
Gingerol, a Natural Antioxidant, Attenuates Hyperglycemia and Downstream Complications
 ,
,  , , , , ,
, , , , , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
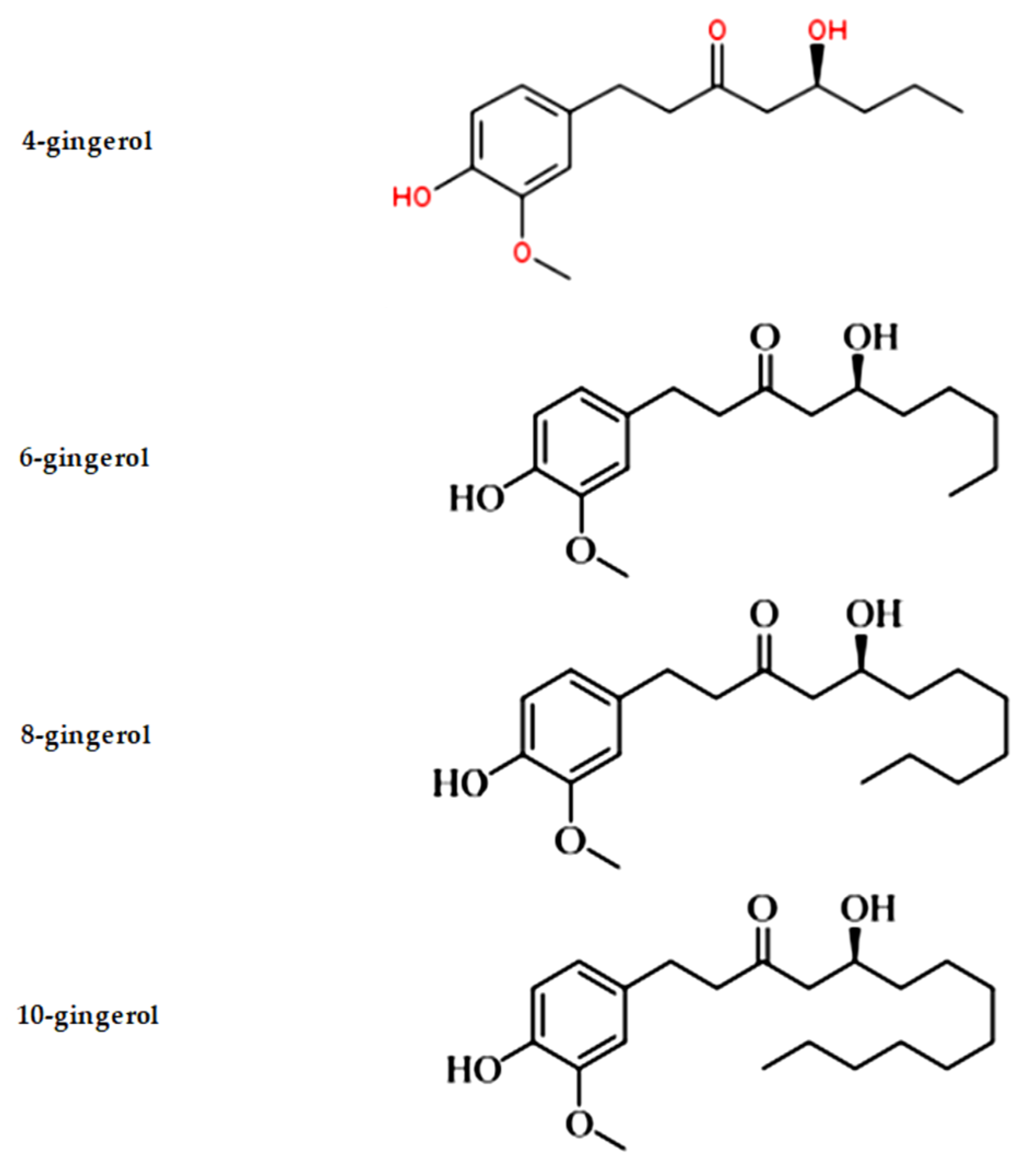
2. Discovery, Source, Biosynthesis, Properties and Action Mechanism of Gingerol
Hyperglycemia and Subsequent Complications
3. Gingerol as an Antioxidant
4. Gingerol as a Curative Agent against Hyperglycemia
5. Gingerol’s Restorative Role in Hyperglycemia Related Complications
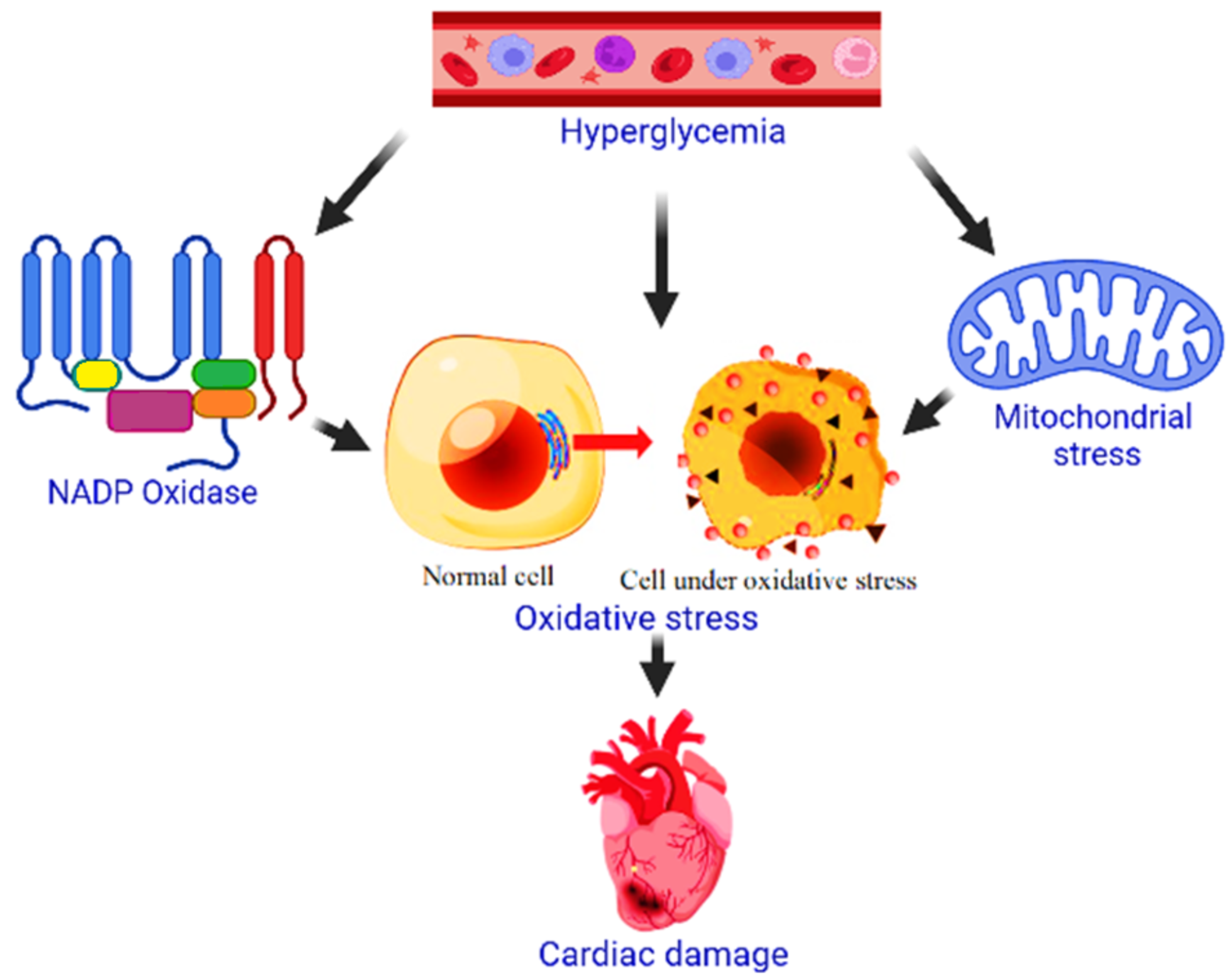
5.1. Cardiomyopathy
5.2. Nephropathy (Kidney Damage or Kidney Failure)
5.3. Retinopathy (Retinal Blood Vessel Damage)
5.4. Cataract (Potentially Leading to Blindness, Clouding of the Normally Clear Lens of Your Eye)
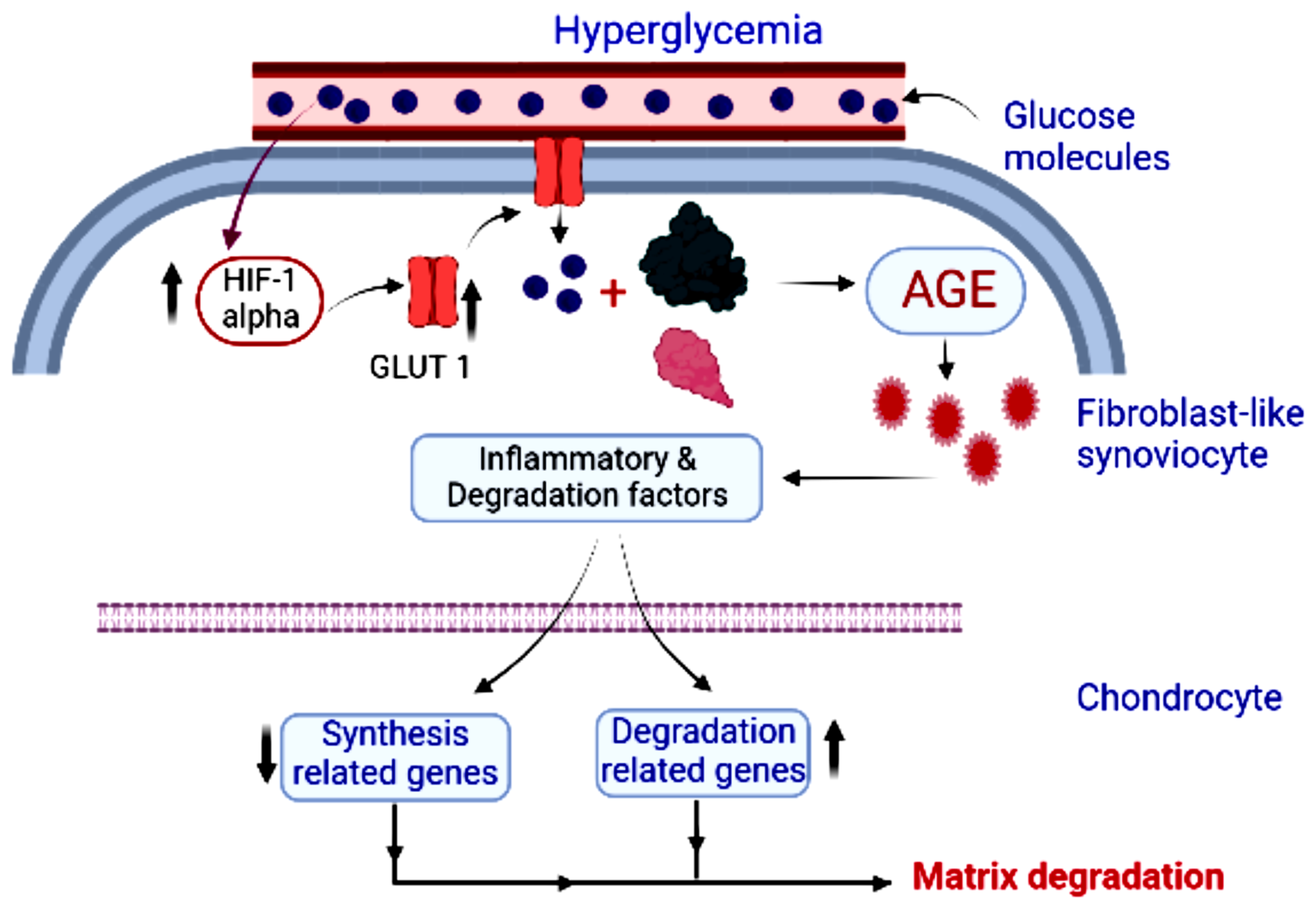
5.5. Bone and Joint Problems
5.6. Periodontitis (Tooth and Gum Infection)
6. Limitations
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ma, R.-H.; Ni, Z.-J.; Zhu, Y.-Y.; Thakur, K.; Zhang, F.; Zhang, Y.-Y.; Hu, F.; Zhang, J.-G.; Wei, Z.-J. A recent update on the multifaceted health benefits associated with ginger and its bioactive components. Food Funct. 2021, 12, 519–542. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.A.; El-Nour, M.E.M.; Yagi, S.M. Total phenolic and flavonoid contents and antioxidant activity of ginger (Zingiber officinale Rosc.) rhizome, callus and callus treated with some elicitors. J. Genet. Eng. Biotechnol. 2018, 16, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Kubra, I.R.; Jagan Mohan Rao, L. Microwave drying of ginger (Zingiber officinale Roscoe) and its effects on polyphenolic content and antioxidant activity. Int. J. Food Sci. Technol. 2012, 47, 2311–2317. [Google Scholar] [CrossRef]
- Wang, S.; Zhang, C.; Yang, G.; Yang, Y. Biological properties of 6-gingerol: A brief review. Nat. Prod. Commun. 2014, 9, 1934578X1400900736. [Google Scholar] [CrossRef] [Green Version]
- Jung Park, E.; Pezzuto, J.M. Botanicals in cancer chemoprevention. Cancer Metastasis Rev. 2002, 21, 231–255. [Google Scholar] [CrossRef] [PubMed]
- Unuofin, J.O.; Masuku, N.P.; Paimo, O.K.; Lebelo, S.L. Ginger from Farmyard to Town: Nutritional and Pharmacological Applications. Front. Pharmacol. 2021, 12, 779352. [Google Scholar] [CrossRef]
- Shukla, Y.; Singh, M. Cancer preventive properties of ginger: A brief review. Food Chem. Toxicol. 2007, 45, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Kou, X.; Zhao, H.; Mak, K.-K.; Balijepalli, M.K.; Pichika, M.R. Zingiber officinale var. rubrum: Red Ginger’s Medicinal Uses. Molecules 2022, 27, 775. [Google Scholar] [CrossRef]
- Jolad, S.D.; Lantz, R.C.; Solyom, A.M.; Chen, G.J.; Bates, R.B.; Timmermann, B.N. Fresh organically grown ginger (Zingiber officinale): Composition and effects on LPS-induced PGE2 production. Phytochemistry 2004, 65, 1937–1954. [Google Scholar] [CrossRef]
- Tjendraputra, E.; Tran, V.H.; Liu-Brennan, D.; Roufogalis, B.D.; Duke, C.C. Effect of ginger constituents and synthetic analogues on cyclooxygenase-2 enzyme in intact cells. Bioorganic Chem. 2001, 29, 156–163. [Google Scholar] [CrossRef]
- He, X.-G.; Bernart, M.W.; Lian, L.-Z.; Lin, L.-Z. High-performance liquid chromatography–electrospray mass spectrometric analysis of pungent constituents of ginger. J. Chromatogr. A 1998, 796, 327–334. [Google Scholar] [CrossRef]
- Direito, J.; Fernandes, C.; Branquinho, R.G.; Ramos, D.F.; Dionísio, T.; Oliveira, G.G.; Pinto, C.R. Secondary hepatic injury in pediatric intensive care: Risk factors and prognostic impact. J. Pediatric Gastroenterol. Nutr. 2021, 73, 471–477. [Google Scholar] [CrossRef] [PubMed]
- E Duncan, A. Hyperglycemia and perioperative glucose management. Curr. Pharm. Des. 2012, 18, 6195–6203. [Google Scholar] [CrossRef] [PubMed]
- Chalkias, A.; Papagiannakis, N.; Mavrovounis, G.; Kolonia, K.; Mermiri, M.; Pantazopoulos, I.; Laou, E.; Arnaoutoglou, E. Sublingual microcirculatory alterations during the immediate and early postoperative period: A systematic review and meta-analysis. Clin. Hemorheol. Microcirc. 2021, 80, 253–265. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, O.M.; Gómez, A.M.; Maira, G.-J.; Mauricio, L.-V.F.; Ruiz-Morales, Á.J. The different methods of assessing glycemic variability, quality of glycemic control and glycemic risk cannot be interpreted as equivalent in clinical practice. Diabetes Metab. Syndr. Clin. Res. Rev. 2018, 12, 555–561. [Google Scholar] [CrossRef]
- Deedwania, P.; Acharya, T. Cardiovascular protection with anti-hyperglycemic agents. Am. J. Cardiovasc. Drugs 2019, 19, 249–257. [Google Scholar] [CrossRef]
- Murphy, C.V.; Saliba, L.; MacDermott, J.; Soe, K.; Dungan, K.M. Individualizing glycemic control in the critically ill. Crit. Care Nurs. Q. 2020, 43, 14–27. [Google Scholar] [CrossRef]
- Almatroodi, S.A.; Alnuqaydan, A.M.; Babiker, A.Y.; Almogbel, M.A.; Khan, A.A.; Husain Rahmani, A. 6-Gingerol, a Bioactive Compound of Ginger Attenuates Renal Damage in Streptozotocin-Induced Diabetic Rats by Regulating the Oxidative Stress and Inflammation. Pharmaceutics 2021, 13, 317. [Google Scholar] [CrossRef]
- Fuhrman, B.; Rosenblat, M.; Hayek, T.; Coleman, R.; Aviram, M. Ginger extract consumption reduces plasma cholesterol, inhibits LDL oxidation and attenuates development of atherosclerosis in atherosclerotic, apolipoprotein E-deficient mice. J. Nutr. 2000, 130, 1124–1131. [Google Scholar] [CrossRef] [Green Version]
- Tzeng, T.F.; Liou, S.S.; Chang, C.J.; Liu, I.M. The Ethanol Extract of Zingiber zerumbet Attenuates Streptozotocin-Induced Diabetic Nephropathy in Rats. Evid. -Based Complementary Altern. Med. Ecam 2013, 2013, 340645. [Google Scholar] [CrossRef]
- Rodrigues, F.A.; Prata, M.M.; Oliveira, I.C.; Alves, N.T.; Freitas, R.E.; Monteiro, H.S.; Silva, J.A.; Vieira, P.C.; Viana, D.A.; Libório, A.B.; et al. Gingerol fraction from Zingiber officinale protects against gentamicin-induced nephrotoxicity. Antimicrob. Agents Chemother. 2014, 58, 1872–1878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semwal, R.B.; Semwal, D.K.; Combrinck, S.; Viljoen, A.M. Gingerols and shogaols: Important nutraceutical principles from ginger. Phytochemistry 2015, 117, 554–568. [Google Scholar] [CrossRef] [PubMed]
- James, P.; Baby, B.; Charles, S.; Nair, L.S.; Nazeem, P.A. Computer aided gene mining for gingerol biosynthesis. Bioinformation 2015, 11, 316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, Y.; Huang, M.; Wisniewski, M.; Li, H.; Zhang, M.; Tao, X.; Liu, Y.; Zou, Y. Transcriptome analysis provides insights into gingerol biosynthesis in ginger (Zingiber officinale). Plant Genome 2018, 11, 180034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.; Zhao, R.; Wang, D.; Wang, L.; Zhang, Q.; Wei, S.; Lu, F.; Peng, W.; Wu, C. Ginger (Zingiber officinale Rosc.) and its bioactive components are potential resources for health beneficial agents. Phytother. Res. 2021, 35, 711–742. [Google Scholar] [CrossRef]
- Gupta, J.; Sharma, S.; Sharma, N.R.; Kabra, D. Phytochemicals enriched in spices: A source of natural epigenetic therapy. Arch. Pharmacal Res. 2020, 43, 171–186. [Google Scholar] [CrossRef]
- Siddiqui, Z.H.; Hareramdas, B.; Abbas, Z.K.; Parween, T.; Khan, M.N. Use of plant secondary metabolites as nutraceuticals for treatment and management of cancer: Approaches and challenges. In Anticancer Plants: Properties and Application; Springer: Berlin/Heidelberg, Germany, 2018; pp. 395–413. [Google Scholar]
- Ding, G.; Naora, K.; Hayashibara, M.; Katagiri, Y.; Kano, Y.; Iwamoto, K.J.C.; Bulletin, P. Pharmacokinetics of [6]-gingerol after intravenous administration in rats. Chem. Pharm. Bull. 1991, 39, 1612–1614. [Google Scholar] [CrossRef] [Green Version]
- Naora, K.; Ding, G.; Hayashibara, M.; Katagiri, Y.; Kano, Y.; Iwamoto, K.J.C.; Bulletin, P. Pharmacokinetics of [6]-gingerol after intravenous administration in rats with acute renal or hepatic failure. Chem. Pharm. Bull. 1992, 40, 1295–1298. [Google Scholar] [CrossRef] [Green Version]
- Nakazawa, T.; Ohsawa, K.J.L.s. Metabolism of [6]-gingerol in rats. Life Sci. 2002, 70, 2165–2175. [Google Scholar] [CrossRef]
- Pfeiffer, E.; Hoehle, S.I.; Walch, S.G.; Riess, A.; Sólyom, A.M.; Metzler, M.J.J.O.A.; Chemistry, F. Curcuminoids form reactive glucuronides in vitro. J. Agric. Food Chem. 2007, 55, 538–544. [Google Scholar] [CrossRef]
- Zick, S.M.; Turgeon, D.K.; Vareed, S.K.; Ruffin, M.T.; Litzinger, A.J.; Wright, B.D.; Alrawi, S.; Normolle, D.P.; Djuric, Z.; Brenner, D.E.J.C.P.R. Phase II study of the effects of ginger root extract on eicosanoids in colon mucosa in people at normal risk for colorectal cancer. Cancer Prev. Res. 2011, 4, 1929–1937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellen Davis, R.; Natalie Mandolfo, M. Hyperglycemia and cancer: A state-of-the-science review. Oncol. Nurs. Forum 2019, 46, 459–472. [Google Scholar]
- Veras-Estévez, B.A.; Chapman, H.J. Strengthening national health priorities for Diabetes prevention and management. MEDICC Rev. 2018, 20, 5. [Google Scholar]
- Das, S.; Misra, B.; Roul, L.; Minz, N.T.; Pattnaik, M.; Baig, M.A.A. Insulin Resistance and β Cell Function As Prognostic Indicator in Multi-Organ Dysfunction Syndrome. Metab. Syndr. Relat. Disord. 2009, 7, 47–51. [Google Scholar] [CrossRef]
- Chawla, A.; Chawla, R.; Jaggi, S. Microvascular and Macrovascular Complications in Diabetes Mellitus: Distinct or Continuum? Recent Adv. Diabetes 2018, 20, 546. [Google Scholar]
- Campbell, M.R.; Shokrani, M. Introduction, Background and Various Types. Clin. Lab. Sci. 2016, 29, 106–110. [Google Scholar] [CrossRef]
- Mathew, T.K.; Tadi, P. Blood Glucose Monitoring. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Mouri, M.; Badireddy, M. Hyperglycemia. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Victor, F.M.; Lima Andrade, S.R.d.; Bandeira, F. Diabetic Ketoacidosis and Hyperosmolar Hyperglycemic State. In Endocrinology and Diabetes; Springer: Berlin/Heidelberg, Germany, 2022; pp. 355–362. [Google Scholar]
- Henry, R.R.; Thakkar, P.; Tong, C.; Polidori, D.; Alba, M. Efficacy and safety of canagliflozin, a sodium–glucose cotransporter 2 inhibitor, as add-on to insulin in patients with type 1 diabetes. Diabetes Care 2015, 38, 2258–2265. [Google Scholar] [CrossRef] [Green Version]
- Lantz, R.; Chen, G.; Sarihan, M.; Solyom, A.; Jolad, S.; Timmermann, B. The effect of extracts from ginger rhizome on inflammatory mediator production. Phytomedicine 2007, 14, 123–128. [Google Scholar] [CrossRef]
- Schwertner, H.A.; Rios, D.C. High-performance liquid chromatographic analysis of 6-gingerol, 8-gingerol, 10-gingerol, and 6-shogaol in ginger-containing dietary supplements, spices, teas, and beverages. J. Chromatogr. B 2007, 856, 41–47. [Google Scholar] [CrossRef]
- Ghasemzadeh, A.; Jaafar, H.Z.; Rahmat, A. Optimization protocol for the extraction of 6-gingerol and 6-shogaol from Zingiber officinale var. rubrum Theilade and improving antioxidant and anticancer activity using response surface methodology. BMC Complementary Altern. Med. 2015, 15, 258. [Google Scholar] [CrossRef] [Green Version]
- Rice-Evans, C.; Miller, N.; Paganga, G. Antioxidant properties of phenolic compounds. Trends Plant Sci. 1997, 2, 152–159. [Google Scholar] [CrossRef]
- Mathew, S.; Abraham, T.E.; Zakaria, Z.A. Reactivity of phenolic compounds towards free radicals under in vitro conditions. J. Food Sci. Technol. 2015, 52, 5790–5798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, G.; Zhong, L.; Jiang, L.; Geng, C.; Cao, J.; Sun, X.; Liu, X.; Chen, M.; Ma, Y. 6-Gingerol prevents patulin-induced genotoxicity in HepG2 cells. Phytother. Res. 2011, 25, 1480–1485. [Google Scholar] [CrossRef] [PubMed]
- Rahmani, A.H. Active ingredients of ginger as potential candidates in the prevention and treatment of diseases via modulation of biological activities. Int. J. Physiol. Pathophysiol. Pharmacol. 2014, 6, 125. [Google Scholar] [PubMed]
- Kuhad, A.; Tirkey, N.; Pilkhwal, S.; Chopra, K. 6-Gingerol prevents cisplatin-induced acute renal failure in rats. Biofactors 2006, 26, 189–200. [Google Scholar] [CrossRef]
- Aeschbach, R.; Löliger, J.; Scott, B.; Murcia, A.; Butler, J.; Halliwell, B.; Aruoma, O. Antioxidant actions of thymol, carvacrol, 6-gingerol, zingerone and hydroxytyrosol. Food Chem. Toxicol. 1994, 32, 31–36. [Google Scholar] [CrossRef]
- Park, I.-H.; Park, S.-J.; Cho, J.-S.; Moon, Y.-M.; Kim, T.H.; Lee, S.H.; Lee, H.-M. Role of reactive oxygen species in transforming growth factor beta1-induced alpha smooth-muscle actin and collagen production in nasal polyp-derived fibroblasts. Int. Arch. Allergy Immunol. 2012, 159, 278–286. [Google Scholar] [CrossRef]
- Chakraborty, D.; Mukherjee, A.; Sikdar, S.; Paul, A.; Ghosh, S.; Khuda-Bukhsh, A.R. [6]-Gingerol isolated from ginger attenuates sodium arsenite induced oxidative stress and plays a corrective role in improving insulin signaling in mice. Toxicol. Lett. 2012, 210, 34–43. [Google Scholar] [CrossRef]
- Juárez-Reyes, K.; Brindis, F.; Medina-Campos, O.N.; Pedraza-Chaverri, J.; Bye, R.; Linares, E.; Mata, R. Hypoglycemic, antihyperglycemic, and antioxidant effects of the edible plant Anoda cristata. J. Ethnopharmacol. 2015, 161, 36–45. [Google Scholar] [CrossRef]
- Shields, J.; Maxwell, A.P. Managing diabetic nephropathy. Clin. Med. 2010, 10, 500. [Google Scholar] [CrossRef]
- Tominaga, T.; Abe, H.; Ueda, O.; Goto, C.; Nakahara, K.; Murakami, T.; Matsubara, T.; Mima, A.; Nagai, K.; Araoka, T. Activation of bone morphogenetic protein 4 signaling leads to glomerulosclerosis that mimics diabetic nephropathy. J. Biol. Chem. 2011, 286, 20109–20116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohkubo, Y.; Kishikawa, H.; Araki, E.; Miyata, T.; Isami, S.; Motoyoshi, S.; Kojima, Y.; Furuyoshi, N.; Shichiri, M. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes mellitus: A randomized prospective 6-year study. Diabetes Res. Clin. Pract. 1995, 28, 103–117. [Google Scholar] [CrossRef] [PubMed]
- Sifuentes-Franco, S.; Padilla-Tejeda, D.E.; Carrillo-Ibarra, S.; Miranda-Díaz, A.G. Oxidative stress, apoptosis, and mitochondrial function in diabetic nephropathy. Int. J. Endocrinol. 2018, 2018, 1875870. [Google Scholar] [CrossRef]
- Mahmoodnia, L.; Aghadavod, E.; Beigrezaei, S.; Rafieian-Kopaei, M. An update on diabetic kidney disease, oxidative stress and antioxidant agents. J. Ren. Inj. Prev. 2017, 6, 153. [Google Scholar] [CrossRef]
- Levy, Y.; Zaltzberg, H.; Ben-Amotz, A.; Kanter, Y.; Aviram, M. β-Carotene affects antioxidant status in non-insulin-dependent diabetes mellitus. Pathophysiology 1999, 6, 157–161. [Google Scholar] [CrossRef]
- Eid, B.G.; Mosli, H.; Hasan, A.; El-Bassossy, H.M. Ginger ingredients alleviate diabetic prostatic complications: Effect on oxidative stress and fibrosis. Evid.-Based Complementary Altern. Med. 2017, 2017, 6090269. [Google Scholar] [CrossRef] [Green Version]
- Talebi, M.; Mohammadi Vadoud, S.A.; Haratian, A.; Talebi, M.; Farkhondeh, T.; Pourbagher-Shahri, A.M.; Samarghandian, S. The interplay between oxidative stress and autophagy: Focus on the development of neurological diseases. Behav. Brain Funct. 2022, 18, 3. [Google Scholar] [CrossRef]
- Lee, J.O.; Kim, N.; Lee, H.J.; Moon, J.W.; Lee, S.K.; Kim, S.J.; Kim, J.K.; Park, S.H.; Kim, H.S. [6]-Gingerol Affects Glucose Metabolism by Dual Regulation via the AMPKα2-Mediated AS160-Rab5 Pathway and AMPK-Mediated Insulin Sensitizing Effects. J. Cell. Biochem. 2015, 116, 1401–1410. [Google Scholar] [CrossRef]
- Wang, Z.; Thurmond, D.C. Mechanisms of biphasic insulin-granule exocytosis–roles of the cytoskeleton, small GTPases and SNARE proteins. J. Cell Sci. 2009, 122, 893–903. [Google Scholar] [CrossRef] [Green Version]
- Samad, M.B.; Mohsin, M.; Bin, N.A.; Razu, B.A.; Hossain, M.T.; Mahzabeen, S.; Unnoor, N.; Muna, I.A.; Akhter, F.; Kabir, A.U. [6]-Gingerol, from Zingiber officinale, potentiates GLP-1 mediated glucose-stimulated insulin secretion pathway in pancreatic β-cells and increases RAB8/RAB10-regulated membrane presentation of GLUT4 transporters in skeletal muscle to improve hyperglycemia in Leprdb/db type 2 diabetic mice. BMC Complementary Altern. Med. 2017, 17, 395. [Google Scholar]
- Bhandari, U.; Pillai, K. Effect of ethanolic extract of Zingiber officinale on dyslipidaemia in diabetic rats. J. Ethnopharmacol. 2005, 97, 227–230. [Google Scholar] [CrossRef] [PubMed]
- Nammi, S.; Sreemantula, S.; Roufogalis, B.D. Protective effects of ethanolic extract of Zingiber officinale rhizome on the development of metabolic syndrome in high-fat diet-fed rats. Basic Clin. Pharmacol. Toxicol. 2009, 104, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Jubaidi, F.F.; Zainalabidin, S.; Taib, I.S.; Hamid, Z.A.; Budin, S.B. The potential role of flavonoids in ameliorating diabetic cardiomyopathy via alleviation of cardiac oxidative stress, inflammation and apoptosis. Int. J. Mol. Sci. 2021, 22, 5094. [Google Scholar] [CrossRef] [PubMed]
- Spillmann, F.; Van Linthout, S.; Schultheiss, H.-P.; Tschöpe, C. Cardioprotective mechanisms of the kallikrein–kinin system in diabetic cardiopathy. Curr. Opin. Nephrol. Hypertens. 2006, 15, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Tschöpe, C.; Schultheiss, H. Diabetic cardiopathy: Pathogenesis, diagnosis and therapy. Der Internist 2003, 44, 806–812, 814. [Google Scholar] [CrossRef]
- Lee, W.S.; Kim, J. Diabetic cardiomyopathy: Where we are and where we are going. Korean J. Intern. Med. 2017, 32, 404–421. [Google Scholar] [CrossRef] [Green Version]
- Kenny, H.C.; Abel, E.D. Heart Failure in Type 2 Diabetes Mellitus. Circ. Res. 2019, 124, 121–141. [Google Scholar] [CrossRef]
- Matough, F.A.; Budin, S.B.; Hamid, Z.A.; Alwahaibi, N.; Mohamed, J. The role of oxidative stress and antioxidants in diabetic complications. Sultan Qaboos Univ. Med. J. 2012, 12, 5–18. [Google Scholar] [CrossRef]
- Reily-Bell, M.; Bahn, A.; Katare, R. Reactive Oxygen Species-Mediated Diabetic Heart Disease: Mechanisms and Therapies. Antioxid. Redox Signal. 2021, 36, 608–630. [Google Scholar] [CrossRef]
- Prasad, S.; Sinha, A.K. Free radical activity in hypertensive type 2 diabetic patients. Int. J. Diabetes Mellit. 2010, 2, 141–143. [Google Scholar] [CrossRef] [Green Version]
- Desco, M.-C.; Asensi, M.; Márquez, R.; Martínez-Valls, J.; Vento, M.; Pallardó, F.V.; Sastre, J.; Viña, J. Xanthine oxidase is involved in free radical production in type 1 diabetes: Protection by allopurinol. Diabetes 2002, 51, 1118–1124. [Google Scholar] [CrossRef] [Green Version]
- Dludla, P.V.; Joubert, E.; Muller, C.J.; Louw, J.; Johnson, R. Hyperglycemia-induced oxidative stress and heart disease-cardioprotective effects of rooibos flavonoids and phenylpyruvic acid-2-O-β-D-glucoside. Nutr. Metab. 2017, 14, 45. [Google Scholar] [CrossRef] [Green Version]
- Yu, L.Y.; Shi, W.L.; Guo, X.G. Cardio-Protective Role of Gingerol along with Prominent Anti-Diabetic Cardiomyopathy Action in A Streptozotocin-Induced Diabetes Mellitus Rat Model. Cell J. 2017, 19, 469–475. [Google Scholar] [CrossRef]
- Chavali, V.; Tyagi, S.C.; Mishra, P.K. Predictors and prevention of diabetic cardiomyopathy. Diabetes Metab. Syndr. Obes. Targets Ther. 2013, 6, 151. [Google Scholar]
- El-Bassossy, H.M.; Elberry, A.A.; Ghareib, S.A.; Azhar, A.; Banjar, Z.M.; Watson, M.L. Cardioprotection by 6-gingerol in diabetic rats. Biochem. Biophys. Res. Commun. 2016, 477, 908–914. [Google Scholar] [CrossRef]
- Cade, W.T. Diabetes-related microvascular and macrovascular diseases in the physical therapy setting. Phys. Ther. 2008, 88, 1322–1335. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.V.; Baliga, R.; Rajapurkar, M.; Fonseca, V.A. Oxidants in chronic kidney disease. J. Am. Soc. Nephrol. 2007, 18, 16–28. [Google Scholar] [CrossRef] [Green Version]
- Ohshiro, Y.; Takasu, N. Molecular mechanism of diabetic nephropathy. Nihon Rinsho. Jpn. J. Clin. Med. 2006, 64, 997–1003. [Google Scholar]
- Khanra, R.; Dewanjee, S.; K Dua, T.; Sahu, R.; Gangopadhyay, M.; De Feo, V.; Zia-Ul-Haq, M. Abroma augusta L.(Malvaceae) leaf extract attenuates diabetes induced nephropathy and cardiomyopathy via inhibition of oxidative stress and inflammatory response. J. Transl. Med. 2015, 13, 6. [Google Scholar] [CrossRef] [Green Version]
- Kashihara, N.; Haruna, Y.; K Kondeti, V.; S Kanwar, Y. Oxidative stress in diabetic nephropathy. Curr. Med. Chem. 2010, 17, 4256–4269. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.B.; Yu, M.-R.; Yang, Y.; Jiang, Z.; Ha, H. Reactive oxygen species-regulated signaling pathways in diabetic nephropathy. J. Am. Soc. Nephrol. 2003, 14, S241–S245. [Google Scholar] [CrossRef] [Green Version]
- Afshari, A.T.; Shirpoor, A.; Farshid, A.; Saadatian, R.; Rasmi, Y.; Saboory, E.; Ilkhanizadeh, B.; Allameh, A. The effect of ginger on diabetic nephropathy, plasma antioxidant capacity and lipid peroxidation in rats. Food Chem. 2007, 101, 148–153. [Google Scholar] [CrossRef]
- Lim, A.K.; Tesch, G.H. Inflammation in diabetic nephropathy. Mediat. Inflamm. 2012, 2012, 146154. [Google Scholar] [CrossRef]
- Al-Quraishy, S.; Dkhil, M.A.; Abdel Moneim, A.E. Anti-hyperglycemic activity of selenium nanoparticles in streptozotocin-induced diabetic rats. Int. J. Nanomed. 2015, 10, 6741–6756. [Google Scholar] [CrossRef] [Green Version]
- Gao, Y.; Zhang, R.; Li, J.; Ren, M.; Ren, Z.; Shi, J.; Pan, Q.; Ren, S. Radix Astragali lowers kidney oxidative stress in diabetic rats treated with insulin. Endocrine 2012, 42, 592–598. [Google Scholar] [CrossRef]
- Rains, J.L.; Jain, S.K. Oxidative stress, insulin signaling, and diabetes. Free Radic. Biol. Med. 2011, 50, 567–575. [Google Scholar] [CrossRef]
- Ceriello, A.; Testa, R. Antioxidant anti-inflammatory treatment in type 2 diabetes. Diabetes Care 2009, 32, S232–S236. [Google Scholar] [CrossRef] [Green Version]
- Klein, G.; Kim, J.; Himmeldirk, K.; Cao, Y.; Chen, X. Antidiabetes and anti-obesity activity of Lagerstroemia speciosa. Evid. -Based Complementary Altern. Med. 2007, 4, 401–407. [Google Scholar] [CrossRef] [Green Version]
- Spiller, H.A.; Sawyer, T.S. Toxicology of oral antidiabetic medications. Am. J. Health-Syst. Pharm. 2006, 63, 929–938. [Google Scholar] [CrossRef]
- Alam, M.M.; Meerza, D.; Naseem, I. Protective effect of quercetin on hyperglycemia, oxidative stress and DNA damage in alloxan induced type 2 diabetic mice. Life Sci. 2014, 109, 8–14. [Google Scholar] [CrossRef]
- Singh, A.B.; Singh, N.; Maurya, R.; Srivastava, A.K. Anti-hyperglycaemic, lipid lowering and anti-oxidant properties of [6]-gingerol in db/db mice. Int. J. Med. Med. Sci. 2009, 1, 536–544. [Google Scholar]
- Al Hroob, A.M.; Abukhalil, M.H.; Alghonmeen, R.D.; Mahmoud, A.M. Ginger alleviates hyperglycemia-induced oxidative stress, inflammation and apoptosis and protects rats against diabetic nephropathy. Biomed. Pharmacother. 2018, 106, 381–389. [Google Scholar] [CrossRef]
- Hegazy, A.M.; Mosaed, M.M.; Elshafey, S.H.; Bayomy, N.A. 6-gingerol ameliorates gentamicin induced renal cortex oxidative stress and apoptosis in adult male albino rats. Tissue Cell 2016, 48, 208–216. [Google Scholar] [CrossRef]
- Wada, J.; Makino, H. Inflammation and the pathogenesis of diabetic nephropathy. Clin. Sci. 2013, 124, 139–152. [Google Scholar] [CrossRef] [Green Version]
- Shalaby, M.A.; Hamowieh, A.R. Safety and efficacy of Zingiber officinale roots on fertility of male diabetic rats. Food Chem. Toxic. 2010, 48, 2920–2924. [Google Scholar] [CrossRef]
- Almatroodi, S.A.; Almatroudi, A.; Alsahli, M.A.; Aljasir, M.A.; Syed, M.A.; Rahmani, A.H. Epigallocatechin-3-Gallate (EGCG), an active compound of green tea attenuates acute lung injury regulating macrophage polarization and Krüpple-like-factor 4 (KLF4) expression. Molecules 2020, 25, 2853. [Google Scholar] [CrossRef]
- Alsahli, M.A.; Almatroodi, S.A.; Almatroudi, A.; Khan, A.A.; Anwar, S.; Almutary, A.G.; Alrumaihi, F.; Rahmani, A.H. 6-Gingerol, a Major Ingredient of Ginger Attenuates Diethylnitrosamine-Induced Liver Injury in Rats through the Modulation of Oxidative Stress and Anti-Inflammatory Activity. Mediat. Inflamm. 2021, 2021, 6661937. [Google Scholar] [CrossRef]
- Yau, J.W.; Rogers, S.L.; Kawasaki, R.; Lamoureux, E.L.; Kowalski, J.W.; Bek, T.; Chen, S.J.; Dekker, J.M.; Fletcher, A.; Grauslund, J.; et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care 2012, 35, 556–564. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.; He, M.; Congdon, N. The worldwide epidemic of diabetic retinopathy. Indian J. Ophthalmol. 2012, 60, 428–431. [Google Scholar] [CrossRef]
- Brownlee, M. Biochemistry and molecular cell biology of diabetic complications. Nature 2001, 414, 813–820. [Google Scholar] [CrossRef]
- Brownlee, M. The pathobiology of diabetic complications: A unifying mechanism. Diabetes 2005, 54, 1615–1625. [Google Scholar] [CrossRef] [Green Version]
- Rangasamy, S.; McGuire, P.G.; Das, A. Diabetic retinopathy and inflammation: Novel therapeutic targets. Middle East Afr. J. Ophthalmol. 2012, 19, 52–59. [Google Scholar] [CrossRef] [Green Version]
- Adamis, A.P. Is diabetic retinopathy an inflammatory disease? Br. J. Ophthalmol. 2002, 86, 363–365. [Google Scholar] [CrossRef] [Green Version]
- Joussen, A.M.; Doehmen, S.; Le, M.L.; Koizumi, K.; Radetzky, S.; Krohne, T.U.; Poulaki, V.; Semkova, I.; Kociok, N. TNF-alpha mediated apoptosis plays an important role in the development of early diabetic retinopathy and long-term histopathological alterations. Mol. Vis. 2009, 15, 1418–1428. [Google Scholar]
- Demircan, N.; Safran, B.G.; Soylu, M.; Ozcan, A.A.; Sizmaz, S. Determination of vitreous interleukin-1 (IL-1) and tumour necrosis factor (TNF) levels in proliferative diabetic retinopathy. Eye 2006, 20, 1366–1369. [Google Scholar] [CrossRef] [Green Version]
- Abu el Asrar, A.M.; Maimone, D.; Morse, P.H.; Gregory, S.; Reder, A.T. Cytokines in the vitreous of patients with proliferative diabetic retinopathy. Am. J. Ophthalmol. 1992, 114, 731–736. [Google Scholar] [CrossRef]
- Carmo, A.; Cunha-Vaz, J.G.; Carvalho, A.P.; Lopes, M.C. L-arginine transport in retinas from streptozotocin diabetic rats: Correlation with the level of IL-1 beta and NO synthase activity. Vis. Res. 1999, 39, 3817–3823. [Google Scholar] [CrossRef] [Green Version]
- Krady, J.K.; Basu, A.; Allen, C.M.; Xu, Y.; LaNoue, K.F.; Gardner, T.W.; Levison, S.W. Minocycline reduces proinflammatory cytokine expression, microglial activation, and caspase-3 activation in a rodent model of diabetic retinopathy. Diabetes 2005, 54, 1559–1565. [Google Scholar] [CrossRef]
- Ben-Mahmud, B.M.; Mann, G.E.; Datti, A.; Orlacchio, A.; Kohner, E.M.; Chibber, R. Tumor necrosis factor-alpha in diabetic plasma increases the activity of core 2 GlcNAc-T and adherence of human leukocytes to retinal endothelial cells: Significance of core 2 GlcNAc-T in diabetic retinopathy. Diabetes 2004, 53, 2968–2976. [Google Scholar] [CrossRef] [Green Version]
- Kowluru, R.A.; Odenbach, S. Role of interleukin-1beta in the development of retinopathy in rats: Effect of antioxidants. Investig. Ophthalmol. Vis. Sci. 2004, 45, 4161–4166. [Google Scholar] [CrossRef] [Green Version]
- Kowluru, R.A.; Koppolu, P.; Chakrabarti, S.; Chen, S. Diabetes-induced activation of nuclear transcriptional factor in the retina, and its inhibition by antioxidants. Free Radic. Res. 2003, 37, 1169–1180. [Google Scholar] [CrossRef] [PubMed]
- Kumar, B.; Gupta, S.K.; Nag, T.C.; Srivastava, S.; Saxena, R.; Jha, K.A.; Srinivasan, B.P. Retinal neuroprotective effects of quercetin in streptozotocin-induced diabetic rats. Exp. Eye Res. 2014, 125, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Ishida, S.; Usui, T.; Yamashiro, K.; Kaji, Y.; Ahmed, E.; Carrasquillo, K.G.; Amano, S.; Hida, T.; Oguchi, Y.; Adamis, A.P. VEGF164 is proinflammatory in the diabetic retina. Investig. Ophthalmol. Vis. Sci. 2003, 44, 2155–2162. [Google Scholar] [CrossRef] [Green Version]
- Obrosova, I.G.; Minchenko, A.G.; Vasupuram, R.; White, L.; Abatan, O.I.; Kumagai, A.K.; Frank, R.N.; Stevens, M.J. Aldose reductase inhibitor fidarestat prevents retinal oxidative stress and vascular endothelial growth factor overexpression in streptozotocin-diabetic rats. Diabetes 2003, 52, 864–871. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.X.; Ma, J.X.; Sima, J.; Chen, Y.; Hu, M.S.; Ottlecz, A.; Lambrou, G.N. Genetic difference in susceptibility to the blood-retina barrier breakdown in diabetes and oxygen-induced retinopathy. Am. J. Pathol. 2005, 166, 313–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kusari, J.; Zhou, S.; Padillo, E.; Clarke, K.G.; Gil, D.W. Effect of memantine on neuroretinal function and retinal vascular changes of streptozotocin-induced diabetic rats. Investig. Ophthalmol. Vis. Sci. 2007, 48, 5152–5159. [Google Scholar] [CrossRef]
- Hernández, C.; Burgos, R.; Cantón, A.; García-Arumí, J.; Segura, R.M.; Simó, R. Vitreous levels of vascular cell adhesion molecule and vascular endothelial growth factor in patients with proliferative diabetic retinopathy: A case-control study. Diabetes Care 2001, 24, 516–521. [Google Scholar] [CrossRef] [Green Version]
- Dongare, S.; Gupta, S.K.; Mathur, R.; Saxena, R.; Mathur, S.; Agarwal, R.; Nag, T.C.; Srivastava, S.; Kumar, P. Zingiber officinale attenuates retinal microvascular changes in diabetic rats via anti-inflammatory and antiangiogenic mechanisms. Mol. Vis. 2016, 22, 599–609. [Google Scholar]
- Lee, S.H.; Cekanova, M.; Baek, S.J. Multiple mechanisms are involved in 6-gingerol-induced cell growth arrest and apoptosis in human colorectal cancer cells. Mol. Carcinog. 2008, 47, 197–208. [Google Scholar] [CrossRef]
- Rossino, M.G.; Casini, G. Nutraceuticals for the treatment of diabetic retinopathy. Nutrients 2019, 11, 771. [Google Scholar] [CrossRef] [Green Version]
- Akhani, S.P.; Vishwakarma, S.L.; Goyal, R.K. Anti-diabetic activity of Zingiber officinale in streptozotocin-induced type I diabetic rats. J. Pharm. Pharmacol. 2004, 56, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.N.; Horng, J.S.; Yin, M.C. Antioxidative and antiglycative effects of six organosulfur compounds in low-density lipoprotein and plasma. J. Agric. Food Chem. 2004, 52, 3674–3678. [Google Scholar] [CrossRef]
- Nonn, L.; Duong, D.; Peehl, D.M. Chemopreventive anti-inflammatory activities of curcumin and other phytochemicals mediated by MAP kinase phosphatase-5 in prostate cells. Carcinogenesis 2007, 28, 1188–1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habib, S.H.; Makpol, S.; Abdul Hamid, N.A.; Das, S.; Ngah, W.Z.; Yusof, Y.A. Ginger extract (Zingiber officinale) has anti-cancer and anti-inflammatory effects on ethionine-induced hepatoma rats. Clinics 2008, 63, 807–813. [Google Scholar] [CrossRef] [Green Version]
- Kim, E.-C.; Min, J.-K.; Kim, T.-Y.; Lee, S.-J.; Yang, H.-O.; Han, S.; Kim, Y.-M.; Kwon, Y.-G. [6]-Gingerol, a pungent ingredient of ginger, inhibits angiogenesis in vitro and in vivo. Biochem. Biophys. Res. Commun. 2005, 335, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Farombi, E.O.; Ajayi, B.O.; Adedara, I.A. 6-Gingerol delays tumorigenesis in benzo [a] pyrene and dextran sulphate sodium-induced colorectal cancer in mice. Food Chem. Toxicol. 2020, 142, 111483. [Google Scholar] [CrossRef]
- Tzeng, T.-F.; Liou, S.-S.; Tzeng, Y.-C.; Liu, I.-M. Zerumbone, a phytochemical of subtropical ginger, protects against hyperglycemia-induced retinal damage in experimental diabetic rats. Nutrients 2016, 8, 449. [Google Scholar] [CrossRef] [Green Version]
- Nizami, A.A.; Gulani, A.C. Cataract. 2019. Available online: https://europepmc.org/books/nbk539699 (accessed on 11 April 2019).
- Saraswat, M.; Suryanarayana, P.; Reddy, P.Y.; Patil, M.A.; Balakrishna, N.; Reddy, G.B. Antiglycating potential of Zingiber officinalis and delay of diabetic cataract in rats. Mol. Vis. 2010, 16, 1525. [Google Scholar]
- Li, Q.; Wen, Y.; Wang, L.; Chen, B.; Chen, J.; Wang, H.; Chen, L. Hyperglycemia-induced accumulation of advanced glycosylation end products in fibroblast-like synoviocytes promotes knee osteoarthritis. Exp. Mol. Med. 2021, 53, 1735–1747. [Google Scholar] [CrossRef]
- Srivastava, K.; Mustafa, T. Ginger (Zingiber officinale) in rheumatism and musculoskeletal disorders. Med. Hypotheses 1992, 39, 342–348. [Google Scholar] [CrossRef]
- Leach, M.J.; Kumar, S. The clinical effectiveness of Ginger (Zingiber officinale) in adults with osteoarthritis. Int. J. Evid. -Based Healthc. 2008, 6, 311–320. [Google Scholar] [PubMed]
- Therkleson, T. Ginger therapy for osteoarthritis: A typical case. J. Holist. Nurs. 2014, 32, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Thomson, M.; Al-Qattan, K.; Al-Sawan, S.; Alnaqeeb, M.; Khan, I.; Ali, M. The use of ginger (Zingiber officinale Rosc.) as a potential anti-inflammatory and antithrombotic agent. Prostaglandins Leukot. Essent. Fat. Acids 2002, 67, 475–478. [Google Scholar] [CrossRef] [PubMed]
- Flynn, D.L.; Rafferty, M.F.; Boctor, A.M. Inhibition of human neutrophil 5-lipoxygenase activity by gingerdione, shogaol, capsaicin and related pungent compounds. Prostaglandins Leukot. Med. 1986, 24, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Young, H.-Y.; Luo, Y.-L.; Cheng, H.-Y.; Hsieh, W.-C.; Liao, J.-C.; Peng, W.-H. Analgesic and anti-inflammatory activities of [6]-gingerol. J. Ethnopharmacol. 2005, 96, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Sharma, J.N.; Srivastava, K.C.; Gan, E.K. Suppressive effects of eugenol and ginger oil on arthritic rats. Pharmacology 1994, 49, 314–318. [Google Scholar] [CrossRef] [PubMed]
- van Breemen, R.B.; Tao, Y.; Li, W. Cyclooxygenase-2 inhibitors in ginger (Zingiber officinale). Fitoterapia 2011, 82, 38–43. [Google Scholar] [CrossRef] [Green Version]
- Grzanna, R.; Lindmark, L.; Frondoza, C.G. Ginger—an herbal medicinal product with broad anti-inflammatory actions. J. Med. Food 2005, 8, 125–132. [Google Scholar] [CrossRef]
- Nurtjahja-Tjendraputra, E.; Ammit, A.J.; Roufogalis, B.D.; Tran, V.H.; Duke, C.C. Effective anti-platelet and COX-1 enzyme inhibitors from pungent constituents of ginger. Thromb. Res. 2003, 111, 259–265. [Google Scholar] [CrossRef]
- Pragasam, S.J.; Kumar, S.; Bhoumik, M.; Sabina, E.P.; Rasool, M. 6-Gingerol, an active ingredient of ginger suppresses monosodium ureate crystal-induced inflammation: An in vivo and in vitro evaluation. Ann Biol Res 2011, 2, 200–208. [Google Scholar]
- Lee, T.-Y.; Lee, K.-C.; Chen, S.-Y.; Chang, H.-H. 6-Gingerol inhibits ROS and iNOS through the suppression of PKC-α and NF-κB pathways in lipopolysaccharide-stimulated mouse macrophages. Biochem. Biophys. Res. Commun. 2009, 382, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Park, S.H.; Lee, M.; Kim, H.J.; Ryu, S.Y.; Kim, N.D.; Hwang, B.Y.; Hong, J.T.; Han, S.B.; Kim, Y. 1-Dehydro-[10]-gingerdione from ginger inhibits IKKβ activity for NF-κB activation and suppresses NF-κB-regulated expression of inflammatory genes. Br. J. Pharmacol. 2012, 167, 128–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Nahain, A.; Jahan, R.; Rahmatullah, M. Zingiber officinale: A potential plant against rheumatoid arthritis. Arthritis 2014, 2014, 159089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bascones-Ilundain, J.; Bascones-Martinez, A.; Matesanz-Perez, P.; Escribano-Bermejo, M.; González-Moles, M.-Á.; Meurman, J.-H. Periodontal disease and diabetes-Review of the literature. Med. Oral Patol. Oral Cir. Bucal 2011, 722–729. [Google Scholar] [CrossRef] [Green Version]
- Chang, P.-C.; Lim, L.P. Interrelationships of periodontitis and diabetes: A review of the current literature. J. Dent. Sci. 2012, 7, 272–282. [Google Scholar] [CrossRef] [Green Version]
- Janket, S.-J.; Jones, J.A.; Meurman, J.H.; Baird, A.E.; Van Dyke, T.E. Oral infection, hyperglycemia, and endothelial dysfunction. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2008, 105, 173–179. [Google Scholar] [CrossRef] [Green Version]
- Park, M.; Bae, J.; Lee, D.S. Antibacterial activity of [10]-gingerol and [12]-gingerol isolated from ginger rhizome against periodontal bacteria. Phytother. Res. Int. J. Devoted Pharmacol. Toxicol. Eval. Nat. Prod. Deriv. 2008, 22, 1446–1449. [Google Scholar] [CrossRef]
- Javid, A.Z.; Bazyar, H.; Gholinezhad, H.; Rahimlou, M.; Rashidi, H.; Salehi, P.; Haghighi-Zadeh, M.H. The effects of ginger supplementation on inflammatory, antioxidant, and periodontal parameters in type 2 diabetes mellitus patients with chronic periodontitis under non-surgical periodontal therapy. A double-blind, placebo-controlled trial. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 1751. [Google Scholar] [CrossRef] [Green Version]
- Menon, P.; Perayil, J.; Fenol, A.; Peter, M.R.; Lakshmi, P.; Suresh, R. Effectiveness of ginger on pain following periodontal surgery–A randomized cross-over clinical trial. J. Ayurveda Integr. Med. 2021, 12, 65–69. [Google Scholar] [CrossRef]
- Shen, C.-L.; Wang, R.; Elmassry, M.; Neugebauer, V.; Hamood, A. Dietary Ginger Root Extract Supplementation Mitigated Diabetic Peripheral Neuropathy in Streptozotocin-Induced Diabetic Rats by Modulating Gut Microbiota. Curr. Dev. Nutr. 2021, 5, 1179. [Google Scholar] [CrossRef]
- Fajrin, F.A.; Nugroho, A.E.; Nurrochmad, A.; Susilowati, R. Ginger extract and its compound, 6-shogaol, attenuates painful diabetic neuropathy in mice via reducing TRPV1 and NMDAR2B expressions in the spinal cord. J. Ethnopharmacol. 2020, 249, 112396. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alharbi, K.S.; Nadeem, M.S.; Afzal, O.; Alzarea, S.I.; Altamimi, A.S.A.; Almalki, W.H.; Mubeen, B.; Iftikhar, S.; Shah, L.; Kazmi, I. Gingerol, a Natural Antioxidant, Attenuates Hyperglycemia and Downstream Complications. Metabolites 2022, 12, 1274. https://doi.org/10.3390/metabo12121274
Alharbi KS, Nadeem MS, Afzal O, Alzarea SI, Altamimi ASA, Almalki WH, Mubeen B, Iftikhar S, Shah L, Kazmi I. Gingerol, a Natural Antioxidant, Attenuates Hyperglycemia and Downstream Complications. Metabolites. 2022; 12(12):1274. https://doi.org/10.3390/metabo12121274
Chicago/Turabian StyleAlharbi, Khalid Saad, Muhammad Shahid Nadeem, Obaid Afzal, Sami I. Alzarea, Abdulmalik S. A. Altamimi, Waleed Hassan Almalki, Bismillah Mubeen, Saima Iftikhar, Luqman Shah, and Imran Kazmi. 2022. "Gingerol, a Natural Antioxidant, Attenuates Hyperglycemia and Downstream Complications" Metabolites 12, no. 12: 1274. https://doi.org/10.3390/metabo12121274