
Development and Validation of Risk Prediction Models for Gestational Diabetes Mellitus Using Four Different Methods
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Outcomes
2.3. Clinical Measurements and Definitions
2.4. Data Collection and Detection of Plasma Biochemical Parameters
2.5. Derivation Cohort for the Score-Scaled GDM Risk Prediction Model
2.6. Statistical Analysis
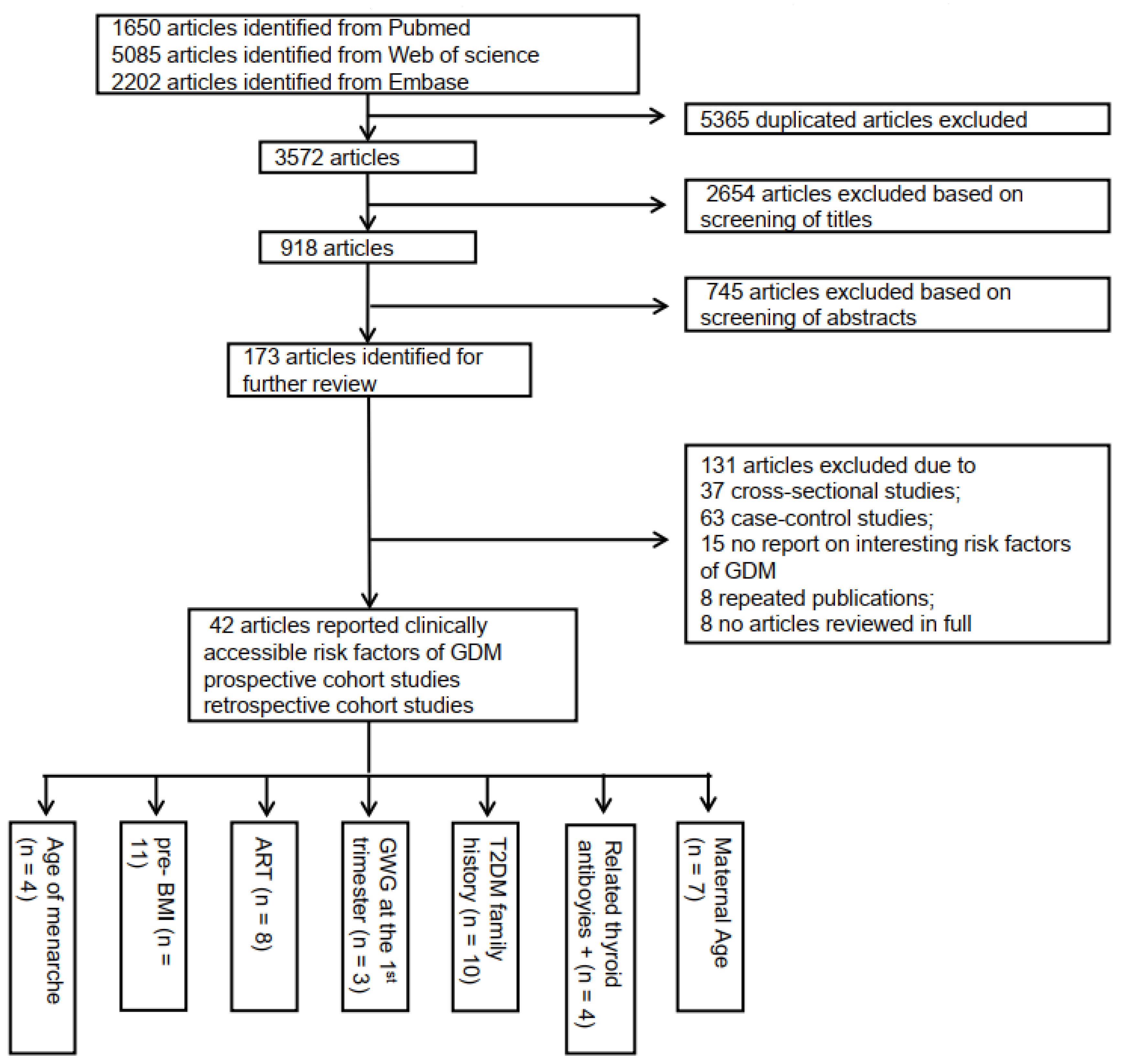
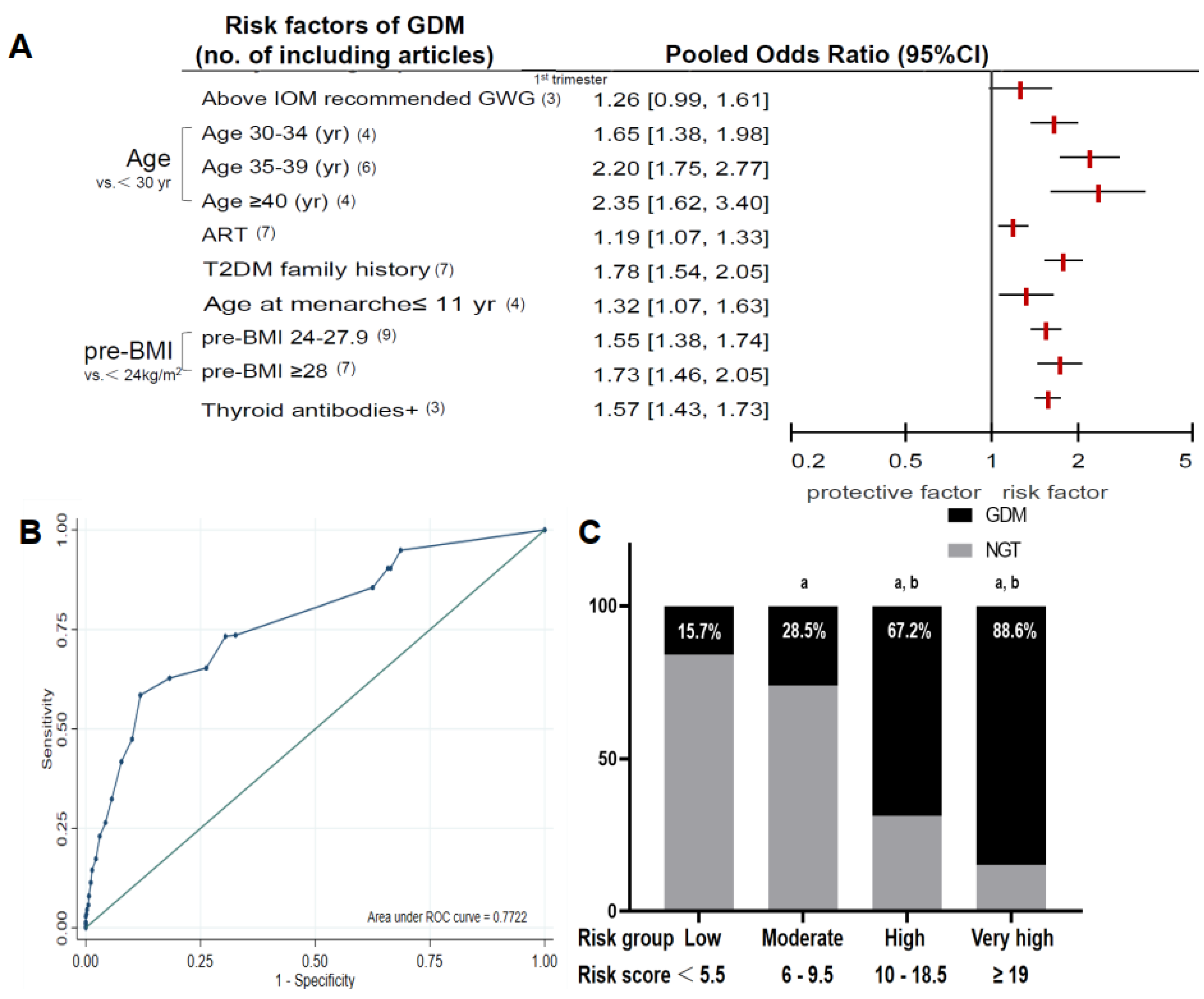
2.6.1. Meta-Analysis
2.6.2. Multiple Imputations
2.6.3. The Logistic Regression Modeling Strategy
2.6.4. The Machine Learning (ML) Algorithms
2.7. Development and Validation of the Models
2.7.1. The Score-Scaled GDM Risk Prediction Model
2.7.2. Logistic Regression Analysis for GDM Risk Prediction Model
2.7.3. ML Prediction Models
3. Results
3.1. The Score-Scaled GDM Risk Prediction Model
3.1.1. Derivation Cohort
3.1.2. Validation Cohort
3.2. Logistic Regression Analysis for the GDM Risk Prediction Model
3.2.1. Training Set
3.2.2. Discriminant Analysis
3.3. Comparison of the Two Prediction Models
3.4. ML Models for GDM Prediction
3.5. Validation of the Established Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| GDM | gestational diabetes mellitus |
| ML | machine learning |
| AUC | area under the curve |
| NGT | normal glucose tolerance |
| OGTT | oral glucose tolerance test |
| pre-BMI | pre-pregnancy body mass index |
| GWG | gestational weight gain |
| TPO-Ab | thyroid peroxidase antibody |
| Tg-Ab | thyroglobulin antibody |
| ART | assisted reproductive technology |
| ALT | glutamic-pyruvic transaminase |
| AST | glutamic oxalacetic transaminase |
| CHO | total cholesterol |
| TG | triglyceride |
| HDL-C | high-density lipoprotein cholesterol |
| LDL-C | low-density lipoprotein cholesterol |
References
- American Diabetes Association Professional Practice Committee. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45, S17–S38. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Newton, K.M.; Knopp, R.H. Gestational diabetes and the incidence of type 2 diabetes: A systematic review. Diabetes Care 2002, 25, 1862–1868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabbe, S.G. Gestational diabetes mellitus. N. Engl. J. Med. 1986, 315, 1025–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sletner, L.; Jenum, A.K.; Yajnik, C.S.; Morkrid, K.; Nakstad, B.; Rognerud-Jensen, O.H.; Birkeland, K.I.; Vangen, S. Fetal growth trajectories in pregnancies of European and South Asian mothers with and without gestational diabetes, a population-based cohort study. PLoS ONE 2017, 12, e0172946. [Google Scholar] [CrossRef] [Green Version]
- Sovio, U.; Murphy, H.R.; Smith, G.C. Accelerated Fetal Growth Prior to Diagnosis of Gestational Diabetes Mellitus: A Prospective Cohort Study of Nulliparous Women. Diabetes Care 2016, 39, 982–987. [Google Scholar] [CrossRef] [Green Version]
- Leong, I. Diabetes: ANGPTL8 as an early predictor of gestational diabetes mellitus. Nat. Rev. Endocrinol. 2018, 14, 64. [Google Scholar] [CrossRef]
- Ning, H.; Tao, H.; Weng, Z.; Zhao, X. Plasma fatty acid-binding protein 4 (FABP4) as a novel biomarker to predict gestational diabetes mellitus. Acta Diabetol. 2016, 53, 891–898. [Google Scholar] [CrossRef]
- Bao, W.; Baecker, A.; Song, Y.; Kiely, M.; Liu, S.; Zhang, C. Adipokine levels during the first or early second trimester of pregnancy and subsequent risk of gestational diabetes mellitus: A systematic review. Metabolism 2015, 64, 756–764. [Google Scholar] [CrossRef] [Green Version]
- Santos, S.; Voerman, E.; Amiano, P.; Barros, H.; Beilin, L.J.; Bergstrom, A.; Charles, M.A.; Chatzi, L.; Chevrier, C.; Chrousos, G.P.; et al. Impact of maternal body mass index and gestational weight gain on pregnancy complications: An individual participant data meta-analysis of European, North American and Australian cohorts. BJOG 2019, 126, 984–995. [Google Scholar] [CrossRef]
- Kim, S.Y.; England, L.; Wilson, H.G.; Bish, C.; Satten, G.A.; Dietz, P. Percentage of gestational diabetes mellitus attributable to overweight and obesity. Am. J. Public Health 2010, 100, 1047–1052. [Google Scholar] [CrossRef]
- Yen, I.W.; Lee, C.N.; Lin, M.W.; Fan, K.C.; Wei, J.N.; Chen, K.Y.; Chen, S.C.; Tai, Y.Y.; Kuo, C.H.; Lin, C.H.; et al. Overweight and obesity are associated with clustering of metabolic risk factors in early pregnancy and the risk of GDM. PLoS ONE 2019, 14, e0225978. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ren, X.; He, L.; Li, J.; Zhang, S.; Chen, W. Maternal age and the risk of gestational diabetes mellitus: A systematic review and meta-analysis of over 120 million participants. Diabetes Res. Clin. Prac. 2020, 162, 108044. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.A.; Nikravan, R.; Smith, H.C.; Sullivan, E.A. Higher prevalence of gestational diabetes mellitus following assisted reproduction technology treatment. Hum. Reprod. 2013, 28, 2554–2561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petry, C.J.; Ong, K.K.; Hughes, I.A.; Acerini, C.L.; Dunger, D.B. The association between age at menarche and later risk of gestational diabetes is mediated by insulin resistance. Acta Diabetol. 2018, 55, 853–859. [Google Scholar] [CrossRef] [Green Version]
- Dereke, J.; Palmqvist, S.; Nilsson, C.; Landin-Olsson, M.; Hillman, M. The prevalence and predictive value of the SLC30A8 R325W polymorphism and zinc transporter 8 autoantibodies in the development of GDM and postpartum type 1 diabetes. Endocrine 2016, 53, 740–746. [Google Scholar] [CrossRef]
- Kang, M.; Zhang, H.; Zhang, J.; Huang, K.; Zhao, J.; Hu, J.; Lu, C.; Shao, J.; Weng, J.; Yang, Y.; et al. A Novel Nomogram for Predicting Gestational Diabetes Mellitus During Early Pregnancy. Front. Endocrinol. 2021, 12, 779210. [Google Scholar] [CrossRef]
- Schoenaker, D.; Vergouwe, Y.; Soedamah-Muthu, S.S.; Callaway, L.K.; Mishra, G.D. Preconception risk of gestational diabetes: Development of a prediction model in nulliparous Australian women. Diabetes Res. Clin. Prac. 2018, 146, 48–57. [Google Scholar] [CrossRef]
- Sweeting, A.N.; Appelblom, H.; Ross, G.P.; Wong, J.; Kouru, H.; Williams, P.F.; Sairanen, M.; Hyett, J.A. First trimester prediction of gestational diabetes mellitus: A clinical model based on maternal demographic parameters. Diabetes Res. Clin. Prac. 2017, 127, 44–50. [Google Scholar] [CrossRef]
- Zheng, T.; Ye, W.; Wang, X.; Li, X.; Zhang, J.; Little, J.; Zhou, L.; Zhang, L. A simple model to predict risk of gestational diabetes mellitus from 8 to 20 weeks of gestation in Chinese women. BMC Pregnancy Childbirth 2019, 19, 252. [Google Scholar] [CrossRef] [Green Version]
- Guo, F.; Yang, S.; Zhang, Y.; Yang, X.; Zhang, C.; Fan, J. Nomogram for prediction of gestational diabetes mellitus in urban, Chinese, pregnant women. BMC Pregnancy Childbirth 2020, 20, 43. [Google Scholar] [CrossRef]
- Zhang, X.; Zhao, X.; Huo, L.; Yuan, N.; Sun, J.; Du, J.; Nan, M.; Ji, L. Risk prediction model of gestational diabetes mellitus based on nomogram in a Chinese population cohort study. Sci. Rep. 2020, 10, 21223. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2011, 34 (Suppl. 1), S62–S69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.; Lu, F.C.; Department of Disease Control Ministry of Health, PR China. The guidelines for prevention and control of overweight and obesity in Chinese adults. Biomed. Environ. Sci. 2004, 17, 1–36. [Google Scholar] [PubMed]
- Institute of Medicine (US); National Research Council (US). Weight Gain During Pregnancy: Reexamining the Guidelines; Rasmussen, K.M., Yaktine, A.L., Eds.; The National Academies Collection: Reports funded by National Institutes of Health; National Academies Press (US): Washington, DC, USA, 2009. [Google Scholar]
- Wang, L.; Yan, B.; Shi, X.; Song, H.; Su, W.; Huang, B.; Zhang, Y.; Wang, S.; Lv, F.; Lin, M.; et al. Age at menarche and risk of gestational diabetes mellitus: A population-based study in Xiamen, China. BMC Pregnancy Childbirth 2019, 19, 138. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Li, S.; He, C.; Zhu, Y.; Buck Louis, G.M.; Yeung, E.; Hu, F.B.; Zhang, C. Age at Menarche and Risk of Gestational Diabetes Mellitus: A Prospective Cohort Study Among 27,482 Women. Diabetes Care 2016, 39, 469–471. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Shen, L.; Song, L.; Liu, B.; Zheng, X.; Xu, S.; Wang, Y. Early age at menarche and gestational diabetes mellitus risk: Results from the Healthy Baby Cohort study. Diabetes Metab. 2017, 43, 248–252. [Google Scholar] [CrossRef]
- Coustan, D.R.; Berkowitz, R.L.; Hobbins, J.C. Tight metabolic control of overt diabetes in pregnancy. Am. J. Med. 1980, 68, 845–852. [Google Scholar] [CrossRef]
- Woodward, M. Epidemiology: Study Design and Data Analysis; Taylor & Francis: Oxfordshire, UK, 2000. [Google Scholar]
- Deeks, J.J.; Higgins, J.; Altman, D. Cochrane Handbook: General Methods for Cochrane Reviews: Ch 9: Analysing Data and Undertaking Meta-Analyses; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Greenland, S. Sensitivity Analysis and Bias Analysis; Springer: New York, NY, USA, 2014. [Google Scholar]
- Sullivan, L.M.; Massaro, J.M.; D′Agostino, R.B.; Sullivan, L.M.; Massaro, J.M.; D’Agostino, R.B. SrPresentation of multivariate data for clinical use: The Framingham Study risk score functions. Stat. Med. 2004, 23, 1631–1660. [Google Scholar] [CrossRef]
- Cook, N. NR: Use and misuse of the receiver operating characteristic curve in risk prediction. Circulation 2007, 115, 928–935. [Google Scholar] [CrossRef] [Green Version]
- Powe, C.E. Early Pregnancy Biochemical Predictors of Gestational Diabetes Mellitus. Curr. Diabetes Rep. 2017, 17, 12. [Google Scholar] [CrossRef]
- Saeedi, M.; Hanson, U.; Simmons, D.; Fadl, H. Characteristics of different risk factors and fasting plasma glucose for identifying GDM when using IADPSG criteria: A cross-sectional study. BMC Pregnancy Childbirth 2018, 18, 225. [Google Scholar] [CrossRef] [PubMed]
- Benhalima, K.; Van Crombrugge, P.; Moyson, C.; Verhaeghe, J.; Vandeginste, S.; Verlaenen, H.; Vercammen, C.; Maes, T.; Dufraimont, E.; De Block, C.; et al. Estimating the risk of gestational diabetes mellitus based on the 2013 WHO criteria: A prediction model based on clinical and biochemical variables in early pregnancy. Acta Diabetol. 2020, 57, 661–671. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Wang, X.; Yuan, L.; Guo, L. Association of thyroid disorders with gestational diabetes mellitus: A meta-analysis. Endocrine 2021, 73, 550–560. [Google Scholar] [CrossRef] [PubMed]
- Montaner, P.; Juan, L.; Campos, R.; Gil, L.; Corcoy, R. Is thyroid autoimmunity associated with gestational diabetes mellitus? Metabolism 2008, 57, 522–525. [Google Scholar] [CrossRef]
- Yang, M.; Du, C.; Wang, Y.; Liu, J. CD19(+)CD24(hi)CD38(hi) regulatory B cells are associated with insulin resistance in type I Hashimoto′s thyroiditis in Chinese females. Exp. Ther. Med. 2017, 14, 3887–3893. [Google Scholar] [CrossRef] [Green Version]
- Correa, P.J.; Venegas, P.; Palmeiro, Y.; Albers, D.; Rice, G.; Roa, J.; Cortez, J.; Monckeberg, M.; Schepeler, M.; Osorio, E.; et al. First trimester prediction of gestational diabetes mellitus using plasma biomarkers: A case-control study. J. Perinat. Med. 2019, 47, 161–168. [Google Scholar] [CrossRef]
- Nombo, A.P.; Mwanri, A.W.; Brouwer-Brolsma, E.M.; Ramaiya, K.L.; Feskens, E.J.M. Gestational diabetes mellitus risk score: A practical tool to predict gestational diabetes mellitus risk in Tanzania. Diabetes Res. Clin. Prac. 2018, 145, 130–137. [Google Scholar] [CrossRef]
- Artzi, N.S.; Shilo, S.; Hadar, E.; Rossman, H.; Barbash-Hazan, S.; Ben-Haroush, A.; Balicer, R.D.; Feldman, B.; Wiznitzer, A.; Segal, E. Prediction of gestational diabetes based on nationwide electronic health records. Nat. Med. 2020, 26, 71–76. [Google Scholar] [CrossRef]
- World Health Organization. Obesity:Preventing and Managing the Global Epidemic; Publications of World Health Organization: Geneva, Switzerland, 1999. [Google Scholar]
- Zhou, B.-f. Effect of Body Mass Index on All-cause Mortality and Incidence of Cardiovascular Diseases—Report for Meta-Analysis of Prospective Studies on Optimal Cut-off Points of Body Mass Index in Chinese Adults. Biomed. Environ. Sci. 2002, 03, 60–67. [Google Scholar]
- Wu, Y.T.; Zhang, C.J.; Mol, B.W.; Kawai, A.; Li, C.; Chen, L.; Wang, Y.; Sheng, J.Z.; Fan, J.X.; Shi, Y.; et al. Early Prediction of Gestational Diabetes Mellitus in the Chinese Population via Advanced Machine Learning. J. Clin. Endocrinol. Metab. 2021, 106, e1191–e1205. [Google Scholar] [CrossRef]
- Qi, Y.; Sun, X.; Tan, J.; Zhang, G.; Chen, M.; Xiong, Y.; Chen, P.; Liu, C.; Zou, K.; Liu, X. Excessive gestational weight gain in the first and second trimester is a risk factor for gestational diabetes mellitus among women pregnant with singletons: A repeated measures analysis. J. Diabetes Investig. 2020, 11, 1651–1660. [Google Scholar] [CrossRef] [PubMed]
- Hedderson, M.M.; Gunderson, E.P.; Ferrara, A. Gestational Weight Gain and Risk of Gestational Diabetes Mellitus. Obstet. Gynecol. 2010, 115, 597–604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, C.; Li, X.; Chen, R.; Zhou, X.; Liu, C.; Wu, J.; Xu, S.; Wang, W.; Xiao, M.; Xiong, G.; et al. Greater early and mid-pregnancy gestational weight gain are associated with increased risk of gestational diabetes mellitus: A prospective cohort study. Clin. Nutr. ESPEN 2017, 22, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Dishi, M.; Enquobahrie, D.A.; Abetew, D.F.; Qiu, C.; Rudra, C.B.; Williams, M.A. Age at menarche, menstrual cycle characteristics and risk of gestational diabetes. Diabetes Res. Clin. Prac. 2011, 93, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Hu, H.; Taylor, B.D.; Kan, H.; Xu, X. Early Menarche and Gestational Diabetes Mellitus at First Live Birth. Matern. Child Heal. J. 2016, 21, 593–598. [Google Scholar] [CrossRef]
- Ying, H.; Tang, Y.-P.; Bao, Y.-R.; Su, X.-J.; Cai, X.; Li, Y.-H.; Wang, D.-F. Maternal TSH level and TPOAb status in early pregnancy and their relationship to the risk of gestational diabetes mellitus. Endocrine 2016, 54, 742–750. [Google Scholar] [CrossRef]
- Li, G.; Wei, T.; Ni, W.; Zhang, A.; Zhang, J.; Xing, Y.; Xing, Q. Incidence and Risk Factors of Gestational Diabetes Mellitus: A Prospective Cohort Study in Qingdao, China. Front. Endocrinol. 2020, 11. [Google Scholar] [CrossRef]
- Männistö, T.; Mendola, P.; Grewal, J.; Xie, Y.; Chen, Z.; Laughon, S.K. Thyroid Diseases and Adverse Pregnancy Outcomes in a Contemporary US Cohort. J. Clin. Endocrinol. Metab. 2013, 98, 2725–2733. [Google Scholar] [CrossRef]
- Yang, S.; Shi, F.-T.; Leung, P.; Huang, H.-F.; Fan, J. Low Thyroid Hormone in Early Pregnancy Is Associated With an Increased Risk of Gestational Diabetes Mellitus. J. Clin. Endocrinol. Metab. 2016, 101, 4237–4243. [Google Scholar] [CrossRef]
- Lei, L.L.; Lan, Y.L.; Wang, S.Y.; Feng, W.; Zhai, Z.J. Perinatal complications and live-birth outcomes following assisted reproductive technology: A retrospective cohort study. Chin. Med. J.-Peking 2019, 132, 2408–2416. [Google Scholar] [CrossRef]
- Barua, S.; Hng, T.-M.; Smith, H.; Bradford, J.; McLean, M. Ovulatory disorders are an independent risk factor for pregnancy complications in women receiving assisted reproduction treatments. Aust. N. Z. J. Obstet. Gynaecol. 2016, 57, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.Q.; Xu, B.; Zhang, Y.N.; Jin, L. Risk factors of gestational diabetes mellitus during assisted reproductive technology procedures. Gynecol. Endocrinol. 2020, 36, 318–321. [Google Scholar]
- Nagata, C.; Yang, L.M.; Yamamoto-Hanada, K.; Mezawa, H.; Ayabe, T.; Ishizuka, K.; Konishi, M.; Ohya, Y.; Saito, H.; Sago, H.; et al. Complications and adverse outcomes in pregnancy and childbirth among women who conceived by assisted reproductive technologies: A nationwide birth cohort study of Japan environment and children’s study. Bmc Pregnancy Childb. 2019, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shevell, T.; Malone, F.D.; Vidaver, J.; Porter, T.; A Luthy, D.; Comstock, C.H.; Hankins, G.D.; Eddleman, K.; Dolan, S.; Dugoff, L.; et al. Assisted reproductive technology and pregnancy outcome–a population based screening study (the faster trial). Am. J. Obstet. Gynecol. 2003, 189, S175. [Google Scholar] [CrossRef]
- Silberstein, T.; Sheiner, E.; Levy, A.; Harlev, A.; Saphier, O. 520: Perinatal outcome of pregnancies following in vitro fertilization and ovulation induction. Am. J. Obstet. Gynecol. 2014, 210, S257. [Google Scholar] [CrossRef]
- Stern, J.E.; Luke, B.; Tobias, M.; Gopal, D.; Hornstein, M.D.; Diop, H. Adverse pregnancy and birth outcomes associated with underlying diagnosis with and without assisted reproductive technology treatment. Fertil. Steril. 2015, 103, 1438–1445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cosson, E.; Cussac-Pillegand, C.; Benbara, A.; Pharisien, I.; Jaber, Y.; Banu, I.; Nguyen, M.T.; Valensi, P.; Carbillon, L. The Diagnostic and Prognostic Performance of a Selective Screening Strategy for Gestational Diabetes Mellitus According to Ethnicity in Europe. J. Clin. Endocrinol. Metab. 2014, 99, 996–1005. [Google Scholar] [CrossRef] [Green Version]
- Hosseini, E.; Janghorbani, M.; Shahshahan, Z. Comparison of risk factors and pregnancy outcomes of gestational diabetes mellitus diagnosed during early and late pregnancy. Midwifery 2018, 66, 64–69. [Google Scholar] [CrossRef]
- Larrabure-Torrealva, G.T.; Martinez, S.; Luque-Fernandez, M.A.; Sanchez, S.E.; Mascaro, P.A.; Ingar, H.; Castillo, W.; Zumaeta, R.; Grande, M.; Motta, V.; et al. Prevalence and risk factors of gestational diabetes mellitus: Findings from a universal screening feasibility program in Lima, Peru. BMC Pregnancy Childbirth 2018, 18, 303. [Google Scholar] [CrossRef] [Green Version]
- Leng, J.; Shao, P.; Zhang, C.; Tian, H.; Zhang, F.; Zhang, S.; Dong, L.; Li, L.; Yu, Z.; Chan, J.; et al. Prevalence of Gestational Diabetes Mellitus and Its Risk Factors in Chinese Pregnant Women: A Prospective Population-Based Study in Tianjin, China. PLoS ONE 2015, 10, e0121029. [Google Scholar] [CrossRef]
- Pirjani, R.; Shirzad, N.; Qorbani, M.; Phelpheli, M.; Nasli-Esfahani, E.; Bandarian, F.; Hemmatabadi, M. Gestational diabetes mellitus its association with obesity: A prospective cohort study. Eat. Weight Disord.-Stud. Anorexia, Bulim. Obes. 2016, 22, 445–450. [Google Scholar] [CrossRef]
- Schaefer, K.K.; Xiao, W.; Chen, Q.; He, J.; Lu, J.; Chan, F.; Chen, N.; Yuan, M.; Xia, H.; Lam, K.B.H.; et al. Prediction of gestational diabetes mellitus in the Born in Guangzhou Cohort Study, China. Int. J. Gynecol. Obstet. 2018, 143, 164–171. [Google Scholar] [CrossRef]
- Shahbazian, H.; Nouhjah, S.; Shahbazian, N.; Jahanfar, S.; Latifi, S.M.; Aleali, A.; Shahbazian, N.; Saadati, N. Gestational diabetes mellitus in an Iranian pregnant population using IADPSG criteria: Incidence, contributing factors and outcomes. Diabetes Metab. Syndr. Clin. Res. Rev. 2016, 10, 242–246. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Luo, B. Risk factors analysis of gestational diabetes mellitus based on International Association of Diabetes Pregnancy Study Groups criteria. Nan fang yi ke da xue xue bao = J. Southern Med. Univ. 2019, 39, 572–578. [Google Scholar]
- Yan, B.; Yu, Y.X.; Lin, M.Z.; Li, Z.B.; Wang, L.Y.; Huang, P.Y.; Song, H.Q.; Shi, X.L.; Yang, S.Y.; Li, X.Y.; et al. High, but stable, trend in the prevalence of gestational diabetes mellitus: A population-based study in Xiamen, China. J. Diabetes Investig. 2019, 10, 1358–1364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalil, A.; Syngelaki, A.; Maiz, N.; Zinevich, Y.; Nicolaides, K.H. Maternal Age and Adverse Pregnancy Outcomes: A Cohort Study EDITORIAL COMMENT. Obstet. Gynecol. Surv. 2013, 68, 779–781. [Google Scholar] [CrossRef]
- Londero, A.P.; Rossetti, E.; Pittini, C.; Cagnacci, A.; Driul, L. Maternal age and the risk of adverse pregnancy outcomes: A retrospective cohort study. BMC Pregnancy Childbirth 2019, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wang, X.Y.; Yang, H.X. [Effect of maternal age on pregnancy outcomes in Beijing]. Zhonghua fu chan ke za zhi 2017, 52, 514–520. [Google Scholar] [PubMed]
- Koo, Y.-J.; Ryu, H.-M.; Yang, J.-H.; Lim, J.-H.; Lee, J.-E.; Kim, M.-Y.; Chung, J.-H. Pregnancy outcomes according to increasing maternal age. Taiwan. J. Obstet. Gynecol. 2012, 51, 60–65. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Shen, Z.; Zhan, Y.; Wang, Y.; Ma, S.; Zhang, S.; Liu, J.; Wu, S.; Feng, Y.; Chen, Y.; et al. Effects of pre-pregnancy body mass index and gestational weight gain on maternal and infant complications. BMC Pregnancy Childbirth 2020, 20, 1–13. [Google Scholar] [CrossRef]
- Rodríguez-Mesa, N.; Robles-Benayas, P.; Rodríguez-López, Y.; Pérez-Fernández, E.M.; Cobo-Cuenca, A.I. Influence of Body Mass Index on Gestation and Delivery in Nulliparous Women: A Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaukat, S.; Nur, U. Effect of prepregnancy maternal BMI on adverse pregnancy and neonatal outcomes: Results from a retrospective cohort study of a multiethnic population in Qatar. BMJ Open 2019, 9, e029757. [Google Scholar] [CrossRef] [Green Version]
- Gao, X.; Yan, Y.; Xiang, S.; Zeng, G.; Liu, S.; Sha, T.; He, Q.; Li, H.; Tan, S.; Chen, C.; et al. The mutual effect of pre-pregnancy body mass index, waist circumference and gestational weight gain on obesity-related adverse pregnancy outcomes: A birth cohort study. PLoS ONE 2017, 12, e0177418. [Google Scholar] [CrossRef] [PubMed]
- Laine, M.K.; Kautiainen, H.; Gissler, M.; Raina, M.; Aahos, I.; Järvinen, K.; Pennanen, P.; Eriksson, J.G. Gestational diabetes in primiparous women-impact of age and adiposity: A register-based cohort study. Acta Obstet. et Gynecol. Scand. 2017, 97, 187–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yong, H.Y.; Shariff, Z.M.; Yusof, B.N.M.; Rejali, Z.; Tee, Y.Y.S.; Bindels, J.; Van Der Beek, E.M. Independent and combined effects of age, body mass index and gestational weight gain on the risk of gestational diabetes mellitus. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Hashemi-Nazari, S.-S.; Najafi, F.; Rahimi, M.-A.; Izadi, N.; Heydarpour, F.; Forooghirad, H. Estimation of gestational diabetes mellitus and dose–response association of BMI with the occurrence of diabetes mellitus in pregnant women of the west of Iran. Health Care Women Int. 2018, 41, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Shao, B.; Mo, M.; Xin, X.; Jiang, W.; Wu, J.; Huang, M.; Wang, S.; Muyiduli, X.; Si, S.; Shen, Y.; et al. The interaction between prepregnancy BMI and gestational vitamin D deficiency on the risk of gestational diabetes mellitus subtypes with elevated fasting blood glucose. Clin. Nutr. 2020, 39, 2265–2273. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Risk Factors for GDM | Category | Scores |
|---|---|---|
| Maternal age (years) * | <30 | 0 |
| 30–34 | 5 | |
| 35–39 | 8 | |
| ≥40 | 9 | |
| T2DM family history | no | 0 |
| yes | 6 | |
| pre–BMI (kg/m2) ** | <24 | 0 |
| 24–27.9 | 4 | |
| ≥28 | 5 | |
| Age at menarche (year) | >11 | 0 |
| ≤11 | 3 | |
| ART | no | 0 |
| yes | 2 | |
| The positive of related thyroid antibodies *** | no | 0 |
| yes | 5 | |
| Above IOM recommended GWG at the 1st trimester | no | 0 |
| yes | 2 |
| Variables | Training Cohort (n = 765) | Validation Cohort 1 (n = 310) | Validation Cohort 2 (n = 210) |
|---|---|---|---|
| GDM | 246 (32.2) | 106 (34.2) | 39(18.5) |
| Maternal age | 31.77 ± 4.14 | 31.5 ± 4.03 | 31.24 ± 4.17 |
| T2DM family history | 70 (9.2) | 33 (10.6) | 15(7.1) |
| pre-BMI | 21.97 ± 3.34 | 22.07 ± 2.97 | 21.4 ± 3.12 |
| Age at menarche ≤ 11 yr | 66 (8.6) | 22 (7.1) | 4(1.9) |
| ART | 53 (6.9) | 31 (10) | 4(1.9) |
| Thyroid antibodies + (TPOAb/TgAb) | 115 (15.0) | 53 (17.1) | 16(7.6) |
| Above IOM recommended GWG at the 1st trimester | 134 (17.5) | 57 (18.4) | 34(16.1) |
| History of macrosomia | 28 (3.7) | 11 (3.5) | 7(3.3) |
| Parity | 1.50 ± 0.60 | 1.49 ± 0.65 | 1.22 ± 0.71 |
| Vitamin B12 (pg/mL) | 64.33 ± 7.34 | 65.36 ± 7.72 | 61.35 ± 6.51 |
| Ferritin (ng/mL) | 46.80 ± 5.57 | 47.03 ± 5.79 | 42.24 ± 4.63 |
| Total protein (g/L) | 69.05 ± 4.13 | 70.18 ± 3.88 | 65.43 ± 3.47 |
| Albumin (g/L) | 40.15 ± 2.31 | 40.0 ± 2.56 | 44.34 ± 3.27 |
| Globulin (g/L) | 29.90 ± 3.31 | 30.18 ± 3.25 | 31.58 ± 2.64 |
| ALT (U/L) | 17.11 ± 10.78 | 18.81 ± 11.83 | 17.31 ± 10.81 |
| AST (U/L) | 19.40 ± 9.38 | 18.66 ± 6.62 | 19.72 ± 7.24 |
| CHO (mmol/L) | 4.13 ± 0.73 | 4.16 ± 0.89 | 4.61 ± 0.63 |
| TG (mmol/L) | 1.51 ± 0.66 | 1.50 ± 0.75 | 1.60 ± 0.69 |
| HDL-C (mmol/L) | 1.67 ± 0.29 | 1.62 ± 0.27 | 1.80 ± 0.31 |
| LDL-C (mmol/L) | 2.31 ± 0.60 | 2.35 ± 0.58 | 2.43 ± 0.52 |
| FBG (mmol/L) | 5.04 ± 0.44 | 5.01 ± 0.41 | 4.88 ± 0.49 |
| B | S.E. | Wald | P | OR (95%CI) | |
|---|---|---|---|---|---|
| Age stratification | 0.492 | 0.131 | 14.202 | <0.001 | 1.636 (1.266–2.113) |
| T2DM family history | 0.976 | 0.307 | 10.120 | 0.001 | 2.653 (1.454–4.838) |
| pre-BMI stratification | 0.691 | 0.167 | 17.153 | <0.001 | 1.996 (1.439–2.769) |
| ART | 0.776 | 0.381 | 4.154 | 0.042 | 2.173 (1.030–4.585) |
| Thyroid antibodies + (TPOAb/TgAb) | 1.381 | 0.269 | 26.423 | <0.001 | 3.979 (2.350–6.737) |
| Above IOM recommended GWG at the 1st trimester | 1.273 | 0.239 | 28.470 | <0.001 | 3.573 (2.238–5.703) |
| FBG stratification | 0.753 | 0.204 | 13.625 | <0.001 | 2.124 (1.424–3.169) |
| Constant | −3.417 | 0.356 | 92.142 | <0.001 | 0.033 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, N.; Guo, H.; Jing, Y.; Song, L.; Chen, H.; Wang, M.; Gao, L.; Huang, L.; Song, Y.; Sun, B.; et al. Development and Validation of Risk Prediction Models for Gestational Diabetes Mellitus Using Four Different Methods. Metabolites 2022, 12, 1040. https://doi.org/10.3390/metabo12111040
Wang N, Guo H, Jing Y, Song L, Chen H, Wang M, Gao L, Huang L, Song Y, Sun B, et al. Development and Validation of Risk Prediction Models for Gestational Diabetes Mellitus Using Four Different Methods. Metabolites. 2022; 12(11):1040. https://doi.org/10.3390/metabo12111040
Chicago/Turabian StyleWang, Ning, Haonan Guo, Yingyu Jing, Lin Song, Huan Chen, Mengjun Wang, Lei Gao, Lili Huang, Yanan Song, Bo Sun, and et al. 2022. "Development and Validation of Risk Prediction Models for Gestational Diabetes Mellitus Using Four Different Methods" Metabolites 12, no. 11: 1040. https://doi.org/10.3390/metabo12111040