
Olive Oil Polyphenols Improve HDL Cholesterol and Promote Maintenance of Lipid Metabolism: A Systematic Review and Meta-Analysis of Randomized Controlled Trials

 ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
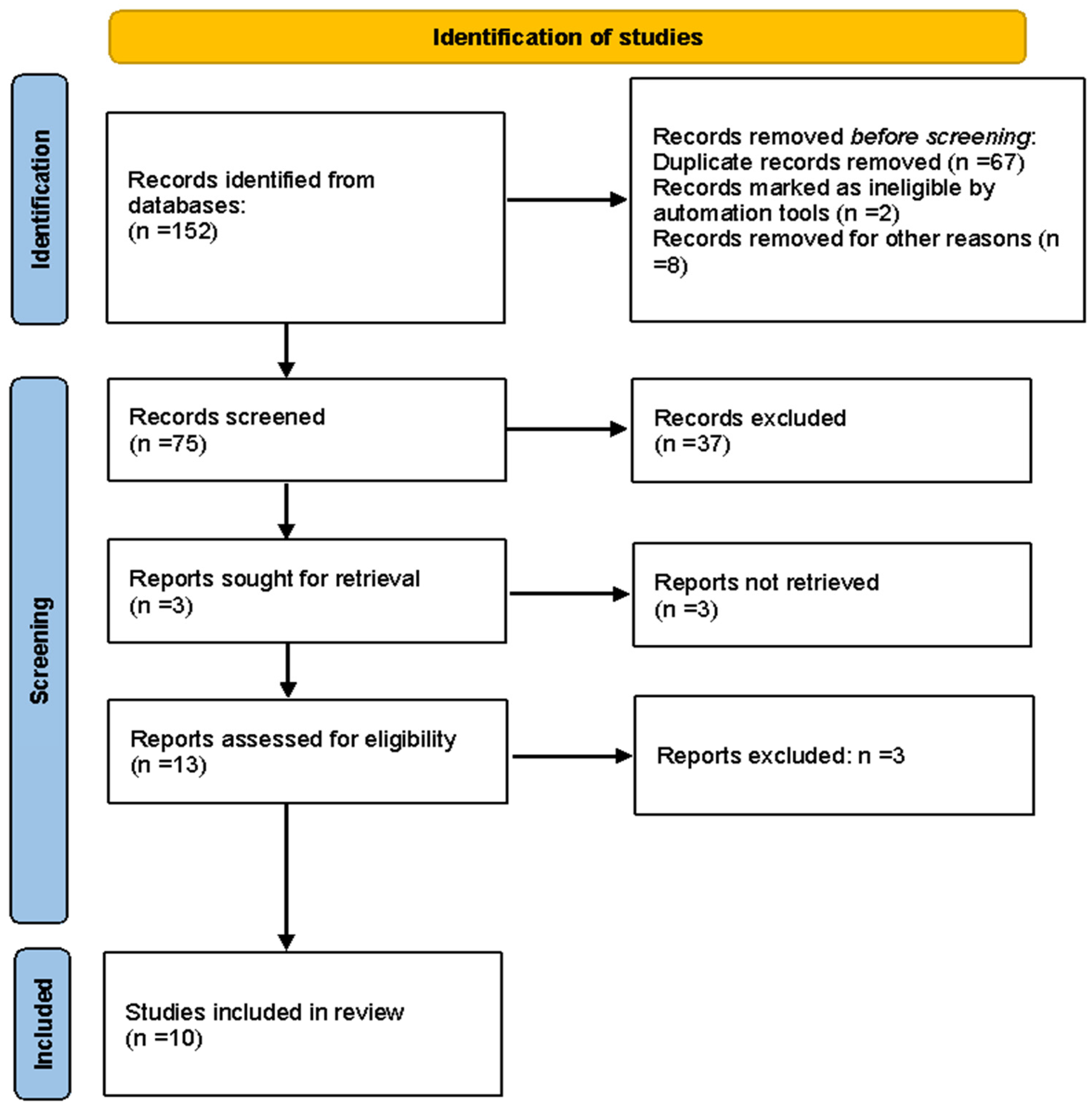
2. Methods
2.1. Search Strategy, Study Selection, and Data Extraction
2.2. Quality Assessment
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Vaduganathan, M.; Mensah, G.A.; Turco, J.V.; Fuster, V.; Roth, G.A. The Global Burden of Cardiovascular Diseases and Risk: A Compass for Future Health. J. Am. Coll. Cardiol. 2022, 80, 2361–2371. [Google Scholar] [CrossRef] [PubMed]
- Clodoveo, M.L.; Tarsitano, E.; Sabbà, C.; Gesualdo, L.; Corbo, F. Med-Index: A Food Product Labeling System to Promote Adherence to the Mediterranean Diet Encouraging Producers to Make Healthier and More Sustainable Food Products. Ital. J. Food Sci. 2021, 33, 67–83. [Google Scholar] [CrossRef]
- Nestel, P.J.; Mori, T.A. Dietary Patterns, Dietary Nutrients and Cardiovascular Disease. Rev. Cardiovasc. Med. 2022, 23, 17. [Google Scholar] [CrossRef] [PubMed]
- Tangney, C.C.; Rasmussen, H.E. Polyphenols, Inflammation, and Cardiovascular Disease. Curr. Atheroscler. Rep. 2013, 15, 324. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific and Technical Guidance for the Preparation and Presentation of a Health Claim Application (Revision 3). EFSA J. 2021, 19, e06554. [Google Scholar]
- Toth, P.P.; Barter, P.J.; Rosenson, R.S.; Boden, W.E.; Chapman, M.J.; Cuchel, M.; D’Agostino, R.B., Sr.; Davidson, M.H.; Davidson, W.S.; Heinecke, J.W.; et al. High-Density Lipoproteins: A Consensus Statement from the National Lipid Association. J. Clin. Lipidol. 2013, 7, 484–525. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Dhindsa, D.; Almuwaqqat, Z.; Ko, Y.-A.; Mehta, A.; Alkhoder, A.A.; Alras, Z.; Desai, S.R.; Patel, K.J.; Hooda, A.; et al. Association between High-Density Lipoprotein Cholesterol Levels and Adverse Cardiovascular Outcomes in High-Risk Populations. JAMA Cardiol. 2022, 7, 672–680. [Google Scholar] [CrossRef]
- Rees, K.; Hartley, L.; Flowers, N.; Clarke, A.; Hooper, L.; Thorogood, M.; Stranges, S. “Mediterranean” Dietary Pattern for the Primary Prevention of Cardiovascular Disease. Cochrane Database Syst. Rev. 2013, CD009825. [Google Scholar] [CrossRef]
- Kastorini, C.-M.; Milionis, H.J.; Esposito, K.; Giugliano, D.; Goudevenos, J.A.; Panagiotakos, D.B. The Effect of Mediterranean Diet on Metabolic Syndrome and Its Components: A Meta-Analysis of 50 Studies and 534,906 Individuals. J. Am. Coll. Cardiol. 2011, 57, 1299–1313. [Google Scholar] [CrossRef]
- Clodoveo, M.L.; Dipalmo, T.; Schiano, C.; La Notte, D.; Pati, S. What’s Now, What’s New and What’s next in Virgin Olive Oil Elaboration Systems? A Perspective on Current Knowledge and Future Trends. J. Agric. Eng. Res. 2014, 45, 49. [Google Scholar] [CrossRef]
- Flynn, M.M.; Tierney, A.; Itsiopoulos, C. Is Extra Virgin Olive Oil the Critical Ingredient Driving the Health Benefits of a Mediterranean Diet? A Narrative Review. Nutrients 2023, 15, 2916. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-López, P.; Lozano-Sanchez, J.; Borrás-Linares, I.; Emanuelli, T.; Menéndez, J.A.; Segura-Carretero, A. Structure-Biological Activity Relationships of Extra-Virgin Olive Oil Phenolic Compounds: Health Properties and Bioavailability. Antioxidants 2020, 9, 685. [Google Scholar] [CrossRef] [PubMed]
- Finicelli, M.; Squillaro, T.; Di Cristo, F.; Di Salle, A.; Melone, M.A.B.; Galderisi, U.; Peluso, G. Metabolic Syndrome, Mediterranean Diet, and Polyphenols: Evidence and Perspectives. J. Cell. Physiol. 2019, 234, 5807–5826. [Google Scholar] [CrossRef] [PubMed]
- Robles-Almazan, M.; Pulido-Moran, M.; Moreno-Fernandez, J.; Ramirez-Tortosa, C.; Rodriguez-Garcia, C.; Quiles, J.L.; Ramirez-Tortosa, M. Hydroxytyrosol: Bioavailability, Toxicity, and Clinical Applications. Food Res. Int. 2018, 105, 654–667. [Google Scholar] [CrossRef] [PubMed]
- Rigacci, S.; Stefani, M. Nutraceutical Properties of Olive Oil Polyphenols. An Itinerary from Cultured Cells through Animal Models to Humans. Int. J. Mol. Sci. 2016, 17, 843. [Google Scholar] [CrossRef] [PubMed]
- Fabiani, R. Anti-Cancer Properties of Olive Oil Secoiridoid Phenols: A Systematic Review of in Vivo Studies. Food Funct. 2016, 7, 4145–4159. [Google Scholar] [CrossRef] [PubMed]
- Cicerale, S.; Lucas, L.J.; Keast, R.S.J. Antimicrobial, Antioxidant and Anti-Inflammatory Phenolic Activities in Extra Virgin Olive Oil. Curr. Opin. Biotechnol. 2012, 23, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Lammi, C.; Bellumori, M.; Cecchi, L.; Bartolomei, M.; Bollati, C.; Clodoveo, M.L.; Corbo, F.; Arnoldi, A.; Mulinacci, N. Extra Virgin Olive Oil Phenol Extracts Exert Hypocholesterolemic Effects through the Modulation of the LDLR Pathway: In Vitro and Cellular Mechanism of Action Elucidation. Nutrients 2020, 12, 1723. [Google Scholar] [CrossRef]
- De Santis, S.; Liso, M.; Verna, G.; Curci, F.; Milani, G.; Faienza, M.F.; Franchini, C.; Moschetta, A.; Chieppa, M.; Clodoveo, M.L.; et al. Extra Virgin Olive Oil Extracts Modulate the Inflammatory Ability of Murine Dendritic Cells Based on Their Polyphenols Pattern: Correlation between Chemical Composition and Biological Function. Antioxidants 2021, 10, 1016. [Google Scholar] [CrossRef]
- Joseph, S.V.; Edirisinghe, I.; Burton-Freeman, B.M. Fruit Polyphenols: A Review of Anti-Inflammatory Effects in Humans. Crit. Rev. Food Sci. Nutr. 2016, 56, 419–444. [Google Scholar] [CrossRef]
- Perez-Martinez, P.; Perez-Jimenez, F.; Lopez-Miranda, J. The Beneficial Effects of Virgin Olive Oil on Nuclear Transcription Factor kappaB and Other Inflammatory Markers. In Olives and Olive Oil in Health and Disease Prevention; Academic Press: Cambridge, MA, USA, 2010; pp. 1067–1070. [Google Scholar]
- De Santis, S.; Clodoveo, M.L.; Corbo, F. Correlation between Chemical Characterization and Biological Activity: An Urgent Need for Human Studies Using Extra Virgin Olive Oil. Antioxidants 2022, 11, 258. [Google Scholar] [CrossRef] [PubMed]
- Parkinson, L.; Cicerale, S. The Health Benefiting Mechanisms of Virgin Olive Oil Phenolic Compounds. Molecules 2016, 21, 1734. [Google Scholar] [CrossRef] [PubMed]
- Peyrol, J.; Riva, C.; Amiot, M.J. Hydroxytyrosol in the Prevention of the Metabolic Syndrome and Related Disorders. Nutrients 2017, 9, 306. [Google Scholar] [CrossRef] [PubMed]
- Crupi, P.; Bleve, G.; Tufariello, M.; Corbo, F.; Clodoveo, M.L.; Tarricone, L. Comprehensive Identification and Quantification of Chlorogenic Acids in Sweet Cherry by Tandem Mass Spectrometry Techniques. J. Food Compost. Anal. 2018, 73, 103–111. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the Substantiation of a Health Claim Related to Polyphenols in Olive and Maintenance of Normal Blood HDL Cholesterol Concentrations (ID 1639, Further Assessment) pursuant to Article 13(1) of Regulation (EC) No 1924/2006. EFSA J. 2012, 10, 2848. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Belur, J.; Tompson, L.; Thornton, A.; Simon, M. Interrater Reliability in Systematic Review Methodology: Exploring Variation in Coder Decision-Making. Sociol. Methods Res. 2021, 50, 837–865. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2021; ISBN 9781119558392. [Google Scholar]
- Sarapis, K.; George, E.S.; Marx, W.; Mayr, H.L.; Willcox, J.; Powell, K.L.; Folasire, O.S.; Lohning, A.E.; Prendergast, L.A.; Itsiopoulos, C.; et al. Extra Virgin Olive Oil Improves HDL Lipid Fraction but Not HDL-Mediated Cholesterol Efflux Capacity: A Double-Blind, Randomised, Controlled, Cross-over Study (OLIVAUS). Br. J. Nutr. 2023, 130, 641–650. [Google Scholar] [CrossRef]
- Khandouzi, N.; Zahedmehr, A.; Nasrollahzadeh, J. Effect of Polyphenol-Rich Extra-Virgin Olive Oil on Lipid Profile and Inflammatory Biomarkers in Patients Undergoing Coronary Angiography: A Randomised, Controlled, Clinical Trial. Int. J. Food Sci. Nutr. 2021, 72, 548–558. [Google Scholar] [CrossRef]
- Sanchez-Rodriguez, E.; Lima-Cabello, E.; Biel-Glesson, S.; Fernandez-Navarro, J.R.; Calleja, M.A.; Roca, M.; Espejo-Calvo, J.A.; Gil-Extremera, B.; Soria-Florido, M.; de la Torre, R.; et al. Effects of Virgin Olive Oils Differing in Their Bioactive Compound Contents on Metabolic Syndrome and Endothelial Functional Risk Biomarkers in Healthy Adults: A Randomized Double-Blind Controlled Trial. Nutrients 2018, 10, 626. [Google Scholar] [CrossRef]
- Santangelo, C.; Filesi, C.; Varì, R.; Scazzocchio, B.; Filardi, T.; Fogliano, V.; D’Archivio, M.; Giovannini, C.; Lenzi, A.; Morano, S.; et al. Consumption of Extra-Virgin Olive Oil Rich in Phenolic Compounds Improves Metabolic Control in Patients with Type 2 Diabetes Mellitus: A Possible Involvement of Reduced Levels of Circulating Visfatin. J. Endocrinol. Investig. 2016, 39, 1295–1301. [Google Scholar] [CrossRef]
- Fernández-Castillejo, S.; Valls, R.-M.; Castañer, O.; Rubió, L.; Catalán, Ú.; Pedret, A.; Macià, A.; Sampson, M.L.; Covas, M.-I.; Fitó, M.; et al. Polyphenol Rich Olive Oils Improve Lipoprotein Particle Atherogenic Ratios and Subclasses Profile: A Randomized, Crossover, Controlled Trial. Mol. Nutr. Food Res. 2016, 60, 1544–1554. [Google Scholar] [CrossRef] [PubMed]
- Hernáez, Á.; Fernández-Castillejo, S.; Farràs, M.; Catalán, Ú.; Subirana, I.; Montes, R.; Solà, R.; Muñoz-Aguayo, D.; Gelabert-Gorgues, A.; Díaz-Gil, Ó.; et al. Olive Oil Polyphenols Enhance High-Density Lipoprotein Function in Humans: A Randomized Controlled Trial. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 2115–2119. [Google Scholar] [CrossRef] [PubMed]
- Konstantinidou, V.; Covas, M.-I.; Muñoz-Aguayo, D.; Khymenets, O.; de la Torre, R.; Saez, G.; Tormos, M.d.C.; Toledo, E.; Marti, A.; Ruiz-Gutiérrez, V.; et al. In Vivo Nutrigenomic Effects of Virgin Olive Oil Polyphenols within the Frame of the Mediterranean Diet: A Randomized Controlled Trial. FASEB J. 2010, 24, 2546–2557. [Google Scholar] [CrossRef] [PubMed]
- Covas, M.-I.; Nyyssönen, K.; Poulsen, H.E.; Kaikkonen, J.; Zunft, H.-J.F.; Kiesewetter, H.; Gaddi, A.; de la Torre, R.; Mursu, J.; Bäumler, H.; et al. The Effect of Polyphenols in Olive Oil on Heart Disease Risk Factors: A Randomized Trial. Ann. Intern. Med. 2006, 145, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Marrugat, J.; Covas, M.-I.; Fitó, M.; Schröder, H.; Miró-Casas, E.; Gimeno, E.; López-Sabater, M.C.; de la Torre, R.; Farré, M. SOLOS Investigators Effects of Differing Phenolic Content in Dietary Olive Oils on Lipids and LDL Oxidation—A Randomized Controlled Trial. Eur. J. Nutr. 2004, 43, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Weinbrenner, T.; Fitó, M.; de la Torre, R.; Saez, G.T.; Rijken, P.; Tormos, C.; Coolen, S.; Albaladejo, M.F.; Abanades, S.; Schroder, H.; et al. Olive Oils High in Phenolic Compounds Modulate Oxidative/antioxidative Status in Men. J. Nutr. 2004, 134, 2314–2321. [Google Scholar] [CrossRef] [PubMed]
- Lockyer, S.; Rowland, I. Authorised EU Health Claims for Polyphenols in Olive Oil. In Foods, Nutrients and Food Ingredients with Authorised EU Health Claims; Woodhead Publishing: Cambridge, UK, 2014; pp. 212–228. [Google Scholar]
- Visioli, F.; Poli, A.; Gall, C. Antioxidant and Other Biological Activities of Phenols from Olives and Olive Oil. Med. Res. Rev. 2002, 22, 65–75. [Google Scholar] [CrossRef] [PubMed]
- González-Santiago, M.; Fonollá, J.; Lopez-Huertas, E. Human Absorption of a Supplement Containing Purified Hydroxytyrosol, a Natural Antioxidant from Olive Oil, and Evidence for Its Transient Association with Low-Density Lipoproteins. Pharmacol. Res. 2010, 61, 364–370. [Google Scholar] [CrossRef]
- Visioli, F.; Caruso, D.; Grande, S.; Bosisio, R.; Villa, M.; Galli, G.; Sirtori, C.; Galli, C. Virgin Olive Oil Study (VOLOS): Vasoprotective Potential of Extra Virgin Olive Oil in Mildly Dyslipidemic Patients. Eur. J. Nutr. 2005, 44, 121–127. [Google Scholar] [CrossRef]
- Carluccio, M.A.; Massaro, M.; Scoditti, E.; De Caterina, R. Vasculoprotective Potential of Olive Oil Components. Mol. Nutr. Food Res. 2007, 51, 1225–1234. [Google Scholar] [CrossRef]
- Alemany, R.; Navarro, M.A.; Vögler, O.; Perona, J.S.; Osada, J.; Ruiz-Gutiérrez, V. Olive Oils Modulate Fatty Acid Content and Signaling Protein Expression in Apolipoprotein E Knockout Mice Brain. Lipids 2010, 45, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Loued, S.; Berrougui, H.; Componova, P.; Ikhlef, S.; Helal, O.; Khalil, A. Extra-Virgin Olive Oil Consumption Reduces the Age-Related Decrease in HDL and Paraoxonase 1 Anti-Inflammatory Activities. Br. J. Nutr. 2013, 110, 1272–1284. [Google Scholar] [CrossRef]
- Malliou, F.; Andreadou, I.; Gonzalez, F.J.; Lazou, A.; Xepapadaki, E.; Vallianou, I.; Lambrinidis, G.; Mikros, E.; Marselos, M.; Skaltsounis, A.-L.; et al. The Olive Constituent Oleuropein, as a PPARα Agonist, Markedly Reduces Serum Triglycerides. J. Nutr. Biochem. 2018, 59, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Pirat, C.; Farce, A.; Lebègue, N.; Renault, N.; Furman, C.; Millet, R.; Yous, S.; Speca, S.; Berthelot, P.; Desreumaux, P.; et al. Targeting Peroxisome Proliferator-Activated Receptors (PPARs): Development of Modulators. J. Med. Chem. 2012, 55, 4027–4061. [Google Scholar] [CrossRef] [PubMed]
- Priore, P.; Siculella, L.; Gnoni, G.V. Extra Virgin Olive Oil Phenols down-Regulate Lipid Synthesis in Primary-Cultured Rat-Hepatocytes. J. Nutr. Biochem. 2014, 25, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Krzeminski, R.; Gorinstein, S.; Leontowicz, H.; Leontowicz, M.; Gralak, M.; Czerwinski, J.; Lojek, A.; Cíz, M.; Martin-Belloso, O.; Gligelmo-Miguel, N.; et al. Effect of Different Olive Oils on Bile Excretion in Rats Fed Cholesterol-Containing and Cholesterol-Free Diets. J. Agric. Food Chem. 2003, 51, 5774–5779. [Google Scholar] [CrossRef] [PubMed]
- Pushpass, R.-A.G.; Alzoufairi, S.; Jackson, K.G.; Lovegrove, J.A. Circulating Bile Acids as a Link between the Gut Microbiota and Cardiovascular Health: Impact of Prebiotics, Probiotics and Polyphenol-Rich Foods. Nutr. Res. Rev. 2022, 35, 161–180. [Google Scholar] [CrossRef]
- Koutsos, A.; Tuohy, K.M.; Lovegrove, J.A. Apples and Cardiovascular Health—Is the Gut Microbiota a Core Consideration? Nutrients 2015, 7, 3959–3998. [Google Scholar] [CrossRef]
- Deiana, M.; Serra, G.; Corona, G. Modulation of Intestinal Epithelium Homeostasis by Extra Virgin Olive Oil Phenolic Compounds. Food Funct. 2018, 9, 4085–4099. [Google Scholar] [CrossRef] [PubMed]
- Skrypnik, K.; Bogdański, P.; Łoniewski, I.; Reguła, J.; Suliburska, J. Effect of Probiotic Supplementation on Liver Function and Lipid Status in Rats. Acta Sci. Pol. Technol. Aliment. 2018, 17, 185–192. [Google Scholar] [PubMed]
- Wu, H.; Chiou, J. Potential Benefits of Probiotics and Prebiotics for Coronary Heart Disease and Stroke. Nutrients 2021, 13, 2878. [Google Scholar] [CrossRef] [PubMed]
- Ambra, R.; Lucchetti, S.; Pastore, G. A Review of the Effects of Olive Oil-Cooking on Phenolic Compounds. Molecules 2022, 27, 661. [Google Scholar] [CrossRef]
- Clodoveo, M.L. An Overview of Emerging Techniques in Virgin Olive Oil Extraction Process: Strategies in the Development of Innovative Plants. J. Agric. Eng. Res. 2013, 44. [Google Scholar] [CrossRef]
- Amirante, P.; Clodoveo, M.L.; Tamborrino, A.; Leone, A.; Paice, A.G. Influence of the Crushing System: Phenol Content in Virgin Olive Oil Produced from Whole and De-Stoned Pastes. In Olives and Olive Oil in Health and Disease Prevention; Academic Press: Cambridge, MA, USA, 2010; pp. 69–76. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year [Ref.] | Country | Population | Design | Inclusion Criteria | Exclusion Criteria | Washout Period | n | Age | Daily Dose (mL) | Intervention Duration |
|---|---|---|---|---|---|---|---|---|---|---|
| Sarapis, 2022 [31] | Australia | Healthy adults | Double-blind, cross-over RCT | BMI between 18.5–40 kg/m2 | Smoking, pregnant, or lactating women, hyperlipidemia, diabetes, hypertension, inflammatory conditions (e.g., rheumatoid arthritis), intestinal disease (e.g., inflammatory bowel disease; irritable bowel syndrome), food intolerances, blood coagulation disorders, and any cognitive or mood disorder | 2-weeks | 20 | 20–70 | 60 | 3-weeks |
| Khandouzi, 2021 [32] | Iran | Men and post-menopausal women | Parallel-arm, RCT | Having at least one of the major cardiovascular risk factors including hypertension, diabetes mellitus, dyslipidemia, or acute cardiac events. | Administering anti-inflammatory medication, dietary antioxidants, or omega-3 supplements the month before the study, consumption of less than 80% of the olive oil delivered to the participants, lipid-lowering medications or coronary artery bypass graft (CABG), and gastrointestinal complications, such as diarrhea. | Not applicable | 20 | 20–75 | 25 | 6-weeks |
| Sanchez-Rodriguez, 2018 [33] | Spain | General population | Double-blind, cross-over RCT | Being in good health based on a physical examination and basic biochemical and hematological analyses, and willingness to provide written informed consent. basic biochemical and hematological analyses, | Smoking, intake of antioxidant supplements, aspirin or any other drugs with established antioxidant properties, hyperlipidemia, obesity (BMI > 30 kg/m2), diabetes, hypertension, celiac, or other intestinal disease, any condition limiting mobility, and life-threatening diseases. | 2-weeks | 51 | 20–50 | 30 | 3-weeks |
| Santangelo, 2016 [34] | Italy | T2D patients | Cross-over RCT | Type 2 diabetes | Age > 80 years, smoking habits, use of antioxidant supplements, insulin treatment, use of aspirin or drugs with established antioxidant properties, history of CVD, any severe chronic illness, liver and renal failure, hormone replacement therapy, hyper- or hypothyroidism, drug or alcoholic addiction, severe history of allergy, or intolerance to olive oil | 4-weeks | 11 | 55–80 | 25 | 4-weeks |
| Fernández-Castillejo, 2016 [35] | Spain | Hypercholesterolemic (TC > 200 mg/dL) | Double blind, cross-over RCT | Normal blood pressure, hypercholesterolemic | Smoking, LDL-C > 190 mg/dL, TG > 350 mg/dL, fasting blood glucose > 126 mg/dL, plasma creatinine levels > 1.4 mg/dL for women and >1.5 mg/dL for men, BMI > 35, smokers (>1 cigarette/day), athletes with physical activity (>3000 METS min/day), hypertension, multiple allergies, intestinal diseases, chronic diseases (i.e., diabetes, cardiovascular) | 2-weeks | 11 | 40–70 | 25 | 3-weeks |
| Hernáez, 2014 [36] | Germany, Finland, Spain | Healthy male volunteers | Cross-over RCT | Healthy men | Smoking, use of antioxidant supplements, aspirin or any drug with antioxidant properties, hyperlipidemia, diabetes, intestinal disease | 2-weeks | 47 | 20–50 | 25 | 3-weeks |
| Konstantinidou, 2010 [37] | UK | Community | Parallel RCT | Healthy | Intake of antioxidant supplements, intake of acetosalicylic acid or any other drug with established antioxidative proper- ties, high levels of physical activity (3000 kcal/week in leisure time physical activity), obesity (body mass index (BMI) > 30 kg/m2), hypercholesterolemia (total cholesterol > 8.0 mM or dyslipidemia therapy), diabetes (glucose > 126 mg/dL or diabetes treatment); hypertension | Not applicable | 30 | 20–50 | 25 | 3 months |
| Covas, 2006 [38] | Spain, Denmark, Germany, Italy, Finland | Healthy male volunteers | Cross-over RCT | Healthy men | Smoking, use of antioxidant supplements, aspirin or any drug with antioxidant properties, hyperlipidemia, diabetes, intestinal disease | 2-weeks | 183 | 20–60 | 25 | 3-weeks |
| Marrugat, 2004 [39] | Spain | Healthy male | Cross-over RCT | Non-smoking volunteers | Smoking, intake of antioxidant supplements, aspirin or any other drug with established antioxidant properties, obesity (body mass index > 30 kg/m2), dyslipidemia, diabetes, celiac or other intestinal disease, any condition limiting mobility, life-threatening diseases, or any other disease or condition that would impair compliance | 2-weeks | 30 | 20–70 | 25 | 4-weeks |
| Weinbrenner, 2004 [40] | Spain | Healthy male | Double blind, cross-over RCT | Healthy by medical history, a complete physical examination, and standard laboratory tests. | Intake of antioxidant supplements, aspirin or any other drug with established antioxidant properties, obesity (BMI 30 kg/m2), diabetes, hyperlipidemia, intestinal diseases, physical activity 12.6 MJ/w, or any condition that would impair compliance. | 10 days | 12 | 20–22 | 25 | 4 days |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zupo, R.; Castellana, F.; Crupi, P.; Desantis, A.; Rondanelli, M.; Corbo, F.; Clodoveo, M.L. Olive Oil Polyphenols Improve HDL Cholesterol and Promote Maintenance of Lipid Metabolism: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Metabolites 2023, 13, 1187. https://doi.org/10.3390/metabo13121187
Zupo R, Castellana F, Crupi P, Desantis A, Rondanelli M, Corbo F, Clodoveo ML. Olive Oil Polyphenols Improve HDL Cholesterol and Promote Maintenance of Lipid Metabolism: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Metabolites. 2023; 13(12):1187. https://doi.org/10.3390/metabo13121187
Chicago/Turabian StyleZupo, Roberta, Fabio Castellana, Pasquale Crupi, Addolorata Desantis, Mariangela Rondanelli, Filomena Corbo, and Maria Lisa Clodoveo. 2023. "Olive Oil Polyphenols Improve HDL Cholesterol and Promote Maintenance of Lipid Metabolism: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Metabolites 13, no. 12: 1187. https://doi.org/10.3390/metabo13121187