
Decompressive Craniectomy in Severe Traumatic Brain Injury: The Intensivist’s Point of View
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
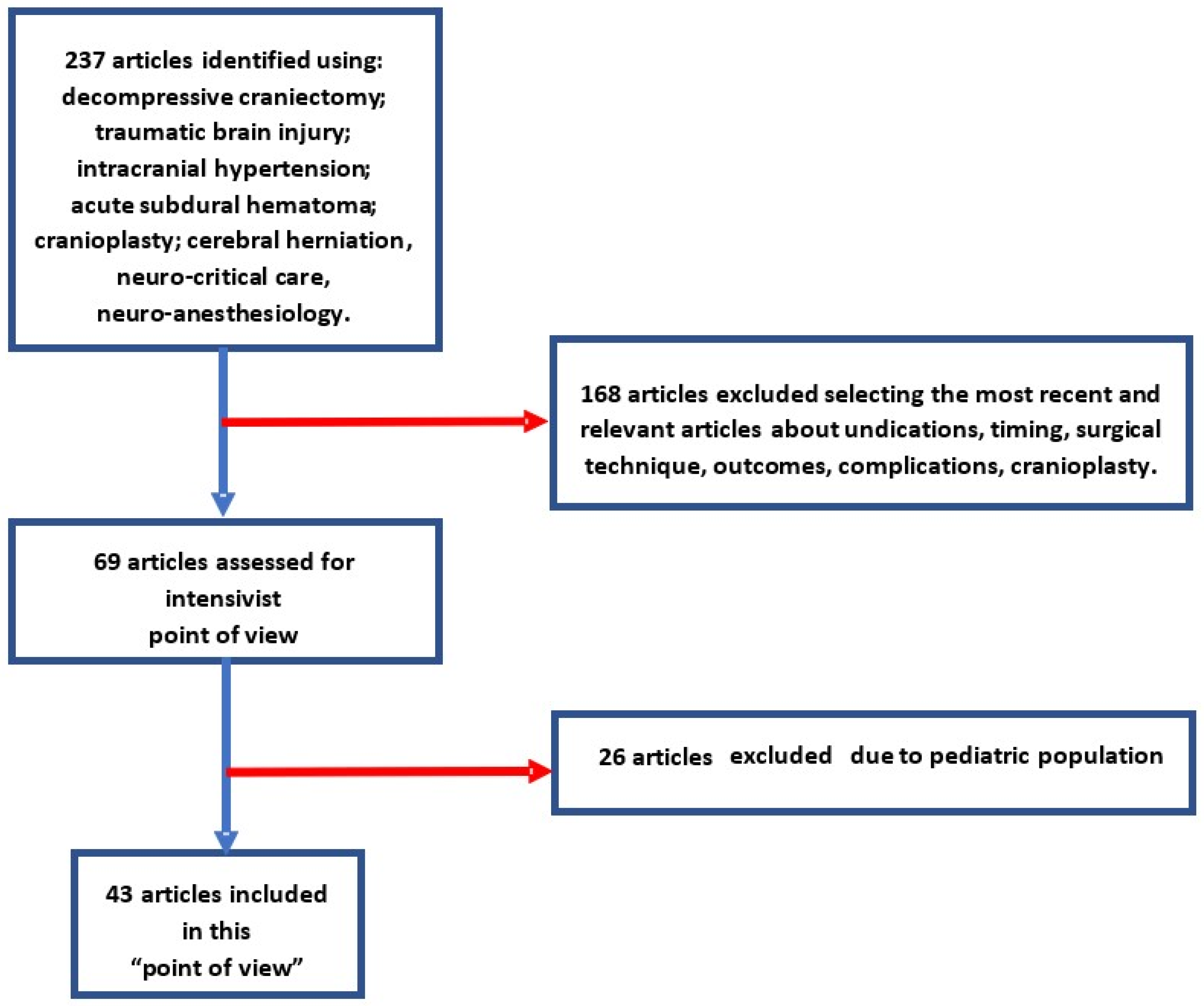
2. Methods
3. Discussion
3.1. Traumatic Brain Injury (TBI)
3.2. Classification
3.3. Pathophysiology
3.4. Decompressive Craniectomy (DC)
3.5. Primary DC
3.6. Secondary DC
3.6.1. Surgical Techniques
3.6.2. Bifrontal DC
3.6.3. Fronto-Parieto-Temporal DC or Hemicraniectomy
3.6.4. Novel Surgical Techniques
3.7. Complications
3.8. Acute Complications
3.9. Late Complication
3.10. Outcome
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Agrawal, D.; Hussain, N. Decompressive craniectomy in cerebral toxoplasmosis. Eur. J. Clin. Microbiol. Infect. Dis. 2005, 24, 772–773. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Bovet, J.; Garcia-Armengol, R.; Buxó-Pujolràs, M.; Lorite-Díaz, N.; Narvaez-Martinez, A.; Caro-Cardera, J.L.; Rimbau-Muñoz, J.; Joly-Torta, M.C.; Castellví-Joan, M.; Martín-Ferrer, S. Decompressive craniectomy for encephalitis with brain herniation: Case report and review of the literature. Acta Neurochir. 2012, 154, 1717–1724. [Google Scholar] [CrossRef] [PubMed]
- Rabelino, G.A.G.; Fons, C.; Rey, A.; Roussos, I.; Campistol, J. Craniectomy in Herpetic Encephalitis. Pediatr. Neurol. 2008, 39, 201–203. [Google Scholar] [CrossRef] [PubMed]
- Wada, Y.; Kubo, T.; Asano, T.; Senda, N.; Isono, M.; Kobayashi, H. Fulminant Subdural Empyema Treated with a Wide Decompressive Craniectomy and Continuous Irrigation. Case Report. Neurol. Med. Chir. 2002, 42, 414–416. [Google Scholar] [CrossRef] [Green Version]
- Ong, Y.; Goh, K.; Chan, C. Bifrontal decompressive craniectomy for acute subdural empyema. Childs Nerv. Syst. 2002, 18, 340–343. [Google Scholar] [CrossRef]
- Ziai, W.C.; Port, J.D.; Cowan, J.A.; Garonzik, I.M.; Bhardwaj, A.; Rigamonti, D. Decompressive Craniectomy for Intractable Cerebral Edema: Experience of a Single Center. J. Neurosurg. Anesthesiol. 2003, 15, 25–32. [Google Scholar] [CrossRef]
- Brazinova, A.; Rehorcikova, V.; Taylor, M.; Buckova, V.; Majdan, M.; Psota, M.; Peeters, W.; Feigin, V.L.; Theadom, A.; Holkovic, L.; et al. Epidemiology of Traumatic Brain Injury in Europe: A Living Systematic Review. J. Neurotrauma 2021, 38, 1411–1440. [Google Scholar] [CrossRef] [Green Version]
- Kaur, P.; Sharma, S. Recent Advances in Pathophysiology of Traumatic Brain Injury. Curr. Neuropharmacol. 2017, 16, 1224–1238. [Google Scholar] [CrossRef]
- Longhitano, Y.; Iannuzzi, F.; Bonatti, G.; Zanza, C.; Messina, A.; Godoy, D.; Dabrowski, W.; Xiuyun, L.; Czosnyka, M.; Pelosi, P.; et al. Cerebral Autoregulation in Non-Brain Injured Patients: A Systematic Review. Front. Neurol. 2021, 12, 732176. [Google Scholar] [CrossRef]
- Zanza, C.; Thangathurai, J.; Audo, A.; Muir, H.A.; Candelli, M.; Pignataro, G.; Thangathurai, D.; Cicchinelli, S.; Racca, F.; Longhitano, Y.; et al. Oxidative stress in critical care and vitamins supplement therapy: “A beneficial care enhancing”. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 7703–7712. [Google Scholar]
- Rossini, Z.; Nicolosi, F.; Kolias, A.; Hutchinson, P.J.; De Sanctis, P.; Servadei, F. The History of Decompressive Craniectomy in Traumatic Brain Injury. Front. Neurol. 2019, 10, 458. [Google Scholar] [CrossRef]
- Hawryluk, G.W.J.; Rubiano, A.M.; Totten, A.M.; O’Reilly, C.; Ullman, J.S.; Bratton, S.L.; Chesnut, R.; Harris, O.A.; Kissoon, N.; Shutter, L.; et al. Guidelines for the management of severe traumatic brain injury: 2020 update of the decompressive craniectomy recommendations. Neurosurgery 2020, 87, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, P.J.; Kolias, A.G.; Tajsic, T.; Adeleye, A.; Aklilu, A.T.; Apriawan, T.; Bajamal, A.H.; Barthélemy, E.J.; Devi, B.I.; Bhat, D.; et al. Consensus statement from the International Consensus Meeting on the Role of Decompressive Craniectomy in the Management of Traumatic Brain Injury: Consensus Statement. Acta Neurochir. 2019, 161, 1261–1274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bullock, M.R.; Chesnut, R.; Ghajar, J.; Gordon, D.; Hartl, R.; Newell, D.W.; Servadei, F.; Walters, B.C.; Wilberger, J.; Surgical Management of Traumatic Brain Injury Author Group. Surgical Management of Traumatic Parenchymal Lesions. Neurosurgery 2006, 58, S25–S46. [Google Scholar] [CrossRef] [PubMed]
- Kolias, A.; Scotton, W.J.; Belli, A.; King, A.; Brennan, P.M.; Bulters, D.O.; Eljamel, M.S.; Wilson, M.H.; Papadopoulos, M.C.; Mendelow, A.D.; et al. Surgical management of acute subdural haematomas: Current practice patterns in the United Kingdom and the Republic of Ireland. Br. J. Neurosurg. 2013, 27, 330–333. [Google Scholar] [CrossRef]
- Li, L.M.; Kolias, A.G.; Guilfoyle, M.R.; Timofeev, I.; Corteen, E.A.; Pickard, J.D.; Menon, D.K.; Kirkpatrick, P.J.; Hutchinson, P.J. Outcome following evacuation of acute subdural haematomas: A comparison of craniotomy with decompressive craniectomy. Acta Neurochir. 2012, 154, 1555–1561. [Google Scholar] [CrossRef]
- Shibahashi, K.; Sugiyama, K.; Tomio, J.; Hoda, H.; Morita, A. In-hospital mortality and length of hospital stay with craniotomy versus craniectomy for acute subdural hemorrhage: A multicenter, propensity score–matched analysis. J. Neurosurg. 2020, 133, 504–513. [Google Scholar] [CrossRef]
- Cooper, D.J.; Rosenfeld, J.V.; Murray, L.; Arabi, Y.M.; Davies, A.R.; D’Urso, P.; Kossmann, T.; Ponsford, J.; Seppelt, I.; Reilly, P.; et al. Decompressive Craniectomy in Diffuse Traumatic Brain Injury. N. Engl. J. Med. 2011, 364, 1493–1502. [Google Scholar] [CrossRef] [Green Version]
- Hutchinson, P.J.; Kolias, A.G.; Timofeev, I.S.; Corteen, E.A.; Czosnyka, M.; Timothy, J.; Anderson, I.; Bulters, D.O.; Belli, A.; Eynon, C.A.; et al. Trial of Decompressive Craniectomy for Traumatic Intracranial Hypertension. N. Engl. J. Med. 2016, 375, 1119–1130. [Google Scholar] [CrossRef] [Green Version]
- Cooper, D.J.; Rosenfeld, J.V.; Murray, L.; Arabi, Y.M.; Davies, A.R.; Ponsford, J.; Seppelt, I.; Reilly, P.; Wiegers, E.; Wolfe, R.; et al. Patient Outcomes at Twelve Months after Early Decompressive Craniectomy for Diffuse Traumatic Brain Injury in the Randomized DECRA Clinical Trial. J. Neurotrauma 2020, 37, 810–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, W.; Guo, C.; Shen, H.; Chen, K.; Wen, L.; Huang, H.; Ding, M.; Sun, L.; Jiang, Q.; Wang, W. Effects of unilateral decompressive craniectomy on patients with unilateral acute post-traumatic brain swelling after severe traumatic brain injury. Crit. Care 2009, 13, R185. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.-Y.; Xu, W.; Li, W.-P.; Xu, W.-H.; Zhang, J.; Bao, Y.-H.; Ying, Y.-H.; Luo, Q.-Z. Efficacy of Standard Trauma Craniectomy for Refractory Intracranial Hypertension with Severe Traumatic Brain Injury: A Multicenter, Prospective, Randomized Controlled Study. J. Neurotrauma 2005, 22, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Schirmer, C.M.; Ackil, A.A.; Malek, A.M. Decompressive Craniectomy. Neurocritical Care 2008, 8, 456–470. [Google Scholar] [CrossRef]
- Reithmeier, T.; Löhr, M.; Pakos, P.; Ketter, G.; Ernestus, R.-I. Relevance of ICP and ptiO2 for indication and timing of decompressive craniectomy in patients with malignant brain edema. Acta Neurochir. 2005, 147, 947–952. [Google Scholar] [CrossRef] [PubMed]
- Soto, J.M.; Feng, D.; Sun, H.; Zhang, Y.; Lyon, K.A.; Liang, B.; Reed, L.K.; Huang, J.H. Novel Decompressive Hemicraniectomy Technique for Traumatic Brain Injury: Technical Note. World Neurosurg. 2021, 146, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Veldeman, M.; Daleiden, L.; Hamou, H.; Höllig, A.; Clusmann, H. An altered posterior question-mark incision is associated with a reduced infection rate of cranioplasty after decompressive hemicraniectomy. J. Neurosurg. 2021, 134, 1262–1270. [Google Scholar] [CrossRef]
- Olivecrona, M.; Rodling-Wahlström, M.; Naredi, S.; Koskinen, L.-O. Effective ICP Reduction by Decompressive Craniectomy in Patients with Severe Traumatic Brain Injury Treated by an ICP-Targeted Therapy. J. Neurotrauma 2007, 24, 927–935. [Google Scholar] [CrossRef]
- Longhitano, Y.L.; Zanza, C. The Route of Neuro-Critical Care. Rev. Recent Clin. Trials 2022, 17, 225–226. [Google Scholar] [CrossRef]
- Picard, N. The syndrome of the trephined. J. Neurosci. Rural. Pr. 2015, 6, 295–296. [Google Scholar] [CrossRef]
- Stiver, S.I.; Wintermark, M.; Manley, G.T. Motor trephine syndrome: A mechanistic hypothesis. Acta Neurochir. Suppl. 2008, 102, 273–277. [Google Scholar] [CrossRef]
- Honeybul, S. Neurological susceptibility to a skull defect. Surg. Neurol. Int. 2014, 5, 83. [Google Scholar] [CrossRef] [PubMed]
- Alkhaibary, A.; Alharbi, A.; Alnefaie, N.; Almubarak, A.O.; Aloraidi, A.; Khairy, S. Cranioplasty: A Comprehensive Review of the History, Materials, Surgical Aspects, and Complications. World Neurosurg. 2020, 139, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Malcolm, J.G.; Rindler, R.S.; Chu, J.K.; Grossberg, J.A.; Pradilla, G.; Ahmad, F.U. Complications following cranioplasty and relationship to timing: A systematic review and meta-analysis. J. Clin. Neurosci. 2016, 33, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Bowers, C.A.; Riva-Cambrin, J.; Hertzler, D.A.; Walker, M.L. Risk factors and rates of bone flap resorption in pediatric patients after decompressive craniectomy for traumatic brain injury. J. Neurosurg. Pediatr. 2013, 11, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Grant, G.A.; Jolley, M.; Ellenbogen, R.G.; Roberts, T.S.; Gruss, J.R.; Loeser, J.D. Failure of autologous bone-assisted cranioplasty following decompressive craniectomy in children and ad-olescents. J. Neurosurg. 2004, 100, 163–168. [Google Scholar] [CrossRef]
- Schuss, P.; Vatter, H.; Oszvald, Á.; Marquardt, G.; Imöhl, L.; Seifert, V.; Güresir, E. Bone Flap Resorption: Risk Factors for the Development of a Long-Term Complication following Cranioplasty after Decompressive Craniectomy. J. Neurotrauma 2013, 30, 91–95. [Google Scholar] [CrossRef]
- Kim, S.H.; Kang, D.S.; Cheong, J.H.; Kim, J.H.; Song, K.Y.; Kong, M.H. Comparison of Complications Following Cranioplasty Using a Sterilized Autologous Bone Flap or Polymethyl Methacrylate. Korean J. Neurotrauma 2017, 13, 15–23. [Google Scholar] [CrossRef] [Green Version]
- Acciarri, N.; Palandri, G.; Cuoci, A.; Valluzzi, A.; Lanzino, G. Cranioplasty in neurosurgery: Is there a way to reduce complications? J. Neurosurg. Sci. 2020, 64, 1–15. [Google Scholar] [CrossRef]
- van de Vijfeijken, S.E.; Münker, T.J.; Spijker, R.; Karssemakers, L.H.; Vandertop, W.P.; Becking, A.G.; Ubbink, D.T.; Dubois, L.; Milstein, D.; Depauw, P.; et al. Autologous Bone Is Inferior to Alloplastic Cranioplasties: Safety of Autograft and Allograft Materials for Cranioplasties, a Systematic Review. World Neurosurg. 2018, 117, 443–452.e8. [Google Scholar] [CrossRef]
- Alkhaibary, A.; Alharbi, A.; Abbas, M.; Algarni, A.; Abdullah, J.M.; Almadani, W.H.; Khairy, I.; Alkhani, A.; Aloraidi, A.; Khairy, S. Predictors of Surgical Site Infection in Autologous Cranioplasty: A Retrospective Analysis of Subcutaneously Preserved Bone Flaps in Abdominal Pockets. World Neurosurg. 2020, 133, e627–e632. [Google Scholar] [CrossRef]
- Celi, F.; Saal-Zapata, G. Decompressive Craniectomy for Traumatic Brain Injury: In-hospital Mortality-Associated Factors. J. Neurosci. Rural. Pract. 2020, 11, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Laic, R.A.G.; Bogaert, L.; Sloten, J.V.; Depreitere, B. Functional outcome, dependency and well-being after traumatic brain injury in the elderly population: A systematic review and meta-analysis. Brain Spine 2021, 100849. [Google Scholar] [CrossRef] [PubMed]
- Alouani, A.T.; Elfouly, T. Traumatic Brain Injury (TBI) Detection: Past, Present, and Future. Biomedicines 2022, 10, 2472. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Decompressive Craniectomy (DC) | Indications | Pathophysiology |
|---|---|---|
| Primary DC | Acute subdural hematoma (ASDH) in TBI and seldom lesions at low–medium risk (such as isolated epidural hematoma (EDH) and intraparenchymal contusion or hematoma) | Intracranial lesions causing a mass effect with altered ICP and brain herniation postoperatively |
| Secondary DC | Treatment of brain edema and the resultant elevated intracranial pressure (ICP) refractory to first-tier interventions. | The secondary injuries consist in metabolic cascade that begins after the head trauma leading to many biochemical cerebral changes (vasogenetic edema, loss of cellular homeostasis with cellular swelling mitochondrial dysfunction, RNS, ROS) |
| Complications | Type of Complications | |
|---|---|---|
| ACUTE COMPLICATIONS (Directly related to DC) | Ultra-early | Peri-operative events, such as blossoming of contusion, epidural hematoma, external cerebral herniation, intracranial infection, epilepsy, CSF leakage, and wound problems |
| Early (in the first months) | Subdural effusions or hygromas, evolution of contralateral mass lesions, paradoxal herniation, and infection | |
| Delayed events (after 30 days from DC) | Syndrome of the sinking skin flap (SSFS) or Trephined syndrome and hydrocephalus. | |
| LATE COMPLICATIONS (Related to cranioplasty) | Bone resorption, osteomyelitis, and hypo-vascular bone necrosis | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vitali, M.; Marasco, S.; Romenskaya, T.; Elia, A.; Longhitano, Y.; Zanza, C.; Abenavoli, L.; Scarpellini, E.; Bertuccio, A.; Barbanera, A. Decompressive Craniectomy in Severe Traumatic Brain Injury: The Intensivist’s Point of View. Diseases 2023, 11, 22. https://doi.org/10.3390/diseases11010022
Vitali M, Marasco S, Romenskaya T, Elia A, Longhitano Y, Zanza C, Abenavoli L, Scarpellini E, Bertuccio A, Barbanera A. Decompressive Craniectomy in Severe Traumatic Brain Injury: The Intensivist’s Point of View. Diseases. 2023; 11(1):22. https://doi.org/10.3390/diseases11010022
Chicago/Turabian StyleVitali, Matteo, Stefano Marasco, Tatsiana Romenskaya, Angela Elia, Yaroslava Longhitano, Christian Zanza, Ludovico Abenavoli, Emidio Scarpellini, Alessandro Bertuccio, and Andrea Barbanera. 2023. "Decompressive Craniectomy in Severe Traumatic Brain Injury: The Intensivist’s Point of View" Diseases 11, no. 1: 22. https://doi.org/10.3390/diseases11010022