

The Effect of a Gluten-Free Diet on Vitamin D Metabolism in Celiac Disease: The State of the Art
 , ,
, ,
Abstract
:1. Introduction
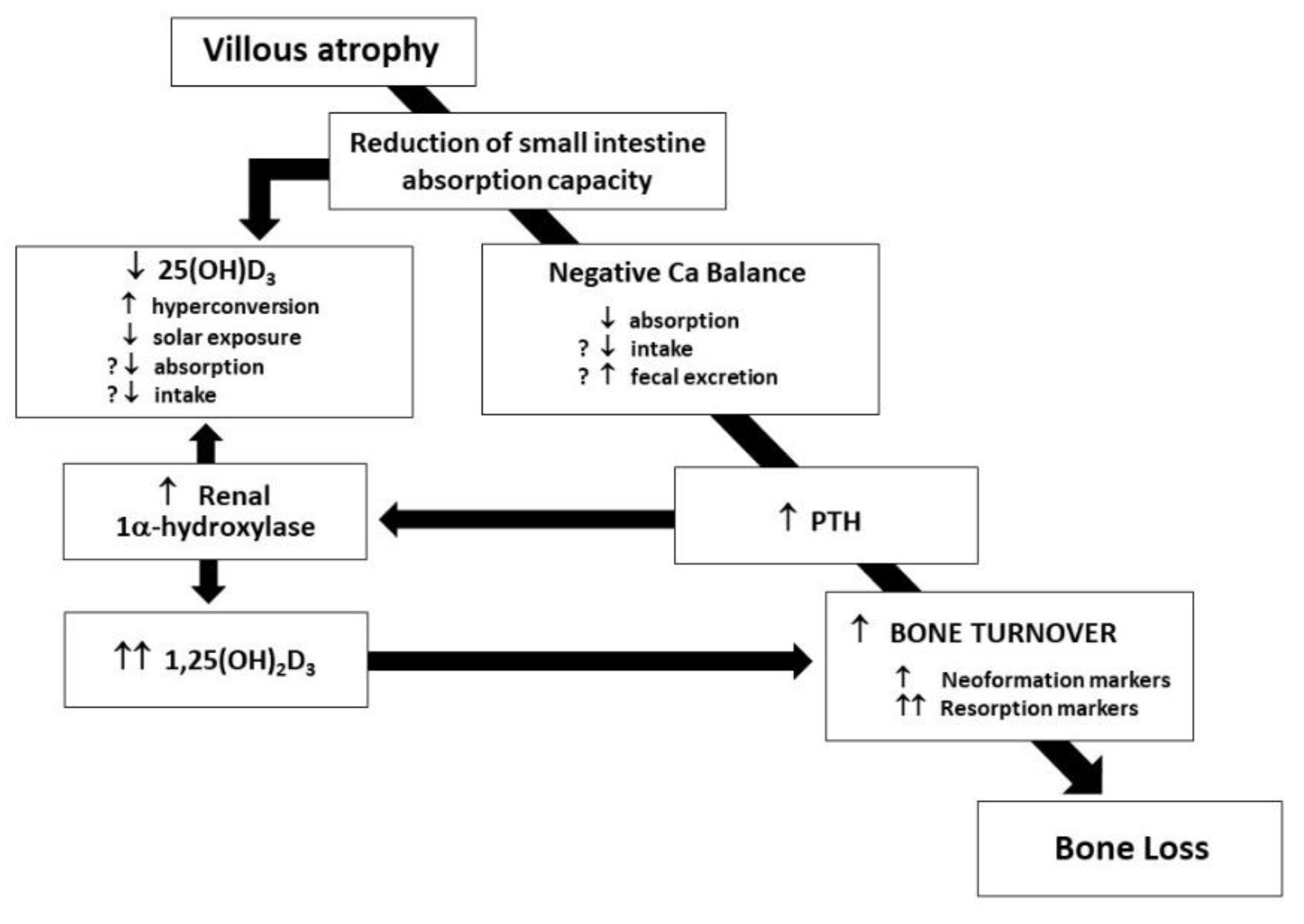
2. Bone and Mineral Metabolism in CD Patients at Diagnosis and after GFD
3. Awareness of the Persistence of Nutritional Deficiencies in CD Patients following GFD
4. When Is It Correct to Supplement Vitamin D in CD Patients?
4.1. Vitamin D Supplementation in Untreated CD Patients
4.2. Vitamin D Supplementation in Treated CD Patients
5. Conclusions
Funding
Conflicts of Interest
References
- Corazza, G.R.; Di Sabatino, A.; Di Sabatino, A.; Corazza, G.R. Coeliac disease. Lancet 2009, 373, 1480–1493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corazza, G.R.; Di Stefano, M.; Maurino, E.; Bai, J.C. Bone and coeliac disease: Diagnosis and treatment. Best Pract. Res. Clin. Gastroenterol. 2005, 19, 453–465. [Google Scholar] [CrossRef]
- Colston, K.W.; Mackay, A.G.; Finlayson, C.; Wu, J.C.J.; Maxwell, J.D. Localisation of vitamin D receptor in normal human duodenum and in patients with coeliac disease. Gut 1994, 35, 1219–1225. [Google Scholar] [CrossRef] [PubMed]
- Taranta, A.; Fortunati, D.; Longo, M.; Rucci, N.; Iacomino, E.; Aliberti, F.; Facciuto, E.; Migliaccio, S.; Bardella, M.T.; Dubini, A.; et al. Imbalance of osteoclastogenesis-regulating factors in patients with celiac disease. J. Bone Miner. Res. 2004, 19, 1112–1121. [Google Scholar] [CrossRef] [PubMed]
- Scott, E.M.; Gaywood, I.; Scott, B.B. Guidelines for osteoporosis in coeliac disease and inflammatory bowel disease. Gut 2000, 46 (Suppl. I), i1–i8. [Google Scholar] [CrossRef]
- American Gastroenterological Association Medical Position Statement: Guidelines on Osteoporosis in Gastrointestinal Diseases. Gastroenterology 2003, 124, 91–794.
- Di Stefano, M.; Mengoli, C.; Bergonzi, M.; Corazza, G.R. Bone mass and mineral metabolism alterations in adult celiac disease: Pathophysiology and clinical approach. Nutrients 2013, 5, 4786–4799. [Google Scholar] [CrossRef] [Green Version]
- Kanis, J.A.; Cooper, C.; Rizzoli, R.; Abrahamsen, B.; Al-Daghri, N.M.; Brandi, M.L.; Cannata-Andia, J.; Cortet, B.; Dimai, H.P.; Ferrari, S.; et al. European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Identification and management of patients at increased risk of osteoporotic fracture: Outcomes of an ESCEO expert consensus meeting. Osteoporos. Int. 2017, 28, 2023–2034. [Google Scholar] [CrossRef] [Green Version]
- Molteni, N.; Caraceni, M.P.; Bardella, M.T.; Ortolani, S.; Gandolini, G.G.; Bianchi, P.A. Bone mineral density in adult celiac patients and the effect of gluten-free diet from childhood. Am. J. Gastroenterol. 1990, 85, 51–53. [Google Scholar]
- Gerenli, N.; Dursun, F.; Celtik, C.; Kirmizibekmez, H. Significant improvement in bone mineral density in pediatric celiac disease: Even at six months with gluten-free diet. J. Ped. Endocrinol. Metab. 2021, 34, 341–348. [Google Scholar] [CrossRef]
- Corazza, G.R.; Di Sario, A.; Cecchetti, L.; Tarozzi, C.; Corrao, G.; Bernardi, M.; Gasbarrini, G. Bone mass and metabolism in patients with celiac disease. Gastroenterology 1995, 109, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Staun, M.; Jarnum, S. Measurement of the 10.000-molecular weight calcium-binding protein in small intestinal biopsy specimens from patients with malabsorption syndrome. Scand. J. Gastroenterol. 1988, 23, 827–832. [Google Scholar] [CrossRef] [PubMed]
- Maierhofer, W.J.; Gray, R.W.; Cheung, H.S.; Lemann, J., Jr. Bone resorption stimulated by elevated serum levels of 1,25-(OH)2-vitamin D concentrations in healthy men. Kidney Int. 1983, 24, 555–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molteni, N.; Bardella, M.T.; Vezzoli, G.; Pozzoli, E.; Bianchi, P. Intestinal calcium absorption as shown by stable strontium test in celiac disease before and after gluten-free diet. Am. J. Gastroenterol. 1995, 90, 2025–2028. [Google Scholar]
- Keaveny, A.P.; Freaney, R.; McKenna, M.J.; Masterson, J.; O’Donoghue, D.P. Bone remodeling indices and secondary hyperparathyroidism in celiac disease. Am. J. Gastroenterol. 1996, 91, 1226–1231. [Google Scholar]
- Corazza, G.R.; Di Sario, A.; Cecchetti, L.; Jorizzo, A.; Di Stefano, M.; Minguzzi, L.; Brusco, G.; Bernardi, M.; Gasbarrini, G. Influence of pattern of clinical presentation and of gluten-free diet on bone mass and metabolism in adult coeliac disease. Bone 1996, 18, 525–530. [Google Scholar] [CrossRef]
- Valdimarsson, T.; Toss, G.; Lofman, O.; Strom, M. Three years’ follow up of bone density in adult coeliac disease: Significance of secondary hyperparathyroidism. Scand. J. Gastroenterol. 2000, 35, 274–280. [Google Scholar] [CrossRef]
- Mautalen, C.; Gonzalez, D.; Mazure, R.; Vazquez, H.; Lorenzetti, M.P.; Maurino, E.; Niveloni, S.; Pedreira, S.; Smecuol, E.; Boerr, L.A.; et al. Effect of treatment on bone mass, mineral metabolism, and body composition in untreated celiac disease patients. Am. J. Gastroenterol. 1997, 92, 313–318. [Google Scholar]
- Stein, E.M.; Rogers, H.; Leib, A.; McMahon, D.J.; Young, P.; Nishijama, K.; Guo, X.E.; Lewis, S.; Green, P.; Shane, E. Abnormal skeletal strength and microarchitecture in women with celiac disease. J. Clin. Endocrinol. Metab. 2015, 100, 2347–2353. [Google Scholar] [CrossRef] [Green Version]
- Selby, P.L.; Davies, M.; Adams, J.E.; Mawer, E.B. Bone loss in celiac disease is related to secondary hyperparathyroidism. J. Bone Miner. Res. 1999, 14, 652–657. [Google Scholar] [CrossRef]
- Corazza, G.R.; Di Stefano, M.; Jorizzo, R.A.; Cecchetti, L.; Minguzzi, L.; Gasbarrini, G. Propeptyde of type I procollagen is predictive of post-treatment bone mass gain in adult celiac disease. Gastroenterology 1997, 113, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Di Stefano, M.; Bergonzi, M.; Benedetti, I.; De Amici, M.; Torre, C.; Brondino, N.; Miceli, E.; Pagani, E.; Marseglia, G.L.; Corazza, G.R.; et al. Alterations of inflammatory and matrix production indices in celiac disease with low bone mass on long-term gluten-free diet. J. Clin. Gastroenterol. 2019, 53, e221–e226. [Google Scholar] [CrossRef] [PubMed]
- Lemieux, B.; Boivin, M.; Brossard, J.H.; Lepage, R.; Picard, D.; Rousseau, L.; D’Amour, P. Normal parathyroid function with decreased bone minerl density in treated celiac disease. Can. J. Gastroenterol. 2001, 15, 302–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, M.; Mawer, E.B.; Krawitt, E.L. Comparative absorption of vitamin D3 and 25-hydroxyvitaminD3 in intestinal disease. Gut 1980, 21, 287–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batchelor, A.J.; Watson, G.; Compston, J.E. Changes in plasma half-life and clearance of 3H-25-hydroxyvitaminD3 in patients with intestinal malabsorption. Gut 1982, 23, 1068–1071. [Google Scholar] [CrossRef]
- Kempainnen, T.; Kroger, H.; Janatuinen, E.; Arnala, I.; Lamberg-Allardt, C.; Karkkainen, M. Bone recovery after a gluten-free diet: A 5-year follow-up study. Bone 1999, 25, 355–360. [Google Scholar] [CrossRef]
- Tavakkoli, A.; DiGiacomo, D.; Green, P.H.; Lebwohl, B. VitaminD status and concomitant autoimmunity in celiac disease. J. Clin. Gastroenterol. 2013, 47, 515–519. [Google Scholar] [CrossRef] [Green Version]
- Ciacci, C.; Bilancio, G.; Russo, I.; Iovino, P.; Cavallo, P.; Santonicola, A.; Bucci, C.; Cirillo, M.; Zingone, F. 25-hydroxyvitaminD, 1,25-dihydroxyvitaminD, and peripheral bone densitometry in adults with celiac disease. Nutrients 2020, 12, 929. [Google Scholar] [CrossRef] [Green Version]
- Sarela, S.; Thompson, D.V.; Nagrant, B.; Thakkar, P.; Clarke, K. A retrospective chart review evaluating the association of psychological disorders and vitamin D deficiency with celiac disease. Minerva Gastroenterol. Dietol. 2016, 62, 240–244. [Google Scholar]
- Marild, K.; Tapia, G.; Haugen, M.; Dahl, S.R.; Cohen, A.S.; Lundqvist, M.; Lie, B.A.; Stene, L.C.; Stordal, K. Matenal and neonatal vitamin D status, genotype and childhood celiac disease. PLoS ONE 2017, 12, e0179080. [Google Scholar] [CrossRef] [Green Version]
- San Pedro, J.I.; Bilbao, J.R.; Perez De Nunclares, G.; Vitoria, J.C.; Martul, P.; Castano, L. Heterogeneity of vitamin D receptor gene association with celiac disease and type I diabetes mellitus. Autoimmunity 2005, 38, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Vogelsang, H.; Suk, E.K.; Janisiw, M.; Stain, C.; Mayr, W.R.; Panzer, S. Calcaneal ultrasound attenuation and vitamin D receptor genotypes in celiac disease. Scand. J. Gastroenterol. 2000, 35, 172–176. [Google Scholar] [PubMed]
- Lu, C.; Zhou, W.; He, X.; Zhou, X.; Yu, C. Vitamin D status and vitamin D receptor genotypes in celiac disease: A meta-analysis. Crit. Rev. Food Sci. Nutr. 2021, 61, 2098–2106. [Google Scholar] [CrossRef] [PubMed]
- Di Nardo, G.; Villa, M.P.; Conti, L.; Ranucci, G.; Pacchiarotti, C.; Principessa, L.; Raucci, U.; Parisi, P. Nutritional deficiencies in children with celiac disease resulting from a gluten-free diet: A systematic review. Nutrients 2019, 11, 1588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jivraj, A.; Hutchinson, J.M.; Ching, E.; Marwaha, A.; Verdu, E.; Armstring, D.; Pinto-Sanchez, M.I. Micronutrient deficiencies are frequent in adult patients with and without celiac disease on a gluten-free diet, regardless of duration and adherence to the diet. Nutrition 2022, 103–104, 111809. [Google Scholar] [CrossRef] [PubMed]
- Cardo, A.; Churruca, I.; Lasa, A.; Navarro, V.; Vázquez-Polo, M.; Perez-Junkera, G.; Larretxi, I. Nutritional Imbalances in Adult Celiac Patients Following a Gluten-Free Diet. Nutrients 2021, 13, 2877. [Google Scholar] [CrossRef] [PubMed]
- Passali, M.; Josefsen, K.; Frederiksen, J.L.; Antvorskov, J.C. Current evidence on the efficacy of gluten-free diet in multiple sclerosis, psoriasis, type I diabetes and autoimmune thyroid disease. Nutrients 2020, 12, 23164. [Google Scholar] [CrossRef]
- Croall, I.D.; Trott, N.; Rej, A.; Aziz, I.; O’Brien, D.J.; George, H.A.; Hossain, M.Y.; Marks, L.J.S.; Richardson, J.I.; Rigby, R.; et al. A Population Survey of Dietary Attitudes towards Gluten. Nutrients 2019, 11, 1276. [Google Scholar] [CrossRef] [Green Version]
- Martin, J.; Geisel, T.; Maresch, C.; Krieger, K.; Stein, J. Inadequate nutrient intake in patients with celiac disease. Results from a German dietary survey. Digestion 2013, 87, 240e6. [Google Scholar] [CrossRef]
- Hallert, C.; Grant, C.; Grehn, S.; Granno, C.; Hulten, S.; Midhagen, G.; Strom, M.; Svensson, M.; Valdimarsson, T. Evidence of poor vitamin status in coeliac patients on a gluten free diet for 10 years. Aliment. Pharmacol. Ther. 2002, 16, 1333–1339. [Google Scholar] [CrossRef]
- Saturni, L.; Ferretti, G.; Bacchetti, T. The gluten-free diet: Safety and nutritional quality. Nutrients 2010, 2, 16–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vici, G.; Belli, L.; Biondi, M.; Polzonetti, V. Gluten free diet and nutrient deficiency: A review. Clin. Nutr. 2016, 35, 1236–1241. [Google Scholar] [CrossRef] [PubMed]
- Freeman, H.J. Iron deficiency anemia in celiac disease. World. J. Gastroenterol. 2015, 21, 9233–9238. [Google Scholar] [CrossRef] [PubMed]
- Tran, C.D.; Katsikeros, R.; Manton, N.; Krebs, N.F.; Hambridge, K.M.; Butler, R.N.; Davidson, G.P. Zinc homeostasis and gut function in children with celiac disease. Am. J. Clin. Nutr. 2011, 94, 1026–1032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dembrinski, L.; Mazur, A.; Dabrowski, M.; Jackowska, T. Knowledge of medical students and medical professionals regarding nutritional deficiencies in patients with celiac disease. Nutrients 2021, 13, 1771. [Google Scholar] [CrossRef] [PubMed]
- Gladys, K.; Dardzinska, J.; Guzek, M.; Adrych, K.; Kochen, Z.; Malgorzewicz, S. Expanded role of a dietitian in monitoring a gluten-free diet in patients with celiac disease: Implications for clinical practice. Nutrients 2021, 13, 1859. [Google Scholar] [CrossRef] [PubMed]
- Kupper, C. Dietary guidelines and implementation for celiac disease. Gastroenterology 2005, 128 (suppl. S1), S121–S127. [Google Scholar] [CrossRef]
- Schuchardt, J.P.; Hahn, A. Intestinal absorption and factors influencing bioavailability of magnesium. An update. Curr. Nutr. Food Sci. 2017, 13, 260–278. [Google Scholar] [CrossRef] [PubMed]
- Stasi, E.; Marafini, I.; Caruso, R.; Soderino, F.; Angelucci, E.; Del Vecchio Blanco, G.; Paoluzi, O.A.; Calabrese, E.; Sedda, S.; Zorzi, F.; et al. Frequency and cause of persistent symptoms in celiac disease patients on a long-term gluten-free diet. J. Clin. Gastroenterol. 2016, 50, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Giustina, A.; Adler, R.A.; Binkley, N.; Bollerslev, J.; Bouillon, R.; Dawson-Hughes, B.; Ebeling, P.R.; Feldman, D.; Formenti, A.M.; Lazzaretti-Castro, M.; et al. Consensus statements from 2nd International Conference on controversies in Vitamin D. Rev. Endocr. Metab. Dis. 2020, 21, 89–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, Z.; McKenzie, J.E.; McDonald, S.; Baram, L.; Page, M.J.; Allman-Farinelli, M.; Raubenheimer, D.; Bero, L.A. Assessment of the methods used to develop vitamin D and calcium recommendations. A systematic review of bone health guidelines. Nutrients 2021, 13, 2423. [Google Scholar] [CrossRef] [PubMed]
- Human Vitamin and Mineral Requirements Report of a Joint FAO/WHO Expert Consultation. Bangkok, Thailand. 2001. Available online: https://www.fao.org/3/y2809e/y2809e.pdf (accessed on 29 September 2022).
- Sempos, C.T.; Heijboer, A.C.; Bikle, D.; Bollerslev, J.; Bouillon, R.; Brannon, P.M.; DeLuca, H.F.; Jones, G.; Munns, C.F.; Bilezikian, J.P.; et al. Vitamin D assays and the definition of hypovitaminosis D: Results from the First International Conference on Controversies in Vitamin D. Br. J. Clin. Pharmacol. 2018, 84, 2194–2207. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R.; Marcocci, C.; Carmeliet, G.; Bikle, D.; White, J.H.; Dawson-Hughes, B.; Lips, P.; Munns, C.F.; Lazaretti-Castro, M.; Giustina, A.; et al. Skeletal and extraskeletal actions of vitamin D: Current evidence and outstanding questions. Endocr. Rev. 2019, 40, 1109–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Kostenberger, M.; Berisha, A.T.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D deficiency 2.0: An update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef] [PubMed]
- Elsenberg, E.H.A.M.; Ten Bockel, E.; Huijgen, H.; Heijboer, A.C. Standardization of automated 25-hydroxyvitamin D assays: How successful is it? Clin. Biochem. 2017, 50, 1126–1130. [Google Scholar] [CrossRef]
- Thomas, S.D.C.; Need, A.G.; Tucker, G.; Slobodian, P.O.; O’Loughlin, P.D.; Nordin, B.E.C. Suppression of parathyroid hormine and bone resorption by calcium carbonate and calcium citrate in postmenopausal women. Calcif. Tissue Int. 2008, 83, 81–84. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M.; Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guidelines. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: What clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef]
- Bouillon, R.; Muls, E.; De Moor, P. Influence of thyroid function on the serum concentration of 1,25-dihydroxyvitaminD3. J. Clin. Endocrinol. Metab. 1980, 51, 793–797. [Google Scholar] [CrossRef]
- Ballestrero-Fernandez, C.; Varela-Moreiras, G.; Ubeda, N.; Alonso-Aperte, E. Nutritional status in Spanish adults with celiac disease following a long-term gluten-free diet is similar to non-celiac. Nutrients 2021, 13, 1626. [Google Scholar] [CrossRef]
- Kim, D. The role of vitamin D in thyroid disease. Int. J. Mol. Sci. 2017, 18, 1949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moscogiuri, G.; Tirabassi, G.; Bizzarro, G.; Orio, F.; Paschou, S.; Vryonidou, A.; Balercia, G.; Shoenfeld, Y.; Colao, A. Vitamin D and thyroid disease: To D or not to D? Eur. J. Clin. Nutr. 2014, 69, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Lucas, R.M.; Gorman, S.; Gedenhuys, S.; Hart, P.H. Vitamin D and immunity. F1000 Prime. Rep. 2014, 6, 118. [Google Scholar] [CrossRef] [PubMed]
- Guillot, X.; Semerano, L.; Saidenberg-Kermanach, N.; Falgarone, G.; Boissier, M.C. Vitamin D and inflammation. Jt. Bone Spine 2010, 77, 552–557. [Google Scholar] [CrossRef]
- Vanoirbeek, E.; Krishnan, A.; Eelen, G.; Verlinden, L.; Bouillon, R.; Feldman, A.; Verstuyf, A. The anti-cancer and anti-inflammatory actions of 1,25(OH)2D3. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 593–604. [Google Scholar] [CrossRef] [Green Version]
- Krysiak, R.; Szkróbka, W.; Okopień, B. The Effect of Vitamin D on Thyroid Autoimmunity in Levothyroxine-Treated Women with Hashimoto’s Thyroiditis and Normal Vitamin D Status. Exp. Clin. Endocrinol. Diabetes. 2017, 125, 229–233. [Google Scholar] [CrossRef]
- O’Kane, M.; Mulhern, M.S.; Pourshahidi, L.K.; Strain, J.J.; Yeates, A.J. Micronutrients, iodine status and concentrations of thyroid hormones: A systematic review. Nutr. Rev. 2018, 76, 418–431. [Google Scholar] [CrossRef]
- Bell, N.H.; Stern, P.H.; Pantzer, E.; Sinha, T.K.; DeLuca, H.F. Evidence that increased circulating 1 alpha, 25-dihydroxyvitaminD is the probable cause for abnormal calcium metabolism in sarcoidosis. J. Clin. Investig. 1979, 64, 218–225. [Google Scholar] [CrossRef] [Green Version]
- Wijarnpreecha, K.; Panjawatanan, P.; Corral, J.E.; Lukens, F.J.; Ungprasert, P. Celiac disease and risk of sarcoidosis: A systematic review and meta-analysis. J. Evid. Based Med. 2019, 12, 194–199. [Google Scholar] [CrossRef]


{kind=link}
| Autoimmune Conditions | Vitamin D Status | Bone Loss |
|---|---|---|
| Hashimoto’s thyroiditis | deficiency | yes |
| Grave’s disease | deficiency | yes |
| Type 1 diabetes | deficiency | yes |
| Autoimmune liver diseases | deficiency | yes |
| Sjogren syndrome | deficiency | yes |
| Rheumatoid arthritis | deficiency | yes |
| Systemic lupus erithematosus | deficiency | yes |
| Sarcoidosis | deficiency | yes |
| Anti-phospholipid syndrome | deficiency | unknown |
| Williams–Beuren syndrome | unknown | yes |
| Addison’s disease | deficiency | yes |
| Autoimmune atrophic gastritis | deficiency | yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Stefano, M.; Miceli, E.; Mengoli, C.; Corazza, G.R.; Di Sabatino, A. The Effect of a Gluten-Free Diet on Vitamin D Metabolism in Celiac Disease: The State of the Art. Metabolites 2023, 13, 74. https://doi.org/10.3390/metabo13010074
Di Stefano M, Miceli E, Mengoli C, Corazza GR, Di Sabatino A. The Effect of a Gluten-Free Diet on Vitamin D Metabolism in Celiac Disease: The State of the Art. Metabolites. 2023; 13(1):74. https://doi.org/10.3390/metabo13010074
Chicago/Turabian StyleDi Stefano, Michele, Emanuela Miceli, Caterina Mengoli, Gino Roberto Corazza, and Antonio Di Sabatino. 2023. "The Effect of a Gluten-Free Diet on Vitamin D Metabolism in Celiac Disease: The State of the Art" Metabolites 13, no. 1: 74. https://doi.org/10.3390/metabo13010074