
Wild-Type AmpC Beta-Lactamase-Producing Enterobacterales Are a Risk Factor for Empirical Treatment Failure in Patients with Bloodstream Infection

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Definitions and Statistical Analysis
3. Results
3.1. Population Characteristics
3.2. Risk Factors for a Worse Clinical Outcome
3.3. Risk Factors for Ineffective Empirical Therapy
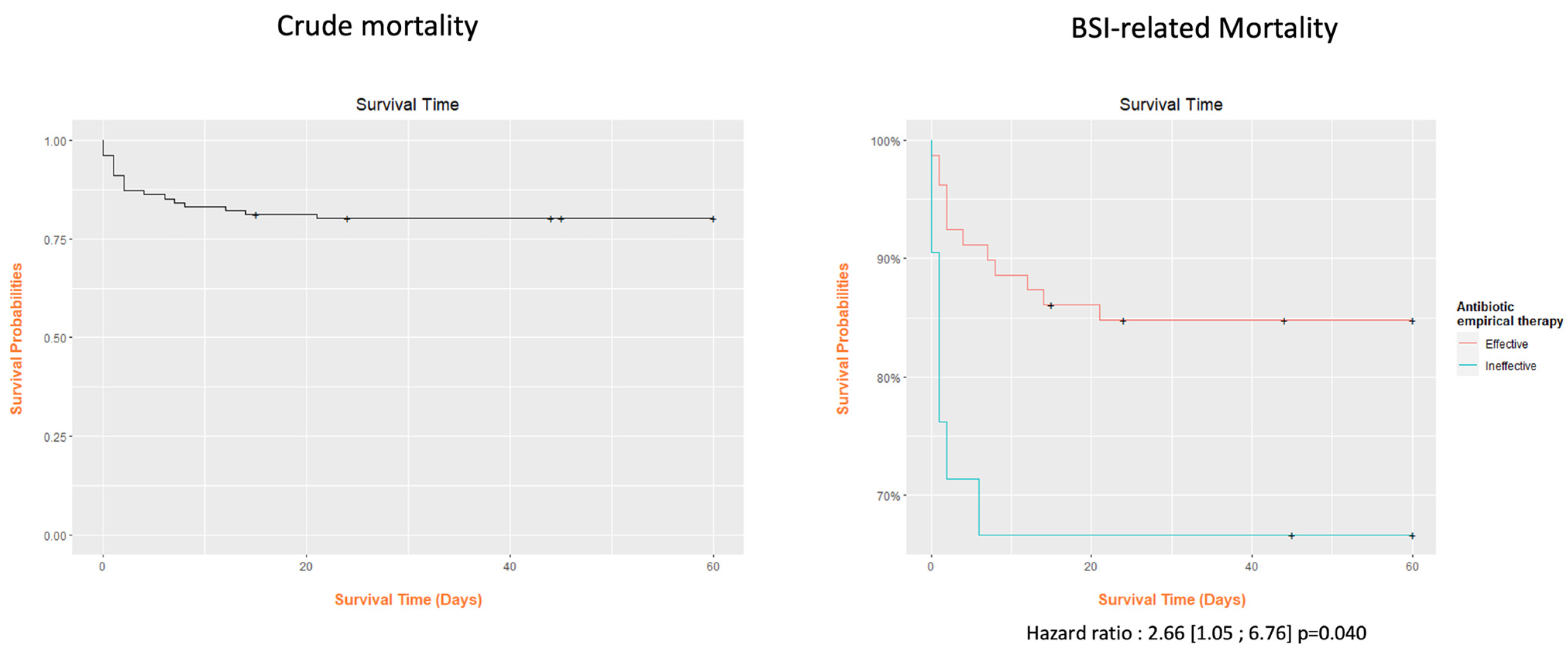
3.4. Analysis of Deaths
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Antimicrobial Resistance and the United Nations Sustainable Development Cooperation Framework: Guidance for United Nations Country Teams. 2021. Available online: https://www.who.int/publications/i/item/9789240036024 (accessed on 25 November 2023).
- Viscoli, C. Bloodstream Infections: The peak of the iceberg. Virulence 2016, 7, 248–251. [Google Scholar] [CrossRef]
- Mizrahi, A.; Delerue, T.; Morel, H.; Le Monnier, A.; Carbonnelle, E.; Pilmis, B.; Zahar, J. Infections caused by naturally AmpC-producing Enterobacterales: Can we use third-generation cephalosporins? A narrative review. Int. J. Antimicrob. Agents 2019, 55, 105834. [Google Scholar] [CrossRef]
- Harris, P.; Ferguson, J. Antibiotic therapy for inducible AmpC β-lactamase-producing Gram-negative bacilli: What are the alternatives to carbapenems, quinolones and aminoglycosides? Int. J. Antimicrob. Agents 2012, 40, 297–305. [Google Scholar] [CrossRef]
- de Lastours, V.; Goulenok, T.; Guérin, F.; Jacquier, H.; Eyma, C.; Chau, F.; Cattoir, V.; Fantin, B. Ceftriaxone promotes the emergence of AmpC-overproducing Enterobacteriaceae in gut microbiota from hospitalized patients. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Aitken, S.L.; Bonomo, R.A.; Mathers, A.J.; van Duin, D.; Clancy, C.J. Infectious Diseases Society of America Guidance on the treatment of AmpC β Lactamase producing Enterobacterales, Carbapenem resistant Acinetobacter baumannii, and Stenotrophomonas maltophilia infections. Clin. Infect. Dis. 2022, 74, 2089–2114. [Google Scholar] [CrossRef] [PubMed]
- Chastre, J.; Wolff, M.; Fagon, J.Y.; Chevret, S.; Thomas, F.; Wermert, D.; Clementi, E.; Gonzalez, J.; Jusserand, D.; Asfar, P.; et al. Comparison of 8 vs. 15 days of antibiotic therapy for ventilator associated pneumonia in adults: A randomized trial. JAMA 2003, 290, 2588–2598. [Google Scholar] [CrossRef]
- Maillard, A.; Delory, T.; Bernier, J.; Villa, A.; Chaibi, K.; Escaut, L.; Contejean, A.; Bercot, B.; Robert, J.; El Alaoui, F.; et al. Effectiveness of third-generation cephalosporins or piperacillin compared with cefepime or carbapenems for severe infections caused by wild-type AmpC β-lactamase-producing Enterobacterales: A multi-centre retrospective propensity-weighted study. Int. J. Antimicrob. Agents 2023, 62, 106809. [Google Scholar] [CrossRef]
- Mounier, R.; Le Guen, R.; Woerther, P.-L.; Nacher, M.; Bonnefon, C.; Mongardon, N.; Langeron, O.; Levesque, E.; Couffin, S.; Houcke, S.; et al. Clinical outcome of wild-type AmpC-producing Enterobacterales infection in critically ill patients treated with β-lactams: A prospective multicenter study. Ann. Intensiv. Care 2022, 12, 107. [Google Scholar] [CrossRef] [PubMed]
- Battle, S.E.; Augustine, M.R.; Watson, C.M.; Bookstaver, P.B.; Kohn, J.; Owens, W.B.; Baddour, L.M.; Al-Hasan, M.N. Derivation of a quick Pitt bacteremia score to predict mortality in patients with Gram-negative bloodstream infection. Infection 2019, 47, 571–578. [Google Scholar] [CrossRef]
- Kang, C.I.; Kim, S.H.; Park, W.B.; Lee, K.D.; Kim, H.B.; Oh, M.D.; Kim, E.C.; Choe, K.W. Bloodstream infections caused by Enterobacter species: Predictors of 30-day mortality rate and impact of broad-spectrum cephalosporin resistance on outcome. Clin. Infect. Dis. 2004, 39, 812–818. [Google Scholar] [CrossRef]
- Kennelly, S.; McCabe, J.J. Acute care of older patients in the emergency department: Strategies to improve patient outcomes. Open Access Emerg. Med. 2015, 7, 45–54. [Google Scholar] [CrossRef]
- Round, A.; Crabb, T.; Buckingham, K.; Mejzner, R.; Pearce, V.; Ayres, R.; Weeks, C.; Hamilton, W. Six month outcomes after emergency admission of elderly patients to a community or a district general hospital. Fam. Pr. 2004, 21, 173–179. [Google Scholar] [CrossRef]
- Hwang, U.; Morrison, R.S. The geriatric emergency department. J. Am. Geriatr. Soc. 2007, 55, 1873–1876. [Google Scholar] [CrossRef]
- Rau, R.; Muszyńska, M.M.; Vaupel, J.W. Europe, the Oldest-Old Continent. In The Demography of Europe; Neyer, G., Andersson, G., Kulu, H., Bernardi, L., Bühler, C., Eds.; Springer: Berlin/Heidelberg, Germany, 2013; pp. 119–137. [Google Scholar]
- Juneja, D.; Nasa, P.; Singh, O. Severe sepsis and septic shock in the elderly: An overview. World J. Crit. Care Med. 2012, 1, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Martín, S.; Pérez, A.; Aldecoa, C. Sepsis and Immunosenescence in the Elderly Patient: A Review. Front. Med. 2017, 4, 20. [Google Scholar] [CrossRef]
- Livorsi, D.J.; Stenehjem, E.; Stephens, D.S. Virulence factors of gram-negative bacteria in sepsis with a focus on Neisseria meningitides. Contrib. Microbiol. 2011, 17, 31–47. [Google Scholar] [CrossRef] [PubMed]
- Baltas, I.; Stockdale, T.; Tausan, M.; Kashif, A.; Anwar, J.; Anvar, J.; Koutoumanou, E.; Sidebottom, D.; Garcia-Arias, V.; Wright, M.; et al. Long-term outcome and risk factors for late mortality in Gram-negative bacteraemia: A retrospective cohort study. J. Glob. Antimicrob. Resist. 2021, 25, 187–192. [Google Scholar] [CrossRef]
- Breijyeh, Z.; Jubeh, B.; Karaman, R. Resistance of Gram-Negative Bacteria to Current Antibacterial Agents and Approaches to Resolve It. Molecules 2020, 25, 1340. [Google Scholar] [CrossRef] [PubMed]
- Lemenand, O.; Caillon, J.; Coeffic, T.; Colomb-Cotinat, M.; Thibaut, S.; Birgand, G. National Primary Care Surveillance of Resistance to 3rd-Generation Cephalosporins and Fluoroquinolones in Urinary Isolates of Escherichia coli: 2015–2019 Trends in France. Article—Bulletin Epidémiologique Hebdomadaire. Available online: www.santepubliquefrance.fr (accessed on 7 December 2023).
- Lemenand, O.; Coeffic, T.; Thibaut, S.; Cotinat, M.C.; Caillon, J.; Birgand, G. Decreasing proportion of extended-spectrum beta-lactamase among E. coli infections during the COVID-19 pandemic in France. J. Infect. 2021, 83, 664–670. [Google Scholar] [CrossRef]
- Antimicrobial Resistance Surveillance in Europe 2022–2020 Data. 2022. Available online: https://www.ecdc.europa.eu/en/publications-data/antimicrobial-resistance-surveillance-europe-2022-2020-data (accessed on 1 December 2023).
- McKinnell, J.A.; Kunz, D.F.; Chamot, E.; Patel, M.; Shirley, R.M.; Moser, S.A.; Baddley, J.W.; Pappas, P.G.; Miller, L.G. Association between vancomycin-resistant Enterococci bacteremia and ceftriaxone usage. Infect. Control. Hosp. Epidemiol. 2012, 33, 718–724. [Google Scholar] [CrossRef]
- Herrmann, J.; Burgener-Gasser, A.-V.; Goldenberger, D.; Roth, J.; Weisser, M.; Tamma, P.D.; Tschudin-Sutter, S. Cefepime versus carbapenems for treatment of AmpC beta-lactamase-producing Enterobacterales bloodstream infections. Eur. J. Clin. Microbiol. Infect. Dis. 2023, 43, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Cosgrove, S.E.; Maragakis, L.L. Combination therapy for treatment of infections with gram-negative bacteria. Clin. Microbiol. Rev. 2012, 25, 450–470. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock. Crit. Care Med. 2021, 49, e1063–e1143. [Google Scholar] [CrossRef] [PubMed]
- Paul, M.; Lador, A.; Grozinsky-Glasberg, S.; Leibovici, L. Beta lactam antibiotic monotherapy versus beta lactam-aminoglycoside antibiotic combination therapy for sepsis. Cochrane Database Syst. Rev. 2014, 2014, CD003344. [Google Scholar] [CrossRef]
- Choi, S.-H.; Lee, J.E.; Park, S.J.; Choi, S.-H.; Lee, S.-O.; Jeong, J.-Y.; Kim, M.-N.; Woo, J.H.; Kim, Y.S. Emergence of Antibiotic Resistance during Therapy for Infections Caused by Enterobacteriaceae Producing AmpC β-Lactamase: Implications for Antibiotic Use. Antimicrob. Agents Chemother. 2008, 52, 995–1000. [Google Scholar] [CrossRef]


{kind=link}
| N (%) or Mean [SD] | |
|---|---|
| Number of patients | 101 |
| Age (years) | 78.6 [12.1] |
| Male gender | 61 (67.4%) |
| With active cancer | 30 (29.7%) |
| Number of comorbid conditions | |
| 0 | 3 (3.0%) |
| 1 | 25 (24.8%) |
| 2 | 37 (36.6%) |
| ≥3 | 36 (35.6%) |
| Healthcare-associated infection | 17 (17.0%) |
| Septic shock associated with BSI | 13 (12.9%) |
| Department at the time of BSI diagnosis | |
| Medical Department | 95 (94.1%) |
| Intensive Care Unit | 6 (5.9%) |
| Site of infection | |
| Urinary tract | 59 (58.4%) |
| Gastrointestinal | 22 (21.8%) |
| Pulmonary | 6 (5.9%) |
| Vascular catheter | 5 (5.0%) |
| Other | 9 (8.9%) |
| Type of Enterobacterales | |
| ESCPM group | 18 (17.8%) |
| Other Enterobacterales | 83 (82.2%) |
| qPitt score for BSI severity | |
| <2 | 83 (82.2%) |
| ≥2 | 18 (17.8%) |
| ESBL | 8 (8.2%) |
| Effective empirical treatment | |
| No | 21 (21.0%) |
| Yes | 79 (79.0%) |
| Type of empirical antimicrobial therapy | |
| Single therapy | 60 (62.5%) |
| Combination therapy | 36 (37.5%) |
| Clinical stability at 48 h | |
| No | 32 (31.7%) |
| Yes | 69 (68.3%) |
| In-hospital death | 24 (23.8%) |
| Death probably related to BSI | |
| No | 4 (16.7%) |
| Yes | 20 (83.3%) |
| Clinical instability at 48 h or death | 36 (35.6%) |
| Recurrent BSI within 14 days | 3 (3.0%) |
| (a) | |||||
|---|---|---|---|---|---|
| Clinically Stable at 48 h and No Death n = 65 | Clinically Unstable at 48 h or Death n = 36 | ||||
| Mean | [SD] | Mean | [SD] | p-Value | |
| Age | 79.9 | [11.3] | 76.3 | [13.2] | 0.249 |
| Days of hospitalization | 12.8 | [10.1] | 12.1 | [10.9] | 0.524 |
| Delay until reassessment of empirical therapy (days) | 3.6 | [1.9] | 3.3 | [2.7] | 0.201 |
| Days of antibiotic therapy | 14.0 | [7.1] | 10.4 | [9.5] | 0.010 |
| qPitt score | 0.5 | [0.77] | 0.8 | [0.95] | 0.123 |
| White-cell count (cc/mmcc) | 13,622.2 | [8757.7] | 14,068.3 | [7650.2] | 0.618 |
| C-reactive protein (mg/L) | 122.6 | [96.8] | 153.6 | [123.0] | 0.242 |
| Procalcitonin (ng/mL) | 31.6 | [52.3] | 38.5 | [59.8] | 0.777 |
| n | (%) | n | (%) | p-Value | |
| Gender | 0.244 | ||||
| Female | 23 | (35.4) | 17 | (47.2) | |
| Male | 39 | (34.2) | 26 | (59.1) | |
| Comorbidities | 1.000 | ||||
| No | 2 | (3.1) | 1 | (2.8) | |
| Yes | 63 | (96.9) | 35 | (97.2) | |
| Healthcare associated BSI | 0.240 | ||||
| No | 51 | (79.7) | 32 | (88.9) | |
| Yes | 13 | (20.3) | 4 | (11.1) | |
| ICU at BSI diagnosis | 0.663 | ||||
| No | 62 | (95.4) | 33 | (91.7) | |
| Yes | 3 | (4.6) | 3 | (8.3) | |
| qPitt score | 0.257 | ||||
| <2 | 56 | (86.2) | 27 | (75.0) | |
| ≥2 | 9 | (13.8) | 9 | (25.0) | |
| Septic shock | 0.011 | ||||
| No | 61 | (92.3) | 27 | (75.0) | |
| Yes | 4 | (6.2) | 9 | (25.0) | |
| ESBL | 1.000 | ||||
| No | 60 | (92.3) | 30 | (90.9) | |
| Yes | 5 | (7.7) | 3 | (9.1) | |
| Type of Enterobacterales | 0.013 | ||||
| ESCPM group | 7 | (10.8) | 11 | (30.6) | |
| Other | 58 | (89.2) | 25 | (71.4) | |
| Effective empirical therapy | 0.001 | ||||
| No | 7 | (10.8) | 14 | (40.0) | |
| Yes | 58 | (89.2) | 21 | (60.0) | |
| Type of empirical therapy | 0.015 | ||||
| Single therapy | 46 | (70.8) | 14 | (45.2) | |
| Combination therapy | 19 | (29.2) | 17 | (54.8) | |
| (b) | |||||
| AdjOR | [95% CI] | p-Value | |||
| Septic shock | |||||
| No | 1 | ||||
| Yes | 5.30 | [1.47; 22.19] | 0.014 | ||
| Initial empirical antibiotic therapy | |||||
| Ineffective | 5.54 | [1.95; 17.01] | 0.002 | ||
| Effective | 1 | ||||
| (a) | |||||
|---|---|---|---|---|---|
| Ineffective Empirical Therapy n = 21 | Effective Empirical Therapy n = 79 | ||||
| Mean | [SD] | Mean | [SD] | p-Value | |
| Age (years) | 76.9 | [10.4] | 79.0 | [12.5] | 0.275 |
| Days of hospitalization | 11.1 | [9.7] | 12.8 | [10.5] | 0.592 |
| Delay until reassessment of empirical therapy (days) | 3.1 | [1.4] | 3.6 | [2.3] | 0.827 |
| White-cell count (cc/mmcc) | 12,107.6 | [6770.2] | 14,416.6 | [8599.6] | 0.341 |
| C-reactive protein (mg/L) | 156.3 | [145.5] | 126.4 | [95.3] | 0.775 |
| Procalcitonin (ng/mL) | 60.1 | [100.2] | 31.0 | [47.6] | 0.975 |
| n | (%) | n | (%) | p-Value | |
| Gender | 0.924 | ||||
| Female | 8 | (38.1) | 31 | (39.2) | |
| Male | 13 | (61.9) | 48 | (60.8) | |
| ICU when BSI | 0.603 | ||||
| No | 19 | (90.5) | 75 | (94.9) | |
| Yes | 2 | (9.5) | 4 | (5.1) | |
| Septic shock | 0.464 | ||||
| No | 17 | (81.0) | 70 | (88.6) | |
| Yes | 4 | (6.2) | 9 | (25.0) | |
| ESBL | 0.008 | ||||
| No | 15 | (75.0) | 75 | (96.2) | |
| Yes | 6 | (25.0) | 3 | (3.8) | |
| Type of Enterobacterales | <0.001 | ||||
| ESCPM group | 10 | (47.6) | 8 | (10.1) | |
| Other | 11 | (52.4) | 71 | (89.9) | |
| Clinically unstable at 48 hr or death | |||||
| No | 7 | (33.3) | 58 | (73.4) | |
| Yes | 14 | (66.7) | 21 | (26.6) | |
| Type of empirical therapy | 0.001 | ||||
| Single therapy | 10 | (47.6) | 49 | (62.0 | |
| Combination therapy | 6 | (28.6) | 30 | (38.0) | |
| No empirical therapy | 5 | (23.8) | 0 | (0.0) | |
| (b) | |||||
| AdjOR | [95% CI] | p-Value | |||
| ESBL | |||||
| No | 1 | ||||
| Yes | 9.40 | [1.70; 62.14] | 0.012 | ||
| Type of Enterobacterales | |||||
| ESCPM group | 5.89 | [1.70; 21.40] | 0.006 | ||
| Other | 1 | ||||
| Clinical instability at 48 hr or death | |||||
| No | 1 | ||||
| Yes | 4.71 | [1.44; 17.08] | 0.012 | ||
| (a) | ||||||||||||
| Patient | Sex | Age (years) | Number of Comorbidities | ESCPM Species | ESBL | Suspected Site Associated witd BSI | Healthcare-Associated Infection | qPitt Score for Severity | Initial Empirical Therapy according to AST | Clinical Stability after 48 h | Delay Until Reassessment of Therapy in Case of Switch (days) | In-Hospital Death |
| 1 | M | 65 | 2 | Enterobacter cloacae | Yes | Urinary | No | 0 | Effective | Yes | No change | No |
| 2 | M | 69 | 2 | Enterobacter cloacae | No | Gastrointestinal | No | 0 | Ineffective | Yes | 5 | No |
| 3 | F | 77 | 3 | Klebsiella aerogenes | No | Vascular | No | 0 | Ineffective | No | 3 | No |
| 4 | M | 72 | 2 | Enterobacter cloacae | No | Pulmonary | Yes | 2 | Ineffective | Yes | No change | Yes |
| 5 | M | 88 | 4 | Enterobacter cloacae | Yes | Urinary | No | 0 | Ineffective | No | 5 | No |
| 6 | F | 69 | 1 | Enterobacter cloacae | No | Gastrointestinal | No | 1 | Ineffective | No | No change | Yes |
| 7 | M | 89 | 2 | Enterobacter cloacae | Yes | Vascular | Yes | 0 | Effective | Yes | 2 | No |
| 8 | F | 70 | 1 | Enterobacter cloacae | No | Gastrointestinal | No | 2 | Effective | Yes | No change | No |
| 9 | M | 58 | 1 | Enterobacter cloacae | No | Gastrointestinal | No | 0 | Ineffective | Yes | 1 | No |
| 10 | M | 56 | 1 | Providencia stuartii | No | Urinary | No | 2 | Ineffective | No | 3 | No |
| 11 | F | 85 | 2 | Morganella morgnaii | No | Urinary | No | 0 | Effective | Yes | No change | No |
| 12 | F | 85 | 3 | Pantoea agglomerans | No | Vascular | No | 0 | Effective | No | 2 | No |
| 13 | M | 91 | 1 | Morganella morgnaii | No | Urinary | No | 1 | Effective | No | 1 | Yes |
| 14 | M | 81 | 3 | Serratia marcescens | No | Gastrointestinal | No | 0 | Ineffective | No | 3 | No |
| 15 | M | 69 | 2 | Serratia marcescens | No | Skin and soft tissues | Yes | 0 | Effective | Yes | No change | No |
| 16 | M | 77 | 4 | Serratia marcescens | No | Gastrointestinal | Yes | 0 | Ineffective | No | No change | No |
| 17 | F | 79 | 3 | Serratia marcescens | No | NA | No | 1 | Ineffective | No | No change | Yes |
| 18 | M | 54 | 2 | Serratia marcescens | No | Vascular | No | 0 | Effective | No | 10 | Yes |
| (b) | ||||||||||||
| Patient | Sex | Age | Number of Comorbidities | Enterobacterales Species | Suspected Site Associated with BSI | Healthcare-Associated Infection | qPitt Score for Severity | Initial Empirical Therapy | Clinical Stability after 48 h | Delay until Reassessment of Therapy in Case of Switch (days) | In-Hospital Death | |
| 1 | M | 65 | 2 | Enterobacter cloacae | Urinary | No | 0 | Effective | Yes | No change | No | |
| 2 | M | 83 | 3 | Escherichia coli | Pulmonary | No | 2 | Ineffective | No | 2 | Yes | |
| 3 | M | 88 | 4 | Enterobacter cloacae | Urinary | No | 0 | Ineffective | No | 5 | No | |
| 4 | M | 89 | 2 | Enterobacter cloacae | Vascular | Yes | 0 | Effective | Yes | 2 | No | |
| 5 | F | 63 | 2 | Escherichia coli | Urinary | No | 0 | Ineffective | No | 2 | No | |
| 6 | F | 83 | 2 | Klebsiella pneumoniae | Urinary | Yes | 1 | Effective | Yes | No change | No | |
| 7 | F | 88 | 3 | Escherichia coli | Gastrointestinal | No | 2 | Ineffective | Yes | 4 | No | |
| 8 | F | 78 | 2 | Escherichia coli | Urinary | No | 0 | Ineffective | Yes | 5 | No | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vassallo, M.; Fabre, R.; Lotte, L.; Manni, S.; Pradier, C. Wild-Type AmpC Beta-Lactamase-Producing Enterobacterales Are a Risk Factor for Empirical Treatment Failure in Patients with Bloodstream Infection. Diseases 2024, 12, 52. https://doi.org/10.3390/diseases12030052
Vassallo M, Fabre R, Lotte L, Manni S, Pradier C. Wild-Type AmpC Beta-Lactamase-Producing Enterobacterales Are a Risk Factor for Empirical Treatment Failure in Patients with Bloodstream Infection. Diseases. 2024; 12(3):52. https://doi.org/10.3390/diseases12030052
Chicago/Turabian StyleVassallo, Matteo, Roxane Fabre, Laurene Lotte, Sabrina Manni, and Christian Pradier. 2024. "Wild-Type AmpC Beta-Lactamase-Producing Enterobacterales Are a Risk Factor for Empirical Treatment Failure in Patients with Bloodstream Infection" Diseases 12, no. 3: 52. https://doi.org/10.3390/diseases12030052