremors, constipation, dyspnea, hypoxia, hypokalemia, rash, edema, sensory neuropathy, and depressed consciousness -Aspirin failed to decrease thromboembolism -THD did not increase survival in people with NSCLC (n = 546), so it was not recommended to add THD to these patients | [141] |
| THD, vincristine, liposomal doxorubicin, and dexamethasone (T-VAD Doxil) | VAD causes a reduction in tumor cells, especially liposomal doxorubicin, which increases the exposure of tumors cells to doxorubicin. THD works by its anti-myeloma mechanism, and hence, when combined with dexamethasone, it shows synergistic action | The combination was effective in treating myeloma patients (n = 39). Almost 74% of patients responded to treatment; of these, 10% had a complete response, 64% a partial response, 8% a minor response, and 18% did not respond to the treatment -Some patients showed grade 3 or 4 toxicity symptoms such as rash, thrombocytopenia, peripheral neuropathy, constipation, neutropenia, deep venous thrombosis, and 2 patients died due to infections | [85] |
| THD, IL-2 | The effective drug in RCC treatment is the combination immunotherapy drug such as THD with IL-2, which has immunomodulating and antineoplastic activity. Even though the entire mechanism is unknown, the THD/IL-2 combination was found to maintain RCC stability in some patients | -THD and IL-2 were effective in treating metastatic RCC according to phase 1 and phase 2 trials (n = 50), with the benefit ranging from 5–71 percent, with disease stability -The combination was relatively safe, and the only side effects were flu-like symptoms, hypotension, and hypothyroidism, all of which were linked to IL-2 treatment. Constipation, neuropathy, and rash are among the THD toxicity symptoms, and two patients had deep venous thromboses | [89] |
| Retinoic acid and THD | Retinoic acid induces the activity of resistance genes (HOXB7, bFGF, VEGF, and IL-8) that participate in GBM cell proliferation, hypoxia, and angiogenesis. THD inhibits HOXB7 and bFGF. THD causes suppression of HOXB7 and bFGF. Therefore, the combination shows synergistic action, as THD inhibits the induction of IL-8, IGFBP-3, HILPDA, and ANGPTL4 in GBM tumors, which are elevated by retinoic acid and linked to hypoxia and angiogenesis | The addition of THD to retinoic acid inhibited the development of human U251 GBM xenografts, and suppressed the resistance genes induced by retinoic acid; thus, this combination prevented hypoxia and angiogenesis linked to these genes | [91] |
| THD and cisplatin | Cisplatin is a toxic agent against murine erythroleukemic cells, and is known for its antimicrobial, immunosuppressive, and mutagenic effects, while THD exerts its effect through its anti-inflammatory and immunomodulatory properties | THD failed to suppress tumor and metastasis when given alone to DBA2/J mice, while cisplatin administration alone or with THD inhibited the multiplication of tumor cells | [150] |
| Bevacizumab, THD, docetaxel, and prednisone | THD suppresses FGF activity, the proliferation of endothelial cells, circulating endothelial cells, and the appearance of TNF. Bevacizumab keeps the balance of VEGF. Docetaxel has anti-tumor action | The combination helped reduce tumor volume of castration-resistant prostate cancer (n = 60), as the antiangiogenic agents THD and bevacizumab reduced the prostatic specific antigen and achieved an unprecedented response | [148] |
| Semaxanib and THD | THD down-regulates TNF α, IL-6, VEGF, and FGF. Semaxanib binds to VEGF-2 and causes its inhibition. It also inhibits the growth of A375 melanoma, C6 glioma, Calu-6 lung, and A431 epidermoid xenografts in athymic mice | -The combination of semaxanib and THD is proved to be a successful therapy in malignant melanoma (n = 12) -Headache, asthenia, constipation, edema in the lower limbs, neuropathy, hyperglycemia, hypercholesterolemia, and thrombosis were among the toxicity symptoms encountered by some individuals, whereas headache and thromboembolic symptoms were linked to semaxanib | [147] |
| THD and infliximab | Infliximab acts as a monoclonal antibody, helps balance TNFα, and down-regulates granulocyte-macrophage colony-stimulating factor expression, which was beneficial in treating TH1 disorders. THD suppresses the formation of TNFα by a mechanism that is different from infliximab | The combination is valuable in the management of refractory entero-Bechet’s disease (n = 1) | [144] |
| THD and antibiotics (rifampicin and isoniazid) | The anti-inflammatory THD agent enters the CSF and decreases TNFα in CSF and blood. Moreover, it decreases leukocytosis, and its penetration of CSF does not interfere with the action of antimycobacterial drugs | The combination of THD and (rifampicin and isoniazid) improved the survival rate of infected rabbits with mycobacterium tuberculosis | [152] |
| Pyrotinib and THD | Pyrotinib has been licensed as an effective and irreversible inhibitor of the epidermal growth factor receptor (EGFR)/HER2 identified in NSCLC. THD is effective in solid tumors due to its antiangiogenic and immunomodulatory effects | Since THD lowers diarrhea caused by pyrotinib, a combination of pyrotinib with THD is beneficial in managing NSCLC (n = 39) | [135] |
| THD and TP chemotherapy | THD and TP chemotherapy reduces VEGF and NRP-1, which are involved in esophageal cancer tumor angiogenesis | Effective in treating esophageal cancer and relieving associated nausea and vomiting (n = 133) | [155] |
| Glucocorticoids and THD | THD’s immunomodulatory and anti-inflammatory properties allow it to boost T cells, suppress cell growth, and reduce lung fibrosis and damage. THD also calms anxiety and reduces oxygen consumption due to its sedative effect. Glucocorticoids reduce cytokinesis levels | Glucocorticoids and THD in combination effectively relieve symptoms associated with pulmonary effusion without side effects (n = 1) | [137] |
| THD, IFNα-1b, and IL 2 | The combination of IL 2, IFNα-1b, and THD lowers minimal residual disease and reverses AML1-ETO fusion gene positivity in individuals with AML | IFNα-1b, IL-2, and THD are effective in the treatment of AML patients (n = 20), and the effective rate reached 72.2% | [146] |
| THD and lenalidomide | THD and lenalidomide have direct anti-tumor effects and affect the bone marrow microenvironment: THD has a cytotoxic effect in tumor cells, and lenalidomide inhibits the proliferation of multiple myeloma cells. They induce apoptosis by the down-regulation of NF-kB signaling and enhancing the intrinsic apoptosis pathway. Lenalidomide inhibits the expression of two anti-apoptotic proteins, cIAP-2 and FLICE inhibitory protein. Both proteins block apoptosis induced by TNF-related apoptosis | A broad spectrum of activities to treat multiple myelomas and other hematologic and solid malignancies | [153] |
| THD, gemcitabine, and carboplatin | THD has an anti-tumor impact on multiple myeloma by inhibiting angiogenesis, mediated by VEGF and bFGF. When coupled with chemotherapeutic drugs, it has a synergistic effect. In mice injected with NSCLC cell lines, THD slows tumor growth | -Overall survival did not improve when THD was combined with chemotherapy -In patients with NSCLC (n = 722), THD was not related to a survival benefit, although survival was lower in the group with non-squamous histology -The most severe side effects of THD were thrombotic events | [142] |
| THD and irinotecan | THD has immunomodulatory and antiangiogenic activities against malignant gliomas, while irinotecan is a topoisomerase-II suppressor | The combination of THD with irinotecan did not achieve enough effectiveness to warrant further investigation against anaplastic glioma (n = 39) although some patients achieved prolonged progression-free survival rate/overall survival rate | [140], |
| THD and ciclosporin | THD works similarly to ciclosporin in that it attaches to intracellular proteins, such as calmodulin and cyclophilin, which play a key role in immune response modulation; however, this has yet to be determined. THD interferes with neutrophil and lymphocyte function, causing suppression of the immune system | THD is an effective and potent immunosuppressive drug in preventing early refusal of cardiac allograft transplantation in rats when paired with low dosages of ciclosporin | [139] |
| THD and intermediate-dose dexamethasone | THD is beneficial in multiple myelomas because it decreases drug resistance in multiple myeloma plasma cells when combined with dexamethasone, so the study used THD and dexamethasone together to treat primary amyloidosis based on these findings | Second-line therapy for amyloidosis (n = 31) | [149] |
| 5-ALA-PDT and THD | 5-ALA-PDT is dependent on prodrug 5-ALA administration. It increases protoporphyrin IX in tumor cell production, and acts as a photosensitizer. After radiation therapy, protoporphyrin is excited, leading to ROS formation that causes a cytotoxic effect on tumor cells. Photodynamic therapy enhances VEGF expression and destroys vessels’ walls, leading to a reduction in tumor proliferation. THD inhibits VEGF and TNFα | -This combination was more effective than monotherapy of each agent on the 2H11 endothelial cell line and 4T1 breast carcinomas -In 2H11 cells, THD alone did not affect VEGF expression, but THD lowered VEGF expression once 5-ALA-PDT was administered | [154] |
| Isotretinoin and THD | Due to P1 or P2 promoter activity, isotretinoin and THD suppress c-MYC expression. Isotretinoin modifies TGFβ expression and also decrease TGFβ signaling degradation of pSMAD1 on the c-MYC promoter. AP-2 and c-MYC interact at the protein level, and AP-2 over-expression reduces c-MYC mRNA expression | -In hepatocellular carcinoma, c-MYC mRNA expression was significantly decreased by 80% (p < 0.05) in cells treated with THD and isotretinoin -Isotretinoin effects reduce HepG2 cell viability | [92] |
| THD and hydroxyurea | The immunomodulating and antiangiogenic effects of THD induce c-globin gene expression, and improve erythroid cell proliferation by amplifying ROS-p38 mitogen-activated protein kinase signaling and histone H4 acetylation during erythropoiesis Hydroxyurea increases hemoglobin by reducing inflammation, hypercoagulability, and induction of HbF expression, which could suppress ineffective erythropoiesis by reducing the build-up and precipitation of precipitation a-globin chains | -For patients with a high risk of organ rejection (n = 25), very high-risk transplant-related mortality and morbidity, or patients who are not willing to undergo a bone marrow transplant -May be used for transplantation in patients with ineligible thalassemia whose iron overload indicates a high risk of treatment-related harm, or who are awaiting donor identification | [151] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eatmann, A.I.; Hamouda, E.; Hamouda, H.; Farouk, H.K.; Jobran, A.W.M.; Omar, A.A.; Madeeh, A.K.; Al-dardery, N.M.; Elnoamany, S.; Abd-Elnasser, E.G.; et al. Potential Use of Thalidomide in Glioblastoma Treatment: An Updated Brief Overview. Metabolites 2023, 13, 543. https://doi.org/10.3390/metabo13040543
Eatmann AI, Hamouda E, Hamouda H, Farouk HK, Jobran AWM, Omar AA, Madeeh AK, Al-dardery NM, Elnoamany S, Abd-Elnasser EG, et al. Potential Use of Thalidomide in Glioblastoma Treatment: An Updated Brief Overview. Metabolites. 2023; 13(4):543. https://doi.org/10.3390/metabo13040543
Chicago/Turabian StyleEatmann, Ahmed Ismail, Esraa Hamouda, Heba Hamouda, Hossam Khaled Farouk, Afnan W. M. Jobran, Abdallah A. Omar, Alyaa Khaled Madeeh, Nada Mostafa Al-dardery, Salma Elnoamany, Eman Gamal Abd-Elnasser, and et al. 2023. "Potential Use of Thalidomide in Glioblastoma Treatment: An Updated Brief Overview" Metabolites 13, no. 4: 543. https://doi.org/10.3390/metabo13040543