
Analysis of Volatile Organic Compounds in Exhaled Breath Following a COMEX-30 Treatment Table

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation and Hyperbaric Exposure
2.2. Collection and GC-MS Analysis of Breath Samples
2.3. Statistical Analysis and Identification of Compounds
3. Results
3.1. Symptoms Experienced after Hyperbaric Exposure
3.2. Identified Compounds
4. Discussion
4.1. Identified Compounds
4.2. Strength and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
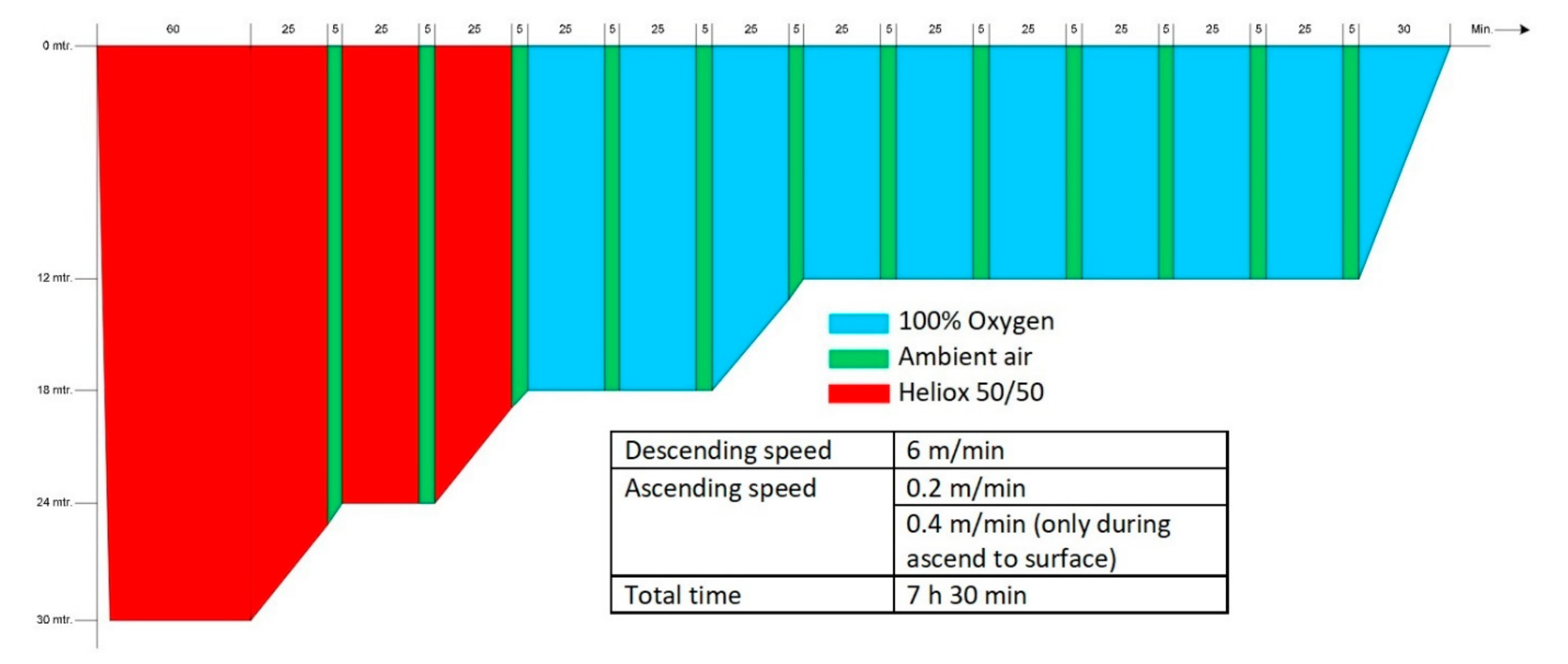
Appendix A. COMEX-30 Hyperbaric Treatment Table

Appendix B. VOCs Varying Significantly over Time




Appendix C. Nonsignificantly Varying VOCs





Appendix D. VOCs Not Varying Significantly over Time in Subjects with Symptoms of POT


References
- Brubakk, A.; Neuman, T. Bennett and Elliott’s Physiology and Medicine of Diving, 5th ed.; Saunders Publishing: Philadelphia, PA, USA; Elsevier: Amsterdam, The Netherlands, 2003; ISBN 978-0702025716. [Google Scholar]
- Mitchell, S.J.; Bennett, M.H.; Moon, R.E. Decompression Sickness and Arterial Gas Embolism. N. Engl. J. Med. 2022, 386, 1254–1264. [Google Scholar] [CrossRef] [PubMed]
- Robinson, T.; Evangelista, J.S.; Latham, E.; Mukherjee, S.T.; Pilmanis, A. Recurrence of Neurological Deficits in an F/A-18D Pilot Following Loss of Cabin Pressure at Altitude. Aerosp. Med. Hum. Perform. 2016, 87, 740–744. [Google Scholar] [CrossRef] [PubMed]
- Andersen, H.L. Decompression sickness during construction of the Great Belt Tunnel, Denmark. Undersea Hyperb. Med. 2002, 29, 172–188. [Google Scholar] [PubMed]
- Moon, R.; Mitchell, S. Hyperbaric Treatment for Decompression Sickness: Current Recommendations. Undersea Hyperb. Med. 2019, 46, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, S.J.; Bennett, M.H.; Bryson, P.; Butler, F.K.; Doolette, D.J.; Holm, J.R.; Kot, J.; Lafère, P. Pre hospital management of decompression illness: Expert review of key principles and controversies. Diving Hyperb. Med. J. 2018, 48, 45–55. [Google Scholar] [CrossRef]
- Compagnie Maritime d’Expertises COMEX. Available online: https://comex.fr/en/home/ (accessed on 21 June 2022).
- Wingelaar, T.T.; van Ooij, P.-J.A.M.; van Hulst, R.A. Oxygen Toxicity and Special Operations Forces Diving: Hidden and Dangerous. Front. Psychol. 2017, 8, 1263. [Google Scholar] [CrossRef] [Green Version]
- Klein, J. Normobaric Pulmonary Oxygen Toxicity. Anesth. Analg. 1990, 70, 195–207. [Google Scholar] [CrossRef]
- Thomson, L.; Paton, J. Oxygen Toxicity. Paediatr. Respir. Rev. 2014, 15, 120–123. [Google Scholar] [CrossRef]
- Miller, J.N.; Winter, P.M. Clinical Manifestations of Pulmonary Oxygen Toxicity. Int. Anesthesiol. Clin. 1980, 19, 179–200. [Google Scholar] [CrossRef]
- Risberg, J.; Nui, B.; van Ooij, P.-J.; Center, R.N.N.D.M. Hyperoxic exposure monitoring in diving: A farewell to the UPTD. Undersea Hyperb. Med. 2022, 49, 395–413. [Google Scholar] [CrossRef]
- Van Ooij, P.-J.A.; Sterk, P.J.; van Hulst, R.A. Oxygen, the lung and the diver: Friends and foes? Eur. Respir. Rev. 2016, 25, 496–505. [Google Scholar] [CrossRef] [Green Version]
- Clark, J.; Lambertsen, C. Pulmonary Oxygen Tolerance in Man and Derivation of Pulmonary Oxygen Tolerance Curves; Institute for Environmental Medicine, University of Pennsylvania: Philadelphia, PA, USA, 1970. [Google Scholar]
- Bardin, H.; Lambertsen, C.J. A Quantitative Method for Calculating Pulmonary Toxicity: Use of the ‘Unit Pulmonary Toxicity Dose’ (UPTD); Institute for Environmental Medicine, University of Pennsylvania: Philadelphia, PA, USA, 1970. [Google Scholar]
- Wright, W.B. Calculation of Cumulative Pulmonary Oxygen Toxicity; Navy Experimental Diving Unit: Panama City, FL, USA, 1972; pp. 1–25. [Google Scholar]
- Arieli, R. Calculated risk of pulmonary and central nervous system oxygen toxicity: A toxicity index derived from the power equation. Diving Hyperb. Med. J. 2019, 49, 154–160. [Google Scholar] [CrossRef]
- Van Ooij, P.-J.A.M. Pulmonary Oxygen Toxicity in Professional Diving: Scire Est Mensurare? Ph.D.Thesis, University of Amsterdam, Amsterdam, The Netherlands, 2013. [Google Scholar]
- Wingelaar, T.T. Detecting Pulmonary Oxygen Toxicity Using Exhaled Breath Markers. Ph.D.Thesis, University of Amsterdam, Amsterdam, The Netherlands, 2020. [Google Scholar]
- De Jong, F.J.M.; Wingelaar, T.T.; Brinkman, P.; van Ooij, P.-J.A.M.; Maitland-van der Zee, A.H.; Hollmann, M.W.; van Hulst, R.A. Pulmonary Oxygen Toxicity Through Exhaled Breath Markers After Hyperbaric Oxygen Treatment Table 6. Front. Physiol. 2022, 13, 899568. [Google Scholar] [CrossRef]
- ICH Harmonized Guideline. Integrated Addendum to ICH E6(R1): Guideline for Good Clinical Practice E6(R2). 2016. Available online: https://database.ich.org/sites/default/files/E6_R2_Addendum.pdf (accessed on 5 May 2022).
- SWOD Keuringsrichtlijn Arbeidsgezondheidskundig Onderzoek Werken Onder Overdruk—Duikarbeid—Cat 003.1 Revisie 4. 2021. Available online: https://www.arbocataloguswoo.nl/images/SWOD/pdf/NL/SWOD-ARBOCAT-WoO-Keuring-CAT003_1-2021-rev4-aug-2021.pdf (accessed on 25 May 2022).
- Wingelaar, T.T.; van Ooij, P.-J.A.M.; Brinkman, P.; van Hulst, R.A. Pulmonary Oxygen Toxicity in Navy Divers: A Crossover Study Using Exhaled Breath Analysis After a One-Hour Air or Oxygen Dive at Nine Meters of Sea Water. Front. Physiol. 2019, 10, 10. [Google Scholar] [CrossRef] [Green Version]
- Wingelaar, T.T.; Brinkman, P.; Van Ooij, P.J.A.M.; Hoencamp, R.; van Ooij, P.-J.A.M.; Maitland-van der Zee, A.-H.; Hollmann, M.W.; van Hulst, R.A. Markers of Pulmonary Oxygen Toxicity in Hyperbaric Oxygen Therapy Using Exhaled Breath Analysis. Front. Physiol. 2019, 10, 475. [Google Scholar] [CrossRef]
- Wingelaar, T.T.; Brinkman, P.; Hoencamp, R.; van Ooij, P.J.A.; Maitland-van der Zee, A.H.; Hollmnan, M.W.; van Hulst, R.A. Assessment of pulmonary oxygen toxicity in special operations forces divers under operational circumstances using exhaled breath analysis. Diving Hyperb. Med. J. 2020, 50, 2–7. [Google Scholar] [CrossRef]
- Kim, S.; Chen, J.; Cheng, T.; Gindulyte, A.; He, J.; He, S.; Li, Q.; Shoemaker, B.A.; Thiessen, P.A.; Yu, B.; et al. PubChem in 2021: New data content and improved web interfaces. Nucleic Acids Res. 2021, 49, D1388–D1395. [Google Scholar] [CrossRef]
- Wishart, D.S.; Guo, A.; Oler, E.; Wang, F.; Anjum, A.; Peters, H.; Dizon, R.; Sayeeda, Z.; Tian, S.; Lee, B.L.; et al. HMDB 5.0: The Human Metabolome Database for 2022. Nucleic Acids Res. 2022, 50, D622–D631. [Google Scholar] [CrossRef]
- Hastings, J.; Owen, G.; Dekker, A.; Ennis, M.; Kale, N.; Muthukrishnan, V.; Turner, S.; Swainston, N.; Mendes, P.; Steinbeck, C. ChEBI in 2016: Improved services and an expanding collection of metabolites. Nucleic Acids Res. 2016, 44, D1214–D1219. [Google Scholar] [CrossRef]
- Sayers, E.W.; Bolton, E.E.; Brister, J.R.; Canese, K.; Chan, J.; Comeau, D.C.; Connor, R.; Funk, K.; Kelly, C.; Kim, S.; et al. Database resources of the national center for biotechnology information. Nucleic Acids Res. 2022, 50, D20–D26. [Google Scholar] [CrossRef]
- Chatfield, M.; Mander, A. The Skillings–Mack Test (Friedman Test when There are Missing Data). Stata J. 2009, 9, 299–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shupak, A.; Atttas, J.; Aviv, S.; Melamed, Y. Oxygen Diving-induced Middle Ear Under-aeration. Acta Oto-Laryngol. 1995, 115, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Bjornson, W.; Rand, C.; Connett, J.E.; Lindgren, P.; Nides, M.; Pope, F.; Buist, A.S.; Hoppe-Ryan, C.; O’Hara, P. Gender differences in smoking cessation after 3 years in the Lung Health Study. Am. J. Public Health 1995, 85, 223–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinkerton, K.E.; Harbaugh, M.; Han, M.L.K.; Le Saux, C.J.; Van Winkle, L.S.; Martin, W.J.; Kosgei, R.J.; Carter, E.J.; Sitkin, N.; Smiley-Jewell, S.M.; et al. Women and Lung Disease. Sex Differences and Global Health Disparities. Am. J. Respir. Crit. Care Med. 2015, 192, 11–16. [Google Scholar] [CrossRef] [Green Version]
- Postma, D.S. Gender Differences in Asthma Development and Progression. Gend. Med. 2007, 4, S133–S146. [Google Scholar] [CrossRef]
- Pollock, N. DAN Annual Diving Report—2007 Edition; Divers Alert Network: Durham, NC, USA, 2007. [Google Scholar]
- Antonelli, C.; Franchi, F.; Della Marta, M.E.; Carinci, A.; Sbrana, G.; Tanasi, P.; De Fina, L.; Brauzzi, M. Guiding principles in choosing a therapeutic table for DCI hyperbaric therapy. Minerva Anestesiol. 2009, 75, 151–161. [Google Scholar]
- Kol, S.; Adir, Y.; Gordon, C.; Melamed, Y. Oxy-helium treatment of severe spinal decompression sickness after air diving. Undersea Hyperb. Med. 1993, 20, 147–154. [Google Scholar]
- Shupak, A.; Melamed, Y.; Ramon, Y.; Bentur, Y.; Abramovich, A.; Kol, S. Helium and Oxygen Treatment of Severe Air-Diving--Induced Neurologic Decompression Sickness. Arch. Neurol. 1997, 54, 305–311. [Google Scholar] [CrossRef]
- Aharon-Peretz, J.; Adir, Y.; Gordon, C.R.; Kol, S.; Gal, N.; Melamed, Y. Spinal Cord Decompression Sickness in Sport Diving. Arch. Neurol. 1993, 50, 753–756. [Google Scholar] [CrossRef]
- Rosen, A.; Oscarsson, N.; Gräbel, O.; Sandström, G. The Use of Treatment Table COMEX 30 for Severe Neurological Decompression Sickness. Lakartidningen 2017, 17, EA77. [Google Scholar]
- Bennett, M.H.; Mitchell, S.J.; Young, D.; King, D. The use of deep tables in the treatment of decompression illness: The Hyperbaric Technicians and Nurses Association 2011 Workshop. Diving Hyperb. Med. J. 2012, 42, 171–180. [Google Scholar]
- Haelewyn, B.; David, H.N.; Blatteau, J.-E.; Vallée, N.; Meckler, C.; Risso, J.-J.; Abraini, J.H. Modulation by the Noble Gas Helium of Tissue Plasminogen Activator: Effects in a Rat Model of Thromboembolic Stroke. Crit. Care Med. 2016, 44, e383–e389. [Google Scholar] [CrossRef]
- Pan, Y.; Zhang, H.; VanDeripe, D.R.; Cruz-Flores, S.; Panneton, W.M. Heliox and oxygen reduce infarct volume in a rat model of focal ischemia. Exp. Neurol. 2007, 205, 587–590. [Google Scholar] [CrossRef]
- Weber, N.C.; Preckel, B. Gaseous mediators: An updated review on the effects of helium beyond blowing up balloons. Intensiv. Care Med. Exp. 2019, 7, 73. [Google Scholar] [CrossRef] [Green Version]
- Ignatescu, M.; Bryson, P.; Klingmann, C. Susceptibility of the inner ear structure to shunt-related decompression sickness. Aviat. Space Environ. Med. 2012, 83, 1145–1151. [Google Scholar] [CrossRef]
- Lamote, K.; Brinkman, P.; Vandermeersch, L.; Vynck, M.; Sterk, P.J.; Van Langenhove, H.; Thas, O.; Van Cleemput, J.; Nackaerts, K.; van Meerbeeck, J.P. Breath analysis by gas chromatography-mass spectrometry and electronic nose to screen for pleural mesothelioma: A cross-sectional case-control study. Oncotarget 2017, 8, 91593–91602. [Google Scholar] [CrossRef] [Green Version]
- Fuchs, P.; Loeseken, C.; Schubert, J.K.; Miekisch, W. Breath gas aldehydes as biomarkers of lung cancer. Int. J. Cancer 2010, 126, 2663–2670. [Google Scholar] [CrossRef]
- Poli, D.; Goldoni, M.; Corradi, M.; Acampa, O.; Carbognani, P.; Internullo, E.; Casalini, A.; Mutti, A. Determination of aldehydes in exhaled breath of patients with lung cancer by means of on-fiber-derivatisation SPME–GC/MS. J. Chromatogr. B 2010, 878, 2643–2651. [Google Scholar] [CrossRef]
- Caldeira, M.; Barros, A.; Bilelo, M.; Parada, A.; Câmara, J.; Rocha, S. Profiling allergic asthma volatile metabolic patterns using a headspace-solid phase microextraction/gas chromatography based methodology. J. Chromatogr. A 2011, 1218, 3771–3780. [Google Scholar] [CrossRef]
- Hakim, M.; Broza, Y.Y.; Barash, O.; Peled, N.; Phillips, M.; Amann, A.; Haick, H. Volatile Organic Compounds of Lung Cancer and Possible Biochemical Pathways. Chem. Rev. 2012, 112, 5949–5966. [Google Scholar] [CrossRef]
- Ratcliffe, N.; Wieczorek, T.; Drabińska, N.; Gould, O.; Osborne, A.; de Lacy Costello, B. A mechanistic study and review of volatile products from peroxidation of unsaturated fatty acids: An aid to understanding the origins of volatile organic compounds from the human body. J. Breath Res. 2020, 14, 034001. [Google Scholar] [CrossRef] [PubMed]
- The Human Metabolome Database Ethyl Acetate. Available online: https://hmdb.ca/metabolites/HMDB0031217 (accessed on 20 April 2022).
- Wingelaar, T.T.; Brinkman, P.; de Vries, R.; van Ooij, P.-J.A.; Hoencamp, R.; Maitland-Van der Zee, A.H.; Hollmann, M.W.; van Hulst, R.A. Detecting Pulmonary Oxygen Toxicity Using eNose Technology and Associations between Electronic Nose and Gas Chromatography–Mass Spectrometry Data. Metabolites 2019, 9, 286. [Google Scholar] [CrossRef] [Green Version]
- Van Mastrigt, E.; Reyes-Reyes, A.; Brand, K.; Bhattacharya, N.; Urbach, H.P.; Stubbs, A.P.; De Jongste, J.C.; Pijnenburg, M.W. Exhaled breath profiling using broadband quantum cascade laser-based spectroscopy in healthy children and children with asthma and cystic fibrosis. J. Breath Res. 2016, 10, 026003. [Google Scholar] [CrossRef] [PubMed]
- Amal, H.; Leja, M.; Funka, K.; Lasina, I.; Skapars, R.; Sivins, A.; Ancans, G.; Kikuste, I.; Vanags, A.; Tolmanis, I.; et al. Breath testing as potential colorectal cancer screening tool. Int. J. Cancer 2016, 138, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Buszewski, B.; Ligor, T.; Jezierski, T.; Wenda-Piesik, A.; Walczak, M.; Rudnicka, J. Identification of volatile lung cancer markers by gas chromatography–mass spectrometry: Comparison with discrimination by canines. Anal. Bioanal. Chem. 2012, 404, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Zou, Y.; Zhang, X.; Chen, X.; Hu, Y.; Ying, K.; Wang, P. Optimization of volatile markers of lung cancer to exclude interferences of non-malignant disease. Cancer Biomark. 2014, 14, 371–379. [Google Scholar] [CrossRef]
- Phillips, M.; Cataneo, R.N.; Saunders, C.; Hope, P.; Schmitt, P.; Wai, J. Volatile biomarkers in the breath of women with breast cancer. J. Breath Res. 2010, 4, 026003. [Google Scholar] [CrossRef]
- Ayala, A.; Muñoz, M.F.; Argüelles, S. Lipid peroxidation: Production, metabolism, and signaling mechanisms of malondialdehyde and 4-hydroxy-2-nonenal. Oxidative Med. Cell. Longev. 2014, 2014, 360438. [Google Scholar] [CrossRef] [Green Version]
- Kneepkens, C.F.; Lepage, G.; Roy, C.C. The potential of the hydrocarbon breath test as a measure of lipid peroxidation. Free. Radic. Biol. Med. 1994, 17, 127–160. [Google Scholar] [CrossRef]
- De Jong, F.J.M.; Brinkman, P.; Wingelaar, T.T.; van Ooij, P.-J.A.M.; van Hulst, R.A. Volatile Organic Compounds Frequently Identified after Hyperbaric Hyperoxic Exposure: The VAPOR Library. Metabolites 2022, 12, 470. [Google Scholar] [CrossRef]
- Van Ooij, P.; van Hulst, R.; Kulik, W.; Brinkman, P.; Houtkooper, A.; Sterk, P. Hyperbaric oxygen diving affects exhaled molecular profiles in men. Respir. Physiol. Neurobiol. 2014, 198, 20–24. [Google Scholar] [CrossRef]
- Lansdorp, N.C.; Van Hulst, R.A. Double-blind trials in hyperbaric medicine: A narrative review on past experiences and considerations in designing sham hyperbaric treatment. Clin. Trials 2018, 15, 462–476. [Google Scholar] [CrossRef]
- Blanchet, L.; Smolinska, A.; Baranska, A.; Tigchelaar, E.; Swertz, M.; Zhernakova, A.; Dallinga, J.W.; Wijmenga, C.; van Schooten, F.J. Factors that influence the volatile organic compound content in human breath. J. Breath Res. 2017, 11, 016013. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 10) | Men (n = 7) | Women (n = 3) | |
|---|---|---|---|
| Age (years) | 34.5 (7.8) | 34 (4.5) | 41 (12) |
| Height (cm) | 180 (8.5) | 184 (9) | 171 (7) |
| Weight (kg) | 79.5 (14.3) | 85 (12) | 69 (5) |
| BMI (kg/m2) | 24.5 (1.3) | 24.7 (1.4) | 22.1 (0.8) |
| Men (n = 7) | Women (n = 3) | Total (n = 10) | |
|---|---|---|---|
| Pulmonary/lower respiratory tract | 4 | 3 | 7 |
| Constitutional | 3 | 3 | 6 |
| Fatigue | 2 | 3 | 5 |
| Dehydration | 2 | 2 | 4 |
| Upper respiratory tract | 5 | 1 | 6 |
| “Oxygen ear” | 4 | 1 | 5 |
| Dry mucosa | 2 | 1 | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Jong, F.J.M.; Wingelaar, T.T.; Brinkman, P.; van Ooij, P.-J.A.M.; Maitland-van der Zee, A.H.; Hollmann, M.W.; van Hulst, R.A. Analysis of Volatile Organic Compounds in Exhaled Breath Following a COMEX-30 Treatment Table. Metabolites 2023, 13, 316. https://doi.org/10.3390/metabo13030316
de Jong FJM, Wingelaar TT, Brinkman P, van Ooij P-JAM, Maitland-van der Zee AH, Hollmann MW, van Hulst RA. Analysis of Volatile Organic Compounds in Exhaled Breath Following a COMEX-30 Treatment Table. Metabolites. 2023; 13(3):316. https://doi.org/10.3390/metabo13030316
Chicago/Turabian Stylede Jong, Feiko J. M., Thijs T. Wingelaar, Paul Brinkman, Pieter-Jan A. M. van Ooij, Anke H. Maitland-van der Zee, Markus W. Hollmann, and Rob A. van Hulst. 2023. "Analysis of Volatile Organic Compounds in Exhaled Breath Following a COMEX-30 Treatment Table" Metabolites 13, no. 3: 316. https://doi.org/10.3390/metabo13030316