
Dental Diseases Increase Risk of Aortic Arch Calcification Independent of Renal Dysfunction in Older Adults: Shenzhen Community Cohort Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Demographic Characteristics and Baseline Diameters Measurement
2.3. Radiographic Evaluation
2.4. Dental Examination
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Participants with or without AoAC
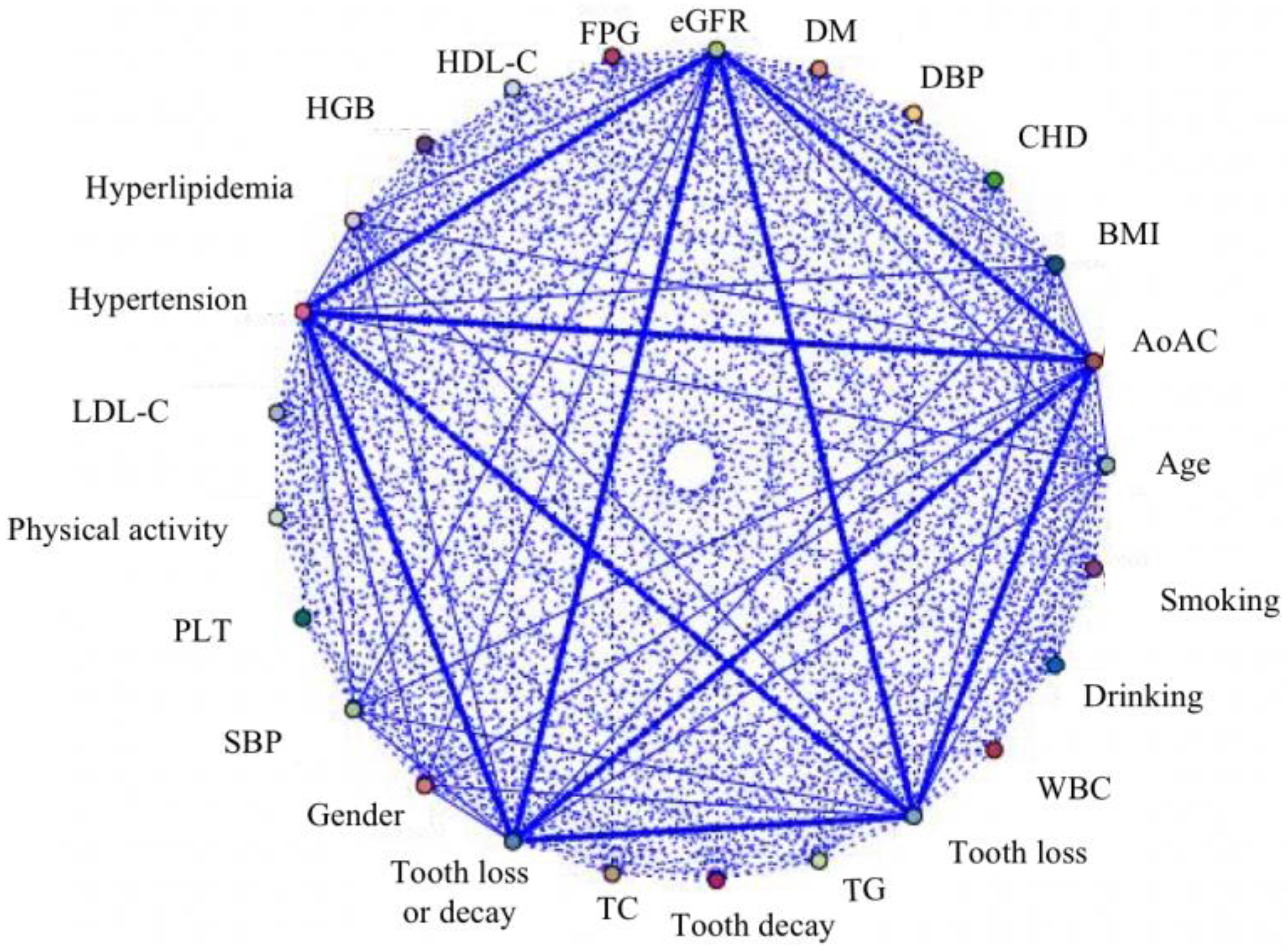
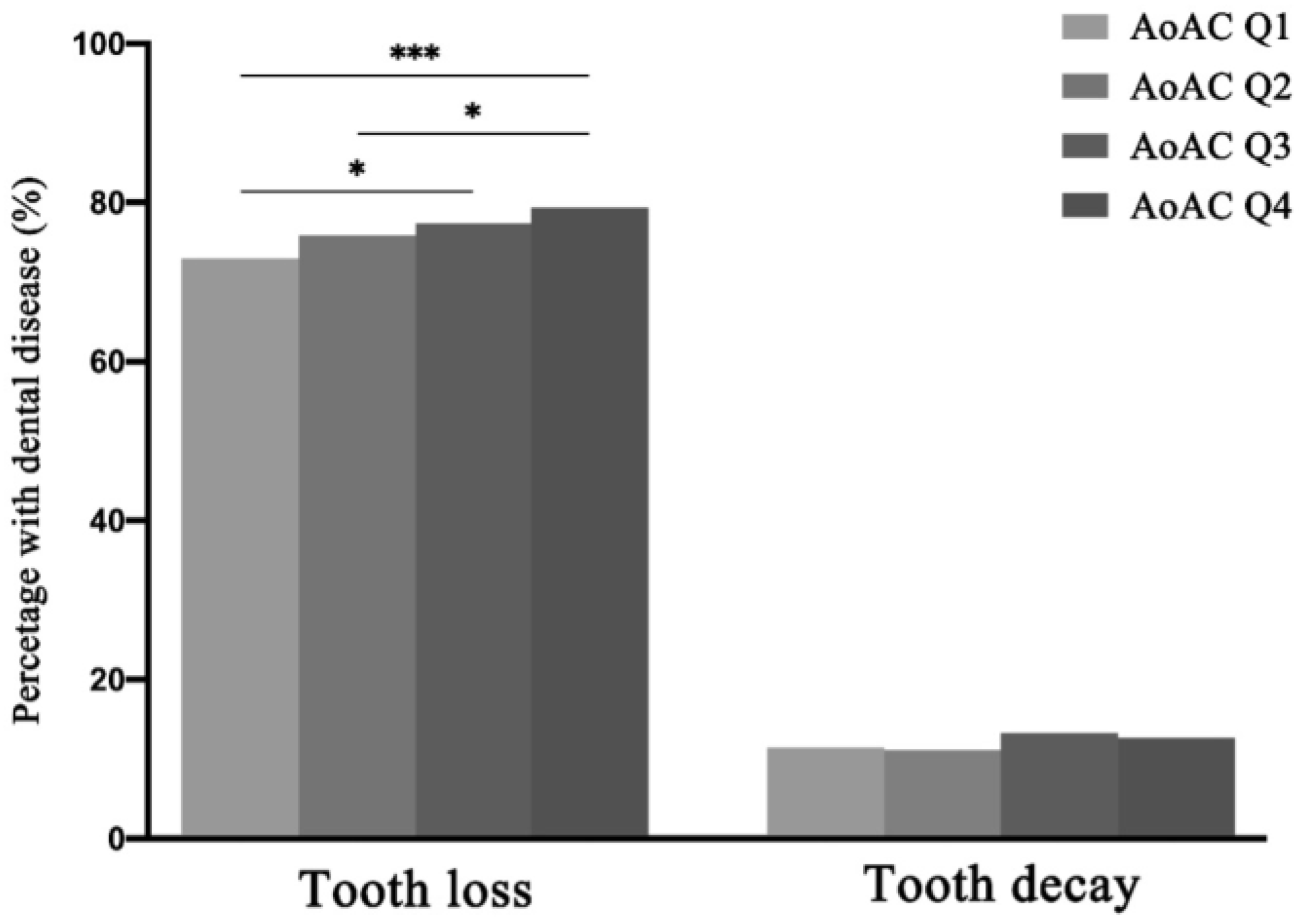
3.2. Association Rule Analysis Suggests a Strong Association between Dental Diseases and AoAC
3.3. Dental Diseases Were Independent Risk Factors for AoAC
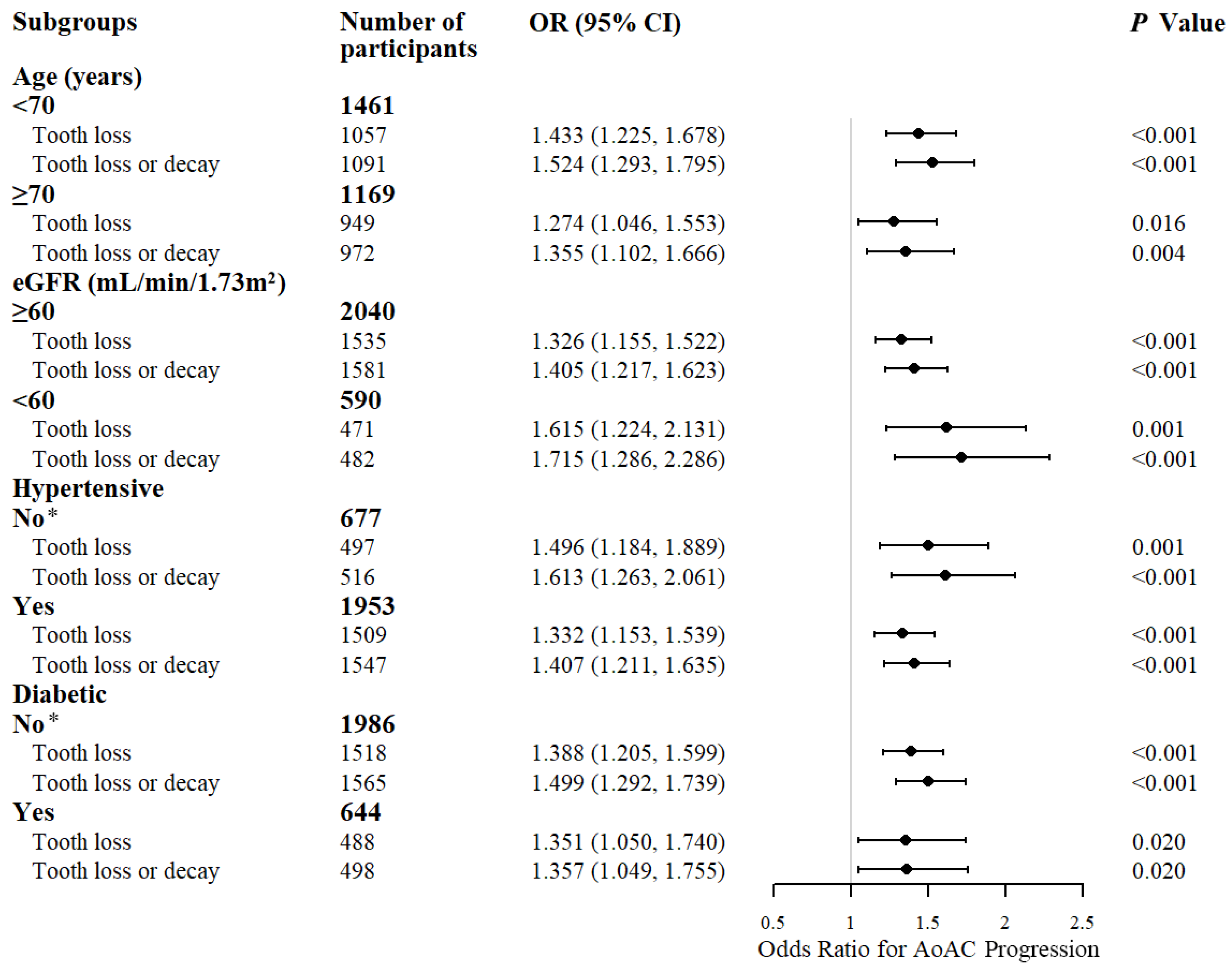
3.4. Dental Diseases Increase the Risk of AoAC Progression Independent of Renal Dysfunction
4. Discussion
5. Conclusions
6. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Colantonio, L.D.; Muntner, P. It Is Time for Reducing Global Cardiovascular Mortality. Circulation 2019, 140, 726–728. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Luo, D.; He, W.; Chen, J.; Su, X.; Huang, H. Diabetes and calcification: The potential role of anti-diabetic drugs on vascular calcification regression. Pharmacol. Res. 2020, 158, 104861. [Google Scholar] [CrossRef] [PubMed]
- Duan, M.; Zhao, W.-L.; Zhou, L.; Novák, P.; Zhu, X.; Yin, K. Omics research in vascular calcification. Clin. Chim. Acta 2020, 511, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Di Minno, M.N.D.; Poggio, P.; Conte, E.; Myasoedova, V.; Songia, P.; Mushtaq, S.; Cavallotti, L.; Moschetta, D.; Di Minno, A.; Spadarella, G.; et al. Cardiovascular morbidity and mortality in patients with aortic valve calcification: A systematic review and meta-analysis. J. Cardiovasc. Comput. Tomogr. 2019, 13, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Bartstra, J.W.; Mali, W.P.T.M.; Spiering, W.; de Jong, P.A. Abdominal aortic calcification: From ancient friend to modern foe. Eur. J. Prev. Cardiol. 2021, 28, 1386–1391. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Q.; Xiong, Q.-C.; Gupta, M.; López-Pintor, R.M.; Chen, X.-L.; Seriwatanachai, D.; Densmore, M.; Man, Y.; Gong, P. Dental implant treatment for renal failure patients on dialysis: A clinical guideline. Int. J. Oral Sci. 2017, 9, 125–132. [Google Scholar] [CrossRef] [Green Version]
- Choi, H.M.; Han, K.; Park, Y.G.; Park, J.-B. Associations between the number of natural teeth and renal dysfunction. Medicine 2016, 95, e4681. [Google Scholar] [CrossRef]
- Han, K.; Park, J.-B. Tooth loss and risk of end-stage renal disease: A nationwide cohort study. J. Periodontol. 2021, 92, 371–377. [Google Scholar] [CrossRef]
- Levy, D.S.; Grewal, R.; Le, T.H. Vitamin K deficiency: An emerging player in the pathogenesis of vascular calcification and an iatrogenic consequence of therapies in advanced renal disease. Am. J. Physiol. Renal Physiol. 2020, 319, F618–F623. [Google Scholar] [CrossRef]
- Muntner, P.; Shimbo, D.; Carey, R.M.; Charleston, J.B.; Gaillard, T.; Misra, S.; Myers, M.G.; Ogedegbe, G.; Schwartz, J.E.; Townsend, R.R.; et al. Measurement of Blood Pressure in Humans: A Scientific Statement From the American Heart Association. Hypertension 2019, 73, e35–e66. [Google Scholar] [CrossRef] [PubMed]
- Teo, B.W.; Xu, H.; Wang, D.; Li, J.; Sinha, A.K.; Shuter, B.; Sethi, S.; Lee, E.J.C. GFR estimating equations in a multiethnic Asian population. Am. J. Kidney Dis. 2011, 58, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Prieto, L.; Lamarca, R.; Casado, A.; Alonso, J. The evaluation of agreement on continuous variables by the intraclass correlation coefficient. J. Epidemiol. Community Health 1997, 51, 579–581. [Google Scholar] [CrossRef] [Green Version]
- Ogawa, T.; Ishida, H.; Matsuda, N.; Fujiu, A.; Matsuda, A.; Ito, K.; Ando, Y.; Nitta, K. Simple evaluation of aortic arch calcification by chest radiography in hemodialysis patients. Hemodial. Int. 2009, 13, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.-S. Number of existing permanent teeth is associated with chronic kidney disease in the elderly Korean population. Korean J. Intern. Med. 2018, 33, 1150–1159. [Google Scholar] [CrossRef] [Green Version]
- Morelli, T.; Agler, C.S.; Divaris, K. Genomics of periodontal disease and tooth morbidity. Periodontol. 2000 2020, 82, 143–156. [Google Scholar] [CrossRef]
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal diseases. Nat. Rev. Dis. Primers 2017, 3, 17038. [Google Scholar] [CrossRef]
- Thomson, W.M.; Barak, Y. Tooth Loss and Dementia: A Critical Examination. J. Dent. Res. 2021, 100, 226–231. [Google Scholar] [CrossRef]
- Ylöstalo, P.V.; Järvelin, M.R.; Laitinen, J.; Knuuttila, M.L. Gingivitis, dental caries and tooth loss: Risk factors for cardiovascular diseases or indicators of elevated health risks. J. Clin. Periodontol. 2006, 33, 92–101. [Google Scholar] [CrossRef]
- Lee, H.J.; Choi, E.K.; Park, J.B.; Han, K.D.; Oh, S. Tooth Loss Predicts Myocardial Infarction, Heart Failure, Stroke, and Death. J. Dent. Res. 2019, 98, 164–170. [Google Scholar] [CrossRef]
- Vedin, O.; Hagström, E.; Östlund, O.; Avezum, A.; Budaj, A.; Flather, M.D.; Harrington, R.A.; Koenig, W.; Soffer, J.; Siegbahn, A.; et al. Associations between tooth loss and prognostic biomarkers and the risk for cardiovascular events in patients with stable coronary heart disease. Int. J. Cardiol. 2017, 245, 271–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beukers, N.G.F.M.; Su, N.; Loos, B.G.; van der Heijden, G.J.M.G. Lower Number of Teeth Is Related to Higher Risks for ACVD and Death-Systematic Review and Meta-Analyses of Survival Data. Front. Cardiovasc. Med. 2021, 8, 621626. [Google Scholar] [CrossRef] [PubMed]
- Polzer, I.; Schwahn, C.; Völzke, H.; Mundt, T.; Biffar, R. The association of tooth loss with all-cause and circulatory mortality. Is there a benefit of replaced teeth? A systematic review and meta-analysis. Clin. Oral Investig. 2012, 16, 333–351. [Google Scholar] [CrossRef] [PubMed]
- Donders, H.C.M.; LM, I.J.; Soffner, M.; van ’t Hof, A.W.J.; Loos, B.G.; de Lange, J. Elevated Coronary Artery Calcium scores are associated with tooth loss. PLoS ONE 2020, 15, e0243232. [Google Scholar] [CrossRef] [PubMed]
- Holmlund, A.; Lind, L. Number of teeth is related to atherosclerotic plaque in the carotid arteries in an elderly population. J. Periodontol. 2012, 83, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Lanzer, P.; Hannan, F.M.; Lanzer, J.D.; Janzen, J.; Raggi, P.; Furniss, D.; Schuchardt, M.; Thakker, R.; Fok, P.-W.; Saez-Rodriguez, J.; et al. Medial Arterial Calcification: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2021, 78, 1145–1165. [Google Scholar] [CrossRef] [PubMed]
- Yao, H.; Sun, Z.; Zang, G.; Zhang, L.; Hou, L.; Shao, C.; Wang, Z. Epidemiological Research Advances in Vascular Calcification in Diabetes. J. Diabetes Res. 2021, 2021, 4461311. [Google Scholar] [CrossRef]
- Wangerin, C.; Pink, C.; Endlich, K.; Rettig, R.; Stracke, S.; Nauck, M.; Völzke, H.; Kocher, T.; Holtfreter, B. Long-term Association of Periodontitis With Decreased Kidney Function. Am. J. Kidney Dis. 2019, 73, 513–524. [Google Scholar] [CrossRef]
- Chang, Y.; Lee, J.S.; Lee, K.-J.; Woo, H.G.; Song, T.-J. Improved oral hygiene is associated with decreased risk of new-onset diabetes: A nationwide population-based cohort study. Diabetologia 2020, 63, 924–933. [Google Scholar] [CrossRef]
- Lee, H.Y.; Lim, S.; Park, S. Role of Inflammation in Arterial Calcification. Korean Circ. J. 2021, 51, 114–125. [Google Scholar] [CrossRef]
- Shen, J.; Zhao, M.; Zhang, C.; Sun, X. IL-1β in atherosclerotic vascular calcification: From bench to bedside. Int. J. Biol. Sci. 2021, 17, 4353–4364. [Google Scholar] [CrossRef] [PubMed]
- Zeb, I.; Jorgensen, N.W.; Blumenthal, R.S.; Burke, G.L.; Lloyd-Jones, D.; Blaha, M.J.; Wong, N.D.; Nasir, K.; Budoff, M.J. Association of inflammatory markers and lipoprotein particle subclasses with progression of coronary artery calcium: The multi-ethnic study of atherosclerosis. Atherosclerosis 2021, 339, 27–34. [Google Scholar] [CrossRef] [PubMed]
- López-Mejías, R.; González-Gay, M.A. IL-6: Linking chronic inflammation and vascular calcification. Nat. Rev. Rheumatol. 2019, 15, 457–459. [Google Scholar] [CrossRef]
- Yu, B.; Wang, C.Y. Osteoporosis and periodontal diseases—An update on their association and mechanistic links. Periodontol. 2000 2022, 89, 99–113. [Google Scholar] [CrossRef] [PubMed]
- Nicopoulou-Karayianni, K.; Tzoutzoukos, P.; Mitsea, A.; Karayiannis, A.; Tsiklakis, K.; Jacobs, R.; Lindh, C.; van der Stelt, P.; Allen, P.; Graham, J.; et al. Tooth loss and osteoporosis: The OSTEODENT Study. J. Clin. Periodontol. 2009, 36, 190–197. [Google Scholar] [CrossRef]
- Taguchi, A.; Kobayashi, J.; Suei, Y.; Ohtsuka, M.; Tanimoto, K.; Sanada, M.; Ohama, K. Relationship between estrogen-receptor genotype and tooth loss in postmenopausal women. JAMA 2001, 286, 2234–2235. [Google Scholar] [CrossRef]
- Karohl, C.; D’Marco Gascón, L.; Raggi, P. Noninvasive imaging for assessment of calcification in chronic kidney disease. Nat. Rev. Nephrol. 2011, 7, 567–577. [Google Scholar] [CrossRef]
- Ma, X.; Hou, F.; Tian, J.; Zhou, Z.; Ma, Y.; Cheng, Y.; Du, Y.; Shen, H.; Hu, B.; Wang, Z.; et al. Aortic Arch Calcification Is a Strong Predictor of the Severity of Coronary Artery Disease in Patients with Acute Coronary Syndrome. BioMed Res. Int. 2019, 2019, 7659239. [Google Scholar] [CrossRef] [Green Version]
- Chung, T.-L.; Liu, Y.-H.; Huang, J.-C.; Wu, P.-Y.; Tu, H.-P.; Chen, S.-C.; Chang, J.-M. Prognostic Implication of Longitudinal Changes in Cardiothoracic Ratio and Aortic Arch Calcification in Hemodialysis Patients. J. Pers. Med. 2021, 11, 788. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Subjects | Non-AoAC | AoAC | p-Value | |
|---|---|---|---|---|
| Number | 9463 | 1432 | 8031 | |
| Demographics | ||||
| Age, years | 70.76 ± 5.74 | 69.59 ± 4.87 | 70.97 ± 5.86 | <0.001 |
| Female, n (%) | 5441 (57.50) | 717 (50.07) | 4724 (58.82) | <0.001 |
| SBP, mmHg | 136.39 ± 17.47 | 134.90 ± 17.22 | 136.65 ± 17.50 | <0.001 |
| DBP, mmHg | 77.36 ± 10.34 | 77.22 ± 10.39 | 77.39 ± 10.33 | 0.555 |
| BMI, kg/m2 | 24.02 ± 3.13 | 24.07 ± 3.03 | 24.01 ± 3.15 | 0.497 |
| Medical history | ||||
| CHD, n (%) | 906 (9.57) | 136 (9.50) | 770 (9.59) | 0.953 |
| Hypertension, n (%) | 7648 (80.82) | 1082 (75.56) | 6566 (81.76) | <0.001 |
| Diabetes Mellitus, n (%) | 1963 (20.74) | 287 (20.04) | 1676 (20.87) | 0.499 |
| Hyperlipidemia, n (%) | 3627 (38.33) | 470 (32.82) | 3157 (39.31) | <0.001 |
| Dental health | ||||
| Tooth loss, n (%) | 7278 (76.91) | 1044 (72.91) | 6234 (77.62) | <0.001 |
| Tooth decay, n (%) | 1160 (12.26) | 163 (11.38) | 997 (12.41) | 0.292 |
| Tooth loss or decay, n (%) | 7550 (79.78) | 1077 (75.21) | 6473 (80.60) | <0.001 |
| Hematology and biochemical test | ||||
| WBC, 109/L | 6.20 (5.20, 7.20) | 6.20 (5.39, 7.30) | 6.12 (5.20, 7.20) | 0.063 |
| HGB, g/L | 134.43 ± 13.51 | 136.04 ± 13.41 | 134.14 ± 13.51 | <0.001 |
| PLT, 109/L | 208.70 ± 50.04 | 209.98 ± 50.10 | 208.47 ± 50.03 | 0.294 |
| TG, mmol/L | 1.28 (0.94, 1.78) | 1.29 (0.94, 1.78) | 1.28 (0.94, 1.78) | 0.814 |
| TC, mmol/L | 5.03 (4.34, 5.75) | 4.98 (4.32, 5.67) | 5.03 (4.34, 5.76) | 0.075 |
| LDL-C, mmol/L | 2.90 (2.28, 3.55) | 2.88 (2.32, 3.49) | 2.91 (2.27, 3.56) | 0.703 |
| HDL-C, mmol/L | 1.40 (1.19, 1.67) | 1.38 (1.15, 1.61) | 1.41 (1.20, 1.68) | <0.001 |
| FPG, mmol/L | 5.46 (4.94, 6.24) | 5.42 (4.86, 6.21) | 5.46 (4.96, 6.24) | 0.022 |
| eGFR, mL/min/1.73 m2 | 72.95 (64.11, 86.58) | 70.21 (63.55, 77.78) | 73.63 (64.36, 88.18) | <0.001 |
| Lifestyle | ||||
| Smoking, n (%) | 1526 (16.13) | 243 (16.97) | 1283 (15.98) | 0.367 |
| Drinking, n (%) | 2092 (22.11) | 337 (23.53) | 1755 (21.85) | 0.168 |
| Physical activity hours/week, n (%) | 0.122 | |||
| <3 h | 2256 (23.84) | 330 (23.04) | 1926 (23.98) | |
| 3–10 h | 6101 (64.47) | 912 (63.69) | 5189 (64.61) | |
| >10 h | 1106 (11.69) | 190 (13.27) | 916 (11.41) |
| Variables | OR | 95% CI | p Value |
| Unadjusted | |||
| Tooth loss | 1.289 | 1.135–1.465 | <0.001 |
| Tooth decay | 1.103 | 0.925–1.316 | 0.273 |
| Tooth loss or decay | 1.369 | 1.200–1.563 | <0.001 |
| Model 1 | |||
| Tooth loss | 1.172 | 1.028–1.336 | 0.018 |
| Tooth decay | 1.113 | 0.932–1.329 | 0.236 |
| Tooth loss or decay | 1.248 | 1.090–1.428 | 0.001 |
| Model 2 | |||
| Tooth loss | 1.154 | 1.012–1.317 | 0.032 |
| Tooth decay | 1.091 | 0.913–1.303 | 0.337 |
| Tooth loss or decay | 1.223 | 1.068–1.401 | 0.004 |
| Model 3 | |||
| Tooth loss | 1.110 | 0.971–1.268 | 0.125 |
| Tooth decay | 1.015 | 0.848–1.216 | 0.868 |
| Tooth loss or decay | 1.158 | 1.010–1.329 | 0.036 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yin, L.; Zhang, Z.; Xie, C.; Luo, D.; He, W.; Huang, S.; Huang, H. Dental Diseases Increase Risk of Aortic Arch Calcification Independent of Renal Dysfunction in Older Adults: Shenzhen Community Cohort Study. Metabolites 2022, 12, 1258. https://doi.org/10.3390/metabo12121258
Yin L, Zhang Z, Xie C, Luo D, He W, Huang S, Huang H. Dental Diseases Increase Risk of Aortic Arch Calcification Independent of Renal Dysfunction in Older Adults: Shenzhen Community Cohort Study. Metabolites. 2022; 12(12):1258. https://doi.org/10.3390/metabo12121258
Chicago/Turabian StyleYin, Li, Zhengzhipeng Zhang, Changming Xie, Dongling Luo, Wanbing He, Suli Huang, and Hui Huang. 2022. "Dental Diseases Increase Risk of Aortic Arch Calcification Independent of Renal Dysfunction in Older Adults: Shenzhen Community Cohort Study" Metabolites 12, no. 12: 1258. https://doi.org/10.3390/metabo12121258