
In Vivo Magnetic Resonance Spectroscopy Methods for Investigating Cardiac Metabolism


Abstract
:1. Myocardial Metabolism in Failing Heart
2. ATP and Phosphocreatine
3. MR Spectroscopy
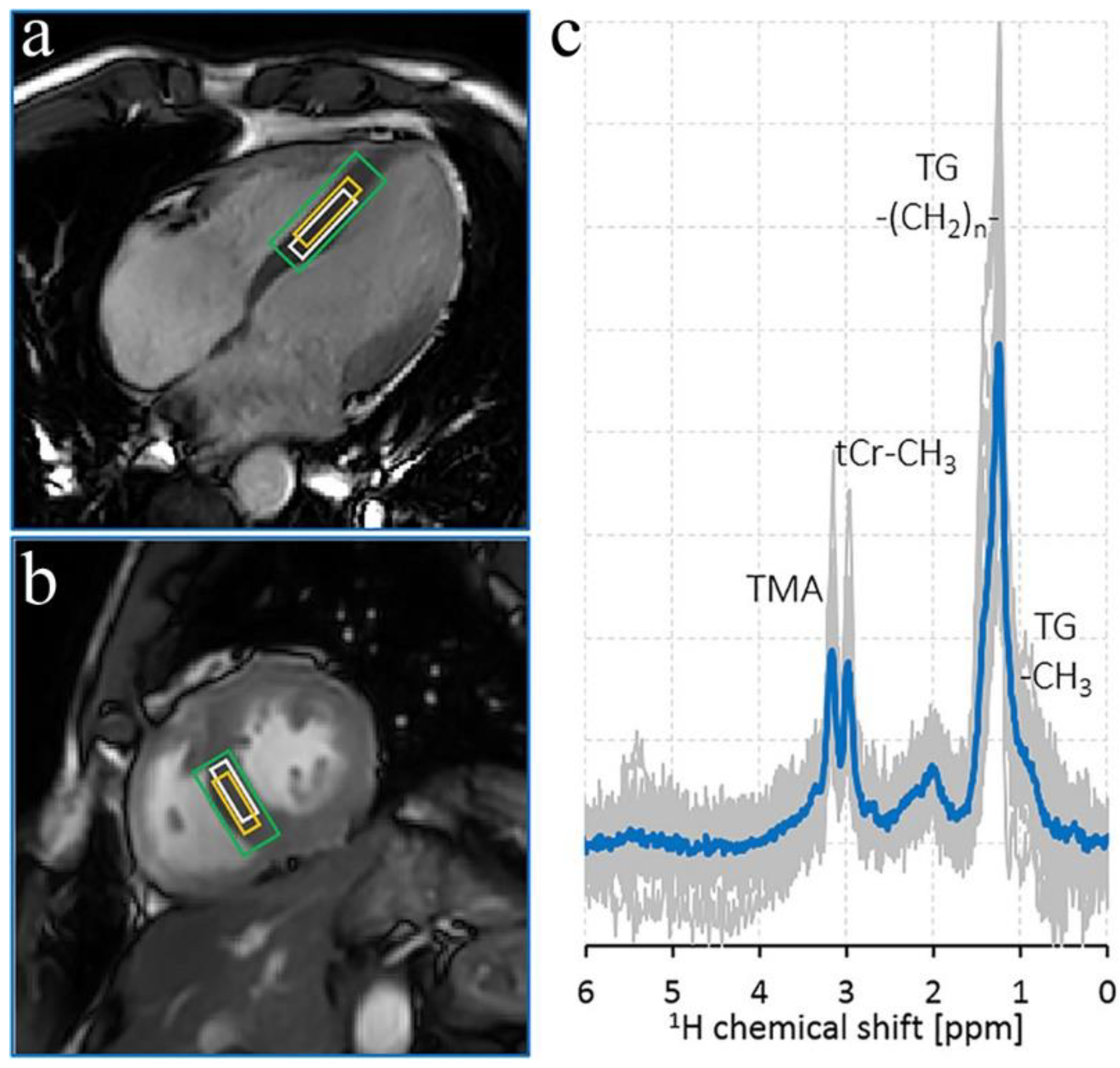
4. Proton Spectroscopy
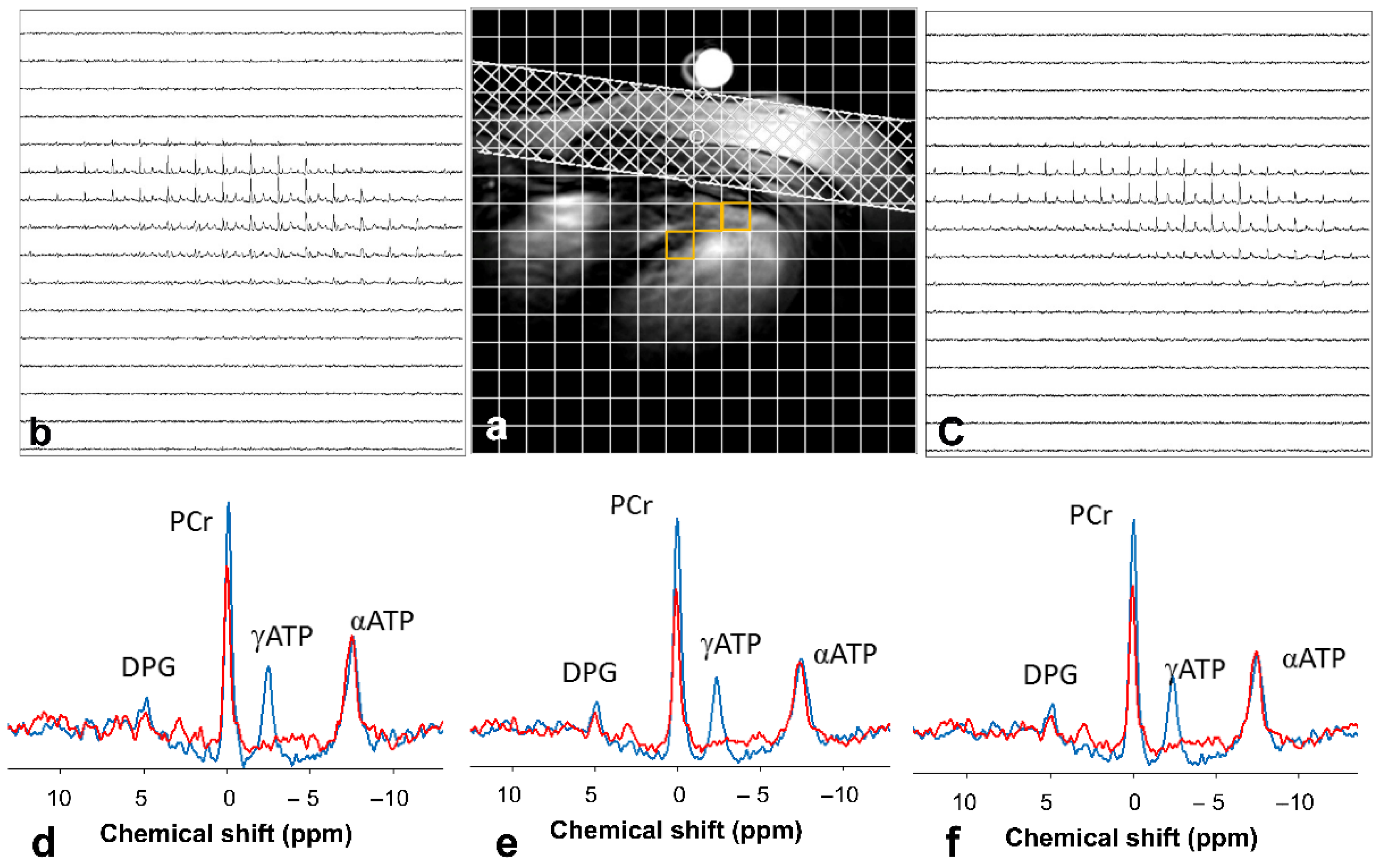
5. Phosphorus Spectroscopy
6. Carbon Spectroscopy
7. Coil and Dynamic Shimming Approaches
8. Summary
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Savarese, G.; Lund, L.H. Global Public Health Burden of Heart Failure. Card Fail. Rev. 2017, 3, 7–11. [Google Scholar] [CrossRef]
- Cowie, M.R.; Simon, M.; Klein, L.; Thokala, P. The cost-effectiveness of real-time pulmonary artery pressure monitoring in heart failure patients: A European perspective. Eur. J. Heart Fail. 2017, 19, 661–669. [Google Scholar] [CrossRef]
- Writing Group, M.; Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Despres, J.P.; et al. Executive Summary: Heart Disease and Stroke Statistics—2016 Update: A Report From the American Heart Association. Circulation 2016, 133, 447–454. [Google Scholar] [CrossRef]
- Neubauer, S. The failing heart--an engine out of fuel. N. Engl. J. Med. 2007, 356, 1140–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertero, E.; Maack, C. Metabolic remodelling in heart failure. Nat. Rev. Cardiol. 2018, 15, 457–470. [Google Scholar] [CrossRef]
- Watson, W.D.; Miller, J.J.J.; Lewis, A.; Neubauer, S.; Tyler, D.; Rider, O.J.; Valkovic, L. Use of cardiac magnetic resonance to detect changes in metabolism in heart failure. Cardiovasc. Diagn. Ther. 2020, 10, 583–597. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.A.; Perry, J.B.; Allen, M.E.; Sabbah, H.N.; Stauffer, B.L.; Shaikh, S.R.; Cleland, J.G.; Colucci, W.S.; Butler, J.; Voors, A.A.; et al. Expert consensus document: Mitochondrial function as a therapeutic target in heart failure. Nat. Rev. Cardiol. 2017, 14, 238–250. [Google Scholar] [CrossRef] [PubMed]
- Ventura-Clapier, R.; Garnier, A.; Veksler, V. Energy metabolism in heart failure. J. Physiol. 2004, 555, 1–13. [Google Scholar] [CrossRef]
- Lopaschuk, G.D.; Karwi, Q.G.; Tian, R.; Wende, A.R.; Abel, E.D. Cardiac Energy Metabolism in Heart Failure. Circ. Res. 2021, 128, 1487–1513. [Google Scholar] [CrossRef]
- Wende, A.R.; Brahma, M.K.; McGinnis, G.R.; Young, M.E. Metabolic Origins of Heart Failure. JACC Basic Transl. Sci. 2017, 2, 297–310. [Google Scholar] [CrossRef]
- Fillmore, N.; Mori, J.; Lopaschuk, G.D. Mitochondrial fatty acid oxidation alterations in heart failure, ischaemic heart disease and diabetic cardiomyopathy. Br. J. Pharm. 2014, 171, 2080–2090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuperman, V. Magnetic Resonance Imaging: Physical Principles and Applications; Academic Press: San Diego, CA, USA; London, UK, 2000; p. xiii. 182p. [Google Scholar]
- De Graaf, R.A. In Vivo NMR Spectroscopy—Principles and Techniques, 2nd ed.; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2007. [Google Scholar]
- Keevil, S.F. Spatial localization in nuclear magnetic resonance spectroscopy. Phys. Med. Biol. 2006, 51, R579–R636. [Google Scholar] [CrossRef] [PubMed]
- Bakermans, A.J.; Boekholdt, S.M.; de Vries, D.K.; Reckman, Y.J.; Farag, E.S.; de Heer, P.; Uthman, L.; Denis, S.W.; Zuurbier, C.J.; Houtkooper, R.H.; et al. Quantification of Myocardial Creatine and Triglyceride Content in the Human Heart: Precision and Accuracy of in vivo Proton Magnetic Resonance Spectroscopy. J. Magn. Reson. Imaging 2021, 54, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Fillmer, A.; Hock, A.; Cameron, D.; Henning, A. Non-Water-Suppressed 1H MR Spectroscopy with Orientational Prior Knowledge Shows Potential for Separating Intra- and Extramyocellular Lipid Signals in Human Myocardium. Sci. Rep. 2017, 7, 16898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, S.; Jiang, H.; Zhuo, C.; Jian, W. Trimethylamine/Trimethylamine-N-Oxide as a Key Between Diet and Cardiovascular Diseases. Cardiovasc. Toxicol. 2021, 21, 593–604. [Google Scholar] [CrossRef] [PubMed]
- Khedr, D.; Hafez, M.; Lumpuy-Castillo, J.; Emam, S.; Abdel-Massih, A.; Elmougy, F.; Elkaffas, R.; Mahillo-Fernandez, I.; Lorenzo, O.; Musa, N. Lipid Biomarkers as Predictors of Diastolic Dysfunction in Diabetes with Poor Glycemic Control. Int. J. Mol. Sci. 2020, 21, 5079. [Google Scholar] [CrossRef]
- Secchi, F.; Di Leo, G.; Petrini, M.; Spairani, R.; Ali, M.; Guazzi, M.; Sardanelli, F. 1H- and 31P-myocardial magnetic resonance spectroscopy in non-obstructive hypertrophic cardiomyopathy patients and competitive athletes. Radiol. Med. 2017, 122, 265–272. [Google Scholar] [CrossRef]
- Sourdon, J.; Roussel, T.; Costes, C.; Viout, P.; Guye, M.; Ranjeva, J.P.; Bernard, M.; Kober, F.; Rapacchi, S. Comparison of single-voxel 1H-cardiovascular magnetic resonance spectroscopy techniques for in vivo measurement of myocardial creatine and triglycerides at 3T. J. Cardiovasc. Magn. Reson. 2021, 23, 53. [Google Scholar] [CrossRef]
- Ding, B.; Peterzan, M.; Mozes, F.E.; Rider, O.J.; Valkovic, L.; Rodgers, C.T. Water-suppression cycling 3-T cardiac 1H-MRS detects altered creatine and choline in patients with aortic or mitral stenosis. NMR Biomed. 2021, 34, e4513. [Google Scholar] [CrossRef]
- Kramer, C.M.; Barkhausen, J.; Bucciarelli-Ducci, C.; Flamm, S.D.; Kim, R.J.; Nagel, E. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. J. Cardiovasc. Magn. Reson. 2020, 22, 17. [Google Scholar] [CrossRef]
- Kording, F.; Yamamura, J.; Lund, G.; Ueberle, F.; Jung, C.; Adam, G.; Schoennagel, B.P. Doppler Ultrasound Triggering for Cardiovascular MRI at 3T in a Healthy Volunteer Study. Magn. Reson. Med. Sci. 2017, 16, 98–108. [Google Scholar] [CrossRef] [Green Version]
- Peereboom, S.M.; Gastl, M.; Fuetterer, M.; Kozerke, S. Navigator-free metabolite-cycled proton spectroscopy of the heart. Magn. Reson. Med. 2020, 83, 795–805. [Google Scholar] [CrossRef]
- Near, J.; Harris, A.D.; Juchem, C.; Kreis, R.; Marjanska, M.; Oz, G.; Slotboom, J.; Wilson, M.; Gasparovic, C. Preprocessing, analysis and quantification in single-voxel magnetic resonance spectroscopy: Experts’ consensus recommendations. NMR Biomed. 2021, 34, e4257. [Google Scholar] [CrossRef]
- Valkovic, L.; Clarke, W.T.; Schmid, A.I.; Raman, B.; Ellis, J.; Watkins, H.; Robson, M.D.; Neubauer, S.; Rodgers, C.T. Measuring inorganic phosphate and intracellular pH in the healthy and hypertrophic cardiomyopathy hearts by in vivo 7T 31P-cardiovascular magnetic resonance spectroscopy. J. Cardiovasc. Magn. Reson. 2019, 21, 19. [Google Scholar] [CrossRef] [Green Version]
- Rata, M.; Giles, S.L.; deSouza, N.M.; Leach, M.O.; Payne, G.S. Comparison of three reference methods for the measurement of intracellular pH using 31P MRS in healthy volunteers and patients with lymphoma. NMR Biomed. 2014, 27, 158–162. [Google Scholar] [CrossRef]
- Rodgers, C.T.; Clarke, W.T.; Snyder, C.; Vaughan, J.T.; Neubauer, S.; Robson, M.D. Human cardiac 31P magnetic resonance spectroscopy at 7 Tesla. Magn. Reson. Med. 2014, 72, 304–315. [Google Scholar] [CrossRef]
- Ellis, J.; Valkovic, L.; Purvis, L.A.B.; Clarke, W.T.; Rodgers, C.T. Reproducibility of human cardiac phosphorus MRS (31P-MRS) at 7 T. NMR Biomed. 2019, 32, e4095. [Google Scholar] [CrossRef] [Green Version]
- Shi, M.; Ellingsen, O.; Bathen, T.F.; Hoydal, M.A.; Stolen, T.; Esmaeili, M. The Effect of Exercise Training on Myocardial and Skeletal Muscle Metabolism by MR Spectroscopy in Rats with Heart Failure. Metabolites 2019, 9, 53. [Google Scholar] [CrossRef] [Green Version]
- Stolen, T.; Shi, M.; Wohlwend, M.; Hoydal, M.A.; Bathen, T.F.; Ellingsen, O.; Esmaeili, M. Effect of exercise training on cardiac metabolism in rats with heart failure. Scand. Cardiovasc. J. 2020, 54, 84–91. [Google Scholar] [CrossRef]
- Valkovic, L.; Chmelik, M.; Krssak, M. In-vivo 31P-MRS of skeletal muscle and liver: A way for non-invasive assessment of their metabolism. Anal. Biochem. 2017, 529, 193–215. [Google Scholar] [CrossRef]
- Kemp, G.J.; Ahmad, R.E.; Nicolay, K.; Prompers, J.J. Quantification of skeletal muscle mitochondrial function by 31P magnetic resonance spectroscopy techniques: A quantitative review. Acta Physiol. 2015, 213, 107–144. [Google Scholar] [CrossRef]
- Gabr, R.E.; El-Sharkawy, A.M.; Schar, M.; Panjrath, G.S.; Gerstenblith, G.; Weiss, R.G.; Bottomley, P.A. Cardiac work is related to creatine kinase energy supply in human heart failure: A cardiovascular magnetic resonance spectroscopy study. J. Cardiovasc. Magn. Reson. 2018, 20, 81. [Google Scholar] [CrossRef] [Green Version]
- Bashir, A.; Zhang, J.; Denney, T.S. Creatine kinase rate constant in the human heart at 7T with 1D-ISIS/2D CSI localization. PLoS ONE 2020, 15, e0229933. [Google Scholar] [CrossRef] [Green Version]
- Clarke, W.T.; Robson, M.D.; Neubauer, S.; Rodgers, C.T. Creatine kinase rate constant in the human heart measured with 3D-localization at 7 tesla. Magn. Reson. Med. 2017, 78, 20–32. [Google Scholar] [CrossRef]
- van Ewijk, P.A.; Schrauwen-Hinderling, V.B.; Bekkers, S.C.; Glatz, J.F.; Wildberger, J.E.; Kooi, M.E. MRS: A noninvasive window into cardiac metabolism. NMR Biomed. 2015, 28, 747–766. [Google Scholar] [CrossRef]
- Sourdon, J.; Lewsey, S.C.; Schar, M.; Weiss, R.G. Measuring Myocardial Energetics with Cardiovascular Magnetic Resonance Spectroscopy. Heart Fail. Clin. 2021, 17, 149–156. [Google Scholar] [CrossRef]
- Dass, S.; Holloway, C.J.; Cochlin, L.E.; Rider, O.J.; Mahmod, M.; Robson, M.; Sever, E.; Clarke, K.; Watkins, H.; Ashrafian, H.; et al. No Evidence of Myocardial Oxygen Deprivation in Nonischemic Heart Failure. Circ. Heart Fail. 2015, 8, 1088–1093. [Google Scholar] [CrossRef]
- Bayeva, M.; Gheorghiade, M.; Ardehali, H. Mitochondria as a therapeutic target in heart failure. J. Am. Coll. Cardiol. 2013, 61, 599–610. [Google Scholar] [CrossRef] [Green Version]
- Mahmod, M.; Pal, N.; Rayner, J.; Holloway, C.; Raman, B.; Dass, S.; Levelt, E.; Ariga, R.; Ferreira, V.; Banerjee, R.; et al. The interplay between metabolic alterations, diastolic strain rate and exercise capacity in mild heart failure with preserved ejection fraction: A cardiovascular magnetic resonance study. J. Cardiovasc. Magn. Reson. 2018, 20, 88. [Google Scholar] [CrossRef]
- Qureshi, W.T.; Nasir, U.B. Principals and clinical applications of magnetic resonance cardiac spectroscopy in heart failure. Heart Fail. Rev. 2017, 22, 491–499. [Google Scholar] [CrossRef]
- Del Franco, A.; Ambrosio, G.; Baroncelli, L.; Pizzorusso, T.; Barison, A.; Olivotto, I.; Recchia, F.A.; Lombardi, C.M.; Metra, M.; Ferrari Chen, Y.F.; et al. Creatine deficiency and heart failure. Heart Fail. Rev. 2021. [Google Scholar] [CrossRef]
- Meyers, T.A.; Townsend, D. Cardiac Pathophysiology and the Future of Cardiac Therapies in Duchenne Muscular Dystrophy. Int. J. Mol. Sci. 2019, 20, 4098. [Google Scholar] [CrossRef] [Green Version]
- Hock, M.; Terekhov, M.; Stefanescu, M.R.; Lohr, D.; Herz, S.; Reiter, T.; Ankenbrand, M.; Kosmala, A.; Gassenmaier, T.; Juchem, C.; et al. B0 shimming of the human heart at 7T. Magn. Reson. Med. 2021, 85, 182–196. [Google Scholar] [CrossRef]
- Darnell, D.; Truong, T.K.; Song, A.W. Recent Advances in Radio-Frequency Coil Technologies: Flexible, Wireless, and Integrated Coil Arrays. J. Magn. Reson. Imaging 2021. [Google Scholar] [CrossRef]
- Josan, S.; Park, J.M.; Hurd, R.; Yen, Y.F.; Pfefferbaum, A.; Spielman, D.; Mayer, D. In vivo investigation of cardiac metabolism in the rat using MRS of hyperpolarized [1-13C] and [2-13C]pyruvate. NMR Biomed. 2013, 26, 1680–1687. [Google Scholar] [CrossRef] [Green Version]
- Ardenkjaer-Larsen, J.H.; Fridlund, B.; Gram, A.; Hansson, G.; Hansson, L.; Lerche, M.H.; Servin, R.; Thaning, M.; Golman, K. Increase in signal-to-noise ratio of >10,000 times in liquid-state NMR. Proc. Natl. Acad. Sci. USA 2003, 100, 10158–10163. [Google Scholar] [CrossRef] [Green Version]
- Stanley, W.C.; Recchia, F.A.; Lopaschuk, G.D. Myocardial substrate metabolism in the normal and failing heart. Physiol. Rev. 2005, 85, 1093–1129. [Google Scholar] [CrossRef]
- Schroeder, M.A.; Lau, A.Z.; Chen, A.P.; Gu, Y.; Nagendran, J.; Barry, J.; Hu, X.; Dyck, J.R.; Tyler, D.J.; Clarke, K.; et al. Hyperpolarized 13C magnetic resonance reveals early- and late-onset changes to in vivo pyruvate metabolism in the failing heart. Eur. J. Heart Fail. 2013, 15, 130–140. [Google Scholar] [CrossRef] [Green Version]
- Sharma, G.; Wu, C.Y.; Wynn, R.M.; Gui, W.; Malloy, C.R.; Sherry, A.D.; Chuang, D.T.; Khemtong, C. Real-time hyperpolarized 13C magnetic resonance detects increased pyruvate oxidation in pyruvate dehydrogenase kinase 2/4-double knockout mouse livers. Sci. Rep. 2019, 9, 16480. [Google Scholar] [CrossRef]
- Befroy, D.E.; Falk Petersen, K.; Rothman, D.L.; Shulman, G.I. Assessment of in vivo mitochondrial metabolism by magnetic resonance spectroscopy. Methods Enzym. 2009, 457, 373–393. [Google Scholar] [CrossRef] [Green Version]
- Bankson, J.A.; Walker, C.M.; Ramirez, M.S.; Stefan, W.; Fuentes, D.; Merritt, M.E.; Lee, J.; Sandulache, V.C.; Chen, Y.; Phan, L.; et al. Kinetic Modeling and Constrained Reconstruction of Hyperpolarized [1-13C]-Pyruvate Offers Improved Metabolic Imaging of Tumors. Cancer Res. 2015, 75, 4708–4717. [Google Scholar] [CrossRef] [Green Version]
- Witney, T.H.; Kettunen, M.I.; Brindle, K.M. Kinetic modeling of hyperpolarized 13C label exchange between pyruvate and lactate in tumor cells. J. Biol. Chem. 2011, 286, 24572–24580. [Google Scholar] [CrossRef] [Green Version]
- Schroeder, M.A.; Atherton, H.J.; Ball, D.R.; Cole, M.A.; Heather, L.C.; Griffin, J.L.; Clarke, K.; Radda, G.K.; Tyler, D.J. Real-time assessment of Krebs cycle metabolism using hyperpolarized 13C magnetic resonance spectroscopy. FASEB J. 2009, 23, 2529–2538. [Google Scholar] [CrossRef] [Green Version]
- Schroeder, M.A.; Swietach, P.; Atherton, H.J.; Gallagher, F.A.; Lee, P.; Radda, G.K.; Clarke, K.; Tyler, D.J. Measuring intracellular pH in the heart using hyperpolarized carbon dioxide and bicarbonate: A 13C and 31P magnetic resonance spectroscopy study. Cardiovasc. Res. 2010, 86, 82–91. [Google Scholar] [CrossRef] [Green Version]
- Fuetterer, M.; Busch, J.; Traechtler, J.; Wespi, P.; Peereboom, S.M.; Sauer, M.; Lipiski, M.; Fleischmann, T.; Cesarovic, N.; Stoeck, C.T.; et al. Quantitative myocardial first-pass cardiovascular magnetic resonance perfusion imaging using hyperpolarized [1-13C] pyruvate. J. Cardiovasc. Magn. Reson. 2018, 20, 73. [Google Scholar] [CrossRef]
- Fuetterer, M.; Busch, J.; Peereboom, S.M.; von Deuster, C.; Wissmann, L.; Lipiski, M.; Fleischmann, T.; Cesarovic, N.; Stoeck, C.T.; Kozerke, S. Hyperpolarized 13C urea myocardial first-pass perfusion imaging using velocity-selective excitation. J. Cardiovasc. Magn. Reson. 2017, 19, 46. [Google Scholar] [CrossRef] [Green Version]
- Niendorf, T.; Schulz-Menger, J.; Paul, K.; Huelnhagen, T.; Ferrari, V.A.; Hodge, R. High Field Cardiac Magnetic Resonance Imaging: A Case for Ultrahigh Field Cardiac Magnetic Resonance. Circ. Cardiovasc. Imaging 2017, 10, e005460. [Google Scholar] [CrossRef] [Green Version]
- Elabyad, I.A.; Terekhov, M.; Stefanescu, M.R.; Lohr, D.; Fischer, M.; Schreiber, L.M. Design of a novel antisymmetric coil array for parallel transmit cardiac MRI in pigs at 7T. J. Magn. Reson. 2019, 305, 195–208. [Google Scholar] [CrossRef]
- Steensma, B.R.; Voogt, I.J.; Leiner, T.; Luijten, P.R.; Habets, J.; Klomp, D.W.J.; van den Berg, C.A.T.; Raaijmakers, A.J.E. An 8-channel Tx/Rx dipole array combined with 16 Rx loops for high-resolution functional cardiac imaging at 7 T. MAGMA 2018, 31, 7–18. [Google Scholar] [CrossRef] [Green Version]
- Stockmann, J.P.; Wald, L.L. In vivo B0 field shimming methods for MRI at 7T. Neuroimage 2018, 168, 71–87. [Google Scholar] [CrossRef] [Green Version]
- Edalati, M.; Zheng, Y.; Watkins, M.P.; Chen, J.; Liu, L.; Zhang, S.; Song, Y.; Soleymani, S.; Lenihan, D.J.; Lanza, G.M. Implementation and prospective clinical validation of AI-based planning and shimming techniques in cardiac MRI. Med. Phys. 2021, 49, 129–143. [Google Scholar] [CrossRef] [PubMed]
- Schar, M.; Vonken, E.J.; Stuber, M. Simultaneous B0- and B1+-map acquisition for fast localized shim, frequency, and RF power determination in the heart at 3 T. Magn. Reson. Med. 2010, 63, 419–426. [Google Scholar] [CrossRef] [Green Version]
- Curtis, A.T.; Gilbert, K.M.; Klassen, L.M.; Gati, J.S.; Menon, R.S. Slice-by-slice B1+ shimming at 7 T. Magn. Reson. Med. 2012, 68, 1109–1116. [Google Scholar] [CrossRef] [PubMed]
- Elabyad, I.A.; Terekhov, M.; Lohr, D.; Stefanescu, M.R.; Baltes, S.; Schreiber, L.M. A Novel Mono-surface Antisymmetric 8Tx/16Rx Coil Array for Parallel Transmit Cardiac MRI in Pigs at 7T. Sci. Rep. 2020, 10, 3117. [Google Scholar] [CrossRef] [Green Version]
- Stockmann, J.P.; Arango, N.S.; Witzel, T.; Mareyam, A.; Sappo, C.; Zhou, J.; Jenkins, L.; Craven-Brightman, L.; Milshteyn, E.; Davids, M.; et al. A 31-channel integrated “AC/DC” B0 shim and radiofrequency receive array coil for improved 7T MRI. Magn. Reson. Med. 2022, 87, 1074–1092. [Google Scholar] [CrossRef]
- Esmaeili, M.; Stockmann, J.; Strasser, B.; Arango, N.; Thapa, B.; Wang, Z.; van der Kouwe, A.; Dietrich, J.; Cahill, D.P.; Batchelor, T.T.; et al. An integrated RF-receive/B0-shim array coil boosts performance of whole-brain MR spectroscopic imaging at 7 T. Sci. Rep. 2020, 10, 15029. [Google Scholar] [CrossRef]
- Eigentler, T.W.; Kuehne, A.; Boehmert, L.; Dietrich, S.; Els, A.; Waiczies, H.; Niendorf, T. 32-Channel self-grounded bow-tie transceiver array for cardiac MR at 7.0T. Magn. Reson. Med. 2021, 86, 2862–2879. [Google Scholar] [CrossRef]
- Xiang, S.F.; Zhang, X.Q.; Yang, S.J.; Gao, Y.Y.; Gao, B.L.; Shi, Q.L.; Li, S. Intravoxel Incoherent Motion Magnetic Resonance Imaging with Integrated Slice-specific Shimming for old myocardial infarction: A Pilot Study. Sci. Rep. 2019, 9, 19766. [Google Scholar] [CrossRef]
- Roat, S.; Vít, M.; Wampl, S.; Schmid, A.I.; Laistler, E. A Flexible Array for Cardiac 31P MR Spectroscopy at 7 T. Front. Phys. 2020, 8, 92. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nuclei | Metabolites | Significance |
|---|---|---|
| Proton (1H) | Creatine, triglyceride, lipid | Lipid and creatine pools within the myocytes |
| Phosphorus (31P) | Adenosine tri phosphate (ATP); phosphocreatine (PCr); PCr/ATP ratio, pHi | Bioenergetics metabolites, intracellular pH measurements |
| Carbon (13C) | Glucose, lactate, pyruvate, fatty acids, lipid | Probe TCA cycle metabolism, pyruvate dehydrogenase, glycolysis, fatty acid metabolism |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esmaeili, M.; Vettukattil, R. In Vivo Magnetic Resonance Spectroscopy Methods for Investigating Cardiac Metabolism. Metabolites 2022, 12, 189. https://doi.org/10.3390/metabo12020189
Esmaeili M, Vettukattil R. In Vivo Magnetic Resonance Spectroscopy Methods for Investigating Cardiac Metabolism. Metabolites. 2022; 12(2):189. https://doi.org/10.3390/metabo12020189
Chicago/Turabian StyleEsmaeili, Morteza, and Riyas Vettukattil. 2022. "In Vivo Magnetic Resonance Spectroscopy Methods for Investigating Cardiac Metabolism" Metabolites 12, no. 2: 189. https://doi.org/10.3390/metabo12020189