
A Successful Bisphosphonates Monotherapy in Spinal Form of Paediatric Chronic Recurrent Multifocal Osteomyelitis (CRMO)—Case Report
 ,
,  ,
,
Abstract
:1. Introduction
2. Case Report
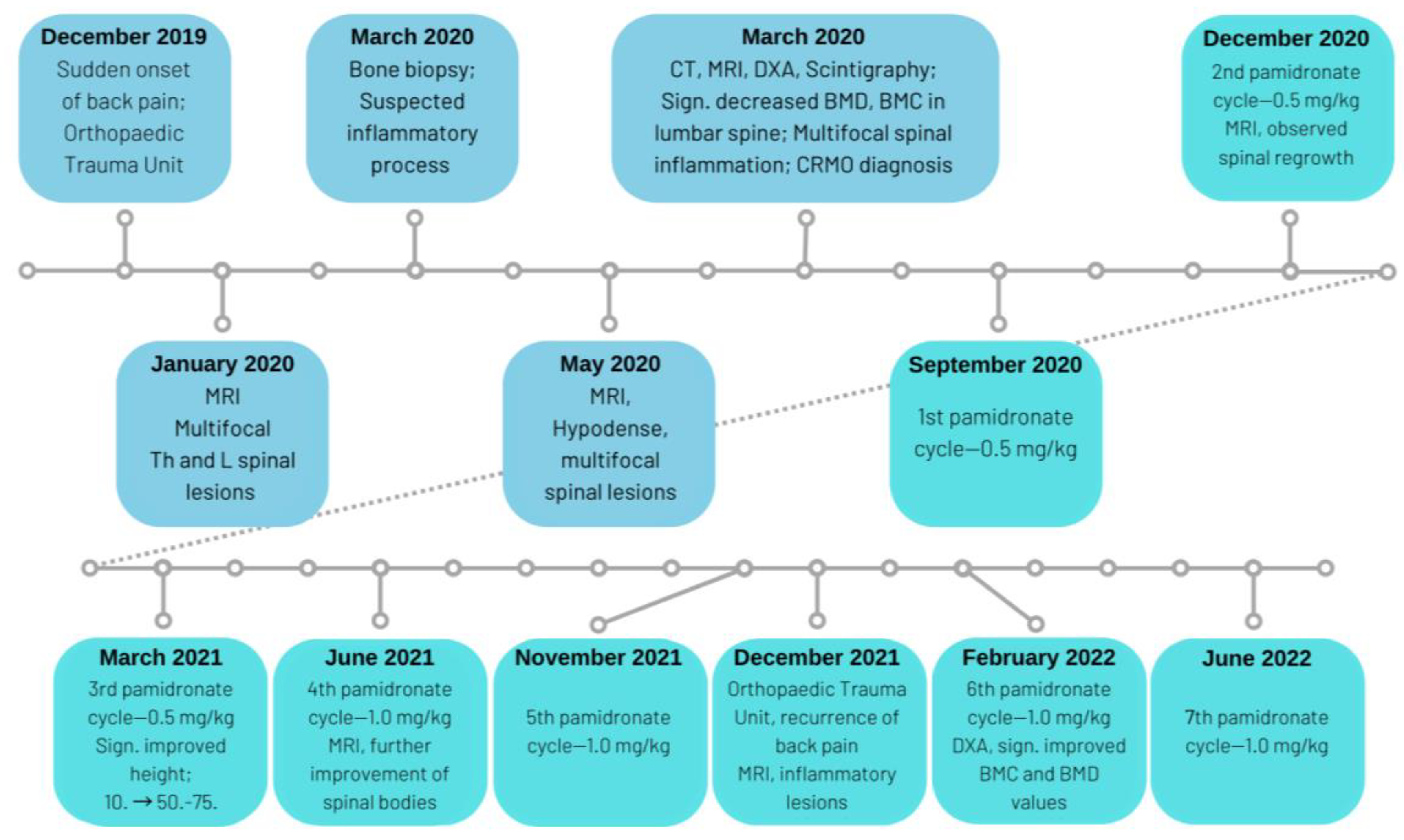
2.1. Patient Information
2.2. Clinical Findings
2.3. Diagnostic Assessment
2.4. Therapeutic Intervention
2.5. Follow-Up and Outcomes
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hofmann, S.R.; Kapplusch, F.; Girschick, H.J.; Morbach, H.; Pablik, J.; Ferguson, P.J.; Hedrich, C.M. Chronic Recurrent Multifocal Osteomyelitis (CRMO): Presentation, Pathogenesis, and Treatment. Curr. Osteoporos. Rep. 2017, 15, 542–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taddio, A.; Zennaro, F.; Pastore, S.; Cimaz, R. An Update on the Pathogenesis and Treatment of Chronic Recurrent Multifocal Osteomyelitis in Children. Pediatr. Drugs 2017, 19, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Cheng, L.; Feng, G. Bone Inflammation and Chronic Recurrent Multifocal Osteomyelitis. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 1380–1386. [Google Scholar] [PubMed]
- Zhao, Y.; Ferguson, P.J. Chronic Nonbacterial Osteomyelitis and Chronic Recurrent Multifocal Osteomyelitis in Children. Pediatr. Clin. N. Am. 2018, 65, 783–800. [Google Scholar] [CrossRef]
- Shah, A.; Rosenkranz, M.; Thapa, M. Review of Spinal Involvement in Chronic Recurrent Multifocal Osteomyelitis (CRMO): What Radiologists Need to Know about CRMO and Its Imitators. Clin. Imaging 2022, 81, 122–135. [Google Scholar] [CrossRef]
- Pigrau-Serrallach, C.; Rodríguez-Pardo, D. Bone and Joint Tuberculosis. Eur. Spine J. 2013, 22, 556–566. [Google Scholar] [CrossRef]
- Van den Brande, R.; MJ Cornips, E.; Peeters, M.; Ost, P.; Billiet, C.; van de Kelft, E. Epidemiology of Spinal Metastases, Metastatic Epidural Spinal Cord Compression and Pathologic Vertebral Compression Fractures in Patients with Solid Tumors: A Systematic Review. J. Bone Oncol. 2022, 35, 100446. [Google Scholar] [CrossRef]
- Moreno-Mateo, F.; Perea, S.H.; Onel, K.B. Chronic Recurrent Multifocal Osteomyelitis: Diagnosis and Treatment. Curr. Opin. Pediatr. 2021, 33, 90–96. [Google Scholar] [CrossRef]
- Zhao, M.; Wu, D.; Yu, K.; Shen, M. Clinical and Genetic Features of Chinese Adult Patients with Chronic Non-Bacterial Osteomyelitis: A Single Center Report. Front. Immunol. 2022, 13, 860646. [Google Scholar] [CrossRef]
- Kieninger, A.; Schäfer, J.F.; Tsiflikas, I.; Moll, M.; Kümmerle-Deschner, J.; Kraus, M.S.; Esser, M. Early Diagnosis and Response Assessment in Chronic Recurrent Multifocal Osteomyelitis: Changes in Lesion Volume and Signal Intensity Assessed by Whole-Body MRI. Br. J. Radiol. 2022, 95, 20211091. [Google Scholar] [CrossRef]
- Okay, E.; Ulu, K.; Demir, F.; Sari, T.; Zeynalov, S.; Toksoz Yildirim, A.N.; Baysal, B.; Zenginkinet, T.; Reddy, K.; Akpinar, F.; et al. Chronic Recurrent Multifocal Osteomyelitis: A Multidisciplinary Experience of 22 Pediatric Cases with a Mean Follow-up of 27 Months. J. Orthop. Sci. 2021; in press. [Google Scholar] [CrossRef] [PubMed]
- Ferjani, H.L.; Makhlouf, Y.; Maatallah, K.; Triki, W.; Nessib, D.B.; Kaffel, D.; Hamdi, W. Management of Chronic Recurrent Multifocal Osteomyelitis: Review and Update on the Treatment Protocol. Expert Opin. Biol. Ther. 2022, 22, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Sułko, J.; Ebisz, M.; Bień, S.; Błażkiewicz, M.; Jurczyk, M.; Namyślak, M. Treatment of Chronic Recurrent Multifocal Osteomyelitis with Bisphosphonates in Children. Jt. Bone Spine 2019, 86, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Gagnier, J.J.; Kienle, G.; Altman, D.G.; Moher, D.; Sox, H.; Riley, D.; Allaire, A.; Aronson, J.; Carpenter, J.; Gagnier, J.; et al. The CARE Guidelines: Consensus-Based Clinical Case Reporting Guideline Development. Headache 2013, 53, 1541–1547. [Google Scholar] [CrossRef] [Green Version]
- Riley, D.S.; Barber, M.S.; Kienle, G.S.; Aronson, J.K.; von Schoen-Angerer, T.; Tugwell, P.; Kiene, H.; Helfand, M.; Altman, D.G.; Sox, H.; et al. CARE Guidelines for Case Reports: Explanation and Elaboration Document. J. Clin. Epidemiol. 2017, 89, 218–235. [Google Scholar] [CrossRef]
- Hospach, T.; Langendoerfer, M.; von Kalle, T.; Maier, J.; Dannecker, G.E. Spinal Involvement in Chronic Recurrent Multifocal Osteomyelitis (CRMO) in Childhood and Effect of Pamidronate. Eur. J. Pediatr. 2010, 169, 1105–1111. [Google Scholar] [CrossRef]
- Sağ, E.; Sönmez, H.E.; Demir, S.; Bilginer, Y.; Ergen, F.B.; Aydıngöz, Ü.; Özen, S. Chronic Recurrent Multifocal Osteomyelitis in Children: A Single Center Experience over Five Years. Turk. J. Pediatr. 2019, 61, 386–391. [Google Scholar] [CrossRef]
- Alshammari, A.; Usmani, S.; Elgazzar, A.; Ashkanani, R. Chronic Recurrent Multifocal Osteomyelitis in Children: A Multidisciplinary Approach Is Needed to Establish a Diagnosis. World J. Nucl. Med. 2013, 12, 120–123. [Google Scholar] [CrossRef]
- Schaal, M.C.; Gendler, L.; Ammann, B.; Eberhardt, N.; Janda, A.; Morbach, H.; Darge, K.; Girschick, H.; Beer, M. Imaging in Non-Bacterial Osteomyelitis in Children and Adolescents: Diagnosis, Differential Diagnosis and Follow-up—An Educational Review Based on a Literature Survey and Own Clinical Experiences. Insights Imaging 2021, 12, 113. [Google Scholar] [CrossRef]
- Beck, N.A.; Nuzzi, L.C.; Parry, G.J.; Padwa, B.L. Assessing Knowledge and Promoting Awareness of Chronic Recurrent Multifocal Osteomyelitis Among Oral and Maxillofacial Surgeons. J. Oral Maxillofac. Surg. 2021, 79, 1689–1693. [Google Scholar] [CrossRef]
- Chang, E.; Vickery, J.; Zaiat, N.; Sallam, E.; Hanan, A.; Baker, S.; Alhamar, M.; Poulik, J.; Demian, E.; Shehata, B.M. Chronic Recurrent Multifocal Osteomyelitis (CRMO): A Study of 12 Cases from One Institution and Literature Review. Fetal Pediatr. Pathol. 2021, 41, 759–770. [Google Scholar] [CrossRef]
- Huang, K.; Lin, B.; Liu, Y.; Guo, Q.; Ren, H. Genomic Expression Profiling and Bioinformatics Analysis of Chronic Recurrent Multifocal Osteomyelitis. BioMed Res. Int. 2021, 2021, 6898093. [Google Scholar] [CrossRef] [PubMed]
- Andronikou, S.; Kraft, J.K.; Offiah, A.C.; Jones, J.; Douis, H.; Thyagarajan, M.; Barrera, C.A.; Zouvani, A.; Ramanan, A.V. Whole-Body MRI in the Diagnosis of Paediatric CNO/CRMO. Rheumatology 2020, 59, 2671–2680. [Google Scholar] [CrossRef] [PubMed]
- Dailey, T.A.; Berven, M.D.; Vroman, P.J. 99mTc-HMPAO-Labeled WBC Scan for the Diagnosis of Chronic Recurrent Multifocal Osteomyelitis. J. Nucl. Med. Technol. 2014, 42, 299–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, L.; Liu, H.; Tang, H.; Zhang, Z.; Zou, L.; Yu, H.; Sun, L.; Li, X.; Tang, X.; Lu, M. Clinical Characteristics and Outcomes of Chronic Nonbacterial Osteomyelitis in Children: A Multicenter Case Series. Pediatr. Rheumatol. 2022, 20, 1. [Google Scholar] [CrossRef] [PubMed]
- Schnabel, A.; Nashawi, M.; Anderson, C.; Felsenstein, S.; Lamoudi, M.; Poole-Cowley, J.; Lindell, E.; Oates, B.; Fowlie, P.; Walsh, J.; et al. TNF-Inhibitors or Bisphosphonates in Chronic Nonbacterial Osteomyelitis?—Results of an International Retrospective Multicenter Study. Clin. Immunol. 2022, 238, 109018. [Google Scholar] [CrossRef] [PubMed]
- Rogers, M.J.; Mönkkönen, J.; Munoz, M.A. Molecular Mechanisms of Action of Bisphosphonates and New Insights into Their Effects Outside the Skeleton. Bone 2020, 139, 115493. [Google Scholar] [CrossRef]
- Gleeson, H.; Wiltshire, E.; Briody, J.; Hall, J.; Chaitow, J.; Sillence, D.; Cowell, C.; Munns, C. Childhood Chronic Recurrent Multifocal Osteomyelitis: Pamidronate Therapy Decreases Pain and Improves Vertebral Shape. J. Rheumatol. 2008, 35, 707–712. [Google Scholar]
- Gaal, A.; Basiaga, M.L.; Zhao, Y.; Egbert, M. Pediatric Chronic Nonbacterial Osteomyelitis of the Mandible: Seattle Children’s Hospital 22-Patient Experience. Pediatr. Rheumatol. 2020, 18, 4. [Google Scholar] [CrossRef]
- Karunaratne, Y.G.; Davies, J.; Carty, C.P.; Graham, D. Chronic Recurrent Multifocal Osteomyelitis of the Hand: A Rare Pediatric Condition. Hand 2021, 16, 213–222. [Google Scholar] [CrossRef]
- Malek, A.; Aelami, M.; Afzali, N.; Parsa, A.; Jalalinia, H. Chronic Recurrent Multifocal Osteomyelitis in a 9-Year-Old Boy. Arch. Bone Jt. Surg. 2017, 5, 196–200. [Google Scholar] [PubMed]
- Kostik, M.M.; Kopchak, O.L.; Maletin, A.S.; Mushkin, A.Y. The Peculiarities and Treatment Outcomes of the Spinal Form of Chronic Non-Bacterial Osteomyelitis in Children: A Retrospective Cohort Study. Rheumatol. Int. 2020, 40, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Concha, S.; Hernández-Ojeda, A.; Contreras, O.; Mendez, C.; Talesnik, E.; Borzutzky, A. Chronic Nonbacterial Osteomyelitis in Children: A Multicenter Case Series. Rheumatol. Int. 2020, 40, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, C.M.; Jurik, A.G.; Glerup, M.B.; Høst, C.; Mahler, B.T.; Hauge, E.M.; Herlin, T. Response to Early-Onset Pamidronate Treatment in Chronic Nonbacterial Osteomyelitis: A Retrospective Single-Center Study. J. Rheumatol. 2019, 46, 1515–1523. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Wu, E.Y.; Oliver, M.S.; Cooper, A.M.; Basiaga, M.L.; Vora, S.S.; Lee, T.C.; Fox, E.; Amarilyo, G.; Stern, S.M.; et al. Consensus Treatment Plans for Chronic Nonbacterial Osteomyelitis Refractory to Nonsteroidal Antiinflammatory Drugs and/or With Active Spinal Lesions. Arthritis Care Res. 2018, 70, 1228–1237. [Google Scholar] [CrossRef] [PubMed]
- Kaut, S.; van den Wyngaert, I.; Christiaens, D.; Wouters, C.; Noppe, N.; Herregods, N.; Dehoorne, J.; de Somer, L. Chronic Nonbacterial Osteomyelitis in Children: A Multicentre Belgian Cohort of 30 Children. Pediatr. Rheumatol. 2022, 20, 41. [Google Scholar] [CrossRef]
- Yousaf, A.; Muhammad, S.; Zoghoul, S.B.M.; Alam, S.I.; Elsyaed, A.M. Chronic Recurrent Multifocal Osteomyelitis and Its Management. Cureus 2021, 13, e18872. [Google Scholar] [CrossRef]
- O’Leary, D.; Wilson, A.G.; MacDermott, E.J.; Lowry, C.; Killeen, O.G. Variability in Phenotype and Response to Treatment in Chronic Nonbacterial Osteomyelitis; the Irish Experience of a National Cohort. Pediatr. Rheumatol. 2021, 19, 45. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ROI | BMD (g/cm2) | BMC (g) | Surface (cm2) | Z-Score |
|---|---|---|---|---|
| L1 | 0.317 | 1.83 | 5.76 | −3.2 (−39%) |
| L2 | 0.355 | 2.81 | 7.91 | −3.0 (−37%) |
| L3 | 0.351 | 2.29 | 6.53 | −3.1 (−37%) |
| L4 | 0.404 | 2.93 | 7.25 | −2.2 (−27%) |
| TBLH | 0.359 | 9.86 | 27.46 | −2.9 (−35%) |
| Date of Hospitalization (Cycle) | Weight in kg (Centile) | Height in cm (Centile) | Dose of Pamidronate (mg/kg) | Total Body bone Density z-Score |
|---|---|---|---|---|
| 13 July 2020 (pre-treatment) | 38.0 (75.-90.) | 129.0 (10.) | - | −2.9 |
| 18–20 September 2020 (1st cycle) | - | - | 0.5 | - |
| 18–20 December 2020 (2nd cycle) | 35.7 (50.-75.) | 137.1 (25.-50.) | 0.5 | - |
| 19–21 March 2021 (3rd cycle) | 36.3 (50.-75.) | 142.0 (50.-75.) | 0.5 | - |
| 25–27 June 2021 (4th cycle) | - | - | 1.0 | - |
| 19–21 November 2021 (5th cycle) | 39.9 (50.-75.) | 147.0 (50.-75.) | 1.0 | - |
| 11–13 February 2022 (6th cycle) | 42.3 (50.-75.) | 148.0 (50.-75.) | 1.0 | 1.2 |
| 13–15 June 2022 (7th cycle) | 46.1 (75.) | 150.0 (50.) | 1.0 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Opala, A.; Hofman, J.; Hutny, M.; Wylazlowska, A.; Matusik, P. A Successful Bisphosphonates Monotherapy in Spinal Form of Paediatric Chronic Recurrent Multifocal Osteomyelitis (CRMO)—Case Report. Metabolites 2023, 13, 344. https://doi.org/10.3390/metabo13030344
Opala A, Hofman J, Hutny M, Wylazlowska A, Matusik P. A Successful Bisphosphonates Monotherapy in Spinal Form of Paediatric Chronic Recurrent Multifocal Osteomyelitis (CRMO)—Case Report. Metabolites. 2023; 13(3):344. https://doi.org/10.3390/metabo13030344
Chicago/Turabian StyleOpala, Aleksandra, Jagoda Hofman, Michał Hutny, Aleksandra Wylazlowska, and Paweł Matusik. 2023. "A Successful Bisphosphonates Monotherapy in Spinal Form of Paediatric Chronic Recurrent Multifocal Osteomyelitis (CRMO)—Case Report" Metabolites 13, no. 3: 344. https://doi.org/10.3390/metabo13030344