
Successful Islet Outcomes Using Australia-Wide Donors: A National Centre Experience


Abstract
:1. Introduction
2. Results
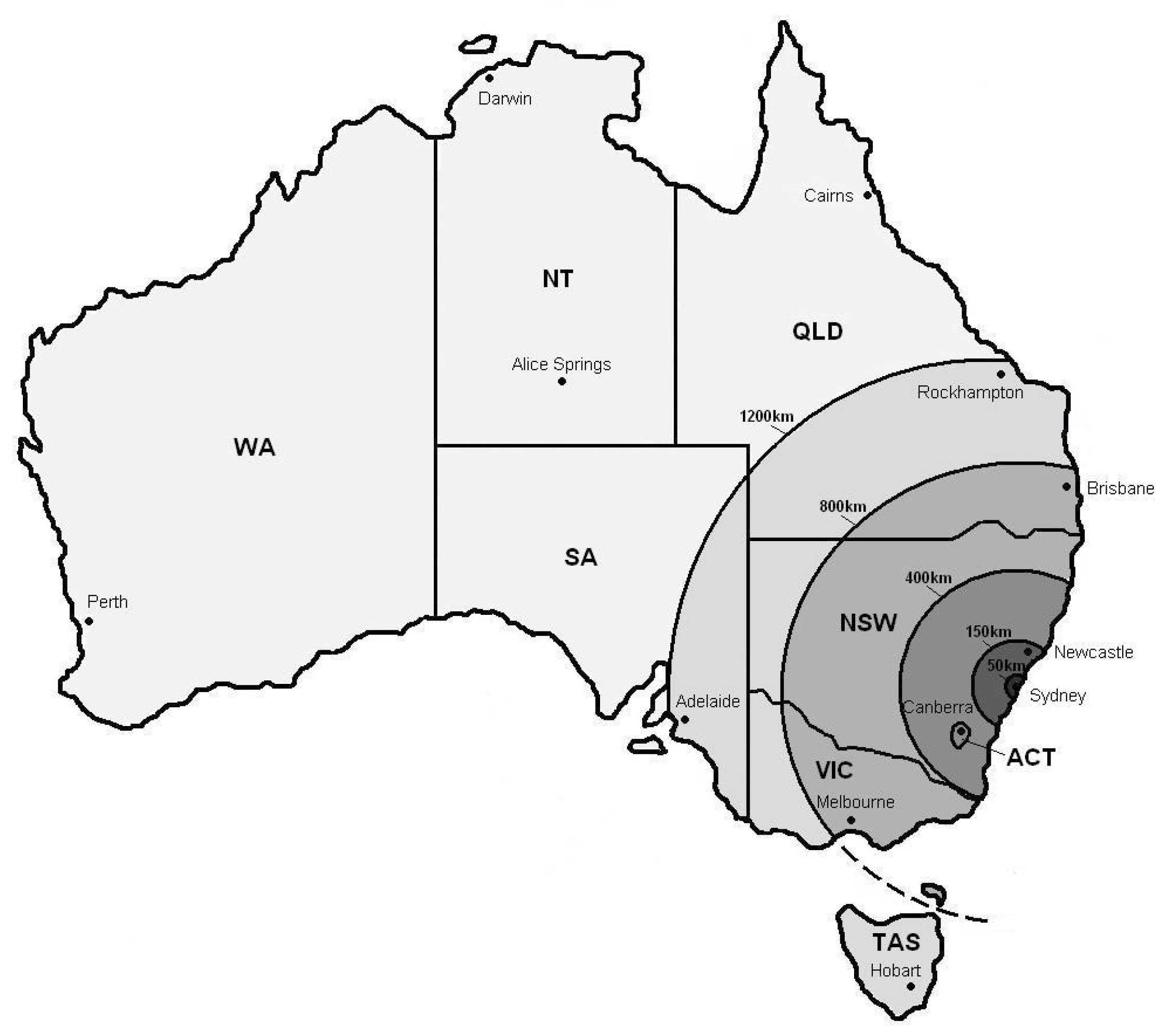
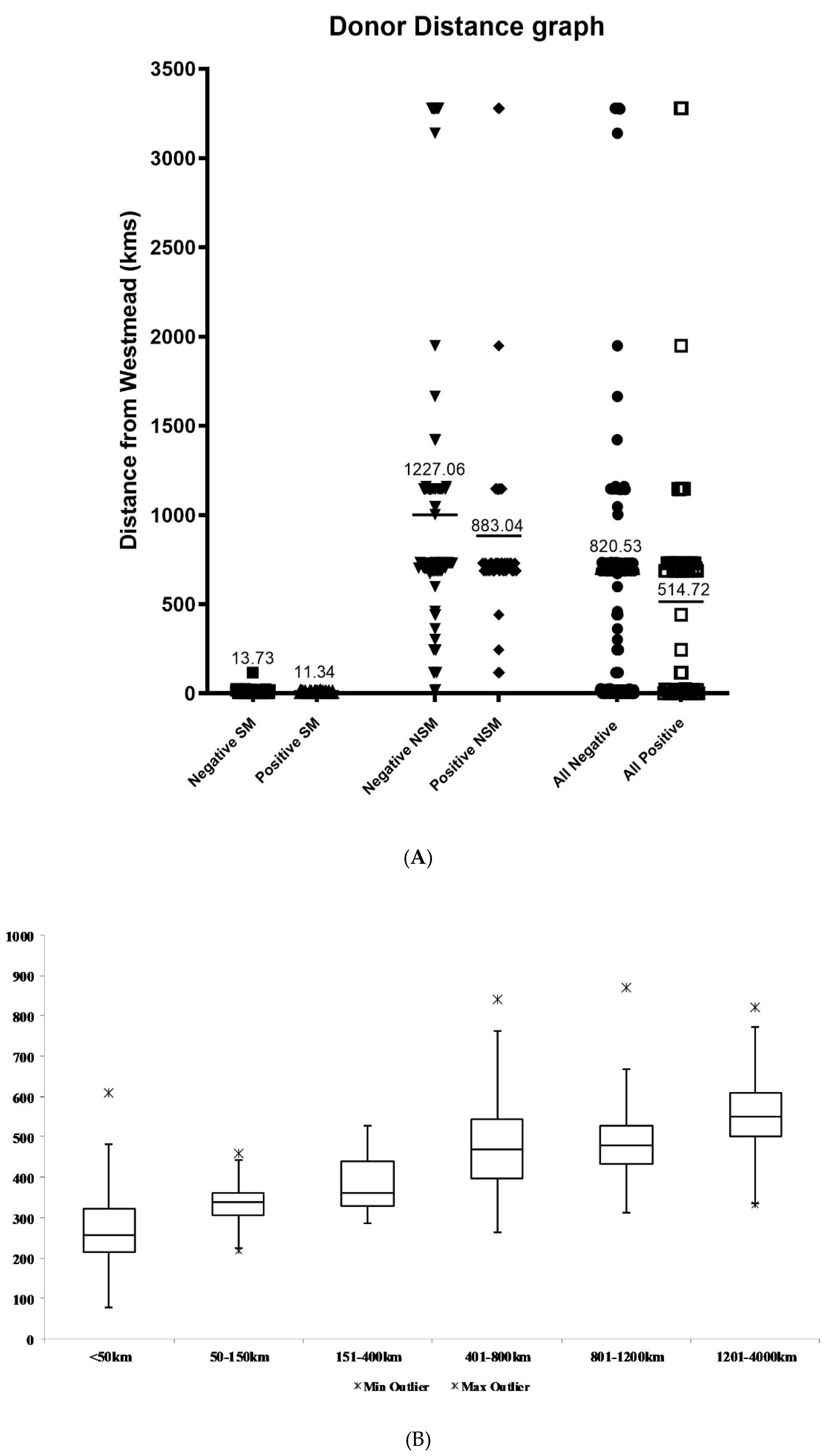
2.1. The Effect of Distance on Isolation Outcome
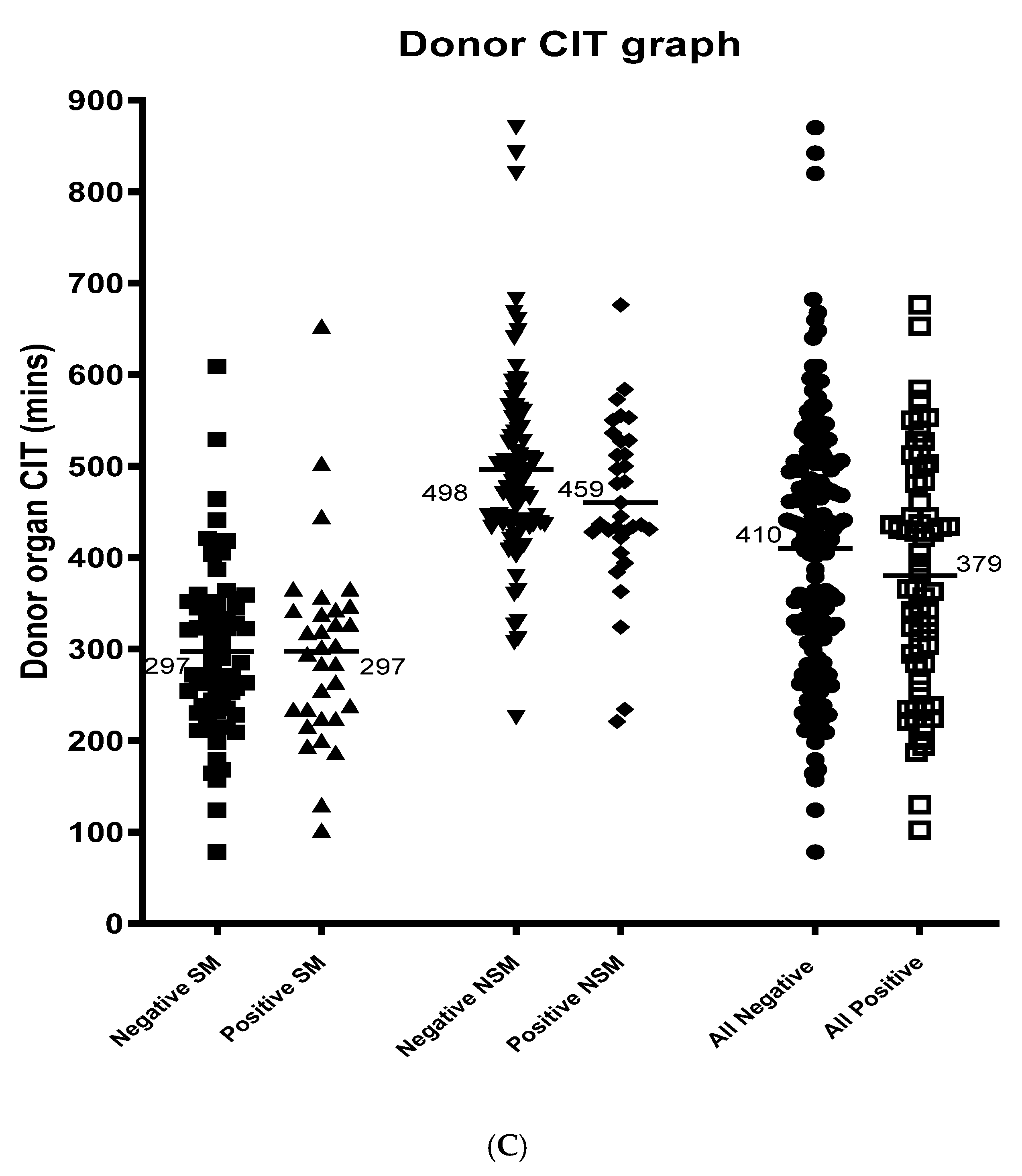
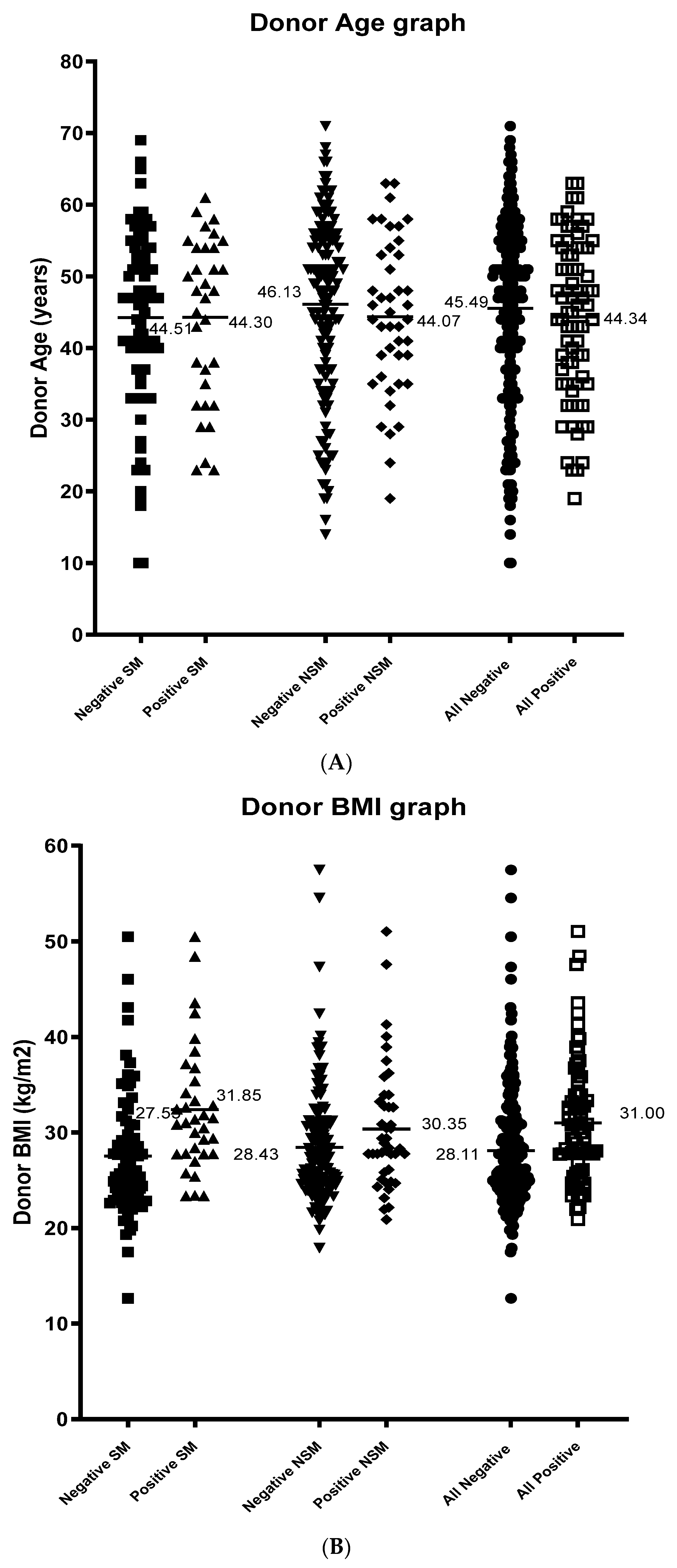
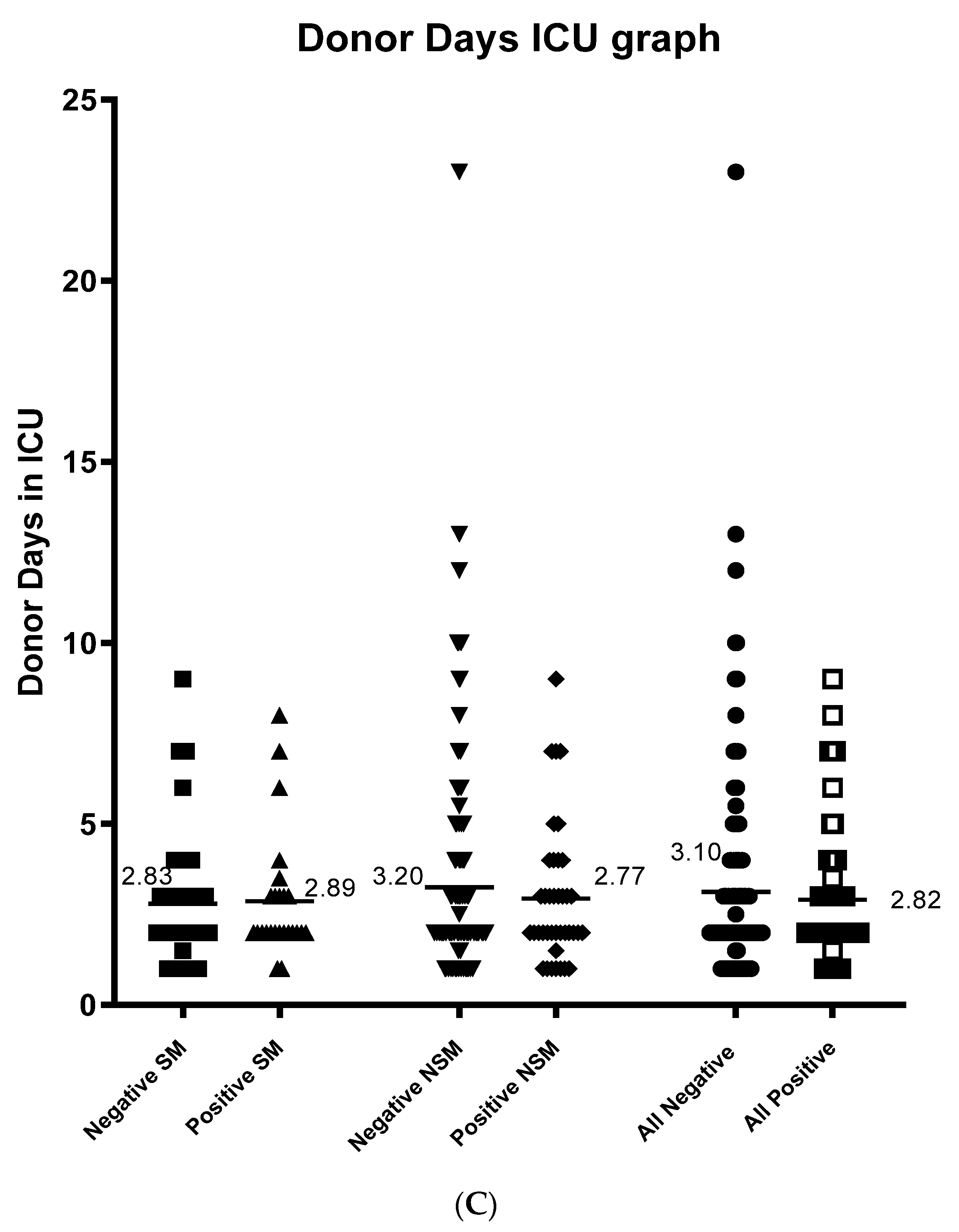
2.2. Other Donor Factors Affecting Isolation Outcome
3. Discussion
4. Materials and Methods
4.1. Donor Selection
4.2. Islet Preparation
4.3. Release Criteria
4.4. Recipient Patients
4.5. Islet Transplantation
4.6. Data Collection and Grouping
4.7. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body mass index |
| CIT | Cold ischemia time |
| ICU | Intensive care unit |
| IEQ | Islet equivalents |
| SD | Standard deviation |
References
- Markmann, J.F.; Deng, S.; Huang, X.; Desai, N.M.; Velidedeoglu, E.H.; Lui, C.; Frank, A.; Markmann, E.; Palanjian, M.; Brayman, K.; et al. Insulin Independence Following Isolated Islet Transplantation and Single Islet Infusions. Ann. Surg. 2003, 237, 741–750. [Google Scholar] [CrossRef]
- Robertson, R.P. Islet Transplantation as a Treatment for Diabetes—A Work in Progress. N. Engl. J. Med. 2004, 350, 694–705. [Google Scholar] [CrossRef] [Green Version]
- Ryan, E.A.; Lakey, J.R.; Paty, B.W.; Imes, S.; Korbutt, G.S.; Kneteman, N.M.; Bigam, D.; Rajotte, R.V.; Shapiro, A.J. Successful islet transplantation: Continued insulin reserve provides long-term glycemic control. Diabetes 2002, 51, 2148–2157. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, A.M.J.; Ricordi, C.; Hering, B.J.; Auchincloss, H.; Lindblad, R.; Robertson, R.P.; Secchi, A.; Brendel, M.D.; Berney, T.; Brennan, D.C.; et al. International Trial of the Edmonton Protocol for Islet Transplantation. N. Engl. J. Med. 2006, 355, 1318–1330. [Google Scholar] [CrossRef] [Green Version]
- O’Connell, P.J.; Hawthorne, W.J.; Nankivell, B.J.; Patel, A.T.; Walters, S.N.; Pleass, H.C.; Allen, R.D.; Chapman, J.R.; Holmes-Walker, D.J.; Gunton, J.E. Clinical islet transplantation in type 1 diabetes mellitus: Results of Australia’s first trial. Med. J. Aust. 2006, 184, 221–225. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, P.J.; Holmes-Walker, D.J.; Goodman, D.; Hawthorne, W.J.; Loudovaris, T.; Gunton, J.E.; Thomas, H.E.; Grey, S.T.; Drogemuller, C.J.; Ward, G.M.; et al. Multicenter Australian Trial of Islet Transplantation: Improving Accessibility and Outcomes. Arab. Archaeol. Epigr. 2013, 13, 1850–1858. [Google Scholar] [CrossRef]
- Alejandro, R.; Barton, F.B.; Hering, B.J.; Wease, S. 2008 Update From the Collaborative Islet Transplant Registry. Transplantation 2008, 86, 1783–1788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goss, J.A.; Schock, A.P.; Brunicardi, F.C.; Goodpastor, S.E.; Garber, A.J.; Soltes, G.; Barth, M.; Froud, T.; Alejandro, R.; Ricordi, C. Achievement of insulin independence in three consecutive type-1 diabetic patients via pancreatic islet transplantation using islets isolated at a remote islet isolation center. Transplantation 2002, 74, 1761–1766. [Google Scholar] [CrossRef] [PubMed]
- Goss, J.A.; Goodpastor, S.E.; Brunicardi, F.C.; Barth, M.H.; Soltes, G.D.; Garber, A.J.; Hamilton, D.J.; Alejandro, R.; Ricordi, C. Development of a human pancreatic islet-transplant program through a collaborative relationship with a remote islet-isolation center. Transplantation 2004, 77, 462–466. [Google Scholar] [CrossRef]
- Kempf, M.-C.; Andres, A.; Morel, P.; Benhamou, P.-Y.; Bayle, F.; Kessler, L.; Badet, L.; Thivolet, C.; Penfornis, A.; Renoult, E.; et al. Logistics and Transplant Coordination Activity in the GRAGIL Swiss-French Multicenter Network of Islet Transplantation. Transplantation 2005, 79, 1200–1205. [Google Scholar] [CrossRef]
- Kin, T.; Murdoch, T.B.; Shapiro, A.M.J.; Lakey, J.R.T. Estimation of Pancreas Weight from Donor Variables. Cell Transplant. 2006, 15, 181–185. [Google Scholar] [CrossRef] [Green Version]
- Briones, R.; Miranda, J.; Mellado-Gil, J.; Castro, M.; Gonzalez-Molina, M.; Cuesta-Munoz, A.; Alonso, A.; Frutos, M. Differential Analysis of Donor Characteristics for Pancreas and Islet Transplantation. Transplant. Proc. 2006, 38, 2579–2581. [Google Scholar] [CrossRef] [PubMed]
- Sakuma, Y.; Ricordi, C.; Miki, A.; Yamamoto, T.; Pileggi, A.; Khan, A.; Alejandro, R.; Inverardi, L.; Ichii, H. Factors That Affect Human Islet Isolation. Transplant. Proc. 2008, 40, 343–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Gorman, D.; Kin, T.; Murdoch, T.; Richer, B.; McGhee-Wilson, D.; Ryan, E.A.; Shapiro, J.A.; Lakey, J.R. The Standardization of Pancreatic Donors for Islet Isolations. Transplantation 2005, 80, 801–806. [Google Scholar] [CrossRef] [PubMed]
- Lakey, J.R.; Warnock, G.L.; Rajotte, R.V.; Suarez-Almazor, M.E.; Ao, Z.; Shapiro, A.J.; Kneteman, N.M. Variables in organ donors that affect the recovery of human islets of Langerhans. Transplantation 1996, 61, 1047–1053. [Google Scholar] [CrossRef]
- Ponte, G.M.; Pileggi, A.; Messinger, S.; Alejandro, A.; Ichii, H.; Baidal, D.A.; Khan, A.; Ricordi, C.; Goss, J.A.; Alejandro, R. Toward Maximizing the Success Rates of Human Islet Isolation: Influence of Donor and Isolation Factors. Cell Transplant. 2007, 16, 595–607. [Google Scholar] [CrossRef]
- Thwaites, S.E.; Gurung, B.; Yao, J.; Kable, K.; Robertson, P.; Ryan, B.J.; Lam, V.W.; Pleass, H.C.; Chapman, J.R.; Hawthorne, W.J.; et al. Excellent outcomes of simultaneous pancreas kidney transplantation in patients from rural and urban Australia: A national service experience. Transplantation 2012, 94, 1230–1235. [Google Scholar] [CrossRef]
- Ricordi, C.; Lacy, P.E.; Scharp, D.W. Automated Islet Isolation from Human Pancreas. Diabetes 1989, 38, 140–142. [Google Scholar] [CrossRef]
- Ricordi, C.; Gray, D.W.R.; Hering, B.J.; Kaufman, D.B.; Warnock, G.L.; Kneteman, N.M.; Lake, S.P.; London, N.J.M.; Socci, C.; Alejandro, R.; et al. Islet isolation assessment in man and large animals. Acta Diabetol. 1990, 27, 185–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, T.; Horiguchi, A.; Ito, M.; Nagata, H.; Ichii, H.; Ricordi, C.; Miyakawa, S. Quality control for clinical islet transplantation: Organ procurement and preservation, the islet processing facility, isolation, and potency tests. J. Hepato-Biliary-Pancreat. Surg. 2009, 16, 131–136. [Google Scholar] [CrossRef]
- Ryan, E.A.; Shandro, T.; Green, K.; Paty, B.W.; Senior, P.A.; Bigam, D.; Shapiro, A.J.; Vantyghem, M.-C. Assessment of the Severity of Hypoglycemia and Glycemic Lability in Type 1 Diabetic Subjects Undergoing Islet Transplantation. Diabetes 2004, 53, 955–962. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | Min | Max | Mean | SD | |
|---|---|---|---|---|---|
| DONOR-RELATED FACTORS | |||||
| Outcome | 263 | 0.00 | 1.00 | 0.27 | 0.44 |
| Donor Distance (kms) | 263 | 0.00 | 3278.70 | 780.06 | 2195.2 |
| Donor Distance Zone | 263 | 1.00 | 6.00 | 3.09 | 1.73 |
| EDMONTON SCORE DONOR-RELATED FACTORS | |||||
| CIT (mins) | 215 | 124.00 | 870.00 | 404.35 | 140.21 |
| Donor Age | 296 | 10.00 | 71.00 | 45.22 | 13.03 |
| Donor BMI | 298 | 19.80 | 57.46 | 28.82 | 6.01 |
| Donor Gender | 308 | 1.00 | 2.00 | 1.49 | 0.49 |
| Donor Days in ICU | 252 | 1.00 | 13.00 | 3.07 | 2.51 |
| Retrieval Team | 268 | 1.00 | 2.00 | 1.56 | 0.50 |
| Cause of Death | 246 | 1.00 | 6.00 | 2.64 | 0.84 |
| Mechanism of Death | 246 | 1.00 | 12.00 | 7.78 | 1.98 |
| Inotrope Usage | 244 | 0.00 | 3.00 | 1.38 | 1.00 |
| Steroid Usage | 244 | 0.00 | 1.00 | 0.02 | 0.13 |
| RECIPIENT-RELATED FACTORS | |||||
| C-Peptide at 1 Month Post-Transplant | 23 | 0.00 | 0.91 | 0.28 | 0.23 |
| C-Peptide level | 73 | 0.00 | 1.00 | 0.55 | 0.36 |
| Cause of Donor Death | Outcome (N) | % Positive | p Value | |
| Negative | Positive | |||
| Anoxia/Cardiac Arrest | 22 | 4 | 15.38 | 0.113 |
| Head Trauma | 40 | 17 | 29.82 | 0.829 |
| Cerebrovascular/Stroke | 108 | 44 | 28.95 | 0.909 |
| Other | 4 | 5 | 55.56 | 0.124 |
| Total | 174 | 70 | 28.69 | - |
| Mechanism of Donor Death | Outcome (N) | % Positive | p Value | |
| Negative | Positive | |||
| Asphyxiation | 8 | 2 | 20.00 | 0.728 |
| Blunt Injury | 2 | 1 | 33.33 | 1.000 |
| Cardiovascular | 4 | 1 | 20.00 | 1.000 |
| Sharp Injury | 4 | 0 | 0.00 | 0.325 |
| Intracranial Haemorrhage/Stroke | 148 | 58 | 28.16 | 0.396 |
| Seizure | 1 | 0 | 0.00 | 1.000 |
| Other | 7 | 8 | 53.33 | 0.042 |
| Total | 170 | 70 | 28.69 | - |
| C-Peptide Level | ||
|---|---|---|
| Correlation Coefficient | Significance (2-Tailed) | |
| Donor Distance (kms) | 0.311 | 0.832 |
| CIT (mins) | −0.308 | 0.065 |
| Donor Age | 0.354 | 0.977 |
| Donor BMI | −0.171 | 0.770 |
| Donor Days in ICU | 0.135 | 0.659 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hawthorne, W.J.; Davies, S.; Mun, H.-c.; Chew, Y.V.; Williams, L.; Anderson, P.; Rogers, N.; O’Connell, P.J. Successful Islet Outcomes Using Australia-Wide Donors: A National Centre Experience. Metabolites 2021, 11, 360. https://doi.org/10.3390/metabo11060360
Hawthorne WJ, Davies S, Mun H-c, Chew YV, Williams L, Anderson P, Rogers N, O’Connell PJ. Successful Islet Outcomes Using Australia-Wide Donors: A National Centre Experience. Metabolites. 2021; 11(6):360. https://doi.org/10.3390/metabo11060360
Chicago/Turabian StyleHawthorne, Wayne J, Sussan Davies, Hee-chang Mun, Yi Vee Chew, Lindy Williams, Patricia Anderson, Natasha Rogers, and Philip J O’Connell. 2021. "Successful Islet Outcomes Using Australia-Wide Donors: A National Centre Experience" Metabolites 11, no. 6: 360. https://doi.org/10.3390/metabo11060360