
Impact of Metabolomics Technologies on the Assessment of Peritoneal Membrane Profiles in Peritoneal Dialysis Patients: A Systematic Review

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. General Information and Literature Search Strategy
2.2. Information Sources and Search Strategy
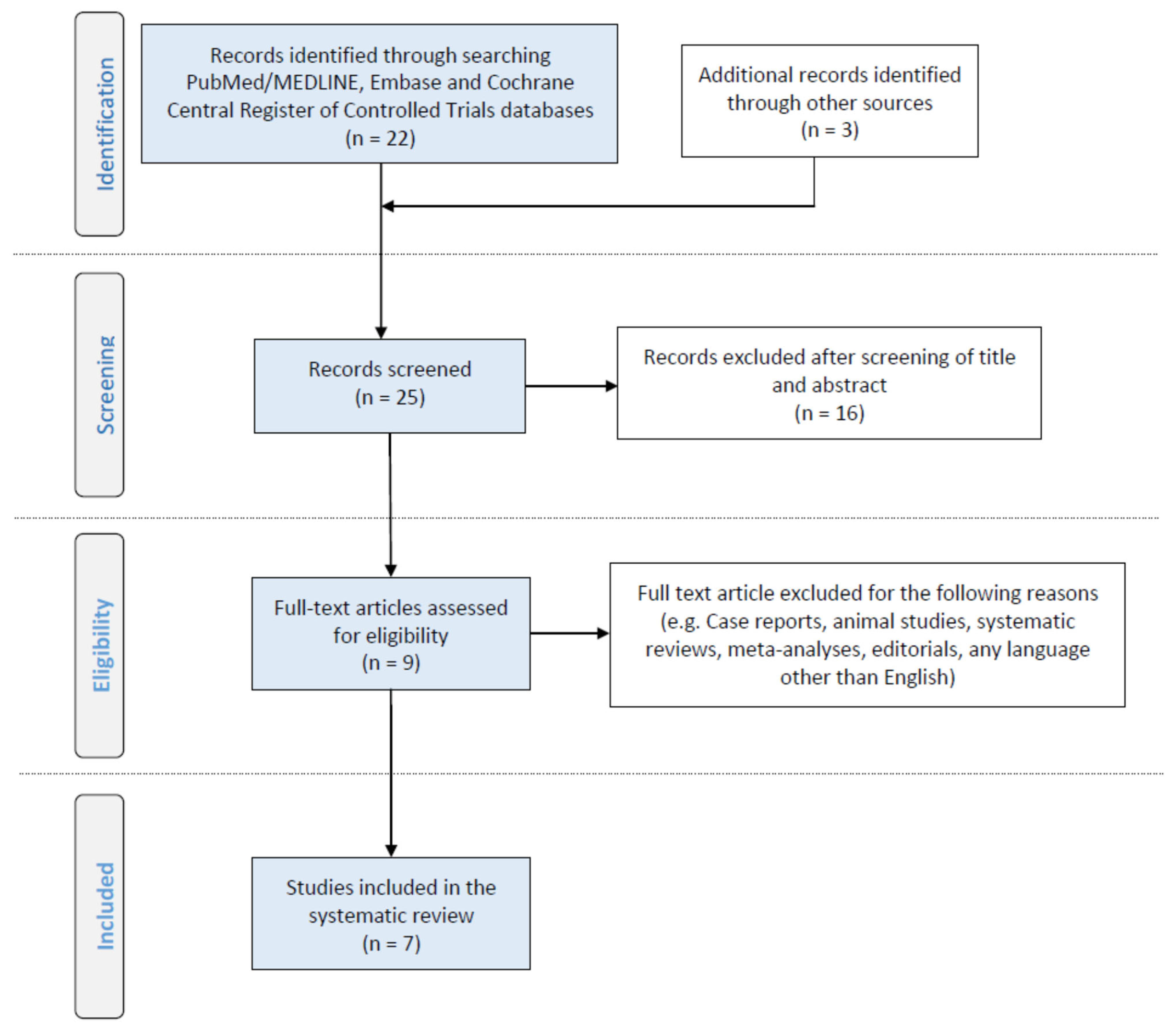
2.3. Study Selection
2.4. Data Extraction
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PDE | peritoneal dialysis effluent |
| PM | peritoneal membrane |
| NPH | normal phase |
| RPH | reversed phase |
| LC | liquid chromatography |
| TOF | time of flight |
| UHPLC | ultra-high-pressure liquid chromatography |
| GC | gas chromatography |
| MS | mass spectroscopy |
| NMR | nuclear magnetic resonance |
| CE | capillary electrophoresis |
| FIA | flow injection analysis |
References
- Gajardo, M.; Cano, F. ABC de la diálisis peritoneal en pediatría [ABC of the peritoneal dialysis in pediatrics]. Rev. Chil. Pediatr. 2020, 91, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Devuyst, O.; Goffin, E. Water and solute transport in peritoneal dialysis: Models and clinical applications. Nephrol. Dial. Transplant. 2008, 23, 2120–2123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krediet, R.T.; Struijk, D.G. Peritoneal changes in patients on long-term peritoneal dialysis. Nat. Rev. Nephrol. 2013, 9, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Mihalache, O.; Bugă, C.; Doran, H.; Catrina, E.; Bobircă, F.; Pătrașcu, T. Encapsulating peritoneal sclerosis—A rare and serious complication of peritoneal dialysis: Case series. J. Med. Life. 2014, 7, 8–12. [Google Scholar]
- Tseng, C.C.; Chen, J.B.; Wang, I.K.; Liao, S.C.; Cheng, B.C.; Wu, A.B.; Chang, Y.T.; Hung, S.Y.; Huang, C.C. Incidence and outcomes of encapsulating peritoneal sclerosis (EPS) and factors associated with severe EPS. PLoS ONE 2018, 13, e0190079. [Google Scholar] [CrossRef] [Green Version]
- Danford, C.J.; Lin, S.C.; Smith, M.P.; Wolf, J.L. Encapsulating peritoneal sclerosis. World J. Gastroenterol. 2018, 24, 3101–3111. [Google Scholar] [CrossRef]
- Nakamoto, H. Encapsulating peritoneal sclerosis—A clinician’s approach to diagnosis and medical treatment. Perit. Dial. Int. 2005, 25, S30–S38. [Google Scholar] [CrossRef]
- Angela, M.; Summers, A.M.; Clancy, M.J.; Syed, F.; Harwood, N.; Brenchley, P.E.; Augustine, T.; Riad, H.; Hutchison, A.J.; Taylor, P.; et al. Single-center experience of encapsulating peritoneal sclerosis in patients on peritoneal dialysis for end-stage renal failure. Kidney Int. 2005, 68, 2381–2388. [Google Scholar]
- Balzer, M.S. Molecular pathways in peritoneal fibrosis. Cell Signal. 2020, 75, 109778. [Google Scholar] [CrossRef]
- Oh, K.H.; Jung, J.Y.; Yoon, M.O.; Song, A.; Lee, H.; Ro, H.; Hwang, Y.-H.; Kim, D.K.; Margetts, P.; Ahn, C. Intra-peritoneal interleukin-6 system is a potent determinant of the baseline peritoneal solute transport inincident peritoneal dialysis patients. Nephrol. Dial. Transplant. 2010, 25, 1639–1646. [Google Scholar] [CrossRef] [Green Version]
- Witowski, J.; Kamhieh-Milz, J.; Kawka, E.; Catar, R.; Jörres, A. IL-17 in Peritoneal Dialysis-Associated Inflammation and Angiogenesis: Conclusions and Perspectives. Front. Physiol. 2018, 9, 1694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Felmeden, D.C.; Blann, A.D.; Lip, G.Y.H. Angiogenesis: Basic pathophysiology and implications for disease. Eur. Heart J. 2003, 24, 586–603. [Google Scholar] [CrossRef] [Green Version]
- Kany, S.; Vollrath, J.T.; Relja, B. Cytokines in Inflammatory Disease. Int. J. Mol. Sci. 2019, 20, 6008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz-Carpio, V.; Sandoval, P.; Aguilera, A.; Albar-Vizcaíno, P.; Perez-Lozano, M.L.; González-Mateo, G.T.; Acuña-Ruiz, A.; García-Cantalejo, J.; Botías, P.; Bajo, M.A.; et al. Genomic reprograming analysis of the Mesothelial to Mesenchymal Transition identifies biomarkers in peritoneal dialysis patients. Sci. Rep. 2017, 7, 44941. [Google Scholar] [CrossRef] [Green Version]
- Loureiro, J.; Gónzalez-Mateo, G.; Jimenez-Heffernan, J.; Selgas, R.; López-Cabrera, M.; Aguilera Peralta, A. Are the mesothelial-to-mesenchymal transition, sclerotic peritonitis syndromes, and encapsulating peritoneal sclerosis part of the same process? Int. J. Nephrol. 2013, 2013, 263285. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Stewart, L.A.; Clarke, M.; Rovers, M.; Riley, R.D.; Simmonds, M.; Stewart, G.; Tierney, J.F.; PRISMA-IPD Development Group. Preferred reporting items for systematic review and meta-analyses of individual participant data: The PRISMA-IPD Statement. JAMA 2015, 313, 1657–1665. [Google Scholar] [CrossRef]
- Tang, W.; Li, M.; Lu, X.-H.; Liu, H.W.; Wang, T. Phospholipids profiling and outcome of peritoneal dialysis patients. Biomarkers 2014, 19, 505–508. [Google Scholar] [CrossRef]
- Dunn, W.B.; Summers, A.; Brown, M.; Goodacre, R.; Lambie, M.; Johnson, T.; Wilkie, M.; Davies, S.; Topley, N.; Brenchley, P. Proof-of-principle study to detect metabolic changes in peritoneal dialysis effluent in patients who develop encapsulating peritoneal sclerosis. Nephrol. Dial. Transplant. 2012, 27, 2502–2510. [Google Scholar] [CrossRef]
- Guleria, A.; Bajpai, N.K.; Rawat, A.; Khetrapal, C.L.; Prasad, N.; Kumar, D. Metabolite characterization in peritoneal dialysis effluent using high-resolution (1) H and (1) H-(13) C NMR Spectroscopy. Magn. Reson. Chem. 2014, 52, 475–479. [Google Scholar] [CrossRef] [Green Version]
- Asano, M.; Ishii, T.; Hirayama, A.; Mizuno, M.; Suzuki, Y.; Sakata, F.; Akiyama, S.I.; Maruyama, S.; Soga, T.; Kinashi, H.; et al. Differences in peritoneal solute transport rates in peritoneal dialysis. Clin. Exp. Nephrol. 2019, 23, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Csaicsich, D.; Lichtenauer, A.M.; Vychytil, A.; Kasper, D.C.; Herzog, R.; Aufricht, C.; Kratochwill, K. Feasibility of metabolomics analysis of dialysate effluents from patients undergoing peritoneal equilibration testing. Perit. Dial. Int. 2015, 35, 590–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kratochwill, K.; Boehm, M.; Herzog, R.; Gruber, K.; Lichtenauer, A.M.; Kuster, L.; Csaicsich, D.; Gleiss, A.; Alper, S.L.; Aufricht, C.; et al. Addition of alanyl-glutamine to dialysis fluid restores peritoneal cellular stress responses—A first-in-man trial. PLoS ONE 2016, 11, e0165045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiesenhofer, F.M.; Herzog, R.; Boehm, M.; Wagner, A.; Unterwurzacher, M.; Kasper, D.C.; Alper, S.L.; Vychytil, A.; Aufricht, C.; Kratochwill, K. Targeted metabolomic profiling of peritoneal dialysis effluents shows anti-oxidative capacity of alanyl-glutamine. Front. Physiol. 2018, 9, 1961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rainville, P.D.; Theodoridis, G.; Plumb, R.S.; Wilson, I.D. Advances in liquid chromatography coupled to mass spectrometry for metabolic phenotyping. TrAC Trends Anal. Chem. 2014, 61, 181–191. [Google Scholar] [CrossRef]
- Theodoridis, G.; Gika, H.G.; Wilson, I.D. LC-MS-based methodology for global metabolite profiling in Metabonomics/Metabolomics. TrAC Trends Anal. Chem. 2008, 27, 251–260. [Google Scholar] [CrossRef]
- Theodoridis, G.A.; Gika, H.G.; Want, E.J.; Wilson, I.D. Liquid chromatography–mass spectrometry based global metabolite profiling: A review. Anal. Chim. Acta. 2012, 711, 7–16. [Google Scholar] [CrossRef]
- Begou, O.; Gika, H.G.; Wilson, I.D.; Theodoridis, G. Hyphenated MS-based targeted approaches in metabolomics. Analyst 2017, 142, 3079–3100. [Google Scholar] [CrossRef]
- Kalim, S.; Rhee, E.P. An overview of renal metabolomics. Kidney Int. 2017, 91, 61–69. [Google Scholar] [CrossRef] [Green Version]
- Vanholder, R.; Boelaert, J.; Glorieux, G.; Eloot, S. New methods and technologies for measuring uremic toxins and quantifying dialysis adequacy. Semin. Dial. 2015, 28, 114–124. [Google Scholar] [CrossRef]
- Ji-Choi, J.Y.; Yoon, Y.J.; Choi, H.J.; Park, S.H.; Kim, C.D.; Kim, I.S.; Kwon, T.H.; Do, J.Y.; Kim, S.H.; Ryu, D.H.; et al. Dialysis modality-dependent changes in serum metabolites: Accumulation of inosine and hypoxanthine in patients on haemodialysis. Nephrol. Dial. Transplant. 2011, 26, 1304–1313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goek, O.N.; Prehn, C.; Sekula, P.; Römisch-Margl, W.; Döring, A.; Gieger, C.; Heier, M.; Koenig, W.; Wang-Sattler, R.; Illig, T.; et al. Metabolites associate with kidney function decline and incident chronic kidney disease in the general population. Nephrol. Dial. Transplant. 2013, 8, 2131–2138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes Barreto, D.; Struijk, D.G. Peritoneal Effluent Biomarker Discovery in Peritoneal Dialysis: The Omics Era. In Biomarkers in Kidney Disease: Methods, Discoveries and Applications; Patel, V., Preedy, V., Eds.; Springer: Dordrecht, The Netherlands, 2016. [Google Scholar]
- Davies, S.J. Peritoneal Solute Transport—We know it is important, but what is It? Nephrol. Dial. Transplant. 2000, 15, 1120–1123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mäkinen, V.P.; Tynkkynen, T.; Soininen, P.; Forsblom, C.; Peltola, T.; Kangas, A.J.; Groop, P.H.; Ala-Korpela, M. Sphingomyelin is associated with kidney disease in type 1 diabetes (The FinnDiane Study). Metabolomics 2012, 8, 369–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavoine, C.; Pecker, F. Sphingomyelinases: Their regulationand roles in cardiovascular pathophysiology. Cardiovasc. Res. 2009, 82, 175–183. [Google Scholar] [CrossRef] [Green Version]
- Hla, T.; Dannenberg, A.J. Sphingolipid signaling in metabolic disorders. Cell Metab. 2012, 16, 420–434. [Google Scholar] [CrossRef] [Green Version]
- Vychytil, A.; Herzog, R.; Probst, P.; Ribitsch, W.; Lhotta, K.; Machold-Fabrizii, V.; Wiesholzer, M.; Kaufmann, M.; Salmhofer, H.; Windpessl, M.; et al. A randomized controlled trial of alanyl-glutamine supplementation in peritoneal dialysis fluid to assess impact on biomarkers of peritoneal health. Kidney Int. 2018, 94, 1227–1237. [Google Scholar] [CrossRef] [Green Version]
- Cruzat, V.; Macedo Rogero, M.; Noel Keane, K.; Curi, R.; Newsholme, P. Glutamine: Metabolism and immune function, supplementation and clinical translation. Nutrients 2018, 10, 1564. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Ref/Year/Country | Type of Study | No Patients | Age (Years) Mean (Range) | PD Vintage (Years) Mean (Range) |
|---|---|---|---|---|
| [18]/2014/China | Prospective Cohort Duration: 38 ± 14 months | 20 | NA | NA |
| [19]/2012/England | Prospective Cohort Duration: 6 years | 22 | 46.5 (35–59) | NA |
| [20]2014/India | Cross-sectional | 8 | ΝA | NA |
| [21]/2019/Japan | Cross-sectional | 19 | 59 (46–68) | 4 (2.6–5.3) |
| [22]/2015/Austria | Cross-sectional | 8 | 62 (49–74) | 2.5 (0.4–4.5) |
| [23]/2016/Austria | Cross-sectional | 20 | 58 (47–68) | 2.38 (0.8–3.46) |
| [24]/2018/Poland | Randomized Controlled Trial | 20 | 58 | 2.4 |
| Ref/Year/Country | Matrix | Compounds | Instrumentation | Sample Preparation | Biomarkers |
|---|---|---|---|---|---|
| [18]/2014/China | Plasma | 190 lipid species | NPH/RPH, LC/LC-qTOF | 200 μL serum + 100 μL IS extracted with 12 mL of chloroform:methanol, 2:1, v/v. Evaporation to dryness and reconstitution with 1 mL chloroform:methanol, 2:1 v/v. | PS41:4, PI40:4, SM16:0, SM20:7, SM21:0, PC35:1, PC2:11, PC42:9 |
| [19]/2012/England | PDE | More than 100 endogenous compounds including sugars, amino acids, organic acids and others | 1. GC-TOF 2. Direct infusion MS | 1. 100 μL of PDE were diluted with IS and then the sample was lyophilized. 2. 100 μL of PDE were diluted with methanol for protein precipitation. After centrifugation, the clear supernatant was directly injected into the MS. | 38 metabolites in total including amino acids, sugars, amines and organic acids |
| [20]/2014/India | PDE | 53 small endogenous metabolites | 1H-13C NMR spectroscopy | 400 μL of untreated PDF diluted with 0.5% sodium salt of 3-trimethylsilyl-(2,2,3,3-d4)- propionic acid (TSP) in deuterium oxide (D2O). | - |
| [21]/2019/Japan | Serum and PDE | 38 small-, middle- and large-sized molecules | CE-TOF | - | - |
| [22]/2015/Austria | PDE | 200 features | UHPLC-ORBITRAP | Centrifugation of PDE. On-line sample clean up. | 29 significant features mainly related to tryptophan metabolism |
| [23]/2016/Austria | PDE | 200 features | UHPLC-ORBITRAP | - | leucine, isoleucine, glutamine, arginine, fatty acids, glycolipids related metabolites, phenylalanine, tyrosine, homocysteic acid, nucleic acids (AlaGln supplementation) |
| [24]/2018/Poland | PDE | 188 endogenous compounds including amino acids, acylcarnitines, amines, glycerophospholipids, hexoses and sphingolipids | LC/FIA-QTRAP | 10 μL PDE + 10 μL IS were evaporated to dryness. Derivatization with phenylisothiocyanate and evaporation to dryness. Reconstitution with 300 μL methanol + 5 mM ammonium acetate. Filtration and centrifugation. | 51 metabolites, including kynurenine, tryptophan, phenylalanine, serine, valine, SDMA, total-DMA and Met-SO |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kondou, A.; Begou, O.; Dotis, J.; Karava, V.; Panteris, E.; Taparkou, A.; Gika, H.; Printza, N. Impact of Metabolomics Technologies on the Assessment of Peritoneal Membrane Profiles in Peritoneal Dialysis Patients: A Systematic Review. Metabolites 2022, 12, 145. https://doi.org/10.3390/metabo12020145
Kondou A, Begou O, Dotis J, Karava V, Panteris E, Taparkou A, Gika H, Printza N. Impact of Metabolomics Technologies on the Assessment of Peritoneal Membrane Profiles in Peritoneal Dialysis Patients: A Systematic Review. Metabolites. 2022; 12(2):145. https://doi.org/10.3390/metabo12020145
Chicago/Turabian StyleKondou, Antonia, Olga Begou, John Dotis, Vasiliki Karava, Eleftherios Panteris, Anna Taparkou, Helen Gika, and Nikoleta Printza. 2022. "Impact of Metabolomics Technologies on the Assessment of Peritoneal Membrane Profiles in Peritoneal Dialysis Patients: A Systematic Review" Metabolites 12, no. 2: 145. https://doi.org/10.3390/metabo12020145