
Volatile Organic Compounds Frequently Identified after Hyperbaric Hyperoxic Exposure: The VAPOR Library

 , , and
, , and
Abstract
:1. Introduction
2. Results
3. Discussion
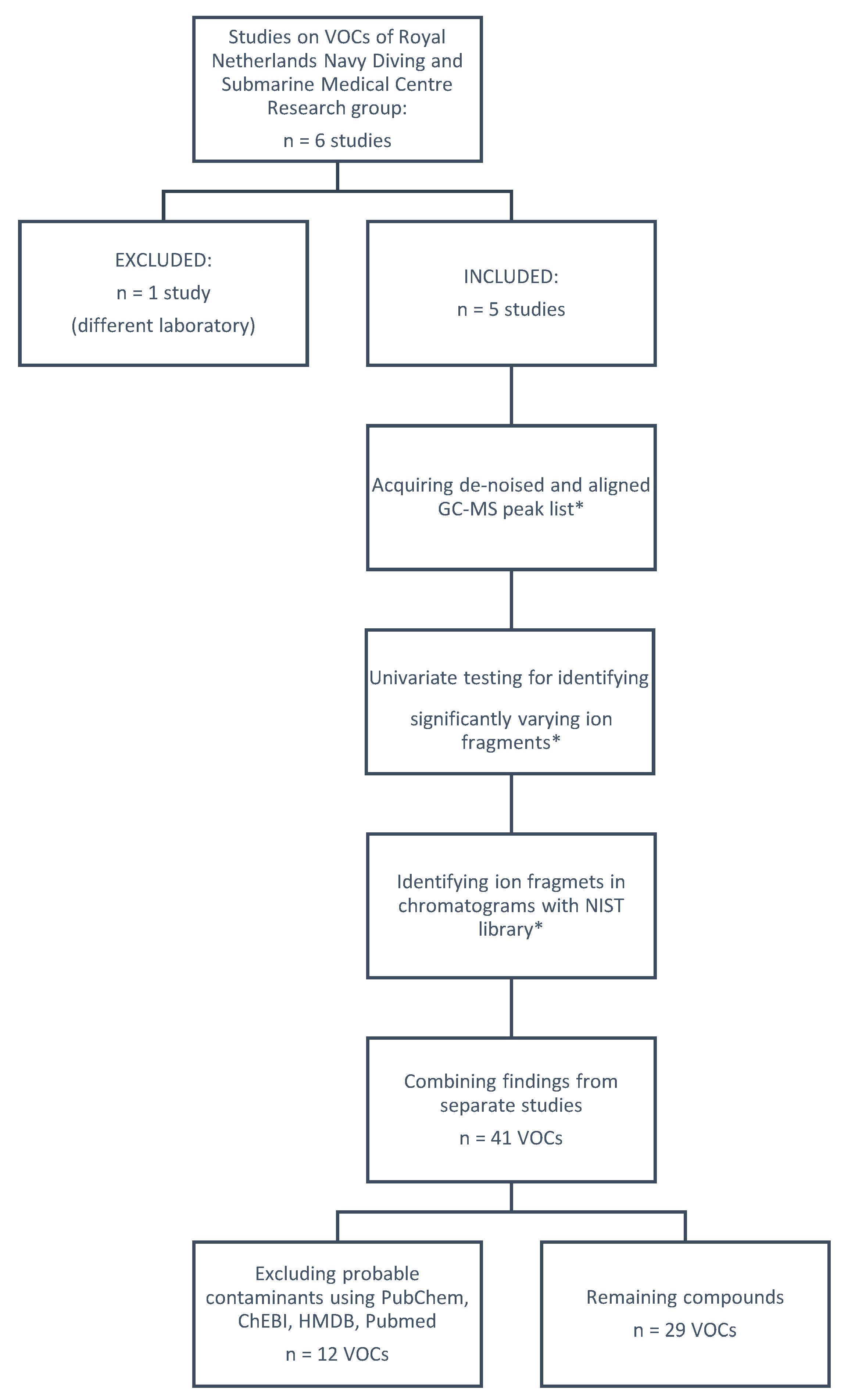
4. Materials and Methods
4.1. Test Subjects and Preparation
4.2. Hyperbaric Hyperoxic Exposure
4.3. Sample Collection and Analysis
4.4. Statistical Methods, Data Analysis, and Identification
4.5. Library Design
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shykoff, B.E.; Lee, R.L. Risks from Breathing Elevated Oxygen. Aerosp. Med. Hum. Perform. 2019, 90, 1041–1049. [Google Scholar] [CrossRef] [PubMed]
- Lorrain Smith, J. The pathological effects due to increase of oxygen tension in the air breathed. J. Physiol. 1899, 24, 19–35. [Google Scholar] [CrossRef] [Green Version]
- Wingelaar, T.T.; van Ooij, P.J.A.M.; van Hulst, R.A. Oxygen Toxicity and Special Operations Forces Diving: Hidden and Dangerous. Front. Physiol. 2017, 8, 1263. [Google Scholar] [CrossRef] [PubMed]
- Thomson, L.; Paton, J. Oxygen Toxicity. Paediatr. Respir. Rev. 2014, 15, 120–123. [Google Scholar] [CrossRef]
- Hafner, S.; Beloncle, F.; Koch, A.; Radermacher, P.; Asfar, P. Hyperoxia in Intensive Care, Emergency, and Peri-Operative Medicine: Dr. Jekyll or Mr. Hyde? A 2015 Update. Ann. Intensive Care 2015, 5, 42. [Google Scholar] [CrossRef] [Green Version]
- Hadanny, A.; Zubari, T.; Tamir-Adler, L.; Bechor, Y.; Fishlev, G.; Lang, E.; Polak, N.; Bergan, J.; Friedman, M.; Efrati, S. Hyperbaric Oxygen Therapy Effects on Pulmonary Functions: A Prospective Cohort Study. BMC Pulm. Med. 2019, 19, 148. [Google Scholar] [CrossRef] [PubMed]
- Van Ooij, P.J.A.M.; Hollmann, M.W.; van Hulst, R.A.; Sterk, P.J. Assessment of Pulmonary Oxygen Toxicity: Relevance to Professional Diving: A Review. Respir. Physiol. Neurobiol. 2013, 189, 117–128. [Google Scholar] [CrossRef]
- Wingelaar, T.T.; van Ooij, P.J.A.M.; Brinkman, P.; Hulst, R.A. van Pulmonary Oxygen Toxicity in Navy Divers: A Crossover Study Using Exhaled Breath Analysis after a One-Hour Air or Oxygen Dive at Nine Meters of Sea Water. Front. Physiol. 2019, 10, 10. [Google Scholar] [CrossRef] [Green Version]
- De Jong, F.; Wingelaar, T.; Brinkman, P.; van Ooij, P.; Maitland-van der Zee, A.; Hollmann, M.; van Hulst, R. Exhaled Breath Analysis on Volatile Organic Compounds after a COMEX-30, 2022; in press.
- De Jong, F.; Wingelaar, T.; Brinkman, P.; van Ooij, P.; Maitland-van der Zee, A.; Hollmann, M.; van Hulst, R. Determining Pulmonary Oxygen Toxicity through Exhaled Breath Markers after a Treatment Table 6. Front. Physiol. 2022, 13, 899568. [Google Scholar] [CrossRef]
- Van Ooij, P.J.A.M.; van Hulst, R.A.; Kulik, W.; Brinkman, P.; Houtkooper, A.; Sterk, P.J. Hyperbaric Oxygen Diving Affects Exhaled Molecular Profiles in Men. Respir. Physiol. Neurobiol. 2014, 198, 20–24. [Google Scholar] [CrossRef]
- Wingelaar, T.T.; Brinkman, P.; van Ooij, P.J.A.M.; Hoencamp, R.; Maitland-van Der Zee, A.H.; Hollmann, M.W.; Hulst, R.A. van Markers of Pulmonary Oxygen Toxicity in Hyperbaric Oxygen Therapy Using Exhaled Breath Analysis. Front. Physiol. 2019, 10, 475. [Google Scholar] [CrossRef] [PubMed]
- Wingelaar, T.T.; Brinkman, P.; Hoencamp, R.; van Ooij, P.-J.A.; Maitland-Van Der Zee, A.-H.; Hollmann, M.W.; van Hulst, R.A. Assessment of Pulmonary Oxygen Toxicity in Special Operations Forces Divers under Operational Circumstances Using Exhaled Breath Analysis. Diving Hyperb Med. 2020, 50, 2–7. [Google Scholar] [CrossRef] [PubMed]
- De Lacy Costello, B.; Amann, A.; Al-Kateb, H.; Flynn, C.; Filipiak, W.; Khalid, T.; Osborne, D.; Ratcliffe, N.M. A Review of the Volatiles from the Healthy Human Body. J. Breath Res. 2014, 8, 014001. [Google Scholar] [CrossRef] [PubMed]
- Drabińska, N.; Flynn, C.; Ratcliffe, N.; Belluomo, I.; Myridakis, A.; Gould, O.; Fois, M.; Smart, A.; Devine, T.; Costello, B.D.L. A Literature Survey of All Volatiles from Healthy Human Breath and Bodily Fluids: The Human Volatilome. J. Breath Res. 2021, 15, 034001. [Google Scholar] [CrossRef] [PubMed]
- Willoughby, C.; Zhou, H.; Mahon, R.; Martin, J.; Dm, F.; Hall, A. Analysis of Volatile Organic Compounds to Predict Hyperbaric Pulmonary Oxygen Toxicity in US Navy Divers; Breath Summit: Leicestershire, UK, 2019. [Google Scholar]
- Barash, O.; Zhang, W.; Halpern, J.M.; Hua, Q.-L.; Pan, Y.-Y.; Kayal, H.; Khoury, K.; Liu, H.; Davies, M.P.A.; Haick, H.; et al. Differentiation between Genetic Mutations of Breast Cancer by Breath Volatolomics. Oncotarget 2015, 6, 44864–44876. [Google Scholar] [CrossRef] [Green Version]
- Filipiak, W.; Ruzsanyi, V.; Mochalski, P.; Filipiak, A.; Bajtarevic, A.; Ager, C.; Denz, H.; Hilbe, W.; Jamnig, H.; Hackl, M.; et al. Dependence of Exhaled Breath Composition on Exogenous Factors, Smoking Habits and Exposure to Air Pollutants. J. Breath Res. 2012, 6, 036008. [Google Scholar] [CrossRef] [Green Version]
- Van Mastrigt, E.; Reyes-Reyes, A.; Brand, K.; Bhattacharya, N.; Urbach, H.P.; Stubbs, A.P.; de Jongste, J.C.; Pijnenburg, M.W. Exhaled Breath Profiling Using Broadband Quantum Cascade Laser-Based Spectroscopy in Healthy Children and Children with Asthma and Cystic Fibrosis. J. Breath Res. 2016, 10, 026003. [Google Scholar] [CrossRef]
- Gruber, M.; Tisch, U.; Jeries, R.; Amal, H.; Hakim, M.; Ronen, O.; Marshak, T.; Zimmerman, D.; Israel, O.; Amiga, E.; et al. Analysis of Exhaled Breath for Diagnosing Head and Neck Squamous Cell Carcinoma: A Feasibility Study. Br. J. Cancer 2014, 111, 790–798. [Google Scholar] [CrossRef] [Green Version]
- Harshman, S.W.; Geier, B.A.; Fan, M.; Rinehardt, S.; Watts, B.S.; Drummond, L.A.; Preti, G.; Phillips, J.B.; Ott, D.K.; Grigsby, C.C. The Identification of Hypoxia Biomarkers from Exhaled Breath under Normobaric Conditions. J. Breath Res. 2015, 9, 047103. [Google Scholar] [CrossRef] [Green Version]
- Blanchet, L.; Smolinska, A.; Baranska, A.; Tigchelaar, E.; Swertz, M.; Zhernakova, A.; Dallinga, J.W.; Wijmenga, C.; van Schooten, F.J. Factors That Influence the Volatile Organic Compound Content in Human Breath. J. Breath Res. 2017, 11, 016013. [Google Scholar] [CrossRef]
- Ayala, A.; Muñoz, M.F.; Argüelles, S. Lipid Peroxidation: Production, Metabolism, and Signaling Mechanisms of Malondialdehyde and 4-Hydroxy-2-Nonenal. Oxidative Med. Cell. Longev. 2014, 2014, 360438. [Google Scholar] [CrossRef] [PubMed]
- Hakim, M.; Broza, Y.Y.; Barash, O.; Peled, N.; Phillips, M.; Amann, A.; Haick, H. Volatile Organic Compounds of Lung Cancer and Possible Biochemical Pathways. Chem. Rev. 2012, 112, 5949–5966. [Google Scholar] [CrossRef] [PubMed]
- Kneepkens, C.M.F.; Lepage, G.; Roy, C.C. The potential of the hydrocarbon breath test as a measure of lipid peroxidation. Free Radic. Biol. Med. 1994, 17, 127–160. [Google Scholar] [CrossRef]
- Gaschler, M.M.; Stockwell, B.R. Lipid Peroxidation in Cell Death. Biochem. Biophys. Res. Commun. 2017, 482, 419–425. [Google Scholar] [CrossRef]
- Harayama, T.; Shimizu, T. Roles of Polyunsaturated Fatty Acids, from Mediators to Membranes. J. Lipid Res. 2020, 61, 1150–1160. [Google Scholar] [CrossRef]
- Phillips, M.; Cataneo, R.N.; Greenberg, J.; Grodman, R.; Gunawardena, R.; Naidu, A. Effect of Oxygen on Breath Markers of Oxidative Stress. Eur. Respir. J. 2003, 21, 48–51. [Google Scholar] [CrossRef] [Green Version]
- Smith, C.A.; Want, E.J.; O’Maille, G.; Abagyan, R.; Siuzdak, G. XCMS: Processing Mass Spectrometry Data for Metabolite Profiling Using Nonlinear Peak Alignment, Matching, and Identification. Anal. Chem. 2006, 78, 779–787. [Google Scholar] [CrossRef]
- SWOD. Keuringsrichtlijn Arbeidsgezondheidskundig Onderzoek Werken Onder Overdruk Duikarbeid. 2021. Available online: https://www.arbocataloguswoo.nl/images/SWOD/pdf/NL/SWOD-ARBOCAT-WoO-Keuring-CAT003_1-2021-rev4-aug-2021.pdf (accessed on 5 April 2022).
- Sola Martínez, R.A.; Pastor Hernández, J.M.; Lozano Terol, G.; Gallego-Jara, J.; García-Marcos, L.; Cánovas Díaz, M.; de Diego Puente, T. Data Preprocessing Workflow for Exhaled Breath Analysis by GC/MS Using Open Sources. Sci. Rep. 2020, 10, 22008. [Google Scholar] [CrossRef]
- CAS Registry. The American Chemical Society (ACS). Available online: https://www.cas.org/ (accessed on 5 April 2022).
- Kim, S.; Chen, J.; Cheng, T.; Gindulyte, A.; He, J.; He, S.; Li, Q.; Shoemaker, B.A.; Thiessen, P.A.; Yu, B.; et al. PubChem in 2021: New Data Content and Improved Web Interfaces. Nucleic Acids Res. 2021, 49, D1388–D1395. [Google Scholar] [CrossRef]
- NIST Chemistry WebBook, SRD 69. The National Institute of Standards and Technology, U.S. Department of Commerce. Available online: https://webbook.nist.gov/chemistry/ (accessed on 16 March 2022).
- Wishart, D.S.; Guo, A.C.; Oler, E.; Wang, F.; Anjum, A.; Peters, H.; Dizon, R.; Sayeeda, Z.; Tian, S.; Lee, B.L.; et al. HMDB 5.0: The Human Metabolome Database for 2022. Nucleic Acids Res. 2022, 50, D622–D631. [Google Scholar] [CrossRef]
- Hastings, J.; Owen, G.; Dekker, A.; Ennis, M.; Kale, N.; Muthukrishnan, V.; Turner, S.; Swainston, N.; Mendes, P.; Steinbeck, C. ChEBI in 2016: Improved Services and an Expanding Collection of Metabolites. Nucleic Acids Res. 2016, 44, D1214–D1219. [Google Scholar] [CrossRef] [PubMed]
- Sayers, E.W.; Bolton, E.E.; Brister, J.R.; Canese, K.; Chan, J.; Comeau, D.C.; Connor, R.; Funk, K.; Kelly, C.; Kim, S.; et al. Database Resources of the National Center for Biotechnology Information. Nucleic Acids Res. 2022, 50, D20–D26. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Name | CAS No. | Molecular Weight | Matching Ion Profiles | References |
|---|---|---|---|---|
| 1,2-Dichloropropane | 78-87-5 | 112 | 1,1-Dichloropropane | [8,9,12] |
| Toluene | 108-88-3 | 92 | 1,3,5-Cycloheptatriene; 2,5-Norbornadiene | [9,13] |
| 4,5-Dimethyl-1,3-dioxane | 1779-22-2 | 116 | 2,6-Dimethyl-1,4-dioxane; 2,5-Dimethyl-1,4-dioxane | [10] |
| Hexamethylcyclotrisiloxane | 541-05-9 | 222 | [8] | |
| Ethylcyclohexane | 1678-91-7 | 112 | [12] | |
| Ethylbenzene | 100-41-4 | 106 | O-Xylene; P-Xylene | [8,13] |
| Hexanenitrile | 628-73-9 | 97 | Heptanonitrile | [10] |
| Cyclohexanone | 108-94-1 | 98 | 2-Methylcyclopentanone | [8] |
| Isopropylbenzene | 98-82-8 | 120 | [8] | |
| 2-Ethyl-1-octene | 51655-64-2 | 140 | 3-Methyl-2-nonene; 3-Methyl-6-methyleneoctane | [8] |
| (Z)-beta-Ocimene | 3338-55-4 | 136 | Trans-Ocimene; Alpha-Ocimene; 3-Isopropenyl-5,5-dimethylcyclopentene | [8] |
| 1-Pentadecene | 13360-61-7 | 210 | [12] |
| Name | CAS No. | Molecular Weight | Matching Ion Profiles | References |
|---|---|---|---|---|
| Isoprene | 78-79-5 | 68 | 1,3-Pentadiene; Ethylidenecyclopropane | [8,10] |
| Hexane | 110-54-3 | 86 | [12,13] | |
| 2,4-Dimethylpentane | 108-08-7 | 100 | iso-Butoxyamine *; Isopentane * | [9,13] |
| Ethyl acetate | 141-78-6 | 88 | 4-Hydroxy-2-butanone *; Ethyl pyruvate *; Methylazoxymethanol acetate * | [9,12] |
| Cyclohexane | 110-82-7 | 84 | Methylcyclopentane; 2-Methyl-1-entene | [8,12,13] |
| Propyl acetate | 109-60-4 | 102 | Isopropyl acetate; Dipropyl sulfite * | [10] |
| Methylcyclohexane | 108-87-2 | 98 | 2,3-Dimethyl-2-pentene *; (E)-3,4-Dimethyl-2-pentene *; (Z)-3,4-Dimethyl-2-pentene *; trans/cis-1-Ethyl-3-Methylcyclopentane * | [8,9,10,12] |
| 3-Methylheptane | 589-81-1 | 114 | 2,4-Dimethylhexane; 3-Ethyl-2-methylhexane | [8,10,12,13] |
| 3-Methyleneheptane | 1632-16-2 | 112 | 3-Methyl-1-heptene *; 2-Ethylhexyl acrylate *; 2-Octene * | [9,10,12] |
| Octane | 111-65-9 | 114 | 2,4-dimethylheptane; Nonane | [8,10,12] |
| Butyl acetate | 123-86-4 | 116 | Isobutyl acetate; Hexyl acetate * | [8,9,10,12] |
| Nonane | 111-84-2 | 128 | 3,4-dimethylheptane; 2-Methylnonane *; Heptane; Decane | [8,9,10,12] |
| 3-Methylnonane | 5911-04-6 | 142 | 2,6-dimethyloctane *; 4-Methyl-1-decene *; 3-Ethyl-5-methylheptane * | [8,10,12,13] |
| 1-Decene | 872-05-9 | 140 | [8,12] | |
| Decane | 124-18-5 | 142 | 2-Methylnonane *; Nonane; 4-Ethyloctane *; Undecane | [8,9,10,12] |
| 2-Butyl-1-octanol | 3913-02-8 | 186 | 2-Methyloctan-1-ol *; 4-Methyl-2-propyl-1-pentanol *; 3,4-Dimethyl-1-decene *; 2,3,5,8-Tetramethyldecane * | [8] |
| 3-[(1,1-Dimethylethoxy)methyl]heptane | 83704-03-4 | 186 | 2,2-Dimethyl-4-decene *; (Z)-, 4-Octanol, propanoate * | [8] |
| 2-Methylundecane | 7045-71-8 | 170 | 4,6,8-Trimethyl-1-nonene *; 2,3,5,8-Tetramethyldecane * | [8,10,12] |
| Undecane | 1120-21-4 | 156 | Decane; Dodecane | [8] |
| 3,7-Dimethyldecane | 17312-54-8 | 170 | 5-butylnonane; Hexadecane | [8] |
| Nonanal | 124-19-6 | 142 | Decanal; Dodecanal; Undecanal *; (E)-2-Nonen-1-ol * | [8,9,10,12] |
| Dodecane | 112-40-3 | 170 | 2-methylundecane; Decane; Tridecane; Undecane; Hexadecane | [8,10,12] |
| Tridecane | 629-50-5 | 184 | 2,3,5,8-Tetramethyldecane; 1-Iodo-2-methylundecane; Dodecane; Pentadecane | [8,9,10,13] |
| Decanal | 112-31-2 | 156 | 1-Nonadecanol *; 1-Eicosanol *; Dodecanal; (E)-2-Decen-1-ol * | [8,9] |
| Tetradecane | 629-59-4 | 198 | 3-Methylundecane; Tridecane; Hexadecane | [8,10,12] |
| 3-Methylundecane | 1002-43-3 | 170 | 2,6,10-Trimethylpentadecane *; 3,5-Dimethyldodecane *; 3-Methyltridecane * | [8,12] |
| Pentadecane | 629-62-9 | 212 | Tridecane; Nonadecane; Dodecane; Tetradecane; Eicosane; Hexadecane | [8,12] |
| Hexadecane | 544-76-3 | 226 | Dodecane; Pentadecane; Tetradecane | [8,12,13] |
| Nonadecane | 629-92-5 | 268 | 5-(2-Methylpropyl)nonane *; 2,6,11-Trimethyldodecane * | [8,13] |
| Characteristics | Matching Ion Profiles | Reference |
|---|---|---|
| Straight-chain alkane; 10–12 carbon molecules | Undecane; Decane; Dodecane | [8] |
| Straight-chain alkane; 11–16 carbon molecules | Dodecane; Tridecane; Hexadecane; Undecane | [8] |
| Straight-chain alkane; 12–16 carbon molecules | Dodecane; Tridecane; Hexadecane | [8] |
| Straight-chain alkane; 12–15 carbon molecules | Pentadecane; Tetradecane; Dodecane | [8] |
| Straight-chain alkane; 15–20 carbon molecules | Eicosane; Hexadecane; Pentadecane | [8] |
| Included Studies | No. of Subjects (No. of Samples) | Hyperbaric Exposure * | Breathing Gas † |
|---|---|---|---|
| Wingelaar TT et al. [8] | 12 (72) | 60 min in-water | 100% O2 (60 min) |
| 193 kPa | |||
| Wingelaar TT et al. [12] | 10 (171) | 10 × 95 min dry | 100% O2 (80 min) |
| 253 kPa | Air ‡ (15 min) | ||
| Wingelaar TT et al. [13] | 4 (12) | 240 min in-water | 100% O2 |
| 132 kPa | |||
| 7 (14) | 180 min in-water | 100% O2 | |
| 132 kPa | |||
| de Jong FJM et al. [10] | 14 (56) | 285 min dry | 100% O2 (240 min) |
| 283 kPa (105 min) 192 kPa (180 min) | Air ‡ (45 min) | ||
| de Jong FJM et al. [9] | 10 (40) | 450 min dry | Heliox 50/50 § (135 min) |
| 405 kPa (90 min) 345 kPa (60 min) 283 kPa (90 min) 192 kPa (210 min) | 100% O2 (255 min) Air ‡ (60 min) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Jong, F.J.M.; Brinkman, P.; Wingelaar, T.T.; van Ooij, P.-J.A.M.; van Hulst, R.A. Volatile Organic Compounds Frequently Identified after Hyperbaric Hyperoxic Exposure: The VAPOR Library. Metabolites 2022, 12, 470. https://doi.org/10.3390/metabo12050470
de Jong FJM, Brinkman P, Wingelaar TT, van Ooij P-JAM, van Hulst RA. Volatile Organic Compounds Frequently Identified after Hyperbaric Hyperoxic Exposure: The VAPOR Library. Metabolites. 2022; 12(5):470. https://doi.org/10.3390/metabo12050470
Chicago/Turabian Stylede Jong, Feiko J. M., Paul Brinkman, Thijs T. Wingelaar, Pieter-Jan A. M. van Ooij, and Rob A. van Hulst. 2022. "Volatile Organic Compounds Frequently Identified after Hyperbaric Hyperoxic Exposure: The VAPOR Library" Metabolites 12, no. 5: 470. https://doi.org/10.3390/metabo12050470