3. Results
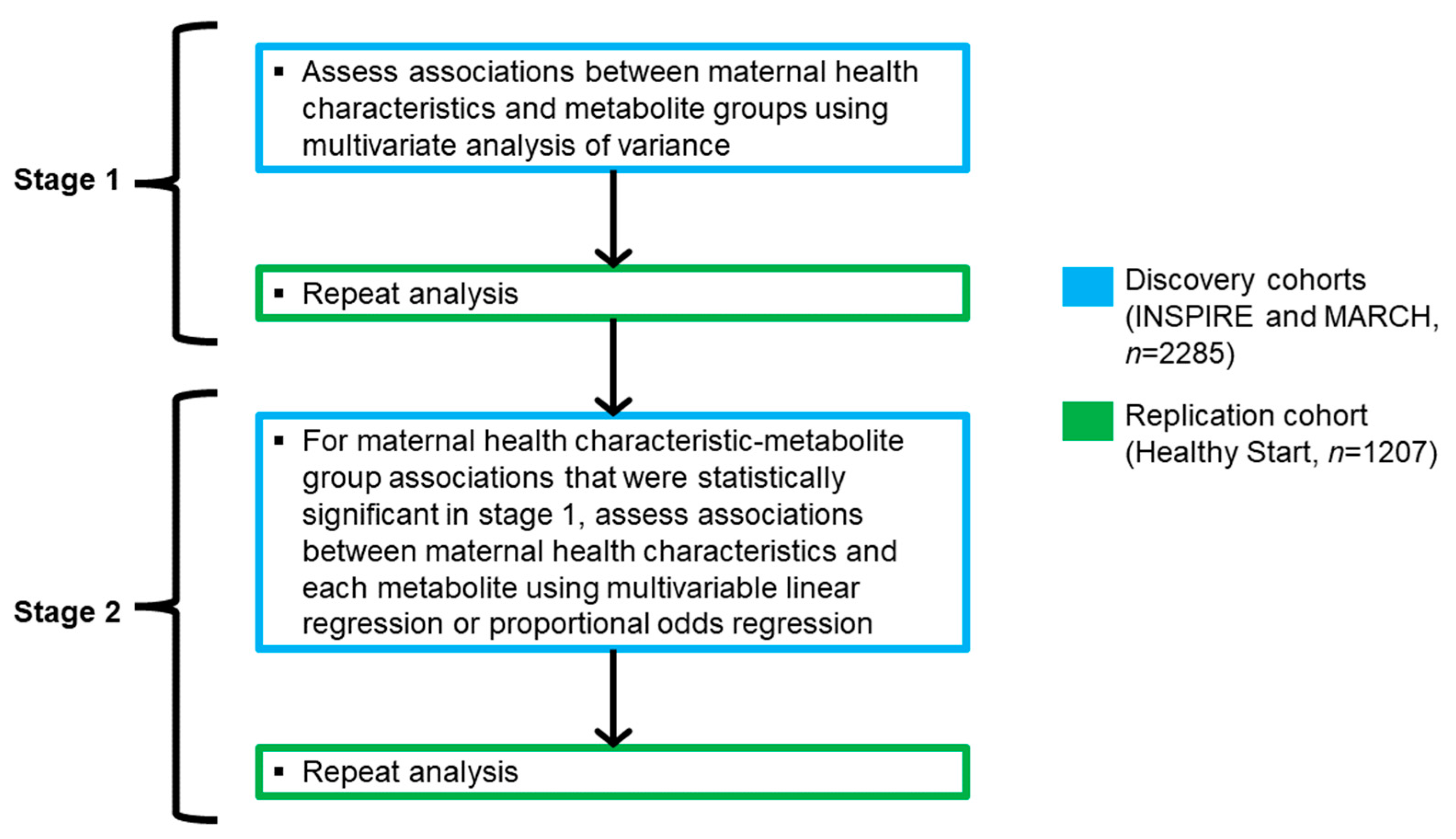
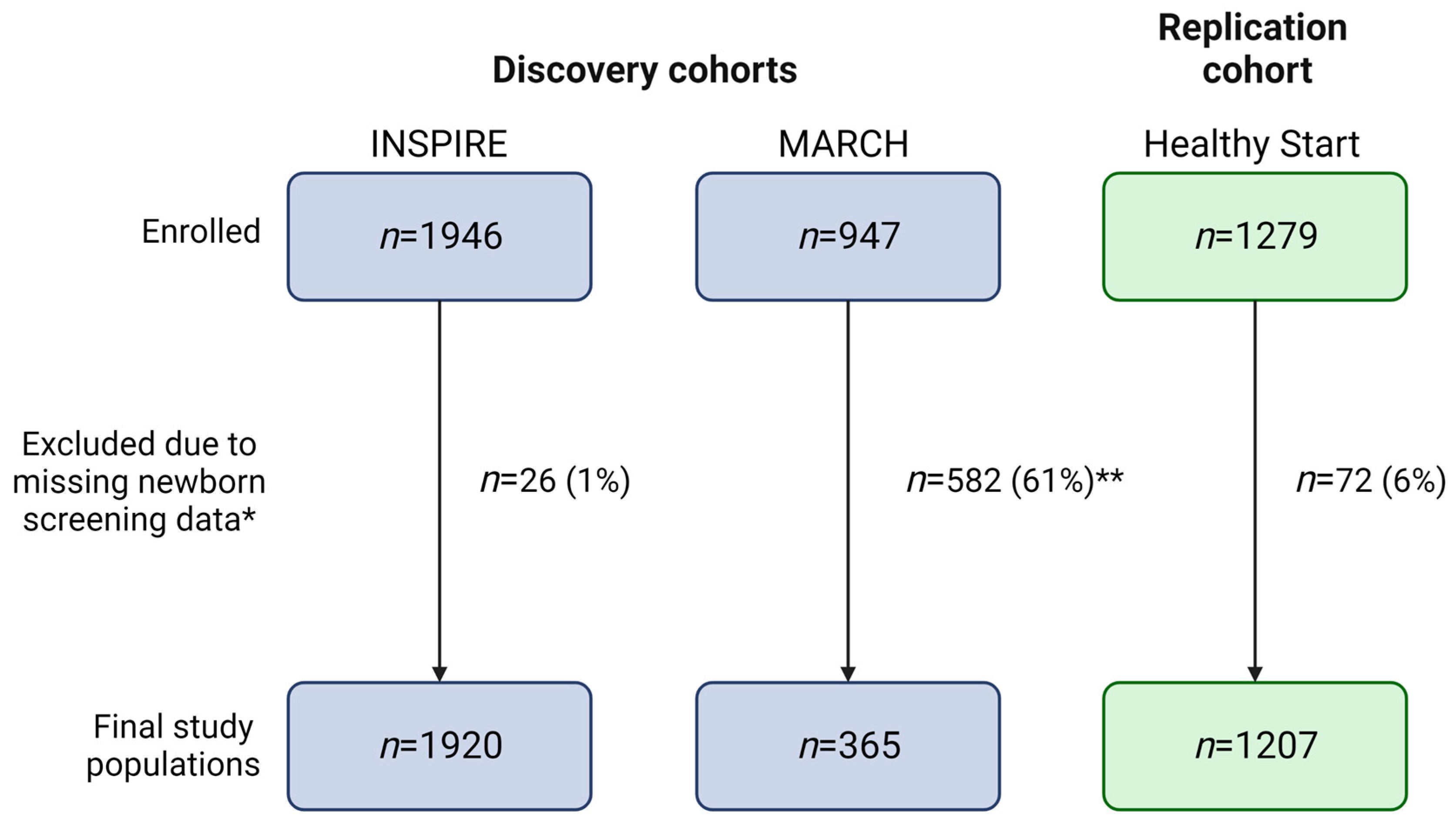
Our final study populations included 1920 (INSPIRE, discovery cohort), 365 (MARCH, discovery cohort), and 1207 (Healthy Start, replication cohort) infants after linking NBS metabolic data to 99%, 39%, and 94% of infants in each cohort, respectively (
Figure 3). As obtaining participant consent for NBS metabolic data linkage is currently ongoing for the MARCH cohort, we were only able to utilize data linked to 39% of the study population for the present study. We did not observe statistically significant differences between MARCH participants with NBS data and all MARCH participants (
Table S5).
The prevalence of maternal health characteristics differed between the cohorts, with prenatal smoking, higher pre-pregnancy BMI, lower education, not being married, gestational diabetes, and delivery via c-section being more prevalent among INSPIRE and MARCH participants than among Healthy Start participants (
Table 1). Maternal unemployment and higher maternal age at delivery were more prevalent among MARCH participants than INSPIRE and Healthy Start participants. Healthy Start participants had the lowest birth weights, and MARCH participants had the lowest gestational ages at birth (
Table 2). Healthy Start was more ethnically diverse than INSPIRE and MARCH, with 29% of infants of Hispanic descent compared to 8% and 9%, respectively in the other two cohorts. The majority of INSPIRE and Healthy Start participants were White (76% and 70%), while MARCH was more racially diverse (53% White, 26% Black, 13% other, 8% missing). INSPIRE participants were enrolled after birth (mean age 2 months, standard deviation [SD] 2 months), while MARCH and Healthy Start participants were enrolled at birth.
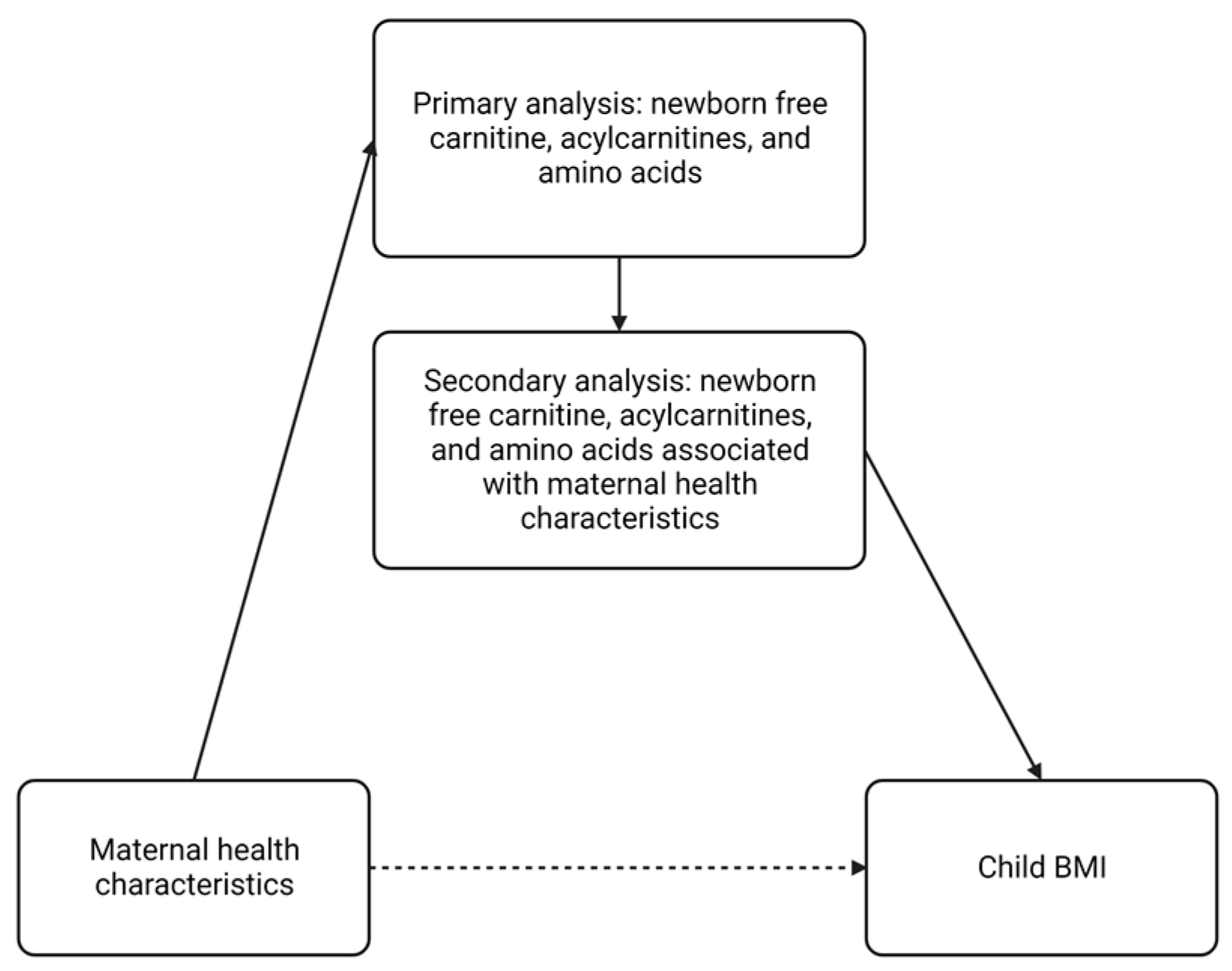
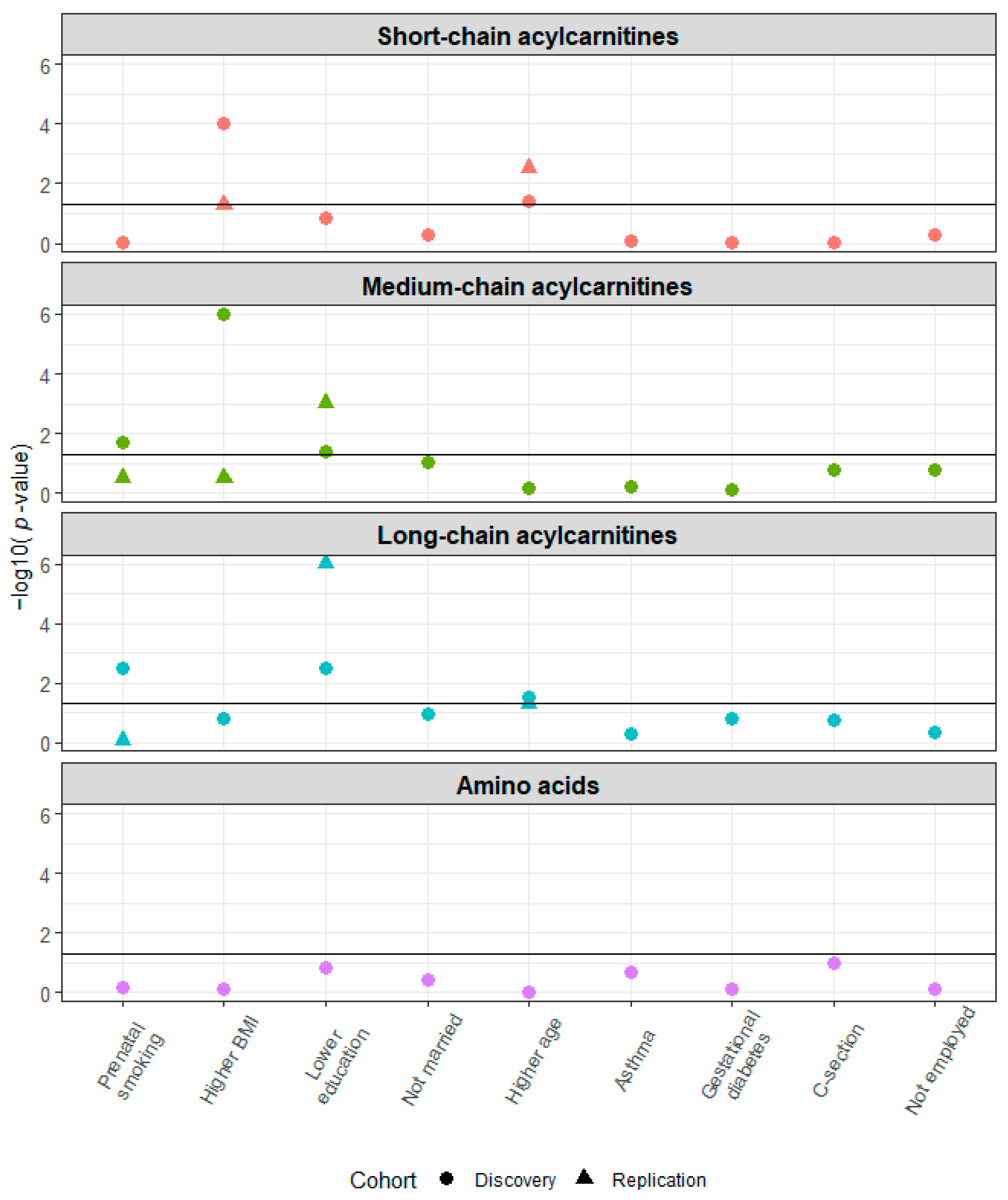
Several maternal health characteristics were associated with the
a priori grouping of NBS metabolites as short-, medium-, and long-chain acylcarnitine concentrations at birth in the discovery cohorts (
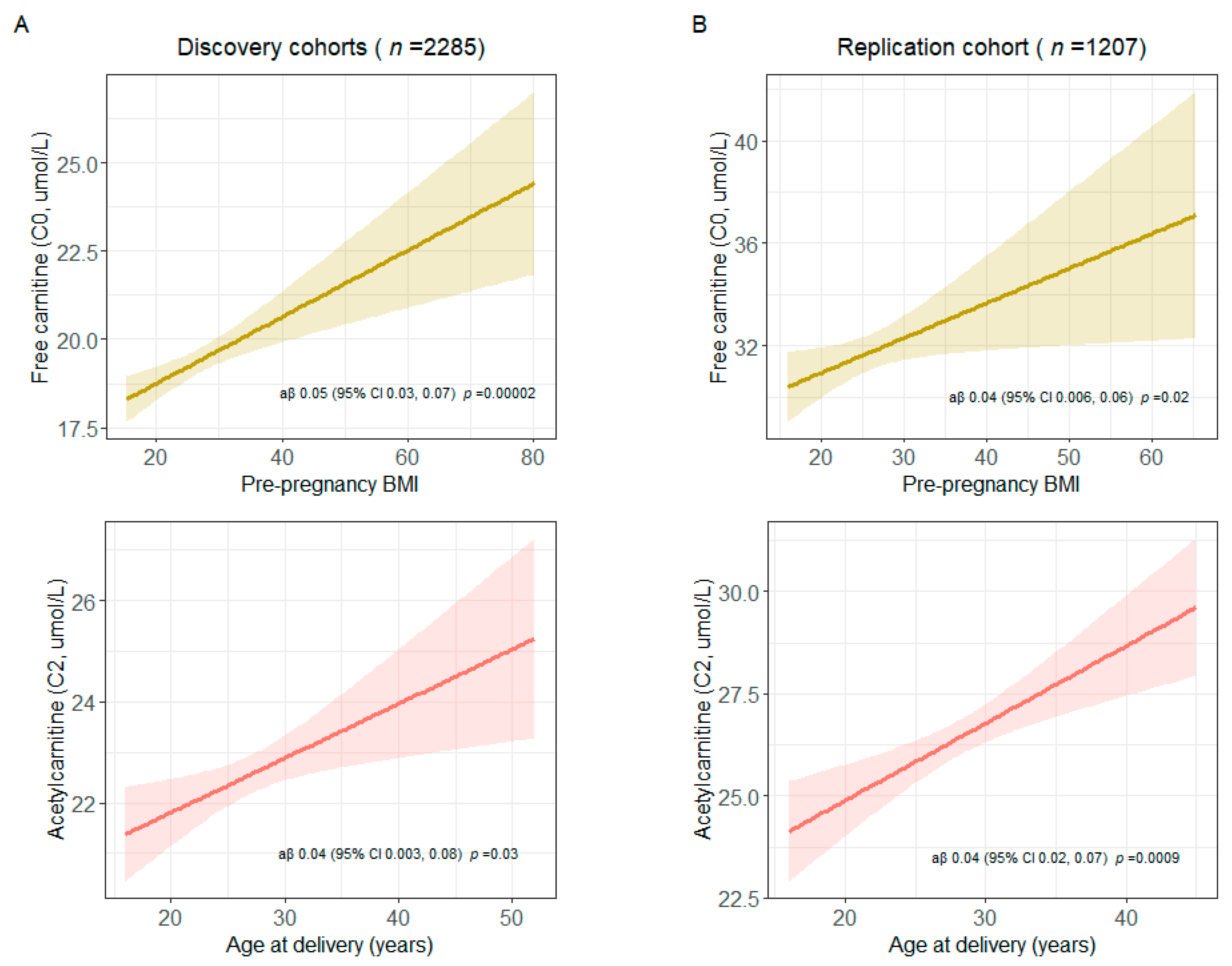
Figure 4). The associations of the following maternal health characteristics with NBS metabolite were also significant in the replication cohort: higher age at delivery and short-chain acylcarnitines; lower education and medium- and long-chain acylcarnitines. In analyses of the associations of maternal health characteristics and specific metabolites, we observed the following statistically significant associations in the discovery and replication cohorts: higher pre-pregnancy BMI and increased free carnitine (C0) concentration (discovery cohorts: aβ 0.05, 95% CI 0.03, 0.07; replication cohort: aβ 0.04, 95% CI 0.006, 0.06); higher age at delivery and increased acetylcarnitine (C2) concentration (discovery cohorts: aβ 0.04, 95% CI 0.003, 0.08; replication cohort: aβ 0.04, 95% CI 0.02, 0.07) (
Figure 5 and
Table S6). The results were unchanged after excluding women with potentially implausible pre-pregnancy BMIs > 50 (INSPIRE:
n = 15 [1%], MARCH:
n = 6 [2%], Healthy Start:
n = 6 [0%]) (
Figure S4).
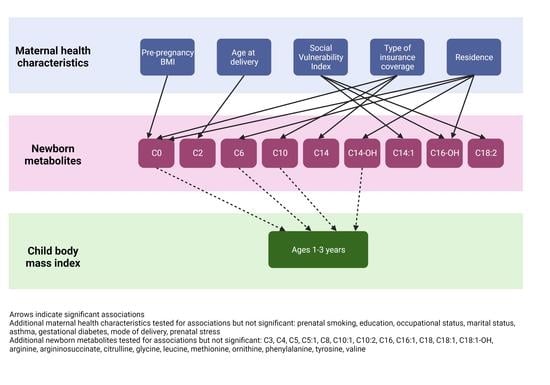
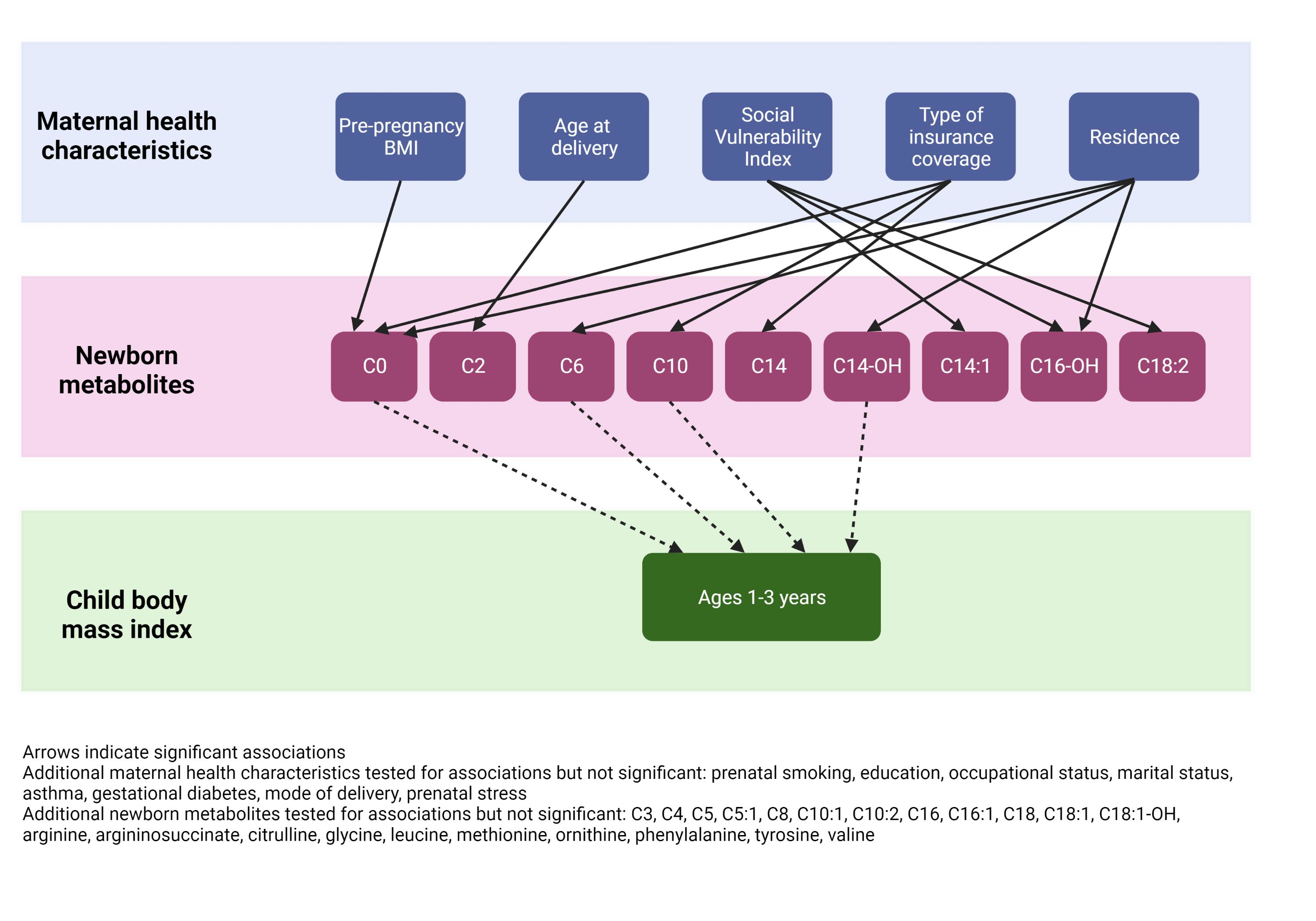
In secondary analysis restricted to INSPIRE participants (n = 1920), we assessed associations between additional maternal health characteristics and newborn metabolite concentrations. Most participants reported no prenatal stress exposure (61%), resided in an urban environment (76%), and were on government insurance (54%) (
Table S7). The mean SVI was 0.51 (SD 0.29). SVI was associated with long-chain acylcarnitine and amino acid concentrations; type of insurance coverage was associated with medium- and long-chain acylcarnitine concentrations; and residence was associated with medium-chain acylcarnitine concentrations (
Figure S5). Prenatal stress exposure was not associated with any of the newborn metabolite groups. In analyses of the associations of prenatal stress exposure, SVI, type of insurance coverage, and residence and specific metabolites, we observed the following statistically significant associations: SVI and tetradecenoylcarnitine (C14:1), 3-hydroxypalmitoylcarnitine (C16-OH), and linoleoylcarnitine (C18:2); government insurance (vs. private insurance) and decanoylcarnitine (C10) and tetradecanoylcarnitine (C14); other insurance (vs. private insurance) and C0; and urban residence and C0, hexanoylcarnitine (C6), 3-hydroxytetradecanoylcarnitine (C14-OH), and C16-OH (
Figure S6 and
Table S8). Additionally, significant associations of pre-pregnancy BMI and C0 and maternal age at delivery and C2 remained after additional adjustment for prenatal stress exposure, SVI, type of insurance coverage, and residence.
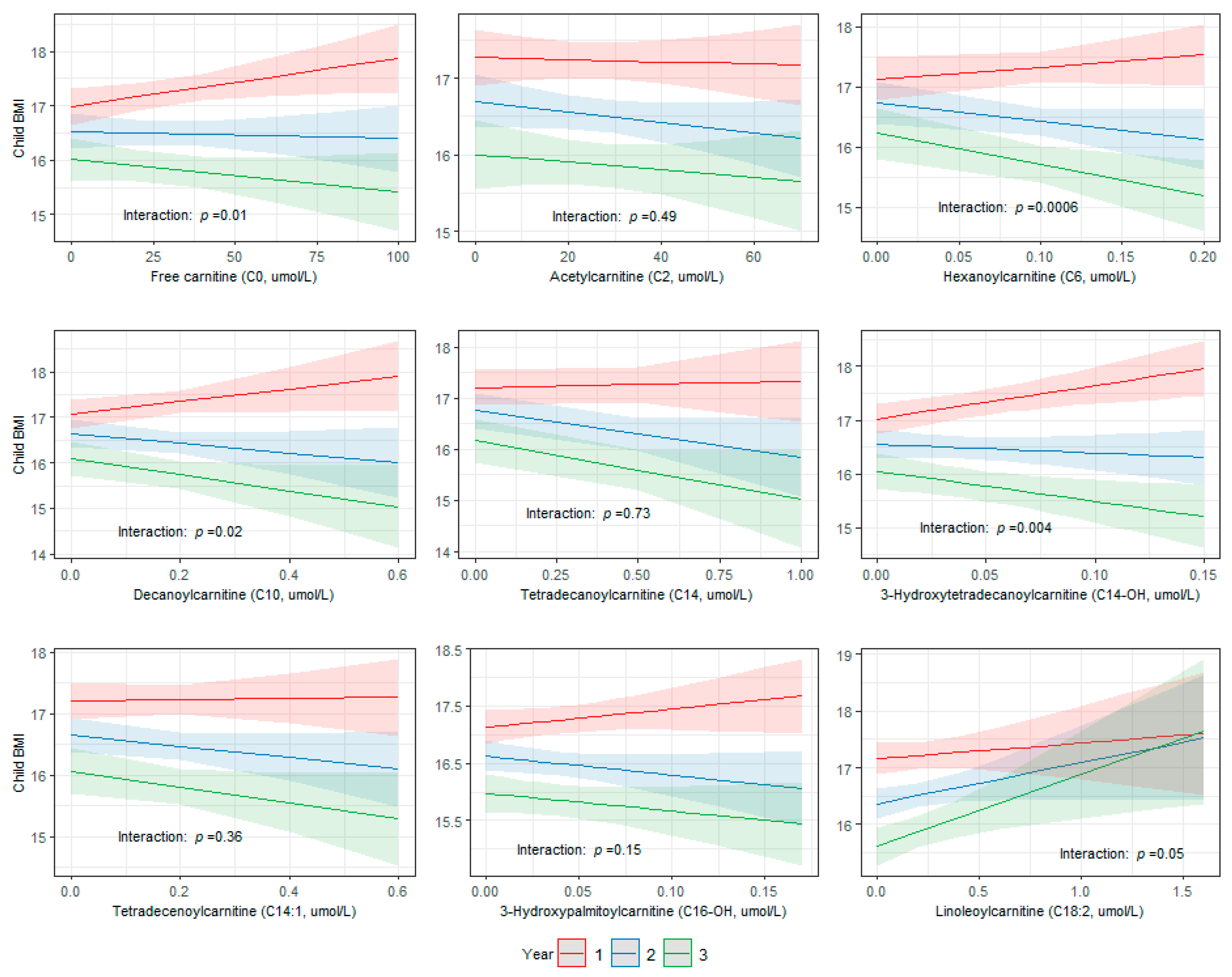
We then assessed the association between newborn metabolites that were significantly associated with maternal health characteristics in the primary and secondary analyses (C0, C2, C6, C10, C14, C14-OH, C14:1, C16-OH, and C18:2) and child BMI from ages 1–3 years in a pooled subset of INSPIRE and Healthy Start children with available weight and height measurements. Of the 2835 children in the pooled subset, 2122 (75%;
n = 1130 INSPIRE,
n = 992 Healthy Start), 2176 (77%;
n = 1161 INSPIRE,
n = 1015 Healthy Start), and 1272 (45%;
n = 398 INSPIRE,
n = 874 Healthy Start) children had weight and height measurements at ages 1, 2, and 3 years, respectively. The mean BMI was 17 (SD 2) at 1 year, 17 (SD 2) at 2 years, and 16 (2) at 3 years (
Figure S7). The associations between C0, C6, C10, and C14-OH and child BMI were modified over time (interaction:
p < 0.05) (
Figure 6). The strongest effects were present at year 1, and the associations waned over time.
4. Discussion
In this multi-cohort study, we identified maternal health characteristics associated with newborn metabolites. We identified and replicated relationships between higher pre-pregnancy BMI and increased C0 concentration at birth and higher age at delivery and increased C2 concentration at birth in discovery and replication cohorts. We also observed relationships between SVI, type of insurance coverage, and residence and C0 and medium- and long-chain acylcarnitine (C6, C10, C14, C14-OH, C14:1, C16-OH, and C18:2) concentrations at birth within a discovery cohort. Additionally, we showed that associations between metabolites associated with maternal health characteristics (C0, C6, C10, and C14-OH) and child BMI were modified from ages 1–3 years. These findings suggest that maternal health characteristics may impact fetal metabolic programming, as measured by NBS metabolites, potentially influencing later life child growth patterns. Future studies should perform formal mediation analyses to further explore the potential biologic pathways through which maternal health characteristics may impact child BMI.
Few studies have assessed associations between maternal complications of pregnancy and environmental stressors and newborn metabolite concentrations. McCarthy et al. showed significant associations between socioeconomic status—comprised of Medicaid coverage; Women, Infants, and Children (WIC) supplemental nutrition receipt; and having a high school education or less—and 41 of 42 targeted NBS (blood spot) metabolites in a California birth cohort [
21]. Lowe et al. found associations between increased second-trimester BMI and insulin resistance and increased cord blood concentrations of branched-chain amino acids and their metabolic byproducts [
22]. In a cohort of preterm infants, Ryckman et al. found associations between preeclampsia and increased concentrations of certain metabolites quantified from NBS panels (alanine, C0, C2, octenotylcarnitine [C8:1], and C18:2) [
23]. We have extended these findings by comprehensively demonstrating and replicating associations between maternal health characteristics and newborn metabolite concentrations and the association of these metabolites with childhood growth patterns. While previous studies have shown associations between newborn metabolites and childhood growth [
24], overweight [
24], and obesity [
25], this study provides additional insights on the maternal factors and potential in utero pathways underlying the relationship observed between newborn metabolism and subsequent child metabolic dysfunction.
We identified associations between several maternal health characteristics (pre-pregnancy BMI, age at delivery, SVI, type of insurance coverage, and residence) and concentrations of free carnitine (C0) and acylcarnitines (C2, C6, C10, C14, C14-OH, C14:1, C16-OH, and C18:2) at birth. C0 and its acylated derivatives (i.e., acylcarnitines), known as the carnitine pool, play a vital role in mitochondrial function and energy production [
9]. Humans oxidize extensive amounts of fats to guarantee continuous energy supply [
26]. C0 is essential for fatty acid oxidation as it is the primary shuttle for long-chain acylcarnitines from the cytosol into the mitochondrion [
26]. Acylcarnitines are formed from carnitine and acyl-CoAs in the mitochondria and are the transport form of fatty acids in the plasma [
27,
28]. External stressors have been shown to impact the carnitine pool. Decreased C0 levels are found in individuals with obesity and insulin resistance due to compromised mitochondrial function and fatty acid oxidation [
29]. The association that we observed in the present study between higher pre-pregnancy BMI and increased C0 concentration at birth may be due to a rebound effect, with increased C0 in the newborn due to diminished supply in utero. Increases in C2 are associated with stress/trauma [
30]. Increased maternal age at delivery is also associated with increased prenatal stress [
31,
32], anxiety [
31], and complications of delivery [
33], suggesting one possible explanation for the observed increased C2 in offspring of older women. Socioeconomic status and stress can impact food access [
34] and eating behaviors [
35,
36], which may lead to metabolite fluctuations [
37]. We observed relationships between SVI and type of insurance and concentrations of several metabolites at birth, which may additionally reflect food access, eating behaviors, and metabolism. Air pollutants contribute to mitochondrial dysfunction [
38], which may account for the relationships observed between urban residence and free carnitine and several acylcarnitines.
As the carnitine pool is tightly regulated, changes in plasma carnitine and acylcarnitine concentrations may contribute to metabolic dysfunction and disease [
9]. This is supported by our findings of associations between metabolite concentrations at birth and subsequent child growth patterns. We observed that some acylcarnitine concentrations at birth (C0, C6, C10, and C14-OH) were associated with maternal health characteristics and child BMI at ages 1–3 years. However, other acylcarnitines associated with maternal health characteristics (C2, C14, C14:1, C16-OH, and C18:2) were not associated with child BMI at ages 1–3 years. C2, C14, C14:1, C16-OH, and C18:2 may be associated with other important metabolic parameters in childhood, such as central adiposity, waist circumference, and triglyceride and fasting insulin levels, and these relationships should be assessed in future studies.
Our study has many important strengths, including our large sample sizes from diverse, longitudinal birth cohorts with rich phenotypic data and our replication of findings in an independent birth cohort. In addition, harmonization of NBS data across cohorts was possible because processing of NBS samples is regulated by the CDC’s Newborn Screening Quality Assurance Program and consensus guidelines on the use of MS/MS analysis in NBS developed by the Clinical and Laboratory Standards Institute ensure standardization across states [
14,
39]. Lastly, we employed a rigorous
a priori two-stage analytic plan to reduce multiple testing of a large NBS metabolite panel.
There are also some limitations of our study. We could only assess maternal health characteristics that were ascertained and harmonizable across cohorts. We assessed the association between additional maternal health characteristics (prenatal stress, SVI, residence, and type of insurance coverage) and newborn metabolite concentrations within the INSPIRE cohort but were unable to replicate these results due to lack of currently available information on these characteristics within MARCH and Healthy Start cohorts. While we were able to harmonize maternal health characteristics across the cohorts in this study, measurement error is possible due to the use of different means and timing of ascertainment of the maternal health characteristics across cohorts. We utilized maternal race and ethnicity as surrogate measures for infant race and ethnicity for participants in whom these data were unavailable. Although this is an imperfect measure, the concordances between maternal race and ethnicity and infant race and ethnicity were high, and use of this surrogate measure is unlikely to have impacted the results. Although NBS data were only available for 39% of MARCH participants enrolled in this birth cohort as obtaining participant consent for NBS metabolic data linkage is currently ongoing, we did not observe differences between MARCH participants with NBS data and all MARCH participants. This suggests that selection bias would not have impacted our results. We chose to only include child BMI measures from ages 1–3 years in the present study. Future studies should assess the association between newborn metabolites associated with maternal health characteristics and child BMI beyond age 3 years to further explore relationships with child growth patterns.
Author Contributions
Conceptualization, B.M.S. and T.V.H.; Data curation, B.M.S.; Formal analysis, B.M.S. and T.G.; Funding acquisition, B.M.S., T.V.H., D.M.D., N.S.P. and J.E.G.; Investigation, B.M.S., T.G. and T.V.H.; Methodology, B.M.S., T.G., T.V.H. and W.D.D.; Project Administration, B.M.S. and N.B.R.; Resources, T.V.H., D.M.D., N.S.P. and J.E.G.; Software, B.M.S. and T.G.; Supervision, T.G., P.W., W.D.D., K.K.R., R.C.F., C.T.M., D.M.D., N.S.P., S.V.L., J.E.G. and T.V.H.; Validation, B.M.S.; Visualization, B.M.S., T.G. and T.V.H.; Writing—Original Draft Preparation, B.M.S.; Writing—Review and Editing, B.M.S., T.G., N.B.R., P.W., W.D.D., K.K.R., R.C.F., C.T.M., D.M.D., N.S.P., S.V.L., J.E.G. and T.V.H. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the National Institutes of Health (grant numbers UG3/UH3 OD023282 to JEG, UH3 OD023282 and U19 AI095227 to TVH, UH3 OD023285 to NSP, UH3 OD023248 to DMD, UH3 OD023288 to CTM, and K01 HL161257 which supports BMS). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Research reported in this publication was supported by the Environmental Influences on Child Health Outcomes (ECHO) program, Office of the Director, National Institutes of Health, under Award Numbers U2COD023375 (Coordinating Center), U24OD023382 (Data Analysis Center), U24OD023319 (PRO Core), UH3OD023282 (Gern), UH3OD023282 and U19 AI095227 (Hartert), UH3OD023248 (Dabelea), and UH3OD023285 (Paneth).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Boards (IRBs) at Vanderbilt University Medical Center (IRB #201595, approved 10/22/2020)), Michigan State University (IRB #STUDY00005436, approved 4/14/2021), University of Colorado (IRB #20-2954, approved 12/22/2020), Tennessee Department of Health (IRB # 2020-0277, approved 3/31/2021), Michigan Department of Health and Human Services (IRB #202104-02-EA, approved 5/20/2021), and Colorado Department of Public Health and Environment (IRB #2021-004, approved 5/7/2021).
Informed Consent Statement
Written informed consent or parent’s/guardian’s permission was obtained, along with child assent as appropriate, for ECHO participation and for participation in specific cohorts.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to linkage to potentially identifying and sensitive patient information of participants in three National Institutes of Health (NIH) Environmental Influences on Child Health Outcomes (ECHO) Program birth cohorts. The dataset includes confidential newborn screening data that cannot be shared without individual approvals from the Tennessee Department of Health, Michigan Department of Health and Human Services, and Colorado Department of Public Health and Environment Institutional Review Boards. Access to confidential ECHO data requires written authorization from the ECHO study sponsor, the ECHO Program, and a data request submitted to the ECHO PI.
Acknowledgments
We are indebted to the following individuals for their assistance with data collection and study preparation: Yinmei Li (Tennessee Department of Health), Chris Dorley (Tennessee Department of Health), Greg Bonn (Colorado Department of Public Health & Environment), Abena Watson-Siriboe (Colorado Department of Public Health & Environment), Joni Koenig (Colorado Department of Public Health & Environment), Shelby Atkinson (Michigan Department of Health & Human Services), Carlotta Allievi-Nagel (Michigan Department of Health & Human Services), Zhouwen Liu (Vanderbilt University Medical Center), Cole Lacey (Vanderbilt University Medical Center), Sweta Singh (University of Wisconsin-Madison), Lisa Gress (University of Wisconsin-Madison), Mercedes Martinez (University of Colorado Anschutz Medical Campus), Traci Bekelman (University of Colorado Anschutz Medical Campus), Jenny Aalborg (University of Colorado Anschutz Medical Campus), Brandy Ringham (University of Colorado Anschutz Medical Campus), Julia Van Dyke (University of Colorado Anschutz Medical Campus), Anna Bellatorre (University of Colorado Anschutz Medical Campus), Allison McCawley (University of Colorado Anschutz Medical Campus), Lisa Testaverde (University of Colorado Anschutz Medical Campus), Christine Ahearn (University of Colorado Anschutz Medical Campus), Alexa Krueger (Michigan State University), Breanna Kornatowski (Michigan State University), Tengfei Ma (Michigan State University), Kelly Hirko (Michigan State University), and Tracy Thompson (Michigan State University). ECHO Collaborators Acknowledgment: The authors wish to thank our ECHO colleagues; the medical, nursing, and program staff; and the children and families participating in the ECHO cohorts. We also acknowledge the contribution of the following ECHO program collaborators: ECHO Components—Coordinating Center: Duke Clinical Research Institute, Durham, North Carolina: Smith PB, Newby KL; Data Analysis Center: Johns Hopkins University Bloomberg School of Public Health, Baltimore, Maryland: Jacobson LP; Research Triangle Institute, Durham, North Carolina: Catellier DJ; Person-Reported Outcomes Core: Northwestern University, Evanston, Illinois: Gershon R, Cella D. ECHO Awardees and Cohorts—University of Wisconsin, Madison, WI: Gern J; Vanderbilt University Medical Center, Nashville, TN: Hartert T; Michigan State University, East Lansing, MI: Paneth N; University of Colorado Anschutz Medical Campus, Aurora, CO: Dabelea D.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Marciniak, A.; Patro-Małysza, J.; Kimber-Trojnar, Ż.; Marciniak, B.; Oleszczuk, J.; Leszczyńska-Gorzelak, B. Fetal programming of the metabolic syndrome. Taiwan. J. Obstet. Gynecol. 2017, 56, 133–138. [Google Scholar] [CrossRef]
- Rinaudo, P.; Wang, E. Fetal programming and metabolic syndrome. Ann. Rev. Physiol. 2012, 74, 107–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, E.J.; Kim, Y.J. What is fetal programming?: A lifetime health is under the control of in utero health. Obstet. Gynecol. Sci. 2017, 60, 506–519. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, K.; Lillycrop, K.A.; Silver, M.J. Fetal programming and epigenetics. Curr. Opin. Endocr. Metab. Res. 2020, 13, 1–6. [Google Scholar] [CrossRef]
- Fiehn, O. Metabolomics—The link between genotypes and phenotypes. Plant Mol. Biol. 2002, 48, 155–171. [Google Scholar] [CrossRef] [PubMed]
- Gallois, A.; Mefford, J.; Ko, A.; Vaysse, A.; Julienne, H.; Ala-Korpela, M.; Laakso, M.; Zaitlen, N.; Pajukanta, P.; Aschard, H. A comprehensive study of metabolite genetics reveals strong pleiotropy and heterogeneity across time and context. Nat. Commun. 2019, 10, 4788. [Google Scholar] [CrossRef] [Green Version]
- de Nava, A.S.L.; Raja, A. Physiology, Metabolism. [Updated 2021 Sep 20]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK546690/ (accessed on 12 December 2022).
- Wishart, D.S.; Feunang, Y.D.; Marcu, A.; Guo, A.C.; Liang, K.; Vázquez-Fresno, R.; Sajed, T.; Johnson, D.; Li, C.; Karu, N.; et al. HMDB 4.0: The human metabolome database for 2018. Nucleic Acids Res. 2018, 46, D608–D617. [Google Scholar] [CrossRef]
- McCann, M.R.; George De la Rosa, M.V.; Rosania, G.R.; Stringer, K.A. L-Carnitine and Acylcarnitines: Mitochondrial Biomarkers for Precision Medicine. Metabolites 2021, 11, 51. [Google Scholar] [CrossRef]
- Bröer, S.; Bröer, A. Amino acid homeostasis and signalling in mammalian cells and organisms. Biochem. J. 2017, 474, 1935–1963. [Google Scholar] [CrossRef] [Green Version]
- Larkin, E.K.; Gebretsadik, T.; Moore, M.L.; Anderson, L.J.; Dupont, W.D.; Chappell, J.D.; Minton, P.A.; Peebles, R.S., Jr.; Moore, P.E.; Valet, R.S.; et al. Objectives, design and enrollment results from the Infant Susceptibility to Pulmonary Infections and Asthma Following RSV Exposure Study (INSPIRE). BMC Pulm. Med. 2015, 15, 45. [Google Scholar] [CrossRef] [Green Version]
- Sauder, K.A.; Stamatoiu, A.V.; Leshchinskaya, E.; Ringham, B.M.; Glueck, D.H.; Dabelea, D. Cord Blood Vitamin D Levels and Early Childhood Blood Pressure: The Healthy Start Study. J. Am. Heart Assoc. 2019, 8, e011485. [Google Scholar] [CrossRef] [Green Version]
- National Institutes of Health: Newborn Screening. Available online: https://www.nichd.nih.gov/health/topics/newborn (accessed on 10 June 2022).
- CLSI. Newborn Screening by Tandem Mass Spectrometry, 2nd ed.; CLSI Guideline NBS04; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2017. [Google Scholar]
- Feuchtbaum, L.; Carter, J.; Dowray, S.; Currier, R.J.; Lorey, F. Birth prevalence of disorders detectable through newborn screening by race/ethnicity. Genet. Med. 2012, 14, 937–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Onis, M.; Onyango, A.; Borghi, E.; Siyam, A.; Blössner, M.; Lutter, C. Worldwide implementation of the WHO Child Growth Standards. Public Health Nutr. 2012, 15, 1603–1610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flegal, K.M.; Cole, T.J. Construction of LMS parameters for the Centers for Disease Control and Prevention 2000 growth charts. In National Health Statistics Reports; National Center for Health Statistics: Hyattsville, MA, USA, 2013; pp. 1–3. [Google Scholar]
- UpToDate: Measurement of Growth in Children. Available online: https://www.uptodate.com/contents/measurement-of-growth-in-children?search=calculator-cdc-nchs-infant-weight-for-length-percentiles-less-than§ionRank=2&usage_type=default&anchor=H3361608930&source=machineLearning&selectedTitle=1~150&display_rank=1#H3361608930 (accessed on 11 November 2022).
- van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef] [Green Version]
- Dambrova, M.; Makrecka-Kuka, M.; Kuka, J.; Vilskersts, R.; Nordberg, D.; Attwood, M.M.; Smesny, S.; Sen, Z.D.; Guo, A.C.; Oler, E.; et al. Acylcarnitines: Nomenclature, Biomarkers, Therapeutic Potential, Drug Targets, and Clinical Trials. Pharmacol. Rev. 2022, 74, 506–551. [Google Scholar] [CrossRef]
- McCarthy, M.E.; Oltman, S.P.; Rogers, E.E.; Ryckman, K.; Jelliffe-Pawlowski, L.L.; Danilack, V.A. The independent and combined influences of small for gestational age and socioeconomic status on newborn metabolite levels. J. Matern Fetal. Neonatal. Med. 2022, 35, 6192–6198. [Google Scholar] [CrossRef]
- Lowe, W.L., Jr.; Bain, J.R.; Nodzenski, M.; Reisetter, A.C.; Muehlbauer, M.J.; Stevens, R.D.; Ilkayeva, O.R.; Lowe, L.P.; Metzger, B.E.; Newgard, C.B.; et al. Maternal BMI and Glycemia Impact the Fetal Metabolome. Diabetes Care 2017, 40, 902–910. [Google Scholar] [CrossRef] [Green Version]
- Ryckman, K.K.; Shchelochkov, O.A.; Cook, D.E.; Berberich, S.L.; Copeland, S.; Dagle, J.M.; Murray, J.C. The influence of maternal disease on metabolites measured as part of newborn screening. J. Matern. Fetal. Neonatal. Med. 2013, 26, 1380–1383. [Google Scholar] [CrossRef] [Green Version]
- Handakas, E.; Keski-Rahkonen, P.; Chatzi, L.; Alfano, R.; Roumeliotaki, T.; Plusquin, M.; Maitre, L.; Richiardi, L.; Brescianini, S.; Scalbert, A.; et al. Cord blood metabolic signatures predictive of childhood overweight and rapid growth. Int. J. Obes. 2021, 45, 2252–2260. [Google Scholar] [CrossRef]
- Cao, T.; Zhao, J.; Hong, X.; Wang, G.; Hu, F.B.; Wang, X.; Liang, L. Cord Blood Metabolome and BMI Trajectory from Birth to Adolescence: A Prospective Birth Cohort Study on Early Life Biomarkers of Persistent Obesity. Metabolites 2021, 11, 739. [Google Scholar] [CrossRef]
- Schooneman, M.G.; Vaz, F.M.; Houten, S.M.; Soeters, M.R. Acylcarnitines: Reflecting or inflicting insulin resistance? Diabetes 2013, 62, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makrecka-Kuka, M.; Sevostjanovs, E.; Vilks, K.; Volska, K.; Antone, U.; Kuka, J.; Makarova, E.; Pugovics, O.; Dambrova, M.; Liepinsh, E. Plasma acylcarnitine concentrations reflect the acylcarnitine profile in cardiac tissues. Sci. Rep. 2017, 7, 17528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giesbertz, P.; Ecker, J.; Haag, A.; Spanier, B.; Daniel, H. An LC-MS/MS method to quantify acylcarnitine species including isomeric and odd-numbered forms in plasma and tissues. J. Lipid Res. 2015, 56, 2029–2039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schooneman, M.G.; Houtkooper, R.H.; Hollak, C.E.M.; Wanders, R.J.A.; Vaz, F.M.; Soeters, M.R.; Houten, S.M. The impact of altered carnitine availability on acylcarnitine metabolism, energy expenditure and glucose tolerance in diet-induced obese mice. Biochim. Biophys. Acta 2016, 1862, 1375–1382. [Google Scholar] [CrossRef]
- L-Acetylcarnitine (HMDB0000201). Available online: https://hmdb.ca/metabolites/HMDB0000201 (accessed on 27 July 2022).
- Bayrampour, H.; Heaman, M.; Duncan, K.A.; Tough, S. Advanced maternal age and risk perception: A qualitative study. BMC Pregnancy Childbirth 2012, 12, 100. [Google Scholar] [CrossRef] [Green Version]
- García-Blanco, A.; Monferrer, A.; Grimaldos, J.; Hervás, D.; Balanzá-Martínez, V.; Diago, V.; Vento, M.; Cháfer-Pericás, C. A preliminary study to assess the impact of maternal age on stress-related variables in healthy nulliparous women. Psychoneuroendocrinology 2017, 78, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Levenson, D.; Romero, R.; Garcia-Flores, V.; Miller, D.; Xu, Y.; Sahi, A.; Hassan, S.S.; Gomez-Lopez, N. The effects of advanced maternal age on T-cell subsets at the maternal-fetal interface prior to term labor and in the offspring: A mouse study. Clin. Exp. Immunol. 2020, 201, 58–75. [Google Scholar] [CrossRef] [PubMed]
- Costa, B.V.L.; Menezes, M.C.; Oliveira, C.D.L.; Mingoti, S.A.; Jaime, P.C.; Caiaffa, W.T.; Lopes, A.C.S. Does access to healthy food vary according to socioeconomic status and to food store type? an ecologic study. BMC Public Health 2019, 19, 775. [Google Scholar] [CrossRef]
- Williamson, V.G.; Dilip, A.; Dillard, J.R.; Morgan-Daniel, J.; Lee, A.M.; Cardel, M.I. The Influence of Socioeconomic Status on Snacking and Weight among Adolescents: A Scoping Review. Nutrients 2020, 12, 167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yau, Y.H.; Potenza, M.N. Stress and eating behaviors. Minerva Endocrinol. 2013, 38, 255–267. [Google Scholar]
- Flanagan, J.L.; Simmons, P.A.; Vehige, J.; Willcox, M.D.P.; Garrett, Q. Role of carnitine in disease. Nutr. Metab. 2010, 7, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reddam, A.; McLarnan, S.; Kupsco, A. Environmental Chemical Exposures and Mitochondrial Dysfunction: A Review of Recent Literature. Curr. Environ. Health Rep. 2022, 9, 631–649. [Google Scholar] [CrossRef] [PubMed]
- De Jesús, V.R.; Mei, J.V.; Cordovado, S.K.; Cuthbert, C.D. The Newborn Screening Quality Assurance Program at the Centers for Disease Control and Prevention: Thirty-five Year Experience Assuring Newborn Screening Laboratory Quality. Int. J. Neonatal. Screen 2015, 1, 13–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}