

Body Mass Index and Caries: Machine Learning and Statistical Analytics of the Dental, Oral, Medical Epidemiological (DOME) Nationwide Big Data Study
 ,
, 
Abstract
:1. Introduction
- To explore the associations of decayed teeth as a dependent variable with different BMI categories in various statistical models adjusted for potential confounding factors, such as (1) socio-demographic variables: age, sex, educational level, socio-economic status (SES), residency, and country of birth; and (2) health-related habits: smoking, teeth brushing, cariogenic nutrition, and sugary drinks as well as other diseases comprising the Metabolic Syndrome (MetS) including, hypertension, diabetes, hyperlipidemia, cardiovascular disease, nonalcoholic Fatty Liver Disease (NAFLD), and obstructive sleep apnea (OSA).
- To employ supervised machine learning (ML) algorithms that will explore the relative clinical features importance for two targets: (a) the dichotomous variable of decayed teeth and (b) obesity (BMI ≥ 30 kg/m2), while using the same set of clinical features that were used in the statistical models.
- To compare the results obtained by the statistical and ML models and discuss and summarize the conclusions.
2. Methods
2.1. Data Source
2.2. Ethical Approval
2.3. Data Collection
2.4. Eligibility Criteria
2.5. Definition of Variables
2.6. Data Analysis
2.6.1. Statistical Analysis
2.6.2. Sub-Section Clinical Features Importance Based on Machine Learning Algorithms
3. Results
3.1. Socio-Demographics across BMI Categories

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | BMI Categories | Total (%) or Mean ± SD | p Value | ||||
| Underweight | Normal Weight | Overweight | Obesity | ||||
| Number (%) | 3113 (4.7) | 38,924 (59.2) | 16,966 (25.8) | 6736 (10.2) | 65,739 (100) | ||
| Age (years) | 19.9 ± 3.2 | 21.5 ± 5.7 | 25.2 ± 8.5 | 26.4 ± 9.0 | 22.8 ± 7.1 | <0.001 * | |
| Sex | Men | 1556 (50.0) | 28,397 (73.0) | 14,113 (83.2) | 5342 (79.3) | 49,408 (75.2) | <0.001 ˅ |
| Woman | 1557 (50.0) | 10,527 (27.0) | 2853 (16.8) | 1394 (20.7) | 16,331 (24.8) | ||
| Education | High school | 2910 (93.7) | 33,064 (85.1) | 11,716 (69.1) | 4417 (65.7) | 52,107 (79.4) | <0.001 ˅ |
| Technician | 75 (2.4) | 1865 (4.8) | 1940 (11.4) | 1038 (15.4) | 4918 (7.5) | ||
| Academics | 120 (3.9) | 3937 (10.1) | 3289 (19.4) | 1272 (18.9) | 8618 (13.1) | ||
| SES | Low | 128 (4.1) | 1642 (4.3) | 951 (5.7) | 4141 (6.3) | 3135 (4.8) | <0.001 ˅ |
| Medium | 1654 (53.5) | 19,419 (50.5) | 9071 (54.5) | 3917 (59.2) | 34,061 (52.6) | ||
| High | 1307 (42.3) | 17,364 (45.2) | 6636 (39.8) | 2288 (34.6) | 27,595 (42.6) | ||
| Locality of residence | Urban Jewish | 2828 (91.2) | 33,151 (85.6) | 14,276 (84.7) | 5831 (87.1) | 56,086 (85.8) | <0.001 ˅ |
| Urban non-Jewish | 267 (8.6) | 5369 (13.9) | 2401 (14.2) | 792 (11.8) | 8829 (13.5) | ||
| Rural | 5 (0.2) | 196 (0.5) | 181 (1.1) | 75 (1.1) | 557 (0.7) | ||
| Birth Country | Western Europe | 38 (1.2) | 896 (2.3) | 526 (3.1) | 223 (3.3) | 1683 (2.6) | <0.001 ˅ |
| Eastern Europe | 238 (7.7) | 2196 (5.6) | 982 (5.8) | 412 (6.1) | 3828 (5.8) | ||
| FSU | 42 (1.4) | 450 (1.2) | 207 (1.2) | 102 (1.5) | 801 (1.2) | ||
| Asia | 3 (0.1) | 73 (0.2) | 64 (0.4) | 23 (0.3) | 163 (0.2) | ||
| East Asia | 5 (0.2) | 57 (0.1) | 25 (0.1) | 7 (0.1) | 94 (0.1) | ||
| Ethiopia | 129 (4.1) | 832 (2.1) | 152 (0.9) | 22 (0.3) | 1135 (1.7) | ||
| Africa | 5 (0.2) | 99 (0.3) | 75 (0.4) | 29 (0.4) | 208 (0.3) | ||
| North America | 39 (1.3) | 995 (2.6) | 441 (2.6) | 112 (1.7) | 1587 (2.4) | ||
| South America | 8 (0.3) | 298 (0.8) | 168 (1.0) | 60 (0.9) | 534 (0.8) | ||
| Oceania | 1 (0.0) | 47 (0.1) | 14 (0.1) | 3 (0.0) | 65 (0.1) | ||
| Israel | 2603 (83.7) | 32,974 (84.7) | 14,306 (84.4) | 5741 (85.3) | 55,624 (84.6) | ||
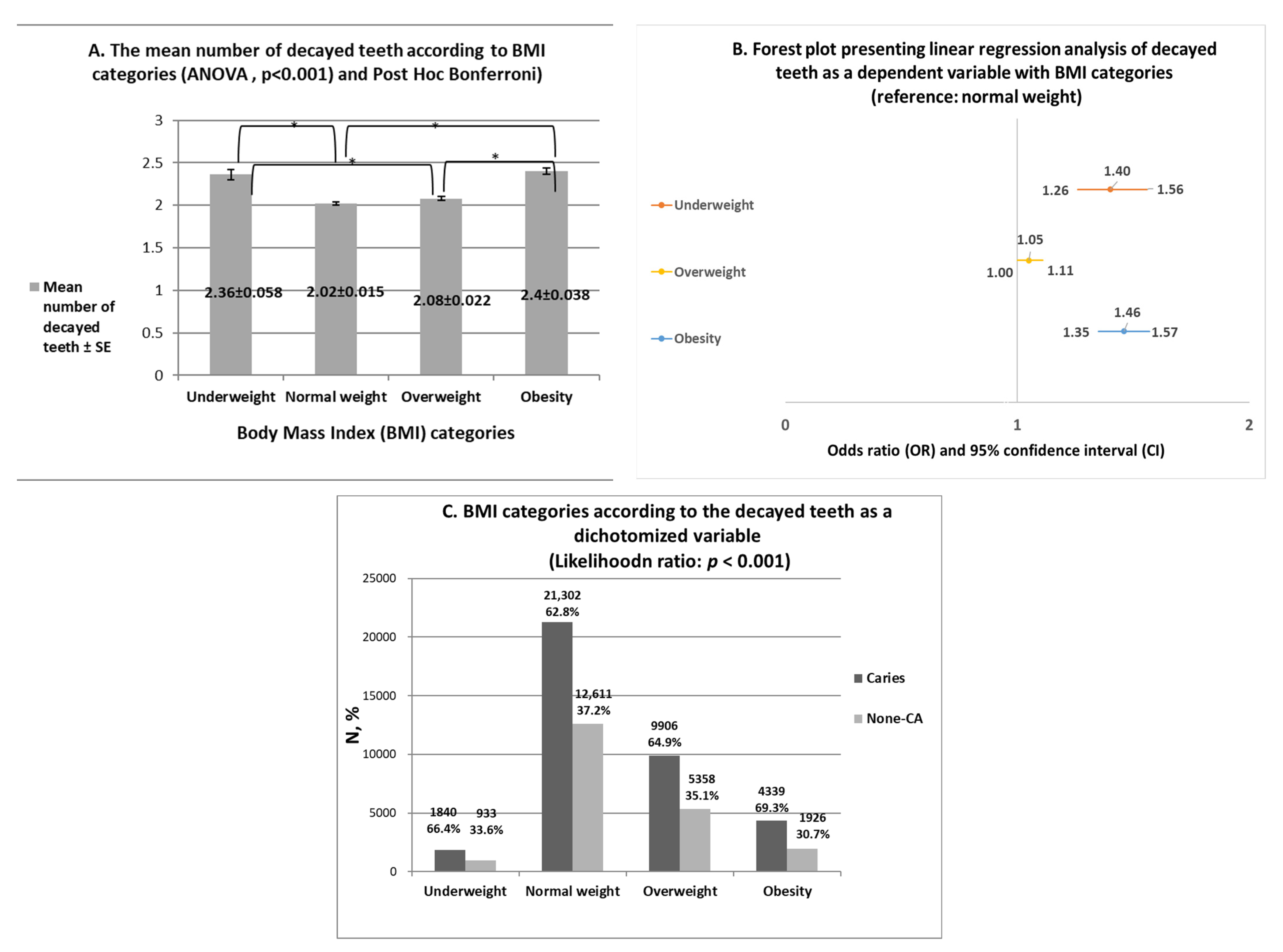
3.2. Mean Number of Decayed Teeth across BMI Categories
3.3. Health-Related Practices and Medical Diagnoses Related to Metabolic Syndrome (MetS) across BMI Categories
| Parameter | BMI Categories | Total (%) or Mean ± SD | p Value | ||||
| Underweight | Normal Weight | Overweight | Obesity | ||||
| Number (%) | 3113 (4.7) | 38,924 (59.2) | 16,966 (25.8) | 6736 (10.2) | 66,790 (100) | ||
| Smoking | No | 3033 (97.4) | 37,210 (95.6) | 14,854 (87.6) | 5541 (82.3) | 60,638 (92.2) | <0.001 ˅ |
| Yes | 80 (2.6) | 1714 (4.4) | 2112 (12.4) | 1195 (17.7) | 5101 (7.8) | ||
| Brushing teeth at least once a day | No | 108 (10.2) | 1262 (10.6) | 607 (12.2) | 359 (17.7) | 2336 (11.7) | <0.001 ˅ |
| Yes | 946 (89.8) | 10,700 (89.4) | 4365 (87.8) | 1167 (82.3) | 17,678 (88.3) | ||
| Consumption of cariogenic nutrition | No | 440 (41. 8) | 5879 (49.2) | 2602 (52.4) | 1016 (50.3) | 9937 (49.7) | <0.001 ˅ |
| Yes | 613 (58.2) | 6074 (50.8) | 2366 (47.6) | 1004 (49.7) | 10,057 (50.3) | ||
| Consumption of sugary drinks | No | 452 (43.0) | 5509 (46.1) | 2346 (47.3) | 887 (43.9) | 9194 (46.0) | 0.014 ˅ |
| Yes | 598 (57.0) | 6429 (53.9) | 2167 (52.7) | 1133 (56.1) | 10,777 (54.0) | ||
| Hypertension | No | 3090 (99.3) | 38,283 (98.4) | 16,034 (94.5) | 5813 (86.3) | 63,220 (96.2) | <0.001 ˅ |
| Yes | 23 (0.7) | 641 (1.6) | 932 (5.5) | 923 (13.7) | 2519 (3.8) | ||
| Diabetes | No | 3111 (99.9) | 38,865 (99.8) | 16,854 (99.3) | 6614 (98.2) | 65,444 (99.6) | <0.001 ˅ |
| Yes | 2 (0.1) | 59 (0.2) | 112 (0.7) | 122 (1.8) | 295 (0.4) | ||
| Hyperlipidemia | No | 3110 (99.9) | 38,704 (99.4) | 16,614 (97.9) | 6555 (97.3) | 64,983 (98.8) | <0.001 ˅ |
| Yes | 3 (0.1) | 220 (0.6) | 352 (2.1) | 181 (2.7) | 756 (1.2) | ||
| Non-alcoholic fatty liver disease (NAFLD) | No | 3112 (100) | 38,837 (9.8) | 16,657 (98.2) | 6338 (94.1) | 64,944 (98.8) | <0.001 ˅ |
| Yes | 0 (0) | 87 (0.2) | 309 (1.8) | 398 (5.9) | 795 (1.2) | ||
| Obstructive sleep apnea (OSA) | No | 3113 (100) | 38,878 (99.9) | 16,867 (99.4) | 6638 (98.5) | 65,496 (99.6) | <0.001 ˅ |
| Yes | 0 (0) | 46 (0.1) | 99 (0.6) | 98 (1.5) | 243 (0.4) | ||
| Cardiovascular disease | No | 3038 (97.6) | 37,919 (97.4) | 16,162 (95.3) | 6297 (93.5) | 63,416 (96.5) | <0.001 ˅ |
| Yes | 75 (2.4) | 1005 (2.6) | 804 (4.7) | 439 (6.5) | 2323 (3.5) | ||
3.4. Carious Teeth According to BMI Categories in Different Multivariate Analyses Models
3.5. Clinical Features Importance Based on Machine Learning Algorithms
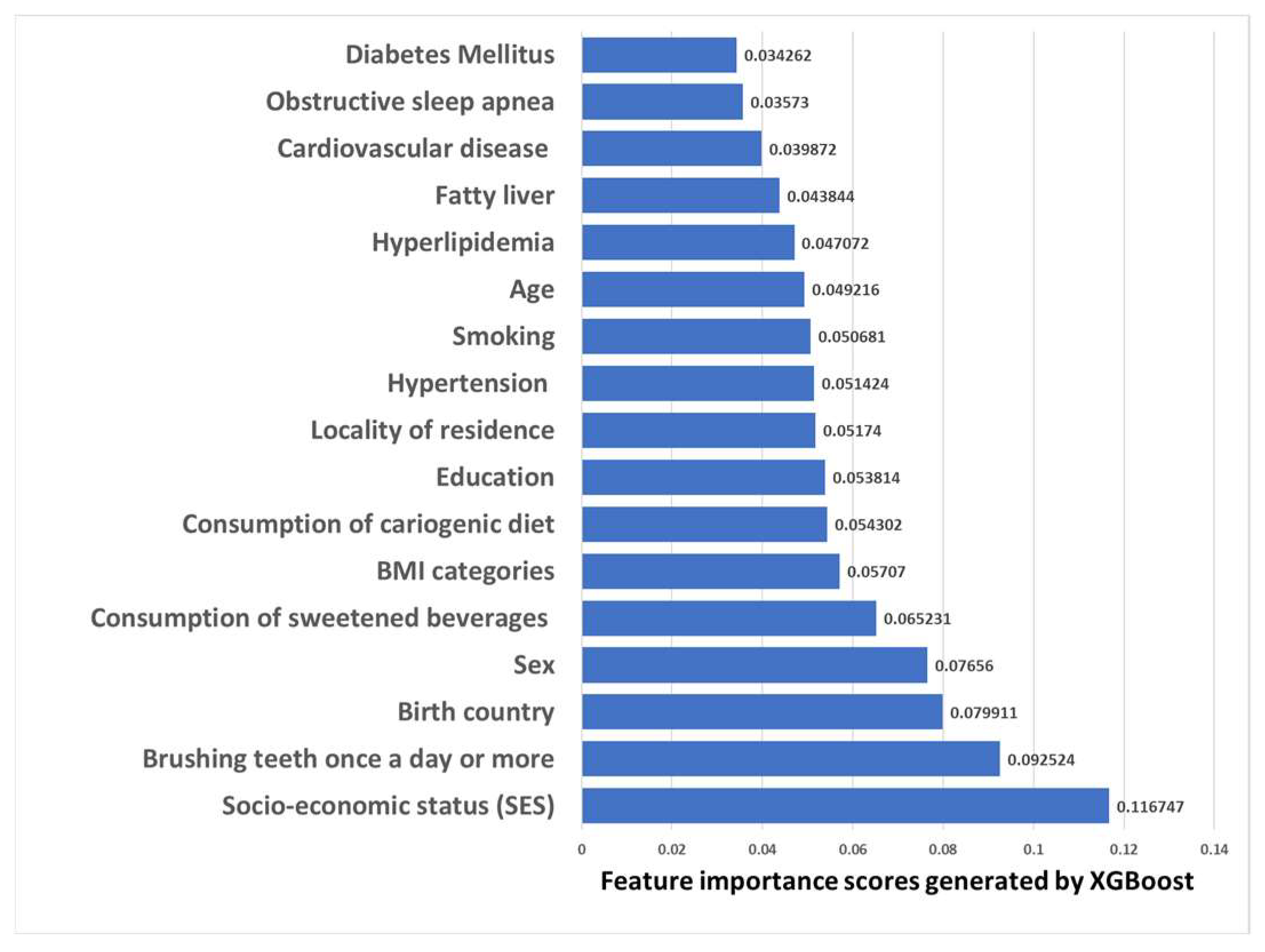
3.5.1. Clinical Features Importance Based on XGBoost Machine Learning Model with the Dichotomous Target Variable of Decayed Teeth
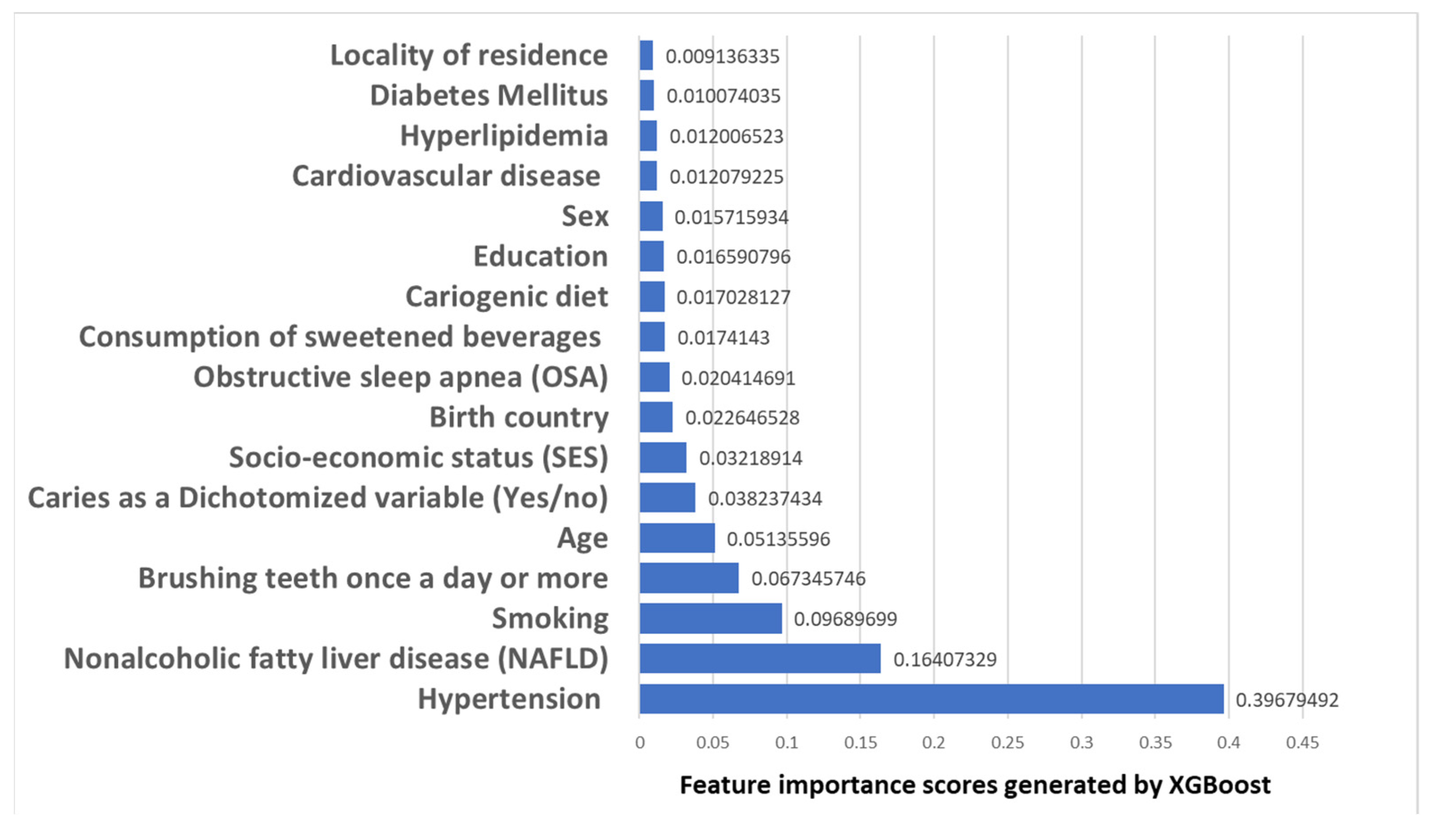
3.5.2. Clinical Features Importance Based on XGBoost Machine Learning Model with Obesity Set as a Target Variable
4. Discussion
Strength and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gallagher, D.; Visser, M.; Sepulveda, D.; Pierson, R.N.; Harris, T.; Heymsfield, S.B. How useful is body mass index for comparison of body fatness across age, sex, and ethnic groups? Am. J. Epidemiol. 1996, 143, 228–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mei, Z.; Grummer-Strawn, L.M.; Pietrobelli, A.; Goulding, A.; Goran, M.I.; Dietz, W.H. Validity of body mass index compared with other body-composition screening indexes for the assessment of body fatness in children and adolescents. Am. J. Clin. Nutr. 2002, 75, 978–985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khanna, D.; Rehman, A. Pathophysiology of Obesity. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Global, B.M.I.M.C.; Di Angelantonio, E.; Bhupathiraju Sh, N.; Wormser, D.; Gao, P.; Kaptoge, S.; Berrington de Gonzalez, A.; Cairns, B.J.; Huxley, R.; Jackson Ch, L.; et al. Body-mass index and all-cause mortality: Individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet 2016, 388, 776–786. [Google Scholar]
- Kassebaum, N.J.; Bernabe, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of untreated caries: A systematic review and metaregression. J. Dent. Res. 2015, 94, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Qin, X.; Zi, H.; Zeng, X. Changes in the global burden of untreated dental caries from 1990 to 2019: A systematic analysis for the Global Burden of Disease study. Heliyon 2022, 8, e10714. [Google Scholar] [CrossRef]
- Paisi, M.; Kay, E.; Bennett, C.; Kaimi, I.; Witton, R.; Nelder, R.; Lapthorne, D. Body mass index and dental caries in young people: A systematic review. BMC Pediatr 2019, 19, 122. [Google Scholar] [CrossRef] [PubMed]
- Gudipaneni, R.K.; Albilasi, R.M.; HadiAlrewili, O.; Alam, M.K.; Patil, S.R.; Saeed, F. Association of Body Mass Index and Waist Circumference With Dental Caries and Consequences of Untreated Dental Caries Among 12- to 14-Year-old Boys: A Cross-Sectional Study. Int. Dent. J. 2021, 71, 522–529. [Google Scholar] [CrossRef]
- Abdellatif, H.; Hebbal, M.I. Dental Caries and Its Association with Body Mass Index among School Children of Riyadh, Saudi Arabia. J. Pharm. Bioallied Sci. 2020, 12 (Suppl. S1), S176–S181. [Google Scholar]
- Alshehri, Y.F.A.; Park, J.S.; Kruger, E.; Tennant, M. Association between body mass index and dental caries in the Kingdom of Saudi Arabia: Systematic review. Saudi Dent. J. 2020, 32, 171–180. [Google Scholar] [CrossRef]
- Alswat, K.; Mohamed, W.S.; Wahab, M.A.; Aboelil, A.A. The Association Between Body Mass Index and Dental Caries: Cross-Sectional Study. J. Clin. Med. Res. 2016, 8, 147–152. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.; Han, K.; Yang, S. Association between overweight, obesity and incidence of advanced dental caries in South Korean adults: A 10-year nationwide population-based observational study. PLoS One 2020, 15, e0229572. [Google Scholar] [CrossRef] [PubMed]
- Alkarimi, H.A.; Watt, R.G.; Pikhart, H.; Sheiham, A.; Tsakos, G. Dental caries and growth in school-age children. Pediatrics 2014, 133, e616–e623. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Zhang, Y.; Yuan, X.; Yu, J.; Chen, S.; Chen, Z.; Guo, D.; Cai, J.; Ma, N.; Guo, E. Caries experience and its association with weight status among 8-year-old children in Qingdao, China. J. Int. Soc. Prev. Community Dent. 2015, 5, 52–58. [Google Scholar] [PubMed] [Green Version]
- Peng, S.M.; Wong, H.M.; King, N.M.; McGrath, C. Is dental caries experience associated with adiposity status in preschool children? Int. J. Paediatr. Dent. 2014, 24, 122–130. [Google Scholar] [CrossRef]
- Sheiham, A.; Watt, R.G. The common risk factor approach: A rational basis for promoting oral health. Community Dent. Oral Epidemiol 2000, 28, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Sara, A.R.; Raslan, M.; Shehata, E.M.; Sabri, N.A. Eslam M Shehata Nagwa A Sabri, impact of Applied Protective Measures of COVID-19 on Public Health. Acta Sci. Pharm. Sci. 2021, 5, 63–72. [Google Scholar]
- Nagib, M.M.; Tadros, M.G.; Al-Khalek, H.A.A.; Rahmo, R.M.; Sabri, N.A.; Khalifa, A.E.; Masoud, S.I. Molecular mechanisms of neuroprotective effect of adjuvant therapy with phenytoin in pentylenetetrazole-induced seizures: Impact on Sirt1/NRF2 signaling pathways. Neurotoxicology 2018, 68, 47–65. [Google Scholar] [CrossRef] [PubMed]
- Elsayed, A.A.; Menze, E.T.; Tadros, M.G.; Ibrahim, B.M.M.; Sabri, N.A.; Khalifa, A.E. Effects of genistein on pentylenetetrazole-induced behavioral and neurochemical deficits in ovariectomized rats. Naunyn Schmiedebergs Arch. Pharm. 2018, 391, 27–36. [Google Scholar] [CrossRef]
- Amany Talaat Elgarf, M.M.M. Nagwa Ali Sabri, Effect of Silymarin Supplementation on Glycemic Control, Lipid Profile and Insulin Resistance in Patients with Type 2 Diabetes Mellitus. Int. J. Adv. Res. 2015, 3, 812–821. [Google Scholar]
- Rizk, S.M.; Sabri, N.A. Evaluation of clinical activity and safety of Daflon 500 mg in type 2 diabetic female patients. Saudi Pharm. J. 2009, 17, 199–207. [Google Scholar] [CrossRef] [Green Version]
- Abou El-Fadl, D.K.; Sabri, N.A.; Abuel-Ela, H.A. A Clinical Study on The Impact of Different Treatment Modalities on Improving The Clinical Outcomes in Chronic Periodontitis Patients. IJPSR 2015, 6, 4198–4209. [Google Scholar]
- Mathew, H.; Farr, O.M.; Mantzoros, C.S. Metabolic health and weight: Understanding metabolically unhealthy normal weight or metabolically healthy obese patients. Metabolism 2016, 65, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Kramer, C.K.; Zinman, B.; Retnakaran, R. Are metabolically healthy overweight and obesity benign conditions? A systematic review and meta-analysis. Ann. Intern. Med. 2013, 159, 758–769. [Google Scholar] [CrossRef] [PubMed]
- Hung, M.; Voss, M.W.; Rosales, M.N.; Li, W.; Su, W.; Xu, J.; Bounsanga, J.; Ruiz-Negron, B.; Lauren, E.; Licari, F.W. Application of machine learning for diagnostic prediction of root caries. Gerodontology 2019, 36, 395–404. [Google Scholar] [CrossRef]
- Park, Y.H.; Kim, S.H.; Choi, Y.Y. Prediction Models of Early Childhood Caries Based on Machine Learning Algorithms. Int. J. Environ. Res. Public Health 2021, 18, 8613. [Google Scholar] [CrossRef] [PubMed]
- Almoznino, G.; Kedem, R.; Turgeman, R.; Bader, T.; Yavnai, N.; Zur, D.; Shay, B. The Dental, Oral, Medical Epidemiological (DOME) Study: Protocol and Study Methods. Methods Inf. Med. 2020, 59, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Almoznino, G.; Zini, A.; Kedem, R.; Protter, N.E.; Zur, D.; Abramovitz, I. Hypertension and Its Associations with Dental Status: Data from the Dental, Oral, Medical Epidemiological (DOME) Nationwide Records-Based Study. J. Clin. Med. 2021, 10, 176. [Google Scholar] [CrossRef]
- Abramovitz, I.; Zini, A.; Atzmoni, M.; Kedem, R.; Zur, D.; Protter, N.E.; Almoznino, G. Cognitive Performance and Its Associations with Dental Caries: Results from the Dental, Oral, Medical Epidemiological (DOME) Records-Based Nationwide Study. Biology 2021, 10, 178. [Google Scholar] [CrossRef]
- Abramovitz, I.; Zini, A.; Kessler Baruch, O.; Kedem, R.; Protter, N.E.; Shay, B.; Yavnai, N.; Zur, D.; Mijiritsky, E.; Almoznino, G. SOS teeth with advanced caries and sociodemographic indicators, health-related habits and dental attendance patterns: Data from the Dental, Oral, Medical Epidemiological (DOME) nationwide records-based study. BMC Oral Health 2021, 21, 389. [Google Scholar] [CrossRef]
- Abramovitz, I.; Zini, A.; Pribluda, P.; Kedem, R.; Zur, D.; Protter, N.E.; Almoznino, G. “Dental Cluster” Versus “Metabolic Cluster”: Analyzing the Associations of Planned and Delivered Dental Procedures with Metabolic Syndrome, Utilizing Data from the Dental, Oral, Medical Epidemiological (DOME) Cross-Sectional Record-Based Nationwide Study. Biology 2021, 10, 608. [Google Scholar] [CrossRef]
- Israel Defence Forces (IDF). The Stges of Volunteering in the IDF. Available online: https://www.mitgaisim.idf.il/%D7%9B%D7%AA%D7%91%D7%95%D7%AA/english/exclusive-service/the-stages-of-volunteering-in-the-idf/#/ (accessed on 30 November 2022).
- Simchoni, M.; Hamiel, U.; Pinhas-Hamiel, O.; Zucker, I.; Cukierman-Yaffe, T.; Lutski, M.; Derazne, E.; Beer, Z.; Behar, D.; Keinan-Boker, L.; et al. Adolescent BMI and early-onset type 2 diabetes among Ethiopian immigrants and their descendants: A nationwide study. Cardiovasc. Diabetol 2020, 19, 168. [Google Scholar] [CrossRef] [PubMed]
- Weir, C.B.; Jan, A. BMI Classification Percentile And Cut Off Points. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Jh, F. Greedy function approximation: A gradient boosting machine. Ann. Statist. 2001, 29, 1189–1232. [Google Scholar]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-Learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Liu, H.; Zhou, M.; Lu, X.S.; Yao, C. Weighted Gini index feature selection method for imbalanced data. In Proceedings of the ICNSC 2018—15th IEEE International Conference on Networking, Sensing and Control, Zhuhai, China, 27–29 March 2018; Institute of Electrical and Electronics Engineers Inc.: Zhuhai, China, 2018; pp. 1–6. [Google Scholar]
- Huang, N.; Lu, G.; Cai, G.; Xu, D.; Xu, J.; Li, F.; Zhang, L. Feature selection of power quality disturbance signals with an entropy-importance-based random forest. Entropy 2016, 18, 44. [Google Scholar] [CrossRef] [Green Version]
- Newton, S.; Braithwaite, D.; Akinyemiju, T.F. Socio-economic status over the life course and obesity: Systematic review and meta-analysis. PLoS One 2017, 12, e0177151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Cheng, L.; Yuan, B.; Hong, X.; Hu, T. Association between socio-economic status and dental caries in elderly people in Sichuan Province, China: A cross-sectional study. BMJ Open 2017, 7, e016557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLaren, L. Socioeconomic status and obesity. Epidemiol Rev. 2007, 29, 29–48. [Google Scholar] [CrossRef] [PubMed]
- Moynihan, P.J.; Kelly, S.A. Effect on caries of restricting sugars intake: Systematic review to inform WHO guidelines. J. Dent. Res. 2014, 93, 8–18. [Google Scholar] [CrossRef] [Green Version]
- Chiolero, A.; Wietlisbach, V.; Ruffieux, C.; Paccaud, F.; Cornuz, J. Clustering of risk behaviors with cigarette consumption: A population-based survey. Prev. Med. 2006, 42, 348–353. [Google Scholar] [CrossRef]




| Variable | BMI Categories | |||
|---|---|---|---|---|
| Normal Weight | Underweight | Overweight | Obesity | |
| 1st Model without adjustment: carious teeth across BMI categories | ||||
| OR and 95%CI | 1 | 1.40 (1.26–1.56) | 1.05 (1.00–1.11) | 1.46 (1.35–1.57) |
| 2nd Model: 1st Model adjusted for age | ||||
| OR and 95%CI | 1 | 1.33 (1.19–1.48) | 1.19 (1.12–1.26) | 1.70 (1.58–1.84) |
| 3rd Model: 2nd model parameters with sex | ||||
| OR and 95%CI | 1 | 1.42 (1.27–1.58) | 1.16 (1.09–1.22) | 1.68 (1.56–1.82) |
| 4th Model: 3rd model parameters with educational level | ||||
| OR and 95%CI | 1 | 1.39 (1.24–1.55) | 1.15 (1.09–1.21) | 1.63 (1.50–1.76) |
| 5th Model: 4th model parameters with socio-economic status (SES) | ||||
| OR and 95%CI | 1 | 1.35 (1.21–1.50) | 1.10 (1.05–1.17) | 1.53 (1.41–1.65) |
| 6th model: 5th model 5 parameters with residence location | ||||
| OR and 95%CI | 1 | 1.32 (1.18–1.47) | 1.11 (1.05–1.17) | 1.51 (1.40–1.64) |
| 7th model: 6th model parameters with birth countries | ||||
| OR and 95%CI | 1 | 1.29 (1.16–1.44) | 1.11 (1.05–1.17) | 1.51 (1.40–1.64) |
| 8th model: 7th model parameters with hypertension | ||||
| OR and 95%CI | 1 | 1.29 (1.16–1.44) | 1.11 (1.05–1.17) | 1.51 (1.39–1.63) |
| 9th model: 8th model parameters with diabetes mellitus | ||||
| OR and 95%CI | 1 | 1.29 (1.16–1.44) | 1.11 (1.05–1.17) | 1.51 (1.39–1.63) |
| 10th model: 9th model parameters with hyperlipidemia | ||||
| OR and 95%CI | 1 | 1.29 (1.16–1.44) | 1.11 (1.05–1.17) | 1.51 (1.39–1.63) |
| 11th model: 10th model parameters with nonalcoholic Fatty Liver Disease (NAFLD) | ||||
| OR and 95%CI | 1 | 1.29 (1.16–1.45) | 1.11 (1.05–1.17) | 1.51 (1.40–1.64) |
| 12th model: 11th model with Obstructive Sleep Apnea (OSA) | ||||
| OR and 95%CI | 1 | 1.30 (1.16–1.45) | 1.11 (1.05–1.17) | 1.52 (1.40–1.64) |
| 13th model: 12th model with cardiovascular disease | ||||
| OR and 95%CI | 1 | 1.30 (1.16–1.45) | 1.11 (1.05–1.17) | 1.52 (1.40–1.64) |
| 14th model: 13th model parameters with smoking | ||||
| OR and 95%CI | 1 | 1.30 (1.16–1.45) | 1.11 (1.05–1.17) | 1.50 (1.39–1.63) |
| 15th model: 14th model parameters and tooth brushing | ||||
| OR and 95%CI | 1 | 1.30 (1.16–1.45) | 1.11 (1.05–1.17) | 1.50 (1.39–1.63) |
| 16th model: 15th model parameters with cariogenic nutrition and sugary drinks | ||||
| OR and 95%CI | 1 | 1.18 (1.004–1.39) | 1.04 (0.96–1.13) | 1.56 (1.39–1.76) |
| Parameter | B | Standard Error | p Value | Exp(B) and 95% Confidence Interval for Exp(B) | Collinearity Statistics | |
|---|---|---|---|---|---|---|
| Tolerance | VIF | |||||
| (Intercept) | 3.78 | 0.14 | <0.001 | 44.06 (33.08–58.69) | ||
| Underweight vs. normal weight | 0.16 | 0.08 | 0.045 | 1.18 (1.004–1.39) | 0.838 | 1.193 |
| Overweight vs. normal weight | 0.04 | 0.04 | 0.309 | 1.04 (0.96–1.13) | 0.858 | 1.165 |
| Obesity vs. normal weight | 0.45 | 0.06 | <0.001 | 1.56 (1.39–1.76) | 0.951 | 1.051 |
| Age | −0.01 | 0.004 | 0.005 | 0.989 (0.981–0.997) | 0.288 | 3.467 |
| Sex: Men vs. women | 0.15 | 0.04 | <0.001 | 1.16 (1.07–1.26) | 0.922 | 1.084 |
| Educational level: technicians vs. high school | −0.62 | 0.08 | <0.001 | 0.54 (0.46–0.63) | 0.564 | 1.774 |
| Educational level: academic vs. high school | −0.50 | 0.07 | <0.001 | 0.60 (0.52–0.70) | 0.441 | 2.269 |
| SES: medium vs. low | −1.03 | 0.08 | <0.001 | 0.35 (0.30–0.41) | 0.946 | 1.057 |
| SES: high vs. low | −1.53 | 0.08 | <0.001 | 0.21 (0.18–0.25) | 0.937 | 1.068 |
| Residence location: Urban Jewish vs. Urban non-Jewish | 0.34 | 0.05 | <0.001 | 1.41 (1.27–1.57) | 0.981 | 1.020 |
| Residence location: Rural vs. Urban non-Jewish | 1.04 | 0.32 | 0.001 | 2.82 (1.49–5.33) | 0.985 | 1.015 |
| Birth countries Western Europe vs. Israeli | 0.41 | 0.06 | <0.001 | 1.51 (1.33–1.70) | 0.983 | 1.017 |
| Birth countries Eastern Europe vs. Israeli | 1.20 | 0.14 | <0.001 | 3.33 (2.49–4.45) | 0.980 | 1.021 |
| Birth countries Asia vs. Israeli | 0.03 | 0.25 | 0.890 | 1.03 (0.63–1.69) | 0.995 | 1.005 |
| Birth countries Ethiopia vs. Israeli | 0.26 | 0.13 | 0.052 | 1.30 ().98–1.69) | 0.986 | 1.015 |
| Birth countries Africa vs. Israeli | 0.02 | 0.31 | 0.943 | 1.02 (0.55–1.88) | 0.986 | 1.015 |
| Birth Countries North America vs. Israeli | −0.63 | 0.13 | <0.001 | 0.53 (0.40–0.69) | 0.991 | 1.010 |
| Birth countries South America vs. Israeli | −0.25 | 0.19 | 0.202 | 0.77 (0.52–1.14) | 0.997 | 1.003 |
| Hypertension | 0.08 | 0.08 | 0.362 | 1.08 (0.91–1.29) | 0.894 | 1.118 |
| Diabetes Mellitus | 0.22 | 0.22 | 0.310 | 1.25 (0.81–1.93) | 0.946 | 1.057 |
| Hyperlipidemia | −0.14 | 0.14 | 0.340 | 0.86 (0.65–1.16) | 0.957 | 1.045 |
| Nonalcoholic Fatty Liver Disease (NAFLD) | −0.11 | 0.13 | 0.412 | 0.89 (0.67–1.17) | 0.907 | 1.103 |
| Obstructive sleep apnea (OSA) | −0.37 | 0.23 | 0.117 | 0.69 (0.43–1.09) | 0.972 | 1.029 |
| Cardiovascular disease | 0.07 | 0.08 | 0.409 | 1.07 (0.90–1.28) | 0.920 | 1.087 |
| Smoking | 0.23 | 0.06 | <0.001 | 1.26 (1.11–1.44) | 0.750 | 1.333 |
| Brushing teeth at least once a day | −0.62 | 0.04 | <0.001 | 0.53 (0.49–0.58) | 0.793 | 1.261 |
| Consumption of cariogenic nutrition | 0.15 | 0.04 | 0.002 | 1.16 (1.06–1.27) | 0.589 | 1.679 |
| Consumption of sugary drinks | 0.50 | 0.04 | <0.001 | 1.65 (1.50–1.81) | 0.578 | 1.731 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ben-Assuli, O.; Bar, O.; Geva, G.; Siri, S.; Tzur, D.; Almoznino, G. Body Mass Index and Caries: Machine Learning and Statistical Analytics of the Dental, Oral, Medical Epidemiological (DOME) Nationwide Big Data Study. Metabolites 2023, 13, 37. https://doi.org/10.3390/metabo13010037
Ben-Assuli O, Bar O, Geva G, Siri S, Tzur D, Almoznino G. Body Mass Index and Caries: Machine Learning and Statistical Analytics of the Dental, Oral, Medical Epidemiological (DOME) Nationwide Big Data Study. Metabolites. 2023; 13(1):37. https://doi.org/10.3390/metabo13010037
Chicago/Turabian StyleBen-Assuli, Ofir, Ori Bar, Gaya Geva, Shlomit Siri, Dorit Tzur, and Galit Almoznino. 2023. "Body Mass Index and Caries: Machine Learning and Statistical Analytics of the Dental, Oral, Medical Epidemiological (DOME) Nationwide Big Data Study" Metabolites 13, no. 1: 37. https://doi.org/10.3390/metabo13010037