
Chromosomal Aberrations and Oxidative Stress in Psoriatic Patients with and without Metabolic Syndrome

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. PASI
2.3. Metabolic Syndrome
- Increased waist circumference (abdominal obesity ≥102 cm for men and ≥88 cm for women);
- Glucose intolerance presented by a higher fasting glucose of 5.6 mmol/L or known treatment for diabetes;
- Elevated triglyceride level (TAG) 1.7 mmol/L;
- Reduced level of high-density lipoproteins (HDL cholesterol) <1.03 mmol/L for men and <1.30 mmol/L for women;
- Elevated blood pressure (systolic blood pressure < 130 mmHg and/or diastolic blood pressure < 85 mmHg).
2.4. Blood Sampling
2.4.1. Biochemical Parameters
2.4.2. Oxidative Damage to DNA/RNA
2.4.3. CAT
2.4.4. Group Analysis
2.4.5. Individual Analysis
2.5. Statistical Analysis
3. Results
3.1. Demographic Data of Participants
3.2. DNA/RNA Damage
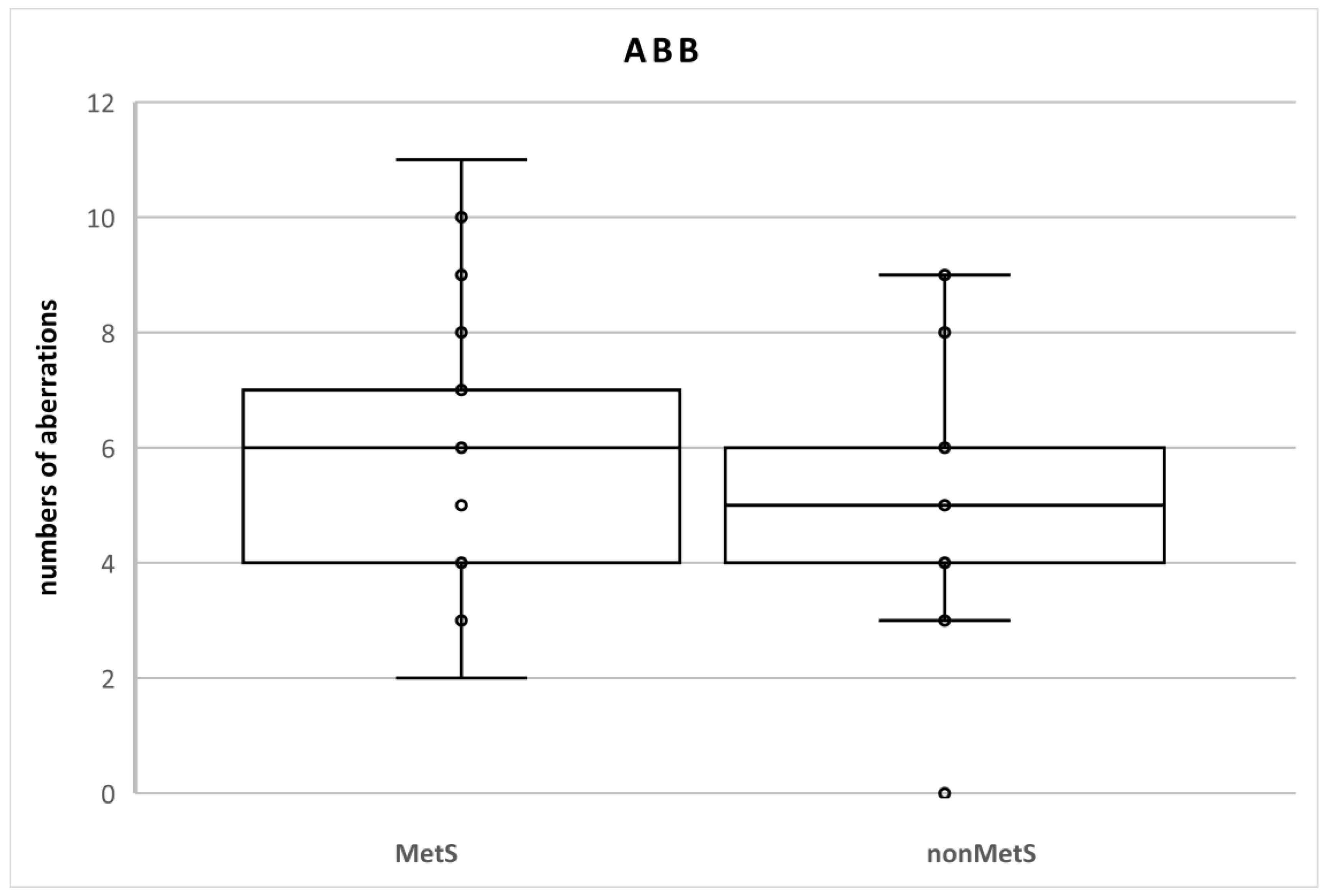
3.3. Chromosomal Aberrations
3.4. Relationships among the Evaluated Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Capon, F. The genetic basis of psoriasis. Int. J. Mol. Sci. 2017, 18, 2526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vičić, M.; Kaštelan, M.; Brajac, I.; Sotošek, V.; Massari, L.P. Current Concepts of Psoriasis Immunopathogenesis. Int. J. Mol. Sci. 2021, 22, 1574. [Google Scholar] [CrossRef]
- Lebwohl, M. Psoriasis. Ann. Intern. Med. 2018, 168, ITC49–ITC64. [Google Scholar] [CrossRef]
- Korman, N.J. Management of psoriasis as a systemic disease: What is the evidence? Br. J. Dermatol. 2020, 182, 840–848. [Google Scholar] [CrossRef]
- Mosca, M.; Hong, J.; Hadeler, E.; Hakimi, M.; Brownstone, N.; Liao, W.; Bhutani, T. Psoriasis and Cardiometabolic Comorbidities: An Evaluation of the Impact of Systemic Treatments in Randomized Clinical Trials. Dermatol. Ther. 2021, 11, 1497–1520. [Google Scholar] [CrossRef]
- De Oliveira, M.; de Oliveira Rocha, B.; Vieira Duarte, G. Psoriasis: Classical and emerging comorbidities. An. Bras. Dermatol. 2015, 90, 9–20. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, A.; Bohannan, B.; Mburu, S.; Alarcon, I.; Kasparek, T.; Toumi, J.; Frade, S.; Barrio, S.F.; Augustin, M. Impact of Psoriatic Disease on Quality of Life: Interim Results of a Global Survey. Dermatol. Ther. 2022, 12, 1055–1064. [Google Scholar] [CrossRef]
- Karas, A.; Holmannova, D.; Borsky, P.; Fiala, Z.; Andrys, C.; Hamakova, K.; Svadlakova, T.; Palicka, V.; Krejsek, J.; Rehacek, V.; et al. Significantly Altered Serum Levels of NAD, AGE, RAGE, CRP, and Elastin as Potential Biomarkers of Psoriasis and Aging—A Case-Control Study. Biomedicines 2022, 10, 1133. [Google Scholar] [CrossRef]
- Grundy, S.M.; Cleeman, J.; Daniels, S.R.; Donato, K.; Eckel, R.H.; Franklin, B.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C.; et al. Diagnosis and management of the metabolic syndrome. Curr. Opin. Cardiol. 2006, 21, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [Green Version]
- Saitoh, S.; van Wijk, K.; Nakajima, O. Crosstalk between metabolic disorders and immune cells. Int. J. Mol. Sci. 2021, 22, 17. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Huang, L.; Lv, P.; Li, X.; Liu, G.; Chen, Y.; Wang, Z.; Qian, X.; Shen, Y.; Li, Y.; et al. The role of Th17 cells in psoriasis. Immunol. Res. 2020, 68, 296–309. [Google Scholar] [CrossRef] [PubMed]
- Chehimi, M.; Vidal, H.; Eljaafari, A. Pathogenic role of il-17-producing immune cells in obesity, and related inflammatory diseases. J. Clin. Med. 2017, 6, 68. [Google Scholar] [CrossRef] [Green Version]
- Salihbegovic, E.M.; Hadzigrahic, N.; Suljagic, E.; Kurtalic, N.; Hadzic, J.; Zejcirovic, A.; Bijedic, M.; Handanagic, A. Psoriasis and Dyslipidemia. Mater. Socio Med. 2015, 27, 15. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, I.; Yoshida, Y.; Suda, M.; Minamino, T. DNA Damage Response and Metabolic Disease. Cell. Metab. 2014, 20, 967–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobrică, E.C.; Cozma, M.A.; Găman, M.A.; Voiculescu, V.M.; Găman, A.M. The Involvement of Oxidative Stress in Psoriasis: A Systematic Review. Antioxidants 2022, 11, 282. [Google Scholar] [CrossRef]
- Abdelazeem, A.H.; Abuelsaad, A.S.A.; Abdel-Moniem, A.; Abdel-Gabbar, M. Association of metabolic syndrome components with alterations in oxidative stress and cytokines expression. J. Taibah Univ. Sci. 2021, 15, 928–940. [Google Scholar] [CrossRef]
- Gorini, F.; Scala, G.; Cooke, M.S.; Majello, B.; Amente, S. Towards a comprehensive view of 8-oxo-7,8-dihydro-2’-deoxyguanosine: Highlighting the intertwined roles of DNA damage and epigenetics in genomic instability. DNA Repair 2021, 97, 103027. [Google Scholar] [CrossRef] [PubMed]
- Niazi, Y.; Thomsen, H.; Smolkova, B.; Vodickova, L.; Vodenkova, S.; Kroupa, M.; Vymetalkova, V.; Kazimirova, A.; Barancokova, M.; Volkovova, K.; et al. DNA repair gene polymorphisms and chromosomal aberrations in healthy, nonsmoking population. DNA Repair 2021, 101, 103079. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.K.; Singh, D.; Dubey, K.; Maurya, R.; Pandey, A.K. Chromosomal aberrations. In Mutagenicity: Assays and Applications; Academic Press: Cambridge, MA, USA, 2017; pp. 69–92. [Google Scholar] [CrossRef]
- Pujol-Canadell, M.; Puig, R.; Armengol, G.; Barrios, L.; Barquinero, J.F. Chromosomal aberration dynamics through the cell cycle. DNA Repair 2020, 89, 102838. [Google Scholar] [CrossRef]
- OECD. Test No. 473: In Vitro Mammalian Chromosomal Aberration Test, OECD Guidelines for the Testing of Chemicals, Section 4; OECD Publishing: Paris, France, 2016. [Google Scholar] [CrossRef]
- Obe, G.; Pfeiffer, P.; Savage, J.; Johannes, C.; Goedecke, W.; Jeppesen, P.; Natarajan, A.; Martínez-López, W.; Folle, G.; Drets, M. Chromosomal aberrations: Formation, identification and distribution. Mutat. Res. Fundam. Mol. Mech. Mutagen. 2002, 504, 17–36. [Google Scholar] [CrossRef]
- Salihbegovic, E.M.; Hadzigrahic, N.; Cickusic, A.J. Psoriasis and metabolic syndrome. Med. Arch. 2015, 69, 85–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorenzo, C.; Williams, K.; Hunt, K.J.; Haffner, S.M. The National Cholesterol Education Program - Adult Treatment Panel III, International Diabetes Federation, and World Health Organization definitions of the metabolic syndrome as predictors of incident cardiovascular disease and diabetes. Diabetes Care 2007, 30, 8–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tichy, A.; Kabacik, S.; O’Brien, G.; Pejchal, J.; Sinkorova, Z.; Kmochova, A.; Sirak, I.; Malkova, A.; Beltran, C.G.; Gonzalez, J.R.; et al. The first in vivo multiparametric comparison of different radiation exposure biomarkers in human blood. PLoS ONE 2018, 13, e0193412. [Google Scholar] [CrossRef] [PubMed]
- Očadlíková, D.; Bavorová, H.; Šmíd, J. Cytogenetická Analýza Periferních Lymfocytů. Acta Hygienica, Epidemiologica et Microbiologica 2007. Available online: http://www.szu.cz/uploads/documents/knihovna_SVI/pdf/2007/full_2007_01.pdf (accessed on 13 October 2021).
- Navab, M.; Reddy, S.T.; Van Lenten, B.J.; Fogelman, A.M. HDL and cardiovascular disease: Atherogenic and atheroprotective mechanisms. Nat. Rev. Cardiol. 2011, 8, 222–232. [Google Scholar] [CrossRef]
- Giammanco, A.; Noto, D.; Barbagallo, C.; Nardi, E.; Caldarella, R.; Ciaccio, M.; Averna, M.; Cefalù, A. Hyperalphalipoproteinemia and beyond: The role of HDL in cardiovascular diseases. Life 2021, 11, 581. [Google Scholar] [CrossRef]
- Namiri-Kalantari, R.; Gao, F.; Chattopadhyay, A.; Wheeler, A.A.; Navab, K.D.; Farias-Eisner, R.; Reddy, S.T. The dual nature of HDL: Anti-Inflammatory and pro-Inflammatory. BioFactors 2015, 41, 153–159. [Google Scholar] [CrossRef]
- Shih, C.M.; Chen, C.C.; Chu, C.K.; Wang, K.H.; Huang, C.Y.; Lee, A.W. The roles of lipoprotein in psoriasis. Int. J. Mol. Sci. 2020, 21, 859. [Google Scholar] [CrossRef] [Green Version]
- Hovland, A.; Retterstøl, K.; Mollnes, T.E.; Halvorsen, B.; Aukrust, P.; Lappegård, K.T. Anti-inflammatory effects of non-statin low-density lipoprotein cholesterol-lowering drugs: An unused potential? Scand. Cardiovasc. J. 2020, 54, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Silva, I.V.G.; De Figueiredo, R.C.; Rios, D.R.A. Effect of different classes of antihypertensive drugs on endothelial function and inflammation. Int. J. Mol. Sci. 2019, 20, 3458. [Google Scholar] [CrossRef] [Green Version]
- Kay, J.; Thadhani, E.; Samson, L.; Engelward, B. Inflammation-induced DNA damage, mutations and cancer. DNA Repair 2019, 83, 102673. [Google Scholar] [CrossRef]
- Kim, M.Y. Intracellular and extracellular factors influencing the genotoxicity of nitric oxide and reactive oxygen species. Oncol. Lett. 2017, 13, 1417–1424. [Google Scholar] [CrossRef] [Green Version]
- Holmannova, D.; Borska, L.; Andrys, C.; Borsky, P.; Kremlacek, J.; Hamakova, K.; Rehacek, V.; Malkova, A.; Svadlakova, T.; Palicka, V.; et al. The Impact of Psoriasis and Metabolic Syndrome on the Systemic Inflammation and Oxidative Damage to Nucleic Acids. J. Immunol. Res. 2020, 2020, 1–9. [Google Scholar] [CrossRef]
- Borska, L.; Kremlacek, J.; Andrys, C.; Krejsek, J.; Hamakova, K.; Borsky, P.; Palicka, V.; Rehacek, V.; Malkova, A.; Fiala, Z. Systemic inflammation, oxidative damage to nucleic acids, and metabolic syndrome in the pathogenesis of psoriasis. Int. J. Mol. Sci. 2017, 18, 2238. [Google Scholar] [CrossRef] [Green Version]
- Durante, M.; Bedford, J.; Chen, D.; Conrad, S.; Cornforth, M.; Natarajan, A.; van Gent, D.; Obe, G. From DNA damage to chromosome aberrations: Joining the break. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2013, 756, 5–13. [Google Scholar] [CrossRef]
- Usman, M.; Woloshynowych, M.; Britto, J.C.; Bilkevic, I.; Glassar, B.; Chapman, S.; Ford-Adams, M.E.; Desai, A.; Bain, M.; Tewfik, I.; et al. Obesity, oxidative DNA damage and vitamin D as predictors of genomic instability in children and adolescents. Int. J. Obes. 2021, 45, 2095–2107. [Google Scholar] [CrossRef]
- Karaman, A.; Aliaǧaoǧlu, C.; Pirim, I. Sister chromatid exchange analysis in patients with psoriasis. Exp. Dermatol. 2008, 17, 524–529. [Google Scholar] [CrossRef]
- Molès, J.-P.; Griez, A.; Guilhou, J.-J.; Girard, C.; Nagot, N.; Van de Perre, P.; Dujols, P. Cytosolic RNA:DNA duplexes generated by endogenous reverse transcriptase activity as autonomous inducers of skin inflammation in psoriasis. PLoS ONE 2017, 12, e0169879. [Google Scholar] [CrossRef]
- Rodríguez-Jiménez, P.; Fernández-Messina, L.; Ovejero-Benito, M.C.; Chicharro, P.; Vera-Tomé, P.; Vara, A.; Cibrian, D.; Martínez-Fleta, P.; Jiménez-Fernández, M.; Sánchez-García, I.; et al. Growth arrest and DNA damage-inducible proteins (GADD45) in psoriasis. Sci Rep. 2021, 11, 1–11. [Google Scholar] [CrossRef]
- Ranna, D.; Andrys, C.; Krejsek, J.; Hamakova, K.; Kremlacek, J.; Fiala, Z.; Borsky, P.; Borska, L. Elevated levels of circulating biomarkers of cell death (nucleosomes) in the patients with plaque psoriasis treated with the Goeckerman regimen. Bratisl. Med. J. 2014, 115, 229–232. [Google Scholar] [CrossRef] [Green Version]
- Malkova, A.; Kohlerova, R.; Fiala, Z.; Hamakova, K.; Selke-Krulichova, I.; Borska, L. Genotoxic changes in peripheral lymphocytes after therapeutic exposure to crude coal tar and ultraviolet radiation. Biomed Pap. 2016, 160, 553–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malkova, A.; Kohlerova, R.; Fiala, Z.; Hamakova, K.; Selke-Krulichova, I.; Borska, L. Structural Chromosome Abnormalities Associated with Obesity: Report of Four New Subjects and Review of Literature. Curr Genomics. 2012, 12, 190–203. [Google Scholar] [CrossRef] [Green Version]
- Franzke, B.; Schwingshackl, L.; Wagner, K.H. Chromosomal damage measured by the cytokinesis block micronucleus cytome assay in diabetes and obesity—A systematic review and meta-analysis. Mutat. Res. Rev. Mutat. Res. 2020, 786, 108343. [Google Scholar] [CrossRef] [PubMed]
- Anand, S.; Nath, B.; Saraswathy, R. Diabetes-increased risk for cancers through chromosomal aberrations? Asian Pac. J. Cancer Prev. 2014, 15, 4571–4573. [Google Scholar] [CrossRef] [Green Version]
- Bankoglu, E.E.; Arnold, C.; Hering, I.; Hankir, M.; Seyfried, F.; Stopper, H. Decreased Chromosomal Damage in Lymphocytes of Obese Patients After Bariatric Surgery. Sci. Rep. 2018, 8, 1–8. [Google Scholar] [CrossRef]
- Fieres, J.; Fischer, M.; Sauter, C.; Moreno-Villanueva, M.; Bürkle, A.; Wirtz, P.H. The burden of overweight: Higher body mass index, but not vital exhaustion, is associated with higher DNA damage and lower DNA repair capacity. DNA Repair 2022, 114, 103323. [Google Scholar] [CrossRef]
- Nagel, G.; Stocks, T.; Späth, D.; Hjartåker, A.; Lindkvist, B.; Hallmans, G.; Jonsson, H.; Bjørge, T.; Manjer, J.; Häggström, C.; et al. Metabolic factors and blood cancers among 578,000 adults in the metabolic syndrome and cancer project (Me-Can). Ann. Hematol. 2012, 91, 1519–1531. [Google Scholar] [CrossRef] [Green Version]
- Esposito, K.; Chiodini, P.; Colao, A.; Lenzi, A.; Giugliano, D. Metabolic syndrome and risk of cancer: A systematic review and meta-analysis. Diabetes Care. 2012, 35, 2402–2411. [Google Scholar] [CrossRef] [Green Version]
- Vaengebjerg, S.; Skov, L.; Egeberg, A.; Loft, N.D. Prevalence, Incidence, and Risk of Cancer in Patients with Psoriasis and Psoriatic Arthritis: A Systematic Review and Meta-analysis. JAMA Dermatol. 2020, 156, 421–429. [Google Scholar] [CrossRef]
- Fuxench, Z.C.C.; Shin, D.B.; Beatty, A.O.; Gelfand, J.M. The risk of cancer in patients with psoriasis a population-based cohort study in the health improvement network. JAMA Dermatol. 2016, 152, 282–290. [Google Scholar] [CrossRef] [Green Version]
- Bellinato, F.; Gisondi, P.; Girolomoni, G. Risk of lymphohematologic malignancies in patients with chronic plaque psoriasis: A systematic review with meta-analysis. J. Am. Acad. Dermatol. 2022, 86, 86–96. [Google Scholar] [CrossRef] [PubMed]
- Borsky, P.; Chmelarova, M.; Fiala, Z.; Hamakova, K.; Palicka, V.; Krejsek, J.; Andrys, C.; Kremlacek, J.; Rehacek, V.; Beranek, M.; et al. Aging in psoriasis vulgaris: Female patients are epigenetically older than healthy controls. Immun. Ageing 2021, 18, 1–10. [Google Scholar] [CrossRef]
- Bonomini, F.; Rodella, L.F.; Rezzani, R. Metabolic Syndrome, Aging and Involvement of Oxidative Stress. Aging Dis. 2015, 6, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gheucă-Solovăstru, L.; Vâţă, D.; Halip, A.I.; Patraşcu, A.; Cozma, A.; Porumb-Andrese, E. Psoriasis—A cancer risk factor? Appl. Sci. 2021, 11, 8366. [Google Scholar] [CrossRef]
- Trafford, A.M.; Parisi, R.; Kontopantelis, E.; Griffiths, C.E.M.; Ashcroft, D.M. Association of Psoriasis with the Risk of Developing or Dying of Cancer: A Systematic Review and Meta-analysis. JAMA Dermatol. 2019, 155, 1390–1403. [Google Scholar] [CrossRef] [Green Version]
- Haverić, A.; Haverić, S.; Ibrulj, S. Chromosome aberrations frequency in peripheral blood lymphocytes in young tobacco smoking and non-smoking people. J. Health Sci. 2016, 6, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Farkas, G.; Kocsis, Z.S.; Székely, G.; Dobozi, M.; Kenessey, I.; Polgár, C.; Jurányi, Z. Smoking, chromosomal aberrations, and cancer incidence in healthy subjects. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2021, 867, 503373. [Google Scholar] [CrossRef]
- Elisia, I.; Lam, V.; Cho, B.; Hay, M.; Li, M.Y.; Yeung, M.; Bu, L.; Jia, W.; Norton, N.; Lam, S.; et al. The effect of smoking on chronic inflammation, immune function and blood cell composition. Sci Rep. 2020, 10, 1–16. [Google Scholar] [CrossRef]
- Tang, M.-S.; Lee, H.-W.; Weng, M.-W.; Wang, H.-T.; Hu, Y.; Chen, L.-C.; Park, S.-H.; Chan, H.-W.; Xu, J.; Wu, X.-R.; et al. DNA damage, DNA repair and carcinogenicity: Tobacco smoke versus electronic cigarette aerosol. Mutat. Res. Mutat. Res. 2022, 789, 108409. [Google Scholar] [CrossRef]
- Salem, A.A.; Trares, K.; Kohl, M.; Jansen, E.; Brenner, H.; Schöttker, B. Long-term effects of smoking on serum concentrations of oxidative stress biomarkers: Results of a large, population-based cohort study. Environ. Res. 2022, 204, 111923. [Google Scholar] [CrossRef]
- Lakhan, S.E.; Kirchgessner, A. Anti-inflammatory effects of nicotine in obesity and ulcerative colitis. J. Transl. Med. 2011, 9, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamaguchi, N.H. Smoking, immunity, and DNA damage. Transl. Lung Cancer Res. 2019, 8 (Suppl. 1), S3–S6. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measured Parameters | Mets; n = 21; nonMetS; n = 20 | Median | Q1–Q3 | p Value |
|---|---|---|---|---|
| Glu mmol/L | MetS | 5.1 | 4.53–6.91 | <0.02 |
| nonMetS | 4.48 | 3.7–4.97 | ||
| Chol mmol/L | MetS | 4.7 | 4.23–5.49 | NS; p = 0.875 |
| nonMetS | 4.77 | 4.2–5.45 | ||
| HDL mmol/L | MetS | 0.91 | 0.83–1.05 | <0.001 |
| nonMetS | 1.27 | 1.09–1.46 | ||
| TAG (mmol/L) | MetS | 1.92 | 1.75–2.66 | <0.001 |
| nonMetS | 1.01 | 0.9–1.46 | ||
| LDL (mmol/L) | MetS (n = 20) | 2.64 | 2.24–3.47 | NS; p = 0.738 |
| nonMetS | 2.92 | 2.17–3.5 | ||
| BMI | MetS | 30.5 | 28.1–32.2 | <0.001 |
| nonMetS | 24.75 | 24.3–28.45 | ||
| Waist (cm) | MetS | 103 | 98–111 | <0.001 |
| nonMetS | 88.5 | 84–98 | ||
| sBP (mmHg) | MetS | 140 | 130–150 | <0.01 |
| nonMetS | 130 | 121–140 | ||
| dBP (mmHg) | MetS | 90 | 88–100 | NS; p = 0.203 |
| nonMetS | 90 | 81–95 | ||
| PASI | MetS | 15.6 | 13.2–30.5 | NS; p = 0.51 |
| nonMetS | 14.7 | 12.15–20.15 | ||
| DoI (years) | MetS | 8 | 4.5–22 | NS; p = 0.815 |
| nonMetS | 10 | 6.25–19.5 |
| Numbers of Analyzed Cells | ABB | SAB | NAB |
|---|---|---|---|
| MetS (2100 cells) | 120 (5.7%) | 116 (5.5%) | 4 (0.2%) |
| nonMetS (2000 cells) | 105 (5.3%) | 105 (5.3%) | 0 |
| Numbers of Patients | ABB | SAB | NAB | |||||
|---|---|---|---|---|---|---|---|---|
| n = 41 | Median | Q1–Q3 | Min, Max | Median | Q1–Q3 | Min, Max | Total Number | p-Value |
| MetS (n = 21) | 6 | 4–7 | 2, 11 | 5 | 4–7 | 2, 11 | 4 | NS, p = 0.70 |
| nonMetS (n = 20) | 5 | 4–6 | 0, 9 | 5 | 4–6 | 0, 9 | 0 | |
| Percentage of Total Aberration | nonMetS n = 20 | MetS n = 21 |
|---|---|---|
| ≥5% ABB | 8 (40%) | 11 (52.4%) |
| ≥10% ABB | 0 (0%) | 2 (9.5%) |
| NAB | 0 (0%) | 3 (19%) (1 person had 2 aberration) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holmannova, D.; Borsky, P.; Andrys, C.; Hamakova, K.; Cermakova, E.; Poctova, G.; Fiala, Z.; Smejkalova, J.; Blaha, V.; Borska, L. Chromosomal Aberrations and Oxidative Stress in Psoriatic Patients with and without Metabolic Syndrome. Metabolites 2022, 12, 688. https://doi.org/10.3390/metabo12080688
Holmannova D, Borsky P, Andrys C, Hamakova K, Cermakova E, Poctova G, Fiala Z, Smejkalova J, Blaha V, Borska L. Chromosomal Aberrations and Oxidative Stress in Psoriatic Patients with and without Metabolic Syndrome. Metabolites. 2022; 12(8):688. https://doi.org/10.3390/metabo12080688
Chicago/Turabian StyleHolmannova, Drahomira, Pavel Borsky, Ctirad Andrys, Kvetoslava Hamakova, Eva Cermakova, Gabriela Poctova, Zdenek Fiala, Jindra Smejkalova, Vladimir Blaha, and Lenka Borska. 2022. "Chromosomal Aberrations and Oxidative Stress in Psoriatic Patients with and without Metabolic Syndrome" Metabolites 12, no. 8: 688. https://doi.org/10.3390/metabo12080688