

Mixed Treatments Comparison of Oral Nutrition Interventions for Blood Immune Cell Parameters in Cancer Patients: Systematic Review and Network Meta-Analysis


Abstract
:1. Introduction
1.1. Rationale
1.2. Objective
2. Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.2.1. Participants (P)
2.2.2. Interventions (I)
2.2.3. Comparators (C)
2.2.4. Outcomes (O)
2.2.5. Study Design (S)
2.2.6. Exclusion Criteria
2.3. Information Sources
2.4. Search
2.5. Study Selection
2.6. Data Collection Process
2.7. Data Items
2.8. Geometry of the Network
2.9. Risk of Bias within Individual Studies
2.10. Summary Measures
2.11. Planned Methods of Analysis
2.12. Assessment of Inconsistency
2.13. Risk of Bias across Studies
2.14. Additional Analyses
3. Results
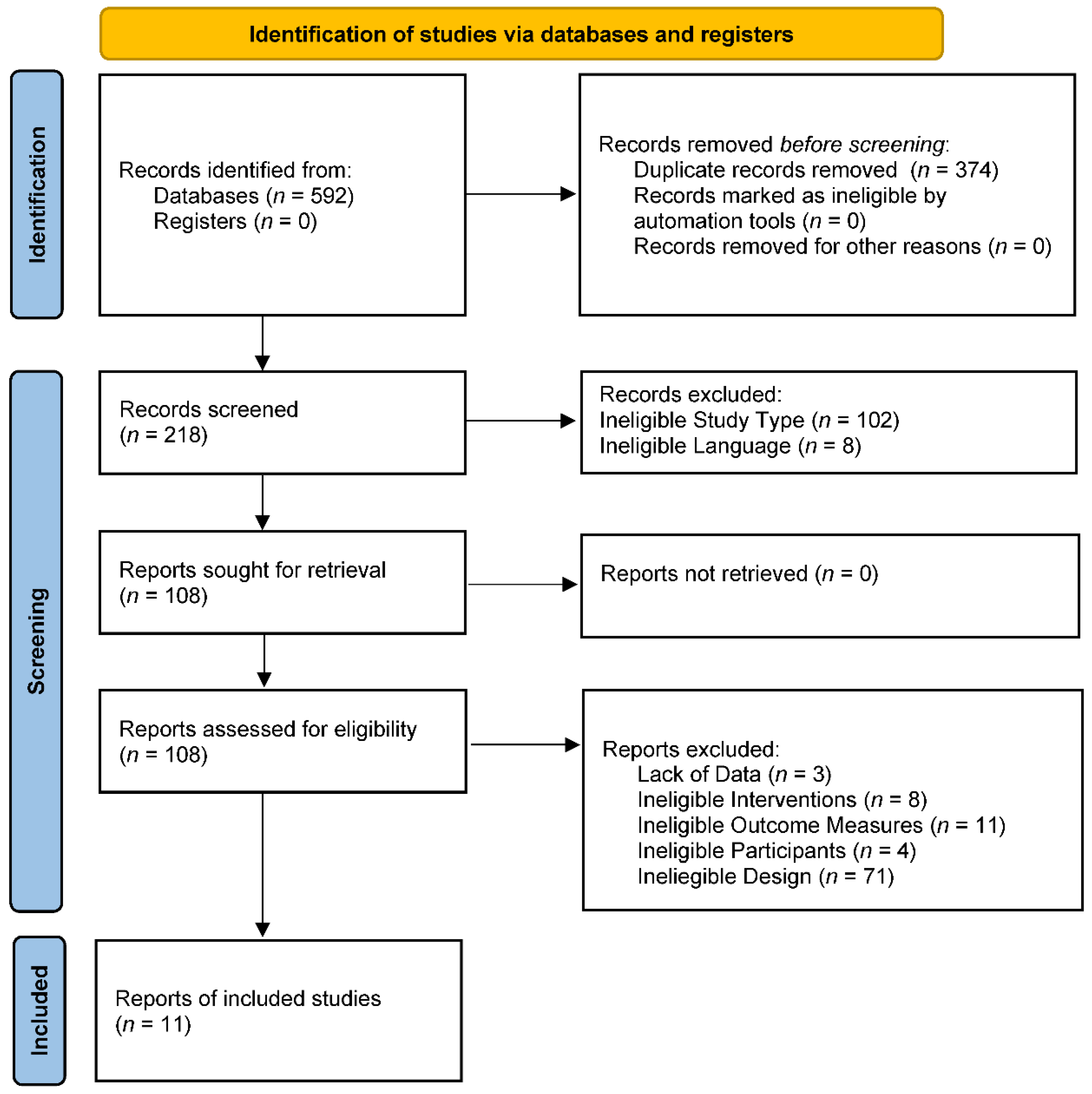
3.1. Study Selection
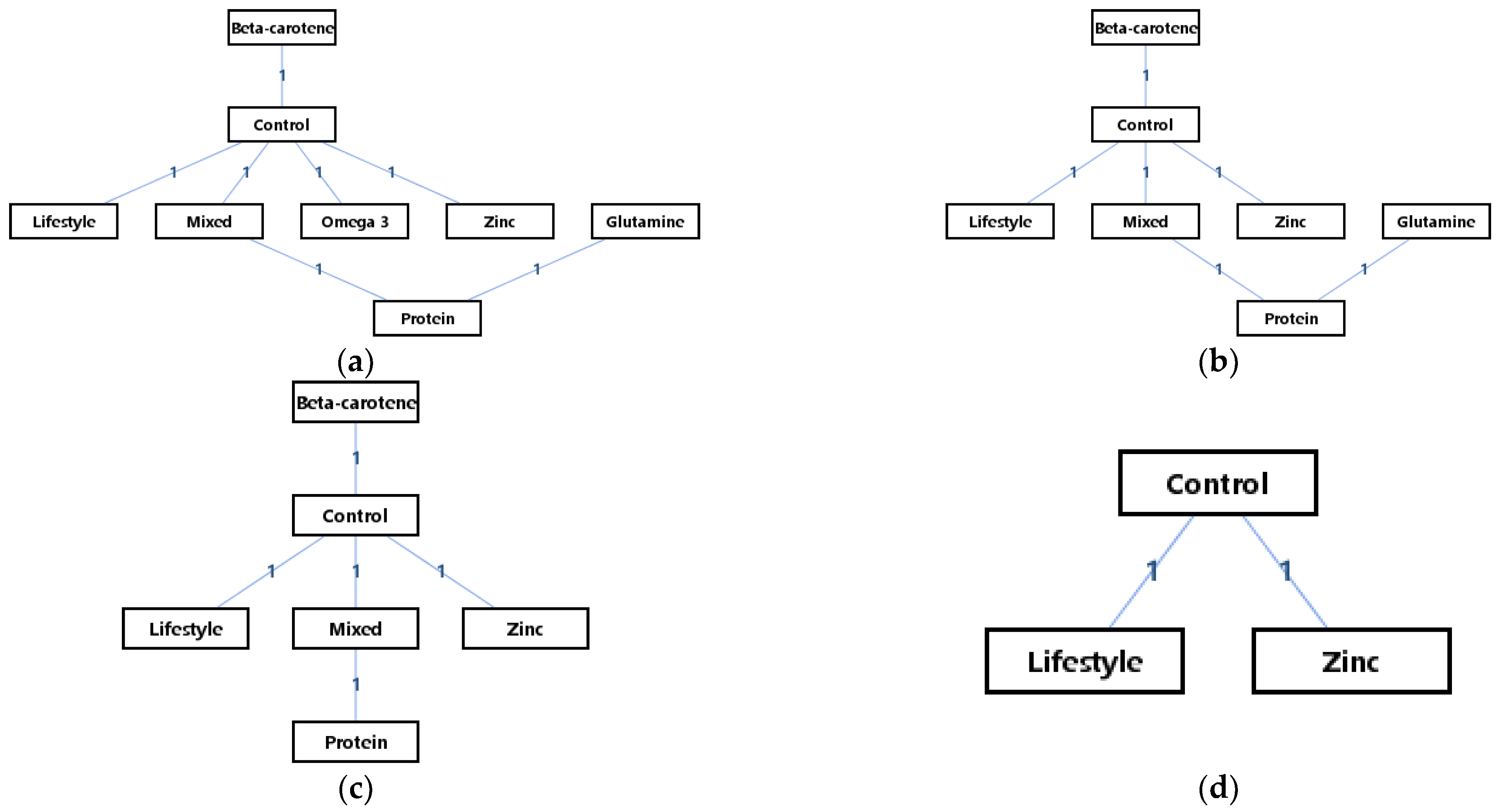
3.2. Presentation of Network Structure
3.3. Study Characteristics
3.4. Risk of Bias within Studies
3.5. Results of Individual Studies
3.6. Synthesis of Results
3.7. Explanation for Inconsistency
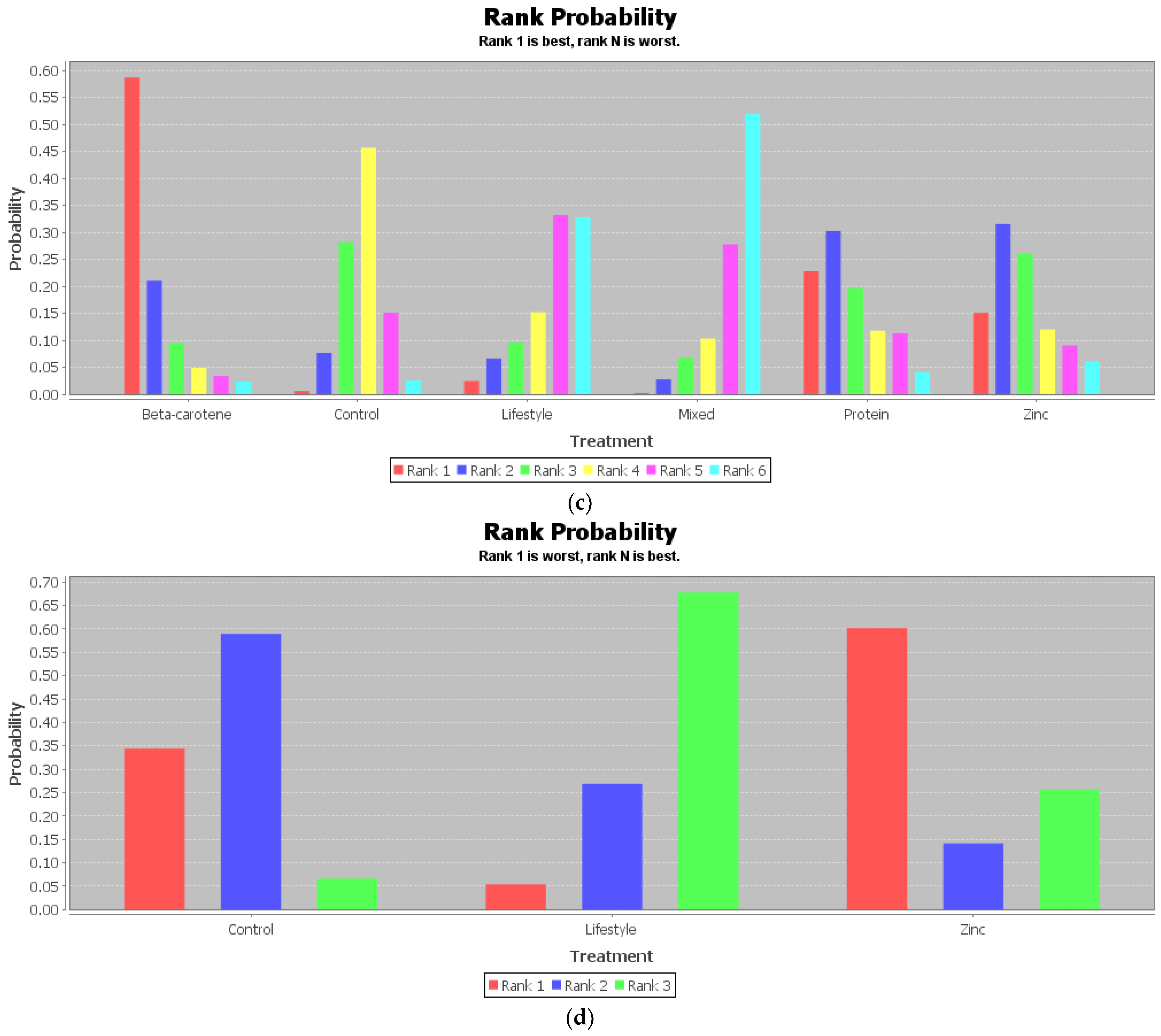
3.8. Results of Additional Analyses
4. Discussion
4.1. Summary of Evidence
4.2. Limitations
4.3. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Mathis, D.; Shoelson, S.E. Immunometabolism: An emerging frontier. Nat. Rev. Immunol. 2011, 11, 81–83. [Google Scholar] [CrossRef]
- Rena, G.; Lang, C.C. Repurposing Metformin for Cardiovascular Disease. Circulation 2018, 137, 422–424. [Google Scholar] [CrossRef] [PubMed]
- Adiamah, A.; Rollins, K.E.; Kapeleris, A.; Welch, N.T.; Iftikhar, S.Y.; Allison, S.P.; Lobo, D.N. Postoperative arginine-enriched immune modulating nutrition: Long-term survival results from a randomised clinical trial in patients with oesophagogastric and pancreaticobiliary cancer. Clin. Nutr. 2021, 40, 5482–5485. [Google Scholar] [CrossRef] [PubMed]
- Dechaphunkul, T.; Arundon, T.; Raungkhajon, P.; Jiratrachu, R.; Geater, S.L.; Dechaphunkul, A. Benefits of immunonutrition in patients with head and neck cancer receiving chemoradiation: A phase II randomized, double-blind study. Clin. Nutr. 2021, 41, 433–440. [Google Scholar] [CrossRef]
- Kilgore, K. An Invitation to Live: Insights from an Older, Long-Term Practitioner of Tai Chi. Phys. Act. Health 2019, 3, 11–22. [Google Scholar] [CrossRef]
- Lavanya, M.; Muthu Kannan, P.; Arivalagan, M. Lung cancer diagnosis and staging using firefly algorithm fuzzy C-means segmentation and support vector machine classification of lung nodules. Int. J. Biomed. Eng. Technol. 2021, 37, 185–200. [Google Scholar] [CrossRef]
- Kumar, A.; Smith, C.; Jobin, C.; Trinchieri, G.; Howcroft, T.K.; Seifried, H.; Espey, M.G.; Flores, R.; Kim, Y.S.; Daschner, P.J. Workshop Report: Modulation of Antitumor Immune Responses by Dietary and Microbial Metabolites. JNCI J. Natl. Cancer Inst. 2017, 109, djx040. [Google Scholar] [CrossRef]
- Caccialanza, R.; De Lorenzo, F.; Gianotti, L.; Zagonel, V.; Gavazzi, C.; Farina, G.; Cotogni, P.; Cinieri, S.; Cereda, E.; Marchetti, P.; et al. Nutritional support for cancer patients: Still a neglected right? Support. Care Cancer 2017, 25, 3001–3004. [Google Scholar] [CrossRef]
- Vernieri, C.; Fucà, G.; Ligorio, F.; Huber, V.; Vingiani, A.; Iannelli, F.; Raimondi, A.; Rinchai, D.; Frigè, G.; Belfiore, A.; et al. Fasting-Mimicking Diet Is Safe and Reshapes Metabolism and Antitumor Immunity in Patients with Cancer. Cancer Discov. 2021, 12, 90–107. [Google Scholar] [CrossRef]
- Rizzo, A.; Ricci, A.D. PD-L1, TMB, and other potential predictors of response to immunotherapy for hepatocellular carcinoma: How can they assist drug clinical trials? Expert Opin. Investig. Drugs 2021, 31, 415–423. [Google Scholar] [CrossRef]
- Westheim, A.J.F.; Stoffels, L.M.; Dubois, L.J.; van Bergenhenegouwen, J.; van Helvoort, A.; Langen, R.C.J.; Shiri-Sverdlov, R.; Theys, J. Fatty Acids as a Tool to Boost Cancer Immunotherapy Efficacy. Front. Nutr. 2022, 9, 868436. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Ling, W.; Shen, Z.Y.; Jin, X.; Cao, H. Clinical application of immune-enhanced enteral nutrition in patients with advanced gastric cancer after total gastrectomy. J. Dig. Dis. 2012, 13, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Nagano, T.; Fujita, H.; Tanaka, T.; Matono, S.; Murata, K.; Ishibashi, N.; Shirouzu, K.; Yanagawa, T. A randomized controlled trial comparing antioxidant-enriched enteral nutrition with immune-enhancing enteral nutrition after esophagectomy for cancer: A pilot study. Surg. Today 2012, 43, 1240–1249. [Google Scholar] [CrossRef] [PubMed]
- Rocha, K.C.; Vieira, M.L.D.S.; Beltrame, R.L.; Cartum, J.; Alves, S.I.P.M.D.N.; Azzalis, L.A.; Junqueira, V.B.C.; Pereira, E.C.; Fonseca, F.L.A. Impact of Selenium Supplementation in Neutropenia and Immunoglobulin Production in Childhood Cancer Patients. J. Med. Food 2016, 19, 560–568. [Google Scholar] [CrossRef]
- Duan, P.; Wang, Z.M. Clinical study on effect of Astragalus in efficacy enhancing and toxicity reducing of chemotherapy in patients of malignant tumor. Zhongguo Zhong Xi Yi Jie He Za Zhi 2002, 22, 515–517. [Google Scholar]
- Zhang, J.W.; Du, P.; Chen, D.W.; Cui, L.; Ying, C.M. Effect of viable Bifidobacterium supplement on the immune status and inflammatory response in patients undergoing resection for colorectal cancer. Zhonghua Wei Chang Wai Ke Za Zhi 2010, 13, 40–43. [Google Scholar]
- Chunbo, X.U.; Shen, M.; Shanming, R. Research Situation of Yang-warming Method for Tumor. J. New Chin. Med. 2019, 8, 51–53. [Google Scholar]
- Dou, J.; Huang, Q.; Zhao, T.; Pharmacy, S.O. Effect of Yanghe Decoction on NF-κB and IL-8 Expression of MDA-MB-231 Cells for Breast Cancer. J. Sichuan Tradit. Chin. Med. 2017, 35, 44–47. [Google Scholar]
- Huang, Q.; Zhang, F.; Li, X. Effect of Yanghe Decoction on Human Breast Cancer MCF-7 Cells and Its PI3K/Akt Signaling Pathway. J. Sichuan Tradit. Chin. Med. 2019, 2, 47–50. [Google Scholar]
- Kangle, L.I.; Peng, P.; Zhang, X.; University, X.J. Effect of Yanghe Decoction on Apoptosis of MDA-MB-231 Cells for Human Breast Cancer. J. Sichuan Tradit. Chin. Med. 2018, 12, 41–42. [Google Scholar]
- Szefel, J.; Ślebioda, T.; Walczak, J.; Kruszewski, W.J.; Szajewski, M.; Ciesielski, M.; Stanisławowski, M.; Buczek, T.; Małgorzewicz, S.; Owczarzak, A.; et al. The effect of l-arginine supplementation and surgical trauma on the frequency of myeloid-derived suppressor cells and T lymphocytes in tumour and blood of colorectal cancer patients. Adv. Med. Sci. 2022, 67, 66–78. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.H.; Dixit, V.D. Dietary Regulation of Immunity. Immunity 2020, 53, 510–523. [Google Scholar] [CrossRef] [PubMed]
- Lamas, O.; Martinez, J.A.; Marti, A. Energy restriction restores the impaired immune response in overweight (cafeteria) rats. J. Nutr. Biochem. 2004, 15, 418–425. [Google Scholar] [CrossRef]
- Nieman, D.C.; Nehlsen-Cannarella, S.L.; Henson, D.A.; Koch, A.J.; Butterworth, D.E.; Fagoaga, O.R.; Utter, A. Immune response to exercise training and/or energy restriction in obese women. Med. Sci. Sports Exerc. 1998, 30, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Afaq, S.; Ali, M.; Ahmad, M.; Hussain, S.; Ali, W.; Munir, I. Metabolic Health Profile of Employees in a Printing Press in Peshawar, Pakistan. Phys. Act. Health 2022, 6, 55–63. [Google Scholar] [CrossRef]
- Methnani, J.; Amor, D.; Yousfi, N.; Bouslama, A.; Omezzine, A.; Bouhlel, E. Sedentary behavior, exercise and COVID-19: Immune and metabolic implications in obesity and its comorbidities. J. Sports Med. Phys. Fit. 2021, 61, 1538–1547. [Google Scholar] [CrossRef]
- Nieman, D.C.; Buckley, K.S.; Henson, D.A.; Warren, B.J.; Suttles, J.; Ahle, J.C.; Simandle, S.; Fagoaga, O.R.; Nehlsen-Cannarella, S.L. Immune function in marathon runners versus sedentary controls. Med. Sci. Sports Exerc. 1995, 27, 986–992. [Google Scholar] [CrossRef]
- Nieman, D.C.; Lila, M.A.; Gillitt, N.D. Immunometabolism: A Multi-Omics Approach to Interpreting the Influence of Exercise and Diet on the Immune System. Annu. Rev. Food Sci. Technol. 2019, 10, 341–363. [Google Scholar] [CrossRef]
- Ramzan, F.; Mitchell, C.J.; Milan, A.M.; Schierding, W.; Zeng, N.; Sharma, P.; Mitchell, S.M.; D’Souza, R.F.; Knowles, S.O.; Roy, N.C.; et al. Comprehensive Profiling of the Circulatory miRNAome Response to a High Protein Diet in Elderly Men: A Potential Role in Inflammatory Response Modulation. Mol. Nutr. Food Res. 2019, 63, e1800811. [Google Scholar] [CrossRef]
- Okala, S.G.; Darboe, M.K.; Sosseh, F.; Sonko, B.; Faye-Joof, T.; Prentice, A.M.; Moore, S.E. Impact of nutritional supplementation during pregnancy on antibody responses to diphtheria-tetanus-pertussis vaccination in infants: A randomised trial in The Gambia. PLoS Med. 2019, 16, e1002854. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.M.; Chiang, B.L.; Wang, L.C. Maternal Nutritional Status and Development of Atopic Dermatitis in Their Offspring. Clin. Rev. Allergy Immunol. 2021, 61, 128–155. [Google Scholar] [CrossRef]
- Hu, F.B. Nutrient supplementation no substitute for healthy diets. Nat. Rev. Cardiol. 2019, 16, 77–79. [Google Scholar] [CrossRef] [PubMed]
- van Daal, M.T.; Folkerts, G.; Garssen, J.; Braber, S. Pharmacological Modulation of Immune Responses by Nutritional Components. Pharmacol. Rev. 2021, 73, 198–232. [Google Scholar] [CrossRef] [PubMed]
- Nobs, S.P.; Zmora, N.; Elinav, E. Nutrition Regulates Innate Immunity in Health and Disease. Annu. Rev. Nutr. 2020, 40, 189–219. [Google Scholar] [CrossRef] [PubMed]
- Bargetzi, L.; Brack, C.; Herrmann, J.; Bargetzi, A.; Hersberger, L.; Bargetzi, M.; Kaegi-Braun, N.; Tribolet, P.; Gomes, F.; Hoess, C.; et al. Nutritional support during the hospital stay reduces mortality in patients with different types of cancers: Secondary analysis of a prospective randomized trial. Ann. Oncol. 2021, 32, 1025–1033. [Google Scholar] [CrossRef] [PubMed]
- Boretti, A. Nutrition, lipidic parameters, and cancer risk and progress. Nutrition 2020, 69, 110538. [Google Scholar] [CrossRef] [PubMed]
- Maumy, L.; Harrissart, G.; Dewaele, P.; Aljaber, A.; Bonneau, C.; Rouzier, R.; Elies, A. Impact of nutrition on breast cancer mortality and risk of recurrence, a review of the evidence. Bull. Cancer 2020, 107, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Shimizu, S.; Shirotani, M.; Yorozu, K.; Kitamura, K.; Oehorumu, M.; Kawai, Y.; Fukuzawa, Y. Nutrition and Cancer Risk from the Viewpoint of the Intestinal Microbiome. Nutrients 2021, 13, 3326. [Google Scholar] [CrossRef] [PubMed]
- Zitvogel, L.; Pietrocola, F.; Kroemer, G. Nutrition, inflammation and cancer. Nat. Immunol. 2017, 18, 843–850. [Google Scholar] [CrossRef] [PubMed]
- Reglero, C.; Reglero, G. Precision Nutrition and Cancer Relapse Prevention: A Systematic Literature Review. Nutrients 2019, 11, 2799. [Google Scholar] [CrossRef] [PubMed]
- Catala-Lopez, F.; Tobias, A.; Cameron, C.; Moher, D.; Hutton, B. Network meta-analysis for comparing treatment effects of multiple interventions: An introduction. Rheumatol. Int. 2014, 34, 1489–1496. [Google Scholar] [CrossRef] [PubMed]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Andrejeva, G.; Rathmell, J.C. Similarities and Distinctions of Cancer and Immune Metabolism in Inflammation and Tumors. Cell Metab. 2017, 26, 49–70. [Google Scholar] [CrossRef]
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of study quality for systematic reviews: A comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: Methodological research. J. Eval. Clin. Pr. 2012, 18, 12–18. [Google Scholar] [CrossRef]
- Rouse, B.; Chaimani, A.; Li, T. Network meta-analysis: An introduction for clinicians. Intern. Emerg. Med. 2017, 12, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Nikolakopoulou, A.; Higgins, J.P.T.; Papakonstantinou, T.; Chaimani, A.; Del Giovane, C.; Egger, M.; Salanti, G. CINeMA: An approach for assessing confidence in the results of a network meta-analysis. PLoS Med. 2020, 17, e1003082. [Google Scholar] [CrossRef] [Green Version]
- Papakonstantinou, T.; Nikolakopoulou, A.; Higgins, J.P.T.; Egger, M.; Salanti, G. CINeMA: Software for semiautomated assessment of the confidence in the results of network meta-analysis. Campbell Syst. Rev. 2020, 16, e1080. [Google Scholar] [CrossRef]
- Homkham, N.; Muangwong, P.; Pisprasert, V.; Traisathit, P.; Jiratrachu, R.; Chottaweesak, P.; Chitapanarux, I. Dynamic changes in practical inflammation and immunity markers in cancer patients receiving immune-enhancing nutritional supplementation during concurrent chemoradiotherapy. Cancer Biomark. 2021, 32, 281–291. [Google Scholar] [CrossRef]
- Saxton, J.M.; Scott, E.J.; Daley, A.J.; Woodroofe, M.; Mutrie, N.; Crank, H.; Powers, H.J.; Coleman, R.E. Effects of an exercise and hypocaloric healthy eating intervention on indices of psychological health status, hypothalamic-pituitary-adrenal axis regulation and immune function after early-stage breast cancer: A randomised controlled trial. Breast Cancer Res. 2014, 16, R39. [Google Scholar] [CrossRef]
- Paixao, E.; Oliveira, A.C.M.; Pizato, N.; Muniz-Junqueira, M.I.; Magalhaes, K.G.; Nakano, E.Y.; Ito, M.K. The effects of EPA and DHA enriched fish oil on nutritional and immunological markers of treatment naive breast cancer patients: A randomized double-blind controlled trial. Nutr. J. 2017, 16, 71. [Google Scholar] [CrossRef]
- Yoshida, S.; Matsui, M.; Shirouzu, Y.; Fujita, H.; Yamana, H.; Shirouzu, K. Effects of glutamine supplements and radiochemotherapy on systemic immune and gut barrier function in patients with advanced esophageal cancer. Ann. Surg. 1998, 227, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Feijo, P.M.; Rodrigues, V.D.; Viana, M.S.; Dos Santos, M.P.; Abdelhay, E.; Viola, J.P.; de Pinho, N.B.; Martucci, R.B. Effects of omega-3 supplementation on the nutritional status, immune, and inflammatory profiles of gastric cancer patients: A randomized controlled trial. Nutrition 2019, 61, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Sangthawan, D.; Phungrassami, T.; Sinkitjarurnchai, W. Effects of zinc sulfate supplementation on cell-mediated immune response in head and neck cancer patients treated with radiation therapy. Nutr. Cancer 2015, 67, 449–456. [Google Scholar] [CrossRef]
- Kazi, N.; Radvany, R.; Oldham, T.; Keshavarzian, A.; Frommel, T.O.; Libertin, C.; Mobarhan, S. Immunomodulatory effect of beta-carotene on T lymphocyte subsets in patients with resected colonic polyps and cancer. Nutr. Cancer 1997, 28, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Wierdak, M.; Surmiak, M.; Milian-Ciesielska, K.; Rubinkiewicz, M.; Rzepa, A.; Wysocki, M.; Major, P.; Klek, S.; Pedziwiatr, M. Immunonutrition Changes Inflammatory Response in Colorectal Cancer: Results from a Pilot Randomized Clinical Trial. Cancers 2021, 13, 1444. [Google Scholar] [CrossRef]
- de Luis, D.A.; Izaola, O.; Aller, R.; Cuellar, L.; Terroba, M.C. A randomized clinical trial with oral Immunonutrition (omega3-enhanced formula vs. arginine-enhanced formula) in ambulatory head and neck cancer patients. Ann. Nutr. Metab. 2005, 49, 95–99. [Google Scholar] [CrossRef]
- Bumrungpert, A.; Pavadhgul, P.; Nunthanawanich, P.; Sirikanchanarod, A.; Adulbhan, A. Whey Protein Supplementation Improves Nutritional Status, Glutathione Levels, and Immune Function in Cancer Patients: A Randomized, Double-Blind Controlled Trial. J. Med. Food 2018, 21, 612–616. [Google Scholar] [CrossRef]
- Wang, J.; Ma, X.; Shang, K.; Wu, S.; Ma, Y.; Ma, Z.; Cao, B. Safety and efficacy of spleen aminopeptide oral lyophilized powder for improving quality of life and immune response in patients with advanced breast cancer: A multicenter, randomized, double-blind, placebo-controlled clinical trial. Anti-Cancer Drugs 2021, 32, 1067–1075. [Google Scholar] [CrossRef]
- Lyra, M.M.F.; Meira, J.E.C.; Guedes, G.D.S.; Bueno, N.B. Immunonutrition in head and neck cancer: Systematic review and metanalysis of its clinical and nutritional effects. Clin. Nutr. ESPEN 2021, 41, 30–41. [Google Scholar] [CrossRef]
- Kim, H.Y.; Nam, S.Y.; Yang, S.Y.; Kim, H.M.; Jeong, H.J. Cucurbita moschata Duch. and its active component, beta-carotene effectively promote the immune responses through the activation of splenocytes and macrophages. Immunopharmacol. Immunotoxicol. 2016, 38, 319–326. [Google Scholar] [CrossRef]
- Vlasova, I.A.; Kazantseva, S.V.; Adrianovskii, V.I.; Eremin Iu, N. Beta-carotene prevention of immune disorders in workers engaged in the fire copper refining. Gig. Sanit. 2002, 28–32. [Google Scholar]
- Wieringa, F.T.; Dijkhuizen, M.A.; Muhilal; Van der Meer, J.W. Maternal micronutrient supplementation with zinc and beta-carotene affects morbidity and immune function of infants during the first 6 months of life. Eur. J. Clin. Nutr. 2010, 64, 1072–1079. [Google Scholar] [CrossRef]
- Mizutani, H.; Engelman, R.W.; Kurata, Y.; Ikehara, S.; Good, R.A. Energy restriction prevents and reverses immune thrombocytopenic purpura (ITP) and increases life span of ITP-prone (NZW × BXSB) F1 mice. J. Nutr. 1994, 124, 2016–2023. [Google Scholar] [CrossRef] [PubMed]
- Dossus, L.; Kaaks, R. Nutrition, metabolic factors and cancer risk. Best Pr. Res. Clin. Endocrinol. Metab. 2008, 22, 551–571. [Google Scholar] [CrossRef] [PubMed]
- Davoodi, S.H.; Yousefinejad, V.; Ghaderi, B.; Akbari, M.E.; Darvishi, S.; Mehrabi, Y.; Darvishi, N. Oral Propolis, Nutritional Status and Quality of Life with Chemotherapy for Breast Cancer: A Randomized, Double-Blind Clinical Trial. Nutr. Cancer 2022, 74, 2029–2037. [Google Scholar] [CrossRef]
- Dhruva, A.; Wu, C.; Miaskowski, C.; Hartogensis, W.; Rugo, H.S.; Adler, S.R.; Kaptchuk, T.J.; Kelkar, R.; Agarawal, S.; Vadodaria, A.; et al. A 4-Month Whole-Systems Ayurvedic Medicine Nutrition and Lifestyle Intervention Is Feasible and Acceptable for Breast Cancer Survivors: Results of a Single-Arm Pilot Clinical Trial. Glob. Adv. Health Med. 2020, 9, 2164956120964712. [Google Scholar] [CrossRef] [PubMed]
- Schmoranzer, F.; Fuchs, N.; Markolin, G.; Carlin, E.; Sakr, L.; Sommeregger, U. Influence of a complex micronutrient supplement on the immune status of elderly individuals. Int. J. Vitam. Nutr. Res. 2009, 79, 308–318. [Google Scholar] [CrossRef]
- Romero, F.G.; Lira, F.S.; Marques, F.A.; Muzy, P.C.; Peres, R.A.; Caperuto, E.C. PAKs supplement improves immune status and body composition but not muscle strength in resistance trained individuals. J. Int. Soc. Sports Nutr. 2010, 7, 36. [Google Scholar] [CrossRef]
- Mudge, L.; Isenring, E.; Jamieson, G.G. Immunonutrition in patients undergoing esophageal cancer resection. Dis. Esophagus 2011, 24, 160–165. [Google Scholar] [CrossRef]
- Munbauhal, G.; Drouin, S.J.; Mozer, P.; Colin, P.; Phe, V.; Cussenot, O.; Roupret, M. Malnourishment in bladder cancer and the role of immunonutrition at the time of cystectomy: An overview for urologists. BJU Int. 2014, 114, 177–184. [Google Scholar] [CrossRef]
- Davies, A.A.; Davey Smith, G.; Harbord, R.; Bekkering, G.E.; Sterne, J.A.; Beynon, R.; Thomas, S. Nutritional interventions and outcome in patients with cancer or preinvasive lesions: Systematic review. J. Natl. Cancer Inst. 2006, 98, 961–973. [Google Scholar] [CrossRef]
- Dunstan, J.A.; Breckler, L.; Hale, J.; Lehmann, H.; Franklin, P.; Lyons, G.; Ching, S.Y.; Mori, T.A.; Barden, A.; Prescott, S.L. Supplementation with vitamins C, E, beta-carotene and selenium has no effect on anti-oxidant status and immune responses in allergic adults: A randomized controlled trial. Clin. Exp. Allergy 2007, 37, 180–187. [Google Scholar] [CrossRef]
- Wood, S.M.; Beckham, C.; Yosioka, A.; Darban, H.; Watson, R.R. beta-Carotene and selenium supplementation enhances immune response in aged humans. Integr. Med. 2000, 2, 85–92. [Google Scholar] [CrossRef]
- Pascual, G.; Dominguez, D.; Elosua-Bayes, M.; Beckedorff, F.; Laudanna, C.; Bigas, C.; Douillet, D.; Greco, C.; Symeonidi, A.; Hernandez, I.; et al. Dietary palmitic acid promotes a prometastatic memory via Schwann cells. Nature 2021, 599, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Bai, H.; Li, Z.; Meng, Y.; Yu, Y.; Zhang, H.; Shen, D.; Chen, L. Effects of parenteral omega-3 fatty acid supplementation in postoperative gastrointestinal cancer on immune function and length of hospital stay: A systematic review and meta-analysis. Asia Pac. J. Clin. Nutr. 2018, 27, 121–128. [Google Scholar] [CrossRef]
- Bairati, I.; Meyer, F.; Jobin, E.; Gelinas, M.; Fortin, A.; Nabid, A.; Brochet, F.; Tetu, B. Antioxidant vitamins supplementation and mortality: A randomized trial in head and neck cancer patients. Int. J. Cancer 2006, 119, 2221–2224. [Google Scholar] [CrossRef] [PubMed]
- Bjelakovic, G.; Nikolova, D.; Gluud, L.L.; Simonetti, R.G.; Gluud, C. Antioxidant supplements for prevention of mortality in healthy participants and patients with various diseases. Cochrane Database Syst. Rev. 2012, 2012, CD007176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjelakovic, G.; Nikolova, D.; Gluud, C. Meta-regression analyses, meta-analyses, and trial sequential analyses of the effects of supplementation with beta-carotene, vitamin A, and vitamin E singly or in different combinations on all-cause mortality: Do we have evidence for lack of harm? PLoS ONE 2013, 8, e74558. [Google Scholar] [CrossRef] [PubMed]
- Gardner, E.M.; Bernstein, E.D.; Popoff, K.A.; Abrutyn, E.; Gross, P.; Murasko, D.M. Immune response to influenza vaccine in healthy elderly: Lack of association with plasma beta-carotene, retinol, alpha-tocopherol, or zinc. Mech. Ageing Dev. 2000, 117, 29–45. [Google Scholar] [CrossRef]
- Hughes, D.A.; Wright, A.J.; Finglas, P.M.; Peerless, A.C.; Bailey, A.L.; Astley, S.B.; Pinder, A.C.; Southon, S. The effect of beta-carotene supplementation on the immune function of blood monocytes from healthy male nonsmokers. J. Lab. Clin. Med. 1997, 129, 309–317. [Google Scholar] [CrossRef]
- Zhang, F.; Jin, Y.; Qiang, W. The effects of dietary advice on malnutrition in Cancer patients: A systematic review and meta-analysis. Support. Care Cancer 2020, 28, 1579–1585. [Google Scholar] [CrossRef]
- Ying, J.; Cen, X.; Yu, P. Effects of Eccentric Exercise on Skeletal Muscle Injury: From An Ultrastructure Aspect: A Review. Phys. Act. Health 2021, 5, 15–20. [Google Scholar] [CrossRef]
- Nicolini, A.; Ferrari, P.; Masoni, M.C.; Fini, M.; Pagani, S.; Giampietro, O.; Carpi, A. Malnutrition, anorexia and cachexia in cancer patients: A mini-review on pathogenesis and treatment. Biomed. Pharmacother. 2013, 67, 807–817. [Google Scholar] [CrossRef] [PubMed]
- Ryan, A.M.; Reynolds, J.V.; Healy, L.; Byrne, M.; Moore, J.; Brannelly, N.; McHugh, A.; McCormack, D.; Flood, P. Enteral nutrition enriched with eicosapentaenoic acid (EPA) preserves lean body mass following esophageal cancer surgery: Results of a double-blinded randomized controlled trial. Ann. Surg. 2009, 249, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Owen, M.; Au, C. The development of a brain controlled interface employing electroencephalography to control a hand prostheses. Int. J. Biomed. Eng. Technol. 2021, 35, 173–190. [Google Scholar] [CrossRef]
- Heys, S.D.; Walker, L.G.; Smith, I.; Eremin, O. Enteral nutritional supplementation with key nutrients in patients with critical illness and cancer: A meta-analysis of randomized controlled clinical trials. Ann. Surg. 1999, 229, 467–477. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Participants | Interventions | Outcome Measures | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Age | Gender (F/M) | Cancer | Nationality | Protocol | Process | Classification | Therapy Form | ||
| Kazi 1997 [54] | 67.47 | 3/16 | Colon cancer | American | Beta-carotene capsules | 30 mg/day, 3 months | Beta-carotene | After surgery | WBC Lymphocyte CD4/CD8 |
| Placebo capsules | 30 mg/day, 3 months | Control | |||||||
| Yoshida 1998 [51] | 61.18 | 2/11 | Esophageal cancer | Japanese | Oral glutamine | 30 g/day, 28 days, | Glutamine | Irradiation and chemotherapy | WBC Lymphocyte |
| Standard amino acid solution | Isonitrogenous aminos, 28 days | Protein | |||||||
| de Luis 2005 [56] | 61.8 | 5/68 | Head and Neck cancer | Spanish | Omega 3-enhanced oral immunonutrition | Omega 3-enhanced supplementation with a basal oral diet, 12 weeks | Omega 3 | After surgery | Lymphocyte |
| Arginine-enhanced oral immunonutrition | Arginine-enhanced supplementation with a basal oral diet, 12 weeks | Arginine | |||||||
| Saxton 2014 [49] | 55.56 | 85/0 | Early-stage breast cancer | British | An exercise and hypocaloric healthy eating intervention | 600 kcal below their calculated energy requirements/day + 3 supervised exercise sessions (30 min aerobic exercise + 10 to 15 min of muscle-strengthening exercises)/week | Lifestyle | After surgery | WBC Lymphocyte CD4/CD8 Neutrophil |
| Blank | A healthy eating booklet | Control | |||||||
| Sangthawan 2015 [53] | 61.00 | 8/64 | Head and Neck cancer | Thai | Zinc sulfate supplementation | Oral syrups zinc sulfate, 5 mg/cc, 50 mg (10 cc)/meal, 3 times/day at mealtimes | Zinc | Radiation Therapy after surgery | WBC Lymphocyte CD4/CD8 Neutrophil |
| Placebo | Oral syrups of a placebo, 3 times/day at mealtimes | Control | |||||||
| Paixao 2017 [50] | 51.06 | 37/0 | Breast cancer | Brazilians | EPA and DHA-enriched fish oil | 2 g/day of fish oil concentrate containing 1.8 g of n-3 fatty acids for 30 days | Omega-3 | Perioperative period | WBC |
| Placebo | 2 g/day of mineral oil for 30 days | Control | |||||||
| Feijo 2019 [52] | 58.00 | 22/44 | Gastric cancer | Brazilians | Omega-3 supplementation | 600 kcal, 24 g protein, and 3.2 g of omega 3/day, 200 mL/day, 30 days | Mixed | Before Surgery | CD4/CD8 |
| Standard formula without Omega-3 | 560 kcal and 29 g protein/day, 30 days | Protein | |||||||
| Wierdak 2021 [55] | 64.26 | 14/12 | Colorectal cancer | Polish | Standard oral nutritional | 2 times Nutricia Nutridrink Protein/day, 2/day, 2 weeks | Protein | Perioperative period | WBC Lymphocyte Neutrophil |
| Immunonutrition | 2 times Arginine + Glutamine + Omega-3 + Nucleotides + Zinc, 2 weeks | Mixed | |||||||
| Wang 2021 [58] | 55.4 | 36/0 | Breast cancer | Chinese | Spleen amino-peptide oral lyophilized powder | 4 mg on the first day of chemotherapy for two cycles. | Mixed | Unlimited | CD4/CD8 |
| Placebo | 4 mg on the first day of chemotherapy for two cycles. | Control | |||||||
| Bumrungpert 2018 [57] | 52.92 | 32/10 | Cancer without metastatic diseases | Thai | Whey Protein Supplementation | 40 g Whey protein isolate with Zn (2.64 mg/day) and Se (0.76 mg/day) | Mixed | During chemotherapy | WBC |
| Maltodextrin oral snack | 40 g of maltodextrin as a daytime snack | Control | |||||||
| Homkham 2021 [48] | 56.00 | 35/49 | Cancer | Thai | Regular diet | 1500 kcal, 60 g protein/day (esophageal cancer patients, 2000 kcal, 75 g/day via feeding tube) | Control | During chemo-therapy | Lymphocyte |
| Immune-enhanced nutritional supplementation | A regular diet + 500 kcal/day of supplementation containing arginine 6.16 g, L-glutamine 3.07 g, and fish oil 2.73 g that prepared in sachet form, 2 times/day | Mixed | |||||||
| Study | Duration | Reporting Time | Main Results of Blood Immune Cell Parameters |
|---|---|---|---|
| Kazi 1997 [54] | 12 weeks | Pre treatment 12 weeks | A significant increase in lymphocytes and CD4. |
| Yoshida 1998 [51] | 4 weeks | Pre treatment 4 weeks |
|
| de Luis 2005 [56] | 12 weeks | Pre treatment 12 weeks | No significant intergroup differences in the trend of the three serum proteins and lymphocytes were detected. |
| Saxton 2014 [49] | 24 weeks | Pre treatment 24 weeks | Women in the control group had higher total leukocyte, neutrophil, and lymphocyte counts in comparison to the intervention group at the 6-month follow-up. |
| Sangthawan 2015 [53] | Unlimited | Pre treatment 5 weeks Post treatment |
|
| Paixao 2017 [50] | 30 days | Pre treatment 30 days |
|
| Feijo 2019 [52] | 30 days | Pre treatment 30 days | There was the maintenance of the immune profile in both groups; |
| Wierdak 2021 [55] | 2 weeks | Pre treatment 2 weeks | In both groups, a decrease in superficial neutrophil infiltration was observed, but this was only statistically significant in the immune group; |
| Wang 2021 [58] | 12 weeks | Pre treatment 3 weeks 6 weeks 12 weeks | On day 84, the number of CD3, CD4, and CD8 cells was significantly higher in the experimental group; |
| Bumrungpert 2018 [57] | 12 weeks | Pre treatment 6 weeks 12 weeks |
|
| Homkham 2021 [48] | 4 weeks | Pre treatment 2 weeks 4 weeks |
|
| WBC | Beta-carotene | 1.26 | 2.23 | 0.81 | 1.20 | 2.37 | 2.04 | 1.45 |
| Control | 0.99 | −0.44 | −0.06 | 1.10 | 0.84 | 0.22 | ||
| Glutamine | −1.42 | −1.05 | 0.13 | −0.16 | −0.76 | |||
| Lifestyle | 0.37 | 1.55 | 1.25 | 0.64 | ||||
| Mixed | 1.16 | 0.88 | 0.25 | |||||
| Omega 3 | −0.28 | −0.89 | ||||||
| Protein | −0.63 | |||||||
| Zinc | ||||||||
| Lymphocyte | Beta-carotene | 58.54 | 318.67 | −29.41 | 149.02 | 186.55 | 57.62 | |
| Control | 260.49 | −87.11 | 89.32 | 129.54 | −1.97 | |||
| Glutamine | −344.58 | −171.71 | −132.38 | −263.43 | ||||
| Lifestyle | 176.71 | 215.26 | 84.98 | |||||
| Mixed | 39.20 | −89.82 | ||||||
| Protein | −132.57 | |||||||
| Zinc | ||||||||
| CD4/CD8 | Beta-carotene | −0.62 | −0.84 | −0.96 | −0.35 | −0.40 | ||
| Control | −0.22 | −0.33 | 0.26 | 0.22 | ||||
| Lifestyle | −0.11 | 0.49 | 0.44 | |||||
| Mixed | 0.60 | 0.55 | ||||||
| Protein | −0.04 | |||||||
| Zinc | ||||||||
| Neutrophil | Control | −376.33 | 285.34 | |||||
| Lifestyle | 650.94 | |||||||
| Zinc | ||||||||
| Outcome | Intervention | Rank 1 | Rank 2 | Rank 3 | Rank 4 | Rank 5 | Rank 6 | Rank 7 | Rank 8 |
|---|---|---|---|---|---|---|---|---|---|
| WBC | Beta-carotene | 0.01 | 0.02 | 0.03 | 0.05 | 0.07 | 0.09 | 0.17 | 0.55 |
| Control | 0.01 | 0.07 | 0.13 | 0.17 | 0.28 | 0.25 | 0.08 | 0.01 | |
| Glutamine | 0.30 | 0.22 | 0.14 | 0.09 | 0.08 | 0.07 | 0.06 | 0.05 | |
| Lifestyle | 0.02 | 0.05 | 0.07 | 0.10 | 0.14 | 0.19 | 0.30 | 0.14 | |
| Mixed | 0.02 | 0.04 | 0.14 | 0.20 | 0.17 | 0.17 | 0.16 | 0.1 | |
| Omega 3 | 0.37 | 0.16 | 0.20 | 0.14 | 0.07 | 0.03 | 0.02 | 0.01 | |
| Protein | 0.14 | 0.30 | 0.17 | 0.12 | 0.08 | 0.09 | 0.07 | 0.03 | |
| Zinc | 0.14 | 0.14 | 0.12 | 0.13 | 0.11 | 0.11 | 0.14 | 0.11 | |
| Lymphocyte | Beta-carotene | 0.04 | 0.06 | 0.10 | 0.13 | 0.16 | 0.24 | 0.27 | |
| Control | 0.00 | 0.03 | 0.14 | 0.32 | 0.35 | 0.14 | 0.02 | ||
| Glutamine | 0.28 | 0.32 | 0.22 | 0.11 | 0.04 | 0.02 | 0.01 | ||
| Lifestyle | 0.02 | 0.03 | 0.06 | 0.10 | 0.15 | 0.28 | 0.36 | ||
| Mixed | 0.13 | 0.30 | 0.26 | 0.14 | 0.09 | 0.05 | 0.02 | ||
| Protein | 0.44 | 0.11 | 0.08 | 0.06 | 0.07 | 0.08 | 0.16 | ||
| Zinc | 0.09 | 0.13 | 0.14 | 0.14 | 0.15 | 0.18 | 0.16 | ||
| CD4/CD8 | Beta-carotene | 0.59 | 0.21 | 0.1 | 0.05 | 0.03 | 0.02 | ||
| Control | 0.01 | 0.08 | 0.28 | 0.46 | 0.15 | 0.03 | |||
| Lifestyle | 0.02 | 0.07 | 0.1 | 0.15 | 0.33 | 0.33 | |||
| Mixed | 0 | 0.03 | 0.07 | 0.1 | 0.28 | 0.52 | |||
| Protein | 0.23 | 0.3 | 0.2 | 0.12 | 0.11 | 0.04 | |||
| Zinc | 0.15 | 0.32 | 0.26 | 0.12 | 0.09 | 0.06 | |||
| Neutrophil | Control | 0.34 | 0.59 | 0.07 | |||||
| Lifestyle | 0.05 | 0.27 | 0.68 | ||||||
| Zinc | 0.60 | 0.14 | 0.26 |
| Outcome | Model | Inference Samples | Random-Effects Standard Deviation | t | Sig. |
|---|---|---|---|---|---|
| WBC | Consistency | 10,000 | 0.64 (0.06, 1.23) | 0.042 | 0.97 |
| Inconsistency | 20,000 | 0.62 (0.04, 1.23) | |||
| Lymphocyte | Consistency | 40,000 | 67.09 (5.76, 127.80) | 0.001 | 0.99 |
| Inconsistency | 40,000 | 64.07 (3.34, 127.67) | |||
| CD4/CD8 | Consistency | 10,000 | 0.32 (0.02, 0.62) | 0.031 | 0.98 |
| Inconsistency | 40,000 | 0.33 (0.02, 0.63) | |||
| Neutrophil | Consistency | 10,000 | 193.51 (12.39, 369.40) | 0.017 | 0.99 |
| Inconsistency | 20,000 | 191.02 (10.13, 369.41) |
| Outcome | Structure | Comparison | Arms | Within-Study Bias | Reporting Bias | Indirectness | Imprecision | Heterogeneity | Incoherence | Confidence Rating | Reason(s) for Downgrading |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Leukocytes (WBC) | Mixed | Beta-carotene:Control | 1 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence |
| Control:Lifestyle | 1 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Control:Mixed | 2 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Control:Omega 3 | 1 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Control:Zinc | 2 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Glutamine:Protein | 3 | Some concerns | Low risk | No concerns | No concerns | No concerns | Major concerns | Low | Incoherence | ||
| Mixed:Protein | 1 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Indirect | Beta-carotene:Glutamine | 0 | Some concerns | Low risk | No concerns | No concerns | No concerns | Major concerns | Low | Incoherence | |
| Beta-carotene:Lifestyle | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Beta-carotene:Mixed | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Beta-carotene:Omega 3 | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Beta-carotene:Protein | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Beta-carotene:Zinc | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Control:Glutamine | 0 | Some concerns | Low risk | No concerns | No concerns | No concerns | Major concerns | Low | Incoherence | ||
| Control:Protein | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Glutamine:Lifestyle | 0 | Some concerns | Low risk | No concerns | No concerns | No concerns | Major concerns | Low | Incoherence | ||
| Glutamine:Mixed | 0 | Some concerns | Low risk | No concerns | No concerns | No concerns | Major concerns | Low | Incoherence | ||
| Glutamine:Omega 3 | 0 | Some concerns | Low risk | No concerns | No concerns | No concerns | Major concerns | Low | Incoherence | ||
| Glutamine:Zinc | 0 | Some concerns | Low risk | No concerns | No concerns | No concerns | Major concerns | Low | Incoherence | ||
| Lifestyle:Mixed | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Lifestyle:Omega 3 | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Lifestyle:Protein | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Lifestyle:Zinc | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Mixed:Omega 3 | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Mixed:Zinc | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Omega 3:Protein | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Omega 3:Zinc | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Protein:Zinc | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Lymphocyte | Mixed | Beta-carotene:Control | 1 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence |
| Control:Lifestyle | 1 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Control:Mixed | 2 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Control:Zinc | 2 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Glutamine:Protein | 3 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Mixed:Protein | 1 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Indirect | Beta-carotene:Glutamine | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | |
| Beta-carotene:Lifestyle | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Beta-carotene:Mixed | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Beta-carotene:Protein | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Beta-carotene:Zinc | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Control:Glutamine | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Control:Protein | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Glutamine:Lifestyle | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Glutamine:Mixed | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Glutamine:Zinc | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Lifestyle:Mixed | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Lifestyle:Protein | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Lifestyle:Zinc | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Mixed:Zinc | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Protein:Zinc | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| CD4/CD8 | Mixed | Beta-carotene:Control | 1 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence |
| Control:Lifestyle | 1 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Control:Mixed | 3 | Some concerns | Low risk | No concerns | No concerns | Major concerns | Major concerns | Very low | Heterogeneity and Incoherence | ||
| Control:Zinc | 2 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Mixed:Protein | 1 | Major concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Indirect | Beta-carotene:Lifestyle | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | |
| Beta-carotene:Mixed | 0 | Some concerns | Low risk | No concerns | No concerns | Major concerns | Major concerns | Very low | Heterogeneity and Incoherence | ||
| Beta-carotene:Protein | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Beta-carotene:Zinc | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Control:Protein | 0 | Major concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Lifestyle:Mixed | 0 | Some concerns | Low risk | No concerns | No concerns | Major concerns | Major concerns | Very low | Heterogeneity and Incoherence | ||
| Lifestyle:Protein | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Lifestyle:Zinc | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Mixed:Zinc | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | Imprecision and Incoherence | ||
| Protein:Zinc | 0 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Low | Imprecision and Incoherence | ||
| Neutrophil | Mixed | Control:Lifestyle | 1 | Some concerns | Low risk | No concerns | None | Unclear | Unclear | Unclear | Unclear |
| Control:Zinc | 2 | Some concerns | Low risk | No concerns | None | Unclear | Unclear | Unclear | Unclear | ||
| Indirect | Lifestyle:Zinc | 0 | Some concerns | Low risk | No concerns | None | Unclear | Unclear | Unclear | Unclear |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fang, Y.; Xu, Y.; Zhang, Y.; Ren, F.; Baker, J.S. Mixed Treatments Comparison of Oral Nutrition Interventions for Blood Immune Cell Parameters in Cancer Patients: Systematic Review and Network Meta-Analysis. Metabolites 2022, 12, 868. https://doi.org/10.3390/metabo12090868
Fang Y, Xu Y, Zhang Y, Ren F, Baker JS. Mixed Treatments Comparison of Oral Nutrition Interventions for Blood Immune Cell Parameters in Cancer Patients: Systematic Review and Network Meta-Analysis. Metabolites. 2022; 12(9):868. https://doi.org/10.3390/metabo12090868
Chicago/Turabian StyleFang, Yufei, Yining Xu, Yuting Zhang, Feng Ren, and Julien S. Baker. 2022. "Mixed Treatments Comparison of Oral Nutrition Interventions for Blood Immune Cell Parameters in Cancer Patients: Systematic Review and Network Meta-Analysis" Metabolites 12, no. 9: 868. https://doi.org/10.3390/metabo12090868