Analysis of the Results of Heel-Rise Test with Sensors: A Systematic Review




Abstract
:1. Introduction
2. Methods
2.1. Research Questions
2.2. Inclusion Criteria
2.3. Search Strategy
2.4. Extraction of Study Characteristics
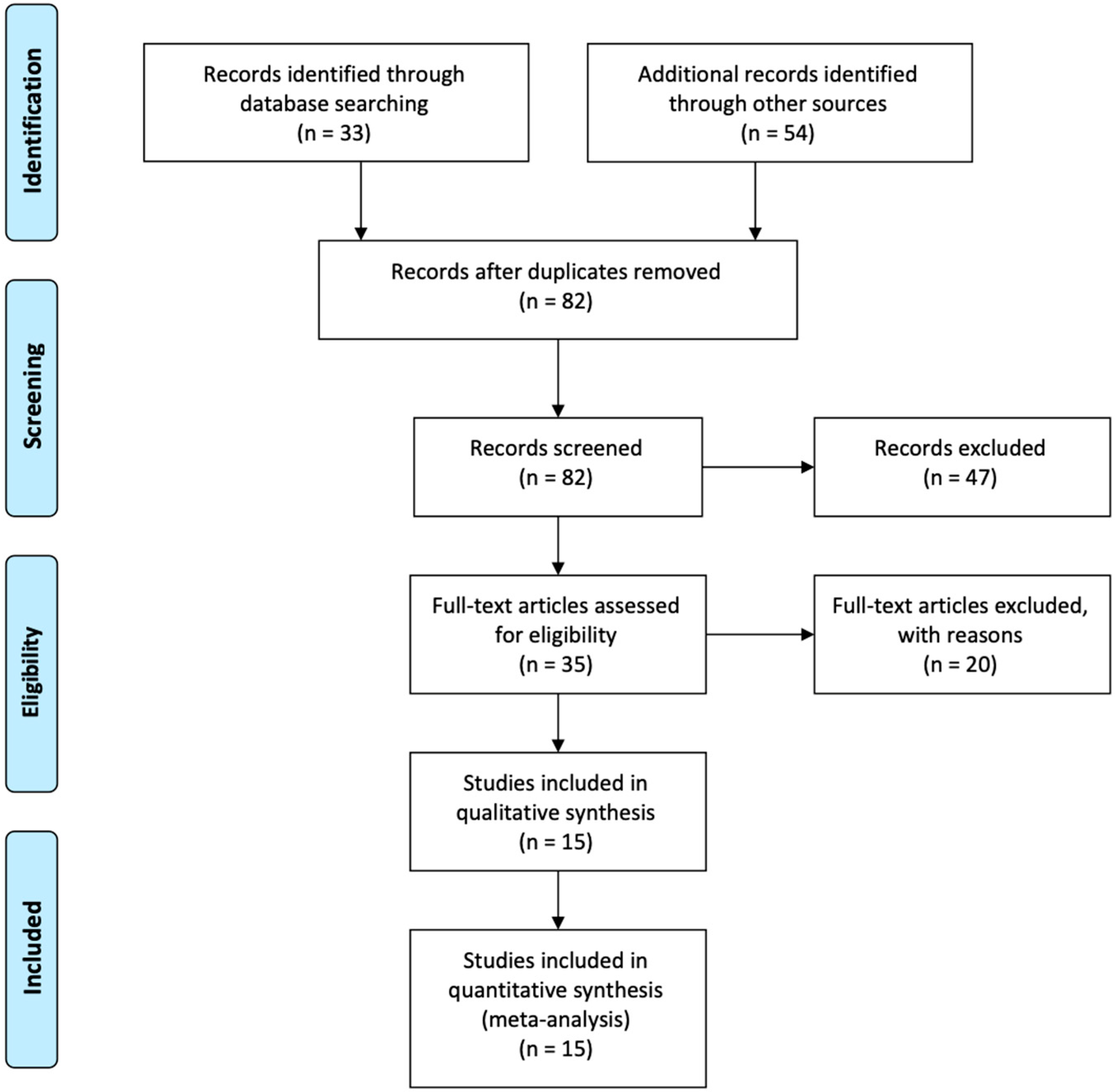
3. Results
4. Discussion
5. Conclusions
- (RQ1) How to measure the Heel-Rise Test with sensors? The use of sensors is a great challenge for the measurement of the Heel-Rise Test. We found in the literature that the most commonly used sensors were pressure sensors. Sensors may help in the measurement of the results of Heel-Rise Test, reducing the number of pieces of equipment needed for the analysis of the results. The sensors may help in the different measurements in physical therapy and medicine subjects.
- (RQ2) Which features extracted from the different sensors may support the analysis of the results of the Heel-Rise Test? Various features can be obtained from the sensors to measure the results of Heel-Rise Test. These are Heel-Rise repetitions, ankle range of motion, Heel-Rise height, Heel-Rise work, LSI, mean speed of the center-of-pressure displacements, surface area covered by the trajectory of the center-of-pressure, and weight-bearing index.
- (RQ3) How to improve the measurement of the Heel-Rise Test in the future? The analysis of the Heel-Rise Test may be enhanced with the use of automated and artificial intelligence methods for the study of the different results of this test in the treatment of various diseases in lower limbs.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Morris, M.E.; Adair, B.; Ozanne, E.; Kurowski, W.; Miller, K.J.; Pearce, A.J.; Santamaria, N.; Long, M.; Ventura, C.; Said, C.M. Smart technologies to enhance social connectedness in older people who live at home: Smart technology and social connectedness. Australas. J. Ageing 2014, 33, 142–152. [Google Scholar] [CrossRef]
- Nicholls, D.A.; Gibson, B.E. The body and physiotherapy. Physiother. Theory Pract. 2010, 26, 497–509. [Google Scholar] [CrossRef]
- Harms, M. Advancing technology in rehabilitation. Physiotherapy 2012, 98, 181–182. [Google Scholar] [CrossRef]
- Aggarwal, D.; Zhang, W.; Hoang, T.; Ploderer, B.; Vetere, F.; Bradford, M. SoPhy: A Wearable Technology for Lower Limb Assessment in Video Consultations of Physiotherapy. In Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems, Denver, CO, USA, 6–11 May 2017; pp. 3916–3928. [Google Scholar]
- Wong, W.Y.; Wong, M.S.; Lo, K.H. Clinical applications of sensors for human posture and movement analysis: A review. Prosthet. Orthot. Int. 2007, 31, 62–75. [Google Scholar] [CrossRef]
- Shany, T.; Redmond, S.J.; Narayanan, M.R.; Lovell, N.H. Sensors-Based Wearable Systems for Monitoring of Human Movement and Falls. IEEE Sens. J. 2012, 12, 658–670. [Google Scholar] [CrossRef]
- Shuangquan, W.; Jie, Y.; Ningjiang, C.; Xin, C.; Qinfeng, Z. Human Activity Recognition with User-Free Accelerometers in the Sensor Networks. In Proceedings of the 2005 International Conference on Neural Networks and Brain, Beijing, China, 13–15 October 2005; pp. 1212–1217. [Google Scholar]
- Pires, I.M.S. Aplicação Móvel e Plataforma Web Para Suporte à Estimação de Gasto Energético em Actividade Física. Master’s Thesis, University of Beira Interior, Covilhã, Portual, 2012. [Google Scholar]
- Pires, I.M.; Marques, G.; Garcia, N.M.; Flórez-Revuelta, F.; Canavarro Teixeira, M.; Zdravevski, E.; Spinsante, S.; Coimbra, M. Pattern Recognition Techniques for the Identification of Activities of Daily Living Using a Mobile Device Accelerometer. Electronics 2020, 9, 509. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, J.M.; Pires, I.M.; Marques, G.; García, N.M.; Zdravevski, E.; Lameski, P.; Flórez-Revuelta, F.; Spinsante, S.; Xu, L. Activities of Daily Living and Environment Recognition Using Mobile Devices: A Comparative Study. Electronics 2020, 9, 180. [Google Scholar] [CrossRef] [Green Version]
- Marques, D.L.; Neiva, H.P.; Pires, I.M.; Marques, M.C. The effects of high-velocity resistance training and detraining on functional and cognitive performance of institutionalised older adults. Motricidade 2019, 15, 5. [Google Scholar]
- Adusumilli, G.; Joseph, S.E.; Samaan, M.A.; Schultz, B.; Popovic, T.; Souza, R.B.; Majumdar, S. iPhone Sensors in Tracking Outcome Variables of the 30-Second Chair Stand Test and Stair Climb Test to Evaluate Disability: Cross-Sectional Pilot Study. JMIR MHealth UHealth 2017, 5, e166. [Google Scholar] [CrossRef]
- Allen, B.; Derveloy, R.; Fell, N.; Gasior, W.; Yu, G.; Sartipi, M. Telemedicine assessment of fall risk using wireless sensors. In Proceedings of the 2013 IEEE International Conference on Sensing, Communications and Networking (SECON), New Orleans, LA, USA, 24–27 June 2013; IEEE: New Orleans, LA, USA, 2013; pp. 245–247. [Google Scholar]
- Cuesta-Vargas, A.I.; Pajares, B.; Trinidad-Fernandez, M.; Alba, E.; Roldan-Jiménez, C. Inertial Sensors Embedded in Smartphones as a Tool for Fatigue Assessment Based on Acceleration in Survivors of Breast Cancer. Phys. Ther. 2020, 100, 447–456. [Google Scholar] [CrossRef]
- Majumder, S.; Deen, M.J. Smartphone Sensors for Health Monitoring and Diagnosis. Sensors 2019, 19, 2164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pires, I.; Felizardo, V.; Pombo, N.; Garcia, N.M. Limitations of energy expenditure calculation based on a mobile phone accelerometer. In Proceedings of the 2017 International Conference on High Performance Computing & Simulation (HPCS), Genoa, Italy, 17–21 July 2017. [Google Scholar]
- Pires, I.M.; Garcia, N.M.; Pombo, N.; Flórez-Revuelta, F. Limitations of the Use of Mobile Devices and Smart Environments for the Monitoring of Ageing People. In Proceedings of the HSP; SciTePress: Funchal, Madeira, Portugal, 2018. [Google Scholar]
- Jung, S.-J.; Myllylä, R.; Chung, W.-Y. Wireless Machine-to-Machine Healthcare Solution Using Android Mobile Devices in Global Networks. IEEE Sens. J. 2013, 13, 1419–1424. [Google Scholar] [CrossRef]
- Klimova, B. Acceptance and Use of Mobile Devices and Apps by Elderly People. In Challenges and Opportunities in the Digital Era; Al-Sharhan, S.A., Simintiras, A.C., Dwivedi, Y.K., Janssen, M., Mäntymäki, M., Tahat, L., Moughrabi, I., Ali, T.M., Rana, N.P., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2018; Volume 11195, pp. 30–36. ISBN 978-3-030-02130-6. [Google Scholar]
- Zdravevski, E.; Lameski, P.; Trajkovik, V.; Kulakov, A.; Chorbev, I.; Goleva, R.; Pombo, N.; Garcia, N. Improving Activity Recognition Accuracy in Ambient-Assisted Living Systems by Automated Feature Engineering. IEEE Access 2017, 5, 5262–5280. [Google Scholar] [CrossRef]
- Pires, I.M.; Andrade, M.; Garcia, N.M.; Crisóstomo, R.; Florez-Revuelta, F. Measurement of heel-rise test results using a mobile device. In Proceedings of the Doctoral Consortium—DCPhyCS (PhyCS 2015), Funchal, Madeira, Portugal, 21–24 March 2015; pp. 9–18. [Google Scholar]
- Ponciano, V.; Pires, I.M.; Ribeiro, F.R.; Garcia, N.M.; Pombo, N.; Spinsante, S.; Crisóstomo, R. Smartphone-Based automatic measurement of the results of the Timed-Up and Go test. In Proceedings of the Proceedings of the 5th EAI International Conference on Smart Objects and Technologies for Social Good, Valencia, Spain, 25–27 September 2019; pp. 239–242. [Google Scholar]
- Ponciano, V.; Pires, I.M.; Ribeiro, F.R.; Garcia, N.M.; Pombo, N. Non-Invasive measurement of results of timed-up and go test: Preliminary results. In Proceedings of the Ageing Congress, Coimbra, Portugal, 25–28 May 2019. [Google Scholar]
- Hébert-Losier, K.; Newsham-West, R.J.; Schneiders, A.G.; Sullivan, S.J. Raising the standards of the calf-raise test: A systematic review. J. Sci. Med. Sport 2009, 12, 594–602. [Google Scholar] [CrossRef] [Green Version]
- Pieper, B.; Templin, T.N.; Birk, T.J.; Kirsner, R.S. The standing heel-rise test: Relation to chronic venous disorders and balance, gait, and walk time in injection drug users. Ostomy. Wound Manage 2008, 54, 18–22, 24, 26–30 passim. [Google Scholar]
- Zdravevski, E.; Lameski, P.; Trajkovik, V.; Chorbev, I.; Goleva, R.; Pombo, N.; Garcia, N.M. Automation in Systematic, Scoping and Rapid Reviews by an NLP Toolkit: A Case Study in Enhanced Living Environments. In Enhanced Living Environments; Ganchev, I., Garcia, N.M., Dobre, C., Mavromoustakis, C.X., Goleva, R., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2019; Volume 11369, pp. 1–18. ISBN 978-3-030-10751-2. [Google Scholar]
- Bayer, M.L.; Hoegberget-Kalisz, M.; Jensen, M.H.; Olesen, J.L.; Svensson, R.B.; Couppé, C.; Boesen, M.; Nybing, J.D.; Kurt, E.Y.; Magnusson, S.P.; et al. Role of tissue perfusion, muscle strength recovery, and pain in rehabilitation after acute muscle strain injury: A randomized controlled trial comparing early and delayed rehabilitation. Scand. J. Med. Sci. Sports 2018, 28, 2579–2591. [Google Scholar] [CrossRef]
- Eliasson, P.; Agergaard, A.-S.; Couppé, C.; Svensson, R.; Hoeffner, R.; Warming, S.; Warming, N.; Holm, C.; Jensen, M.H.; Krogsgaard, M.; et al. The Ruptured Achilles Tendon Elongates for 6 Months after Surgical Repair Regardless of Early or Late Weightbearing in Combination with Ankle Mobilization: A Randomized Clinical Trial. Am. J. Sports Med. 2018, 46, 2492–2502. [Google Scholar] [CrossRef]
- Byrne, C.; Keene, D.J.; Lamb, S.E.; Willett, K. Intrarater reliability and agreement of linear encoder derived heel-rise endurance test outcome measures in healthy adults. J. Electromyogr. Kinesiol. Off. J. Int. Soc. Electrophysiol. Kinesiol. 2017, 36, 34–39. [Google Scholar] [CrossRef] [Green Version]
- Brorsson, A.; Olsson, N.; Nilsson-Helander, K.; Karlsson, J.; Eriksson, B.I.; Silbernagel, K.G. Recovery of calf muscle endurance 3 months after an Achilles tendon rupture: Evaluation of standardized seated heel-rises. Scand. J. Med. Sci. Sports 2016, 26, 844–853. [Google Scholar] [CrossRef]
- Nawoczenski, D.A.; DiLiberto, F.E.; Cantor, M.S.; Tome, J.M.; DiGiovanni, B.F. Ankle Power and Endurance Outcomes Following Isolated Gastrocnemius Recession for Achilles Tendinopathy. Foot Ankle Int. 2016, 37, 766–775. [Google Scholar] [CrossRef]
- Tengman, T.; Coleman, S.; Grävare Silbernagel, K.; Karlsson, J.; Riad, J. Muscle fatigue after Achilles tendon rupture: A limited heel-rise test with electromyography reveals decreased endurance. Eur. J. Physiother. 2015, 17, 200–207. [Google Scholar] [CrossRef]
- Olsson, N.; Petzold, M.; Brorsson, A.; Karlsson, J.; Eriksson, B.I.; Grävare Silbernagel, K. Predictors of Clinical Outcome after Acute Achilles Tendon Ruptures. Am. J. Sports Med. 2014, 42, 1448–1455. [Google Scholar] [CrossRef] [PubMed]
- Neville, C.; Flemister, A.S.; Houck, J. Total and Distributed Plantar Loading in Subjects with Stage II Tibialis Posterior Tendon Dysfunction during Terminal Stance. Foot Ankle Int. 2013, 34, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Robbins, D.; Goss-Sampson, M. The influence of whole body vibration on the plantarflexors during heel raise exercise. J. Electromyogr. Kinesiol. 2013, 23, 614–618. [Google Scholar] [CrossRef]
- Bicici, S.; Karatas, N.; Baltaci, G. Effect of athletic taping and kinesiotaping® on measurements of functional performance in basketball players with chronic inversion ankle sprains. Int. J. Sports Phys. Ther. 2012, 7, 154–166. [Google Scholar]
- Silbernagel, K.G.; Steele, R.; Manal, K. Deficits in heel-rise height and achilles tendon elongation occur in patients recovering from an Achilles tendon rupture. Am. J. Sports Med. 2012, 40, 1564–1571. [Google Scholar] [CrossRef]
- Olsson, N.; Nilsson-Helander, K.; Karlsson, J.; Eriksson, B.I.; Thomée, R.; Faxén, E.; Silbernagel, K.G. Major functional deficits persist 2 years after acute Achilles tendon rupture. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 1385–1393. [Google Scholar] [CrossRef] [PubMed]
- Nilsson-Helander, K.; Silbernagel, K.G.; Thomeé, R.; Faxén, E.; Olsson, N.; Eriksson, B.I.; Karlsson, J. Acute achilles tendon rupture: A randomized, controlled study comparing surgical and nonsurgical treatments using validated outcome measures. Am. J. Sports Med. 2010, 38, 2186–2193. [Google Scholar] [CrossRef]
- Silbernagel, K.G.; Nilsson-Helander, K.; Thomeé, R.; Eriksson, B.I.; Karlsson, J. A new measurement of heel-rise endurance with the ability to detect functional deficits in patients with Achilles tendon rupture. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 258–264. [Google Scholar] [CrossRef]
- Vuillerme, N.; Boisgontier, M. Changes in the relative contribution of each leg to the control of quiet two-legged stance following unilateral plantar–flexor muscles fatigue. Eur. J. Appl. Physiol. 2010, 110, 207–213. [Google Scholar] [CrossRef]
- Gaasvaer, J.I.; Bahr, R. The musclelab®—A new method for the evaluation of dynamic muscle action. Med. Sci. Sports Exerc. 1999, 31, S280. [Google Scholar] [CrossRef]
- Steele, R. Social media, mobile devices and sensors: Categorizing new techniques for health communication. In Proceedings of the 2011 Fifth International Conference on Sensing Technology, Palmerston North, New Zealand, 28 Noverber–1 December 2011; pp. 187–192. [Google Scholar]
- Pires, I.M.; Marques, G.; Garcia, N.M.; Pombo, N.; Flórez-Revuelta, F.; Spinsante, S.; Teixeira, M.C.; Zdravevski, E. Recognition of Activities of Daily Living and Environments Using Acoustic Sensors Embedded on Mobile Devices. Electronics 2019, 8, 1499. [Google Scholar] [CrossRef] [Green Version]
- Piper, A.M.; Garcia, R.C.; Brewer, R.N. Understanding the Challenges and Opportunities of Smart Mobile Devices among the Oldest Old. Int. J. Mob. Hum. Comput. Interact. 2016, 8, 83–98. [Google Scholar] [CrossRef] [Green Version]
- Lunsford, B.R.; Perry, J. The Standing Heel-Rise Test for Ankle Plantar Flexion: Criterion for Normal. Phys. Ther. 1995, 75, 694–698. [Google Scholar] [CrossRef] [PubMed]
- Hébert-Losier, K.; Schneiders, A.G.; Newsham-West, R.J.; Sullivan, S.J. Scientific bases and clinical utilisation of the calf-raise test. Phys. Ther. Sport 2009, 10, 142–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segura-Ortí, E.; Martínez-Olmos, F.J. Test-Retest Reliability and Minimal Detectable Change Scores for Sit-to-Stand-to-Sit Tests, the Six-Minute Walk Test, the One-Leg Heel-Rise Test, and Handgrip Strength in People Undergoing Hemodialysis. Phys. Ther. 2011, 91, 1244–1252. [Google Scholar] [CrossRef] [Green Version]
- Felizardo, V.; Sousa, P.; Sabugueiro, D.; Alexandre, C.; Couto, R.; Garcia, N.; Pires, I. E-Health: Current status and future trends. In Handbook of Research on Democratic Strategies and Citizen-Centered E-Government Services; IGI Global: Hershey, PA, USA, 2015; pp. 302–326. [Google Scholar]
- Ponciano, V.; Pires, I.M.; Ribeiro, F.R.; Marques, G.; Garcia, N.M.; Pombo, N.; Spinsante, S.; Zdravevski, E. Is the Timed-up and Go Test Feasible in Mobile Devices? A Systematic Review. Electronics 2020, 9, 528. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Study | Year of Publication | Location | Population | Purpose | Sensors Used | Diseases |
|---|---|---|---|---|---|---|
| Bayer et al. [27] | 2018 | Denmark | 50 patients with unknown age | Examination of the relation between tissue perfusion and morphological changes of the muscle | MuscleLab measurement system | hamstring injuries, calf injuries, and quadriceps injuries |
| Eliasson et al. [28] | 2018 | Denmark | 75 patients aged between 18 and 65 years old | Examination of whether tendon elongation, mechanical properties, and functional outcomes during rehabilitation | MuscleLab measurement system | Achilles tendon ruptures |
| Byrne et al. [29] | 2017 | United Kingdom | 38 participants aged between 27 and 45 years old | Comparison of the intrarater test–retest reliability and measurement agreement with standard device | MuscleLab measurement system | Healthy people |
| Brorsson et al. [30] | 2016 | Sweden | 101 patients aged between 18 and 65 years old | Evaluation of the ability to perform standardized seated Heel-Rises after an Achilles tendon rupture | MuscleLab measurement system | Achilles tendon ruptures |
| Nawoczenski et al. [31] | 2016 | Unites States of America | 14 patients with unknown age | Determination of the effect of an isolated gastrocnemius recession procedure on ankle power and endurance | Flock of Bird 6 degree of freedom electromagnetic sensor motion capture system | Achilles tendinopathy |
| Tengman et al. [32] | 2015 | Sweden | 52 participants aged between 37 and 58 years old | Evaluation of muscle fatigue | Electromyography | Achilles tendon ruptures |
| Olsson et al. [33] | 2014 | Sweden | 93 individuals with mean age of 40 years old | Study of the symptoms maximum Heel-Rise height for function | Linear encoder | Achilles tendon ruptures |
| Neville et al. [34] | 2013 | Unites States of America | 30 subjects with unknown age | Comparison of total and distributed loading patterns in subjects with stage II Tibialis Posterior Tendon Dysfunction | Capacitive sensors | Stage II tibialis posterior tendon dysfunction |
| Robbins et al. [35] | 2013 | United Kingdom | 10 male subjects aged between 22 and 32 years old | Determination of whole-body vibration on the myoelectrical activity of selected plantar flexors | Power Plate pro | Healthy people |
| Bicici et al. [36] | 2012 | Turkey | 15 male subjects aged between 18 and 22 years old | Evaluation of functional performance in athletes | Tilt sensors | Chronic inversion ankle sprains |
| Silbernagel et al. [37] | 2012 | Unites States of America | 18 participants aged between 20 and 59 years old | Evaluation of side-to-side differences in maximal Heel-Rise height | Linear encoder | Achilles tendon ruptures |
| Olsson et al. [38] | 2011 | Sweden | 81 individuals with unknown age | Evaluation of the results after an acute Achilles tendon rupture | MuscleLab measurement system | Achilles tendon ruptures |
| Nilsson-Helander et al. [39] | 2010 | Sweden | 97 individuals with mean age of 41 years old | Comparison of outcomes between patients | MuscleLab measurement system | Achilles tendon ruptures |
| Silbernagel et al. [40] | 2010 | Sweden | 78 subjects aged between 33 and 51 years old | Evaluation of the validity and ability to detect differences in outcome of a Heel-Rise work test | MuscleLab measurement system | Achilles tendon ruptures |
| Vuillerme et al. [41] | 2010 | France | 18 healthy male adults aged between 24 and 28 years old | Assessment of the capacity of the central nervous system | Pressure sensors | Healthy people |
| Features | Number of Studies | Studies |
|---|---|---|
| Heel-Rise height | 10 | [27,28,29,30,32,33,37,38,39,40] |
| Heel-Rise repetitions | 7 | [27,30,32,36,37,38,40] |
| Heel-Rise work | 3 | [38,39,40] |
| Limb symmetry index (LSI) | 3 | [31,38,40] |
| Ankle range of motion | 2 | [38,40] |
| Concentric power | 1 | [39] |
| Drop countermovement jump (CMJ) | 1 | [39] |
| Eccentric power | 1 | [39] |
| Electromyography (EMG) amplitude | 1 | [35] |
| Forefoot abduction/adduction | 1 | [34] |
| Frequency analysis | 1 | [35] |
| Heel-Rise index | 1 | [28] |
| Hindfoot inversion/eversion | 1 | [34] |
| Hopping | 1 | [39] |
| Mean speed of the centre-of-pressure displacements | 1 | [41] |
| Medial longitudinal arch (MLA) height | 1 | [34] |
| Muscle isokinetic strength of the thigh muscles | 1 | [27] |
| Muscle isometric strength | 1 | [27] |
| Muscle volume | 1 | [27] |
| Plantar flexion strength 0° | 1 | [28] |
| Plantar flexion strength 12° | 1 | [28] |
| Range of motion | 1 | [28] |
| Surface area covered by the trajectory of the center-of-pressure | 1 | [41] |
| Timing of EMG activity | 1 | [35] |
| Weight-bearing index | 1 | [41] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pires, I.M.; Ponciano, V.; Garcia, N.M.; Zdravevski, E. Analysis of the Results of Heel-Rise Test with Sensors: A Systematic Review. Electronics 2020, 9, 1154. https://doi.org/10.3390/electronics9071154
Pires IM, Ponciano V, Garcia NM, Zdravevski E. Analysis of the Results of Heel-Rise Test with Sensors: A Systematic Review. Electronics. 2020; 9(7):1154. https://doi.org/10.3390/electronics9071154
Chicago/Turabian StylePires, Ivan Miguel, Vasco Ponciano, Nuno M. Garcia, and Eftim Zdravevski. 2020. "Analysis of the Results of Heel-Rise Test with Sensors: A Systematic Review" Electronics 9, no. 7: 1154. https://doi.org/10.3390/electronics9071154