
Plasminogen Activator Inhibitor-1 (PAI-1) Gene Polymorphisms Associated with Cardiovascular Risk Factors Involved in Cerebral Venous Sinus Thrombosis



 ,
,
Abstract
:1. Introduction
2. Results
2.1. Patient Population
2.1.1. Demographic Characteristics
2.1.2. Clinical Features
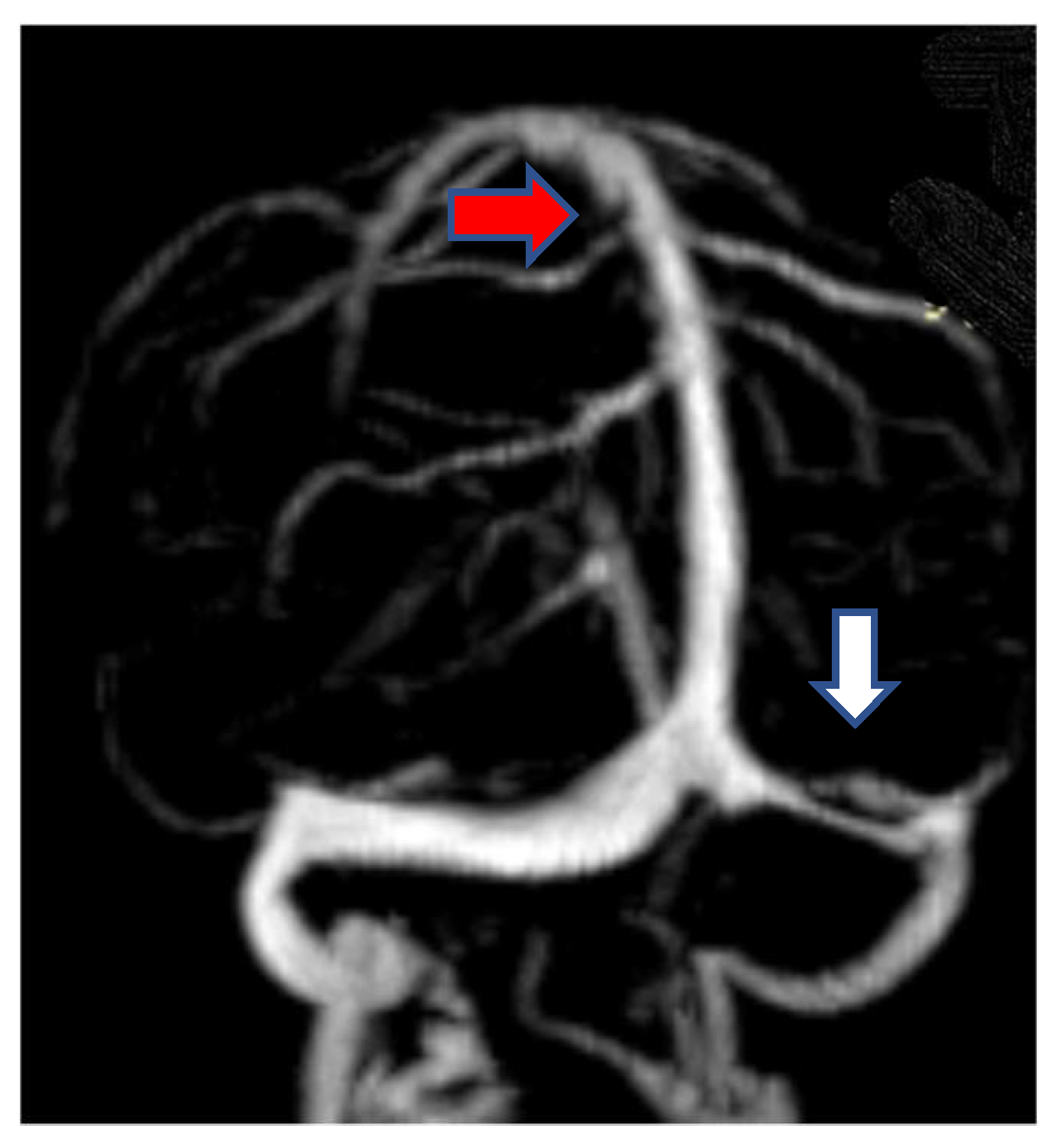
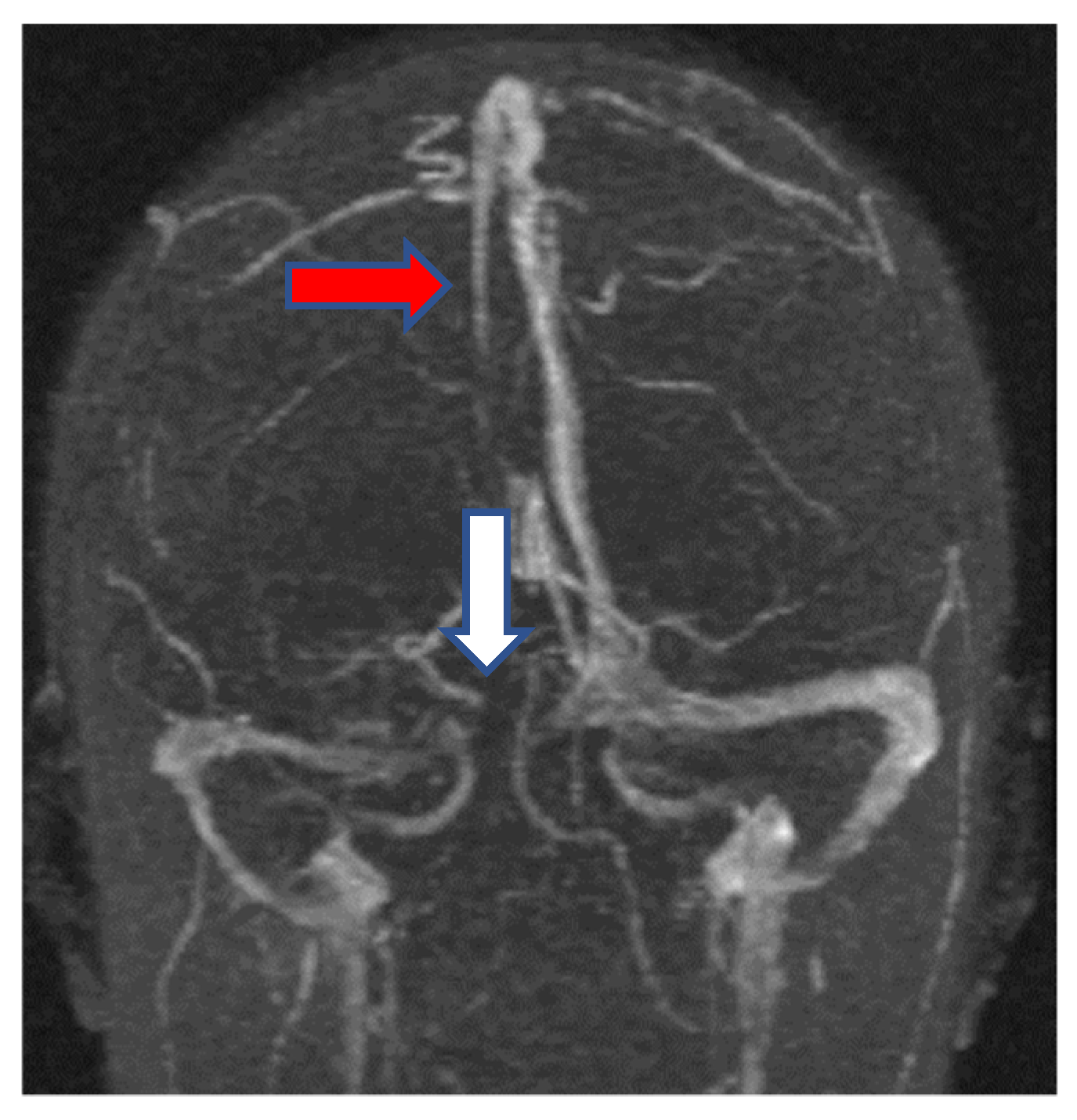
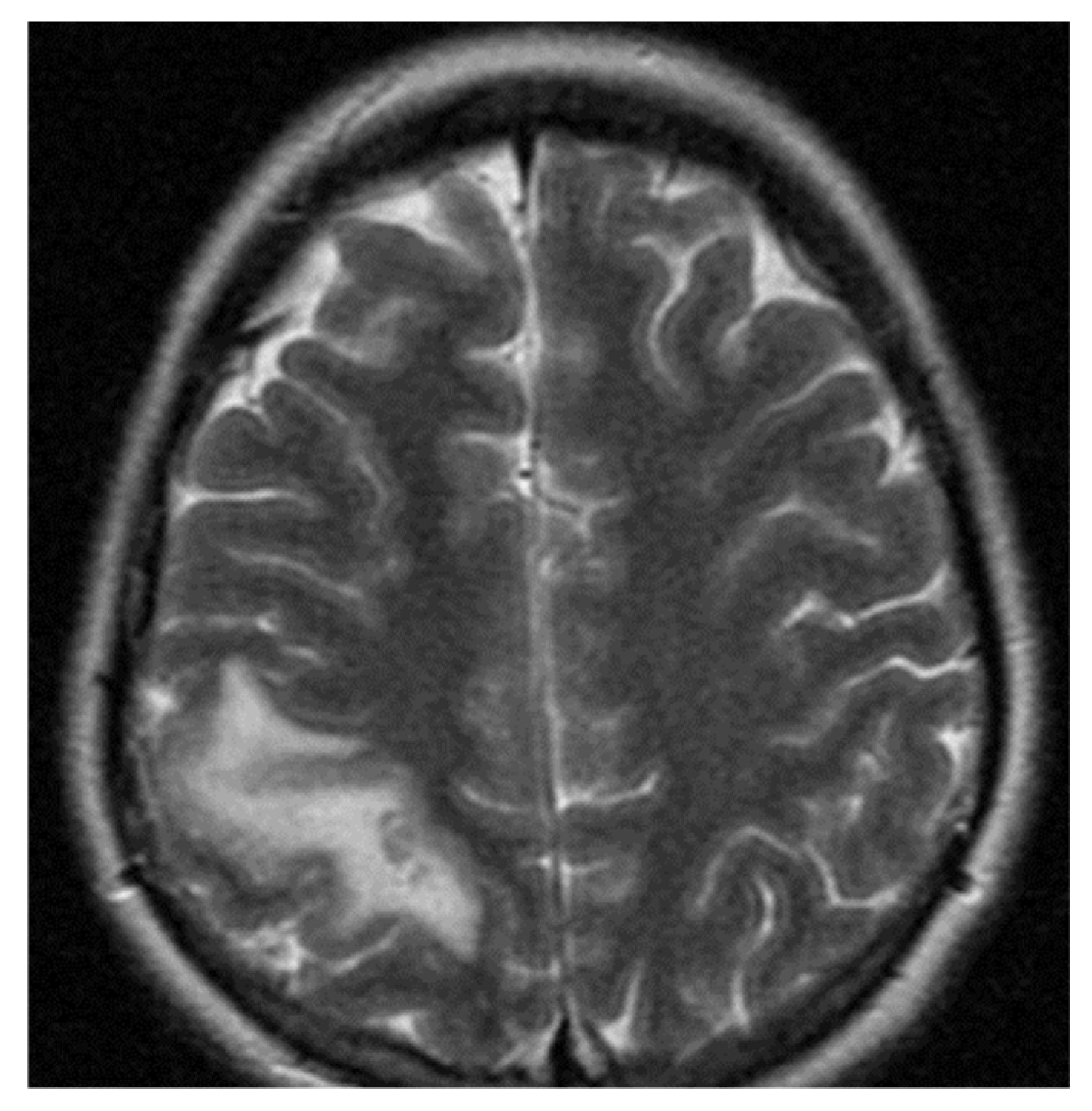
2.1.3. Neuroimaging
2.1.4. Biochemical and Genetic Findings
- in the 5G/5G genotype comparison was a statistically significant difference between the TGL levels (p < 0.001) between the CVST group and control group. The differences between the TC levels were not statistically significant (195.5 mg/dL vs. 194.2 mg/dL; p = 0.712) between the CVST group and control group. The differences between the LDLc levels were not statistically significant (116 mg/dL vs. 110.4 mg/dL; p = 0.124) between the CVST group and control group. The differences between the hsCRP levels were not statistically significant (6.61 mg/L vs. 4.34 mg/L; p = 0.398) between the CVST group and control group. The IMT values were not statistically significant between the CVST group and control group (0.85 mm vs. 1 mm; p = 0.966).
- in the 4G/4G genotype comparison was not found a statistically significant difference between the TC, LDLc, TGL, hsCRP levels and IMT between the CVST group and control group. The differences between the TC levels were not statistically significant (199.03 mg/dL vs. 203.68 mg/dL; p = 0.201) between the CVST group and control group. The differences between the LDLc levels were not statistically significant (116.03 mg/dL vs. 114.23 mg/dL; p = 0.571) between the CVST group and control group. The differences between the TGL levels were not statistically significant (149.78 mg/dL vs. 153.32 mg/dL; p = 0.264) between the CVST group and control group. The differences between the hsCRP levels were not statistically significant (7.42 mg/L vs. 4.84 mg/L; p = 0.571) between the CVST group and control group. The IMT values were not statistically significant between the CVST group and control group (0.98 mm vs. 0.91 mm; p = 0.984).
- in the 4G/5G genotype comparison was a statistically significant difference between the TC, LDLc and TGL levels (p < 0.001) between the CVST group and control group. The differences between the hsCRP levels were not statistically significant (8.02 mg/L vs. 4.17 mg/L; p = 0.264) between the CVST group and control group. The IMT values were not statistically significant between the CVST group and control group (0.9 mm vs. 0.86 mm; p = 0.991).
3. Discussion
4. Materials and Methods
4.1. Patient Population
4.2. Clinical, Biochemical and Genetic Evaluation
4.3. Neuroimaging
4.4. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Biller, J. Stroke in Children and Young Adults. Stroke Child. Young Adults 2009, 12, 233–244. [Google Scholar]
- Matić, T.B.; Gavrilović, A.; Simović, S.; Aleksić, D.; Vesić, K.; Azanjac, A.; Tončev, S.; Drakulić, S.M. Specific Polymorphism 4G/5G Gene for PAI-1 as a Possible Cause of Cerebral Venous Thrombosis: A Case Report. Serb. J. Exp. Clin. Res. 2017, 18, 169–173. [Google Scholar] [CrossRef] [Green Version]
- Alvis-Miranda, H.R.; Castellar-Leones, S.M.; Alcala-Cerra, G.; Moscote-Salazar, L.R. Cerebral sinus venous thrombosis. J. Neurosci. Rural Pract. 2013, 4, 427–438. [Google Scholar] [CrossRef] [PubMed]
- Ferro, J.M.; Canhao, P.; Stam, J.; Bousser, M.G.; Barinagarrementeria, F. ISCVT Investigators. Prognosis of cerebral vein and dural sinus thrombosis: Results of the international study on cerebral vein and dural sinus thrombosis. Stroke 2004, 35, 664–670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tadi, P.; Behgam, B.; Barrufi, S. Cerebral Venous Thrombosis; StatPearls Publishing: Treasure Island, SF, USA, 2020. [Google Scholar]
- Yildiz, S.Y.; Kuru, P.; Oner, E.T.; Agirbasli, M. Functional Stability of Plasminogen Activator Inhibitor-1. Sci. World J. 2014, 2014, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Saadatnia, M.; Salehi, M.; Movahedian, A.; Shariat, S.Z.S.; Salari, M.; Tajmirriahi, M.; Kheradmand, E. Factor V Leiden, Factor V Cambridge, factor II GA 20210 and MTHFR in cerebral venous and sinus thrombosis: A case-control study. J. Res. Med. Sci. 2015, 20, 554–562. [Google Scholar] [CrossRef]
- Grant, P.J. Diabetes mellitus as a prothrombotic condition. J. Intern. Med. 2007, 262, 157–172. [Google Scholar] [CrossRef]
- Van Goor, M.L.; Gomez, G.E.; Leebeek, F.; Brouwers, G.J.; Koudstaal, P.; Dippel, D. The plasminogen activator inhibitor (PAI-1) 4G/5G promoter polymorphism and PAI-1 levels in IS. A case-control study. Thromb. Haemost. 2005, 93, 92–96. [Google Scholar]
- Jiang, S.; Zhao, R.; Pan, M.; Venners, S.A.; Zhong, G.; Hsu, Y.-H. Associations of MTHFR and MTRR Polymorphisms With Serum Lipid Levels in Chinese Hypertensive Patients. Clin. Appl. Thromb. 2012, 20, 400–410. [Google Scholar] [CrossRef] [Green Version]
- Tekesin, A.; Tunç, A. Inflammatory markers are beneficial in the early stages of cerebral venous thrombosis. Arq. Neuropsiquiatr. 2019, 77, 101–105. [Google Scholar] [CrossRef]
- Zairis, M.N.; Ambrose, J.A.; Manousakis, S.J.; Stefanidis, A.S.; Papadaki, O.A.; Bilianou, H.I. The impact of plasma levels of C-reactive protein, lipoprotein(a) and ho-mocysteine on the long-term prognosis after successful coronary stenting. J. Am. Coll Cardiol. 2002, 40, 1375–1382. [Google Scholar] [CrossRef] [Green Version]
- Marcucci, R.; Brogi, D.; Sofi, F.; Giglioli, C.; Valente, S.; Liotta, A.; Lenti, M.; Gori, A.M.; Gensini, G.F. PAI-1and homocysteine, but not lipoprotein(a) and thrombophilic polymorphisms, are independently associated with the occurrence of major adverse cardiac events after successful coronary stenting. Heart 2006, 92, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Homocysteine Studies Collaboration. Homocysteine and risk of ischemic heart disease and stroke: A meta-analysis. JAMA 2002, 288, 2015–2022. [CrossRef] [PubMed]
- Huber, K. Plasminogen activator inhibitor type-1 (part one): Basic mechanisms, regulation, and role for thromboembolic disease. J. Thromb. Thrombolysis 2001, 11, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Hoekstra, T.; Schouten, E.G.; Kluft, C.; Geleijnse, J.M. Plasminogen activator inhibitor-type 1: Its plasma determinants and relation with cardiovascular risk. Thromb. Haemost. 2004, 91, 861–872. [Google Scholar] [CrossRef] [PubMed]
- Dudman, N.P. An alternative view of homocysteine. Lancet 1999, 354, 2072–2074. [Google Scholar] [CrossRef]
- Korte, W.; Greiner, J.; Feldges, A.; Riesen, W.F. Increased Lp(a) levels are not a steady prothrombotic defect. Blood J. Am. Soc. Hematol. 2001, 98, 1993–1994. [Google Scholar]
- Gogu, A.; Lupu, M.; Axelerad, A.D. The Relationship between Ischemic Stroke and Atrial Fibrillation. Procedia Soc. Behav. Sci. 2015, 197, 2004–2010. [Google Scholar] [CrossRef] [Green Version]
- Gogu, A.E.; Jianu, D.C. Cerebral venous thrombosis and intracerebral hemorrhage. Cerebrovasc. Dis. 2014, 37, 707–708. [Google Scholar]
- Gogu, A.E.; Scutelnicu, D.; Ignea, A. Relationship between low total serum cholesterol levels and intracerebral hemorrhage. J. Neurol. 2013, 260, 80. [Google Scholar]
- Jianu, D.C.; Jianu, S.N.; Dan, T.F.; Motoc, A.G.M.; Poenaru, M. Pulsatile tinnitus caused by a dilated left petrosquamosal sinus. Rom. J. Morphol. Embryol. 2016, 57, 319–322. [Google Scholar]
- Petrica, L.; Petrica, M.; Munteanu, M.; Vlad, A.; Bob, F.; Gluhovschi, C.; Jianu, D.C.; Bozdog, G. Cerebral microangiopathy in pa-tients with non-insulin-dependent diabetes mellitus. Ann. Acad. Singap. 2007, 36, 259–266. [Google Scholar]
- Vlad, A.; Vlad, M.; Petrica, L.; Ursoniu, S.; Gadalean, F.; Vlad, D.; Dumitrascu, V.; Jianu, D.C. Therapy with atorvas-tatin versus rosuvastatin reducers urinary podocytes, podocytes-associated molecules, and proximal tubule dysfunction bi-omarkers in patients with Type 2 diabetes mellitus: A pilot study. Ren. Fail. 2017, 39, 112–119. [Google Scholar] [CrossRef] [Green Version]
- Korathanakhum, P.; Sathirapanya, P.; Geater, S.L.; Petpichetchian, W. Predictors of hospital outcome in patients with cere-bral venous thrombosis. J. Stroke Cereb. Dis. 2014, 23, 2725–2729. [Google Scholar] [CrossRef] [PubMed]
- Gogu, A.E.; Scutelnicu, D. Cerebral venous and sinus thrombosis at young patients. Eur. J. Neurol. 2012, 19, 519. [Google Scholar]
- Biswas, A.; Ranjan, R.; Meena, A.; Akhter, M.S.; Yadav, B.K.; Munisamy, M.; Saxena, R. Homocysteine levels, Polymorphisms and the Risk of Is-chemic Stroke in Young Asian Indians. J. Stroke Cereb. Dis. 2009, 18, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Varga, E.A.; Sturm, A.C.; Misita, C.P.; Moll, S. Homocysteine and MTHFR Mutations. Circulation 2005, 111, e289–e293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moll, S.; Varga, E.A. Homocysteine and MTHFR Mutations. Circulation 2015, 132, e6–e9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, P.J.; Rosand, J.; Kistler, J.P.; Shih, V.E.; Silveira, S.; Plomaritoglou, A.; Furie, K.L. Homocysteine, MTHFR 677C->T polymorphism, and risk of ischemic stroke: Results of a meta-analysis. Neurology 2002, 59, 529–536. [Google Scholar] [CrossRef]
- Akhter, M.S.; Biswas, A.; Abdullah, S.M.; Behari, M.; Saxena, R. The Role of PAI-1 4G/5G Promoter Polymorphism and Its Levels in the Development of Ischemic Stroke in Young Indian Population. Clin. Appl. Thromb. 2017, 23, 1071–1076. [Google Scholar] [CrossRef] [PubMed]
- Jones, W.J.; Williams, L.S.; Meschia, J.F. Validating the Questionnaire for Verifying Stroke-Free Status (QVSFS) by neurologi-cal history and examination. Stroke 2001, 32, 2232–2236. [Google Scholar] [CrossRef] [Green Version]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapono, A.L.; Cooney, M.T. European guidelines on cardio-vascular disease prevention in clinical practice. Eur. Heart J. 2006, 37, 2315–2381. [Google Scholar] [CrossRef]
- American Diabetes Association. American Diabetes Association Standards of Medical Care in Diabetes. Diabetes Care 2010, 34, S11–S61. [Google Scholar]
- Little, R.; Rohlfing, C.; Wiedmeyer, H.M.; Myers, G.L.; Sacks, D.B.; Goldstein, D.E. The national glycohemoglobin standardi-zation program: A five-year progress report. Clin. Chem. 2001, 47, 1985–1992. [Google Scholar] [PubMed]
- Gogu, A.E.; Jianu, D.C.; Dumitrascu, V.; Ples, H.; Stroe, A.Z.; Docu Axelerad, D.; Docu Axelerad, A. MTHFR Gene Poly-morphisms and Cardiovascular Risk Factors, Clinical-Imagistic Features and Outcome in Cerebral Venous Sinus Thrombosis. Brain Sci. 2021, 11, 23. [Google Scholar] [CrossRef]
- Morris, M.S. Homocysteine and Alzheimer disease. Lancet Neurol. 2003, 2, 425–428. [Google Scholar] [CrossRef]
- Gogu, A. New Clinical-Imagistic Features in Cerebral Venous and Sinus Thrombosis. Procedia Soc. Behav. Sci. 2015, 191, 1650–1659. [Google Scholar] [CrossRef] [Green Version]
- Jianu, D.C.; Jianu, S.N.; Motoc, A.G.; Poenaru, M.; Petrica, L.; Vlad, A.; Ursoniu, S.; Gogu, A.E.; Dan, F.T. Diagnosis and management of a young women with isolated lateral sinus thrombosis. Rom. J. Morphol. Embryol. 2017, 58, 1515–1518. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Variable | CVST Group (n = 80) | Controls (n = 80) | p-Value | ||
|---|---|---|---|---|---|---|
| Mean ± Std Deviation (Median) | Mean Rank | Mean ± Std Deviation (Median) | Mean Rank | |||
| 1 | Age, years | 33.77 ± 6.60 | 34.82 | 33.12 ± 6.12 | 32.04 | 0.374 * |
| 2 | Male n (%) | 36 (45%) | 37.31 | 36 (45%) | 34.67 | 0.360 * |
| 3 | Female n (%) | 54 (55%) | 55.96 | 54 (55%) | 52.01 | 0.263 * |
| 4 | HTN 1 n (%) | 21 (26.25%) | 19.61 | 13 (16.25%) | 14.37 | p < 0.05 |
| 5 | SBP 2, mmHg | 128.56 ± 23.15 | 131.79 | 123 ± 19.03 | 119.75 | 0.075 |
| 6 | DBP 3, mmHg | 81.18 ± 14.78 | 82.57 | 75.37 ± 13.58 | 73.93 | 0.132 |
| 7 | SSS 4/SSS + LS, n (%) | 45 (56.25%) | 34.56 | NA | NA | NA |
| 8 | LS 5, n (%) | 23 (28.75%) | 17.66 | NA | NA | NA |
| 9 | CAV.S 6, n (%) | 12 (15%) | 9.21 | NA | NA | NA |
| 10 | PAI75G/5G, n (%) | 6 (7.5%) | 9.97 | 20 (25%) | 16.02 | p < 0.05 |
| 11 | PAI74G/4G, n (%) | 32 (40%) | 30.49 | 22 (27.5%) | 23.5 | p < 0.05 |
| 12 | PAI74G/5G, n (%) | 42 (52.5%) | 42.45 | 38 (47.5%) | 37.52 | 0.245 * |
| 13 | tHcy 8, μmol/L | 31.39 ± 31.25 | 28.03 | 12.3 ± 7.41 | 16.47 | p < 0.05 |
| 14 | TC 9, mg/dL | 204.8 ± 36.60 | 210.5 | 198.26 ± 34.11 | 192.46 | p < 0.05 |
| 15 | LDLc 10, mg/dL | 117.11 ± 25.89 | 118.96 | 108.11 ± 26.21 | 106.21 | 0.050 |
| 16 | HDLc 11, mg/dL | 56.65 ± 15.19 | 58.16 | 54.6 ± 12.14 | 53.06 | 0.242 |
| 17 | TGL 12, mg/dL | 144.15 ± 70.41 | 145.93 | 131.33 ± 67.73 | 129.37 | p < 0.05 |
| 18 | Blood glucose 13, mg/dL | 102.07 ± 34.93 | 103.6 | 93.91 ± 24.56 | 92.33 | 0.084 |
| 19 | HbA1c 14, % | 5.56 ± 1.35 | 5.67 | 5.24 ± 0.95 | 5.12 | 0.703 * |
| 20 | hsCRP 15, mg/L | 7.67 ± 2.94 | 7.06 | 4.39 ± 1.7 | 4.99 | p < 0.05 |
| 21 | IMT 16, mm | 0.93 ± 0.17 | 0.95 | 0.91 ± 0.16 | 0.88 | p < 0.05 * |
| CVST Group (n = 80) | Controls (n = 80) | ||||
|---|---|---|---|---|---|
| 4G/5G Genotype | Number (%) | tHcy, µmol/L | Number (%) | tHcy, µmol/L | p-Value |
| Mean ± Std | Mean ± Std | ||||
| 5G/5G | 6 (7.5%) | 21.5 ± 11.67 | 20 (25%) | 11.1 ± 3.17 | 0.001 |
| 4G/4G | 32 (40%) | 50.56 ± 37.98 | 22 (27.5%) | 20.22 ± 7.41 | 0.032 |
| 4G/5G | 42 (52.5%) | 18.19 ± 17.16 | 38 (47.5%) | 8.14 ± 4.94 | 0.516 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gogu, A.E.; Motoc, A.G.; Stroe, A.Z.; Docu Axelerad, A.; Docu Axelerad, D.; Petrica, L.; Jianu, D.C. Plasminogen Activator Inhibitor-1 (PAI-1) Gene Polymorphisms Associated with Cardiovascular Risk Factors Involved in Cerebral Venous Sinus Thrombosis. Metabolites 2021, 11, 266. https://doi.org/10.3390/metabo11050266
Gogu AE, Motoc AG, Stroe AZ, Docu Axelerad A, Docu Axelerad D, Petrica L, Jianu DC. Plasminogen Activator Inhibitor-1 (PAI-1) Gene Polymorphisms Associated with Cardiovascular Risk Factors Involved in Cerebral Venous Sinus Thrombosis. Metabolites. 2021; 11(5):266. https://doi.org/10.3390/metabo11050266
Chicago/Turabian StyleGogu, Anca Elena, Andrei Gheorghe Motoc, Alina Zorina Stroe, Any Docu Axelerad, Daniel Docu Axelerad, Ligia Petrica, and Dragos Catalin Jianu. 2021. "Plasminogen Activator Inhibitor-1 (PAI-1) Gene Polymorphisms Associated with Cardiovascular Risk Factors Involved in Cerebral Venous Sinus Thrombosis" Metabolites 11, no. 5: 266. https://doi.org/10.3390/metabo11050266