Measurement of Results of Functional Reach Test with Sensors: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Questions
2.2. Inclusion Criteria
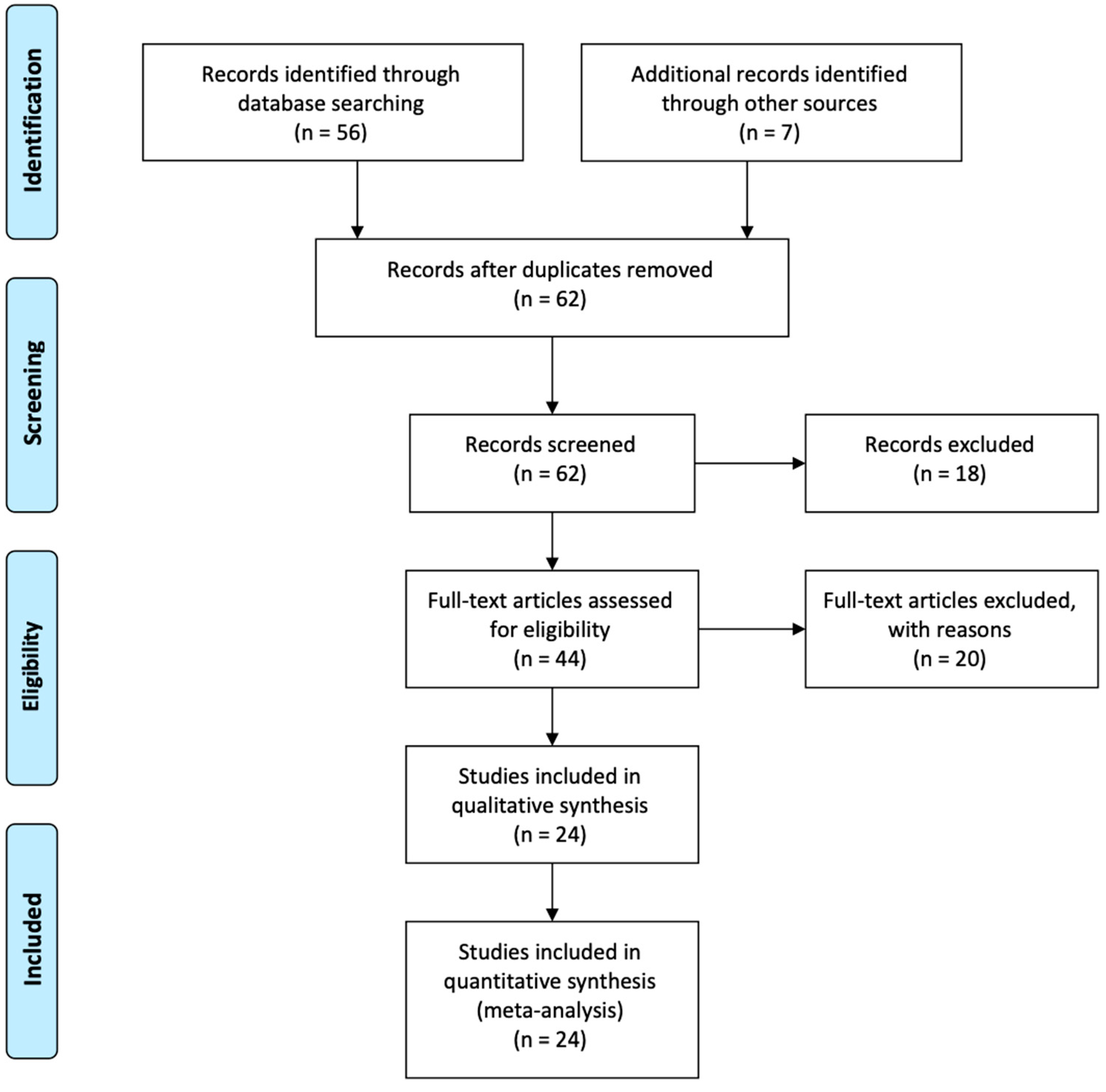
2.3. Search Strategy
2.4. Extraction of Study Characteristics
3. Results
3.1. Healthy People
3.2. Stroke Disease
3.3. Other Diseases
4. Discussion
5. Conclusions
- (RQ1)
- How can sensors improve the measurement of the Functional Reach Test results? The use of embedded sensors in mobile devices is very convenient because it allows patients to autonomously perform the Functional Reach Test without the presence of a healthcare professional. The sensors are starting to be used in physiotherapy and medicine subjects widely. The data collected from the different sensors may allow the creation of accurate methods for the measurement of the results of this test. The main concern is that the accuracy often was not reported in the analyzed studies. However, the correlation coefficient in the different studies analyzed, when presented, shows high correlation values except for one study. More research is needed to measure different variables and increase the results;
- (RQ2)
- Which features extracted from the different sensors may be used in the analysis of the Functional Reach Test? The most used features for the analysis of the results of the Functional Reach Test are mean speed, mean acceleration, distance, and different angles. However, the reliability can be evaluated with the correlation coefficient, verifying that the correlation with other instruments is commonly high for the different methods for the calculation and analysis of the different features;
- (RQ3)
- How are sensors combined with the Functional Reach Test to allow improvements in the assessment of stroke patients? The combination of the Functional Reach Test with sensors allows the constant and autonomous monitoring of the state of stroke patients. It also enables the development of new technological systems for the remote control of people. Thus, ten studies are related to the treatment and recovery of different types of strokes, to the presence of strokes, and to the post-stroke treatment with the Functional Reach Test.
- (RQ4)
- What are the limitations on the use of sensors in this type of study? There are different limitations on the use of sensors related to the accuracy and reliability of the sensors, but other challenges are related to the different diseases and capabilities of people. The positioning of the sensors is another limitation that can influence the data acquisition. However, the use of inertial sensors is expected to be more convenient than the use of traditional methods with medical personnel using rulers and measuring tapes because the measurements could be performed at real time, even at the expense of somewhat lower accuracy.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Population Structure and Ageing—Statistics Explained. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php/Population_structure_and_ageing (accessed on 17 May 2020).
- Istance, D. Education at OECD: Recent themes and recommendations. Eur. J. Educ. 2011, 46, 87–100. [Google Scholar] [CrossRef]
- Sidik, S.M.; Rampal, L.; Afifi, M. Physical and mental health problems of the elderly in a rural community of Sepang, Selangor. Malays. J. Med. Sci. 2004, 11, 52–59. [Google Scholar]
- Garcia, N.M. A roadmap to the design of a personal digital life coach. In Advances in Intelligent Systems and Computing; AISC: Chicago, IL, USA, 2015. [Google Scholar]
- Goleva, R.I.; Ganchev, I.; Dobre, C.; Garcia, N.; Valderrama, C. Enhanced Living Environments: From Models to Technologies; IET: London, UK, 2017. [Google Scholar]
- Garcia, N.M.; Rodrigues, J.J.P.C. Ambient Assisted Living; CRC Press: Boca Raton, FL, USA, 2015; ISBN 9781439869857. [Google Scholar]
- Pires, I.M.; Garcia, N.M.; Pombo, N.; Flórez-Revuelta, F. Identification of activities of daily living using sensors available in off-the-shelf mobile devices: Research and hypothesis. In Advances in Intelligent Systems and Computing; AISC: Chicago, IL, USA, 2016. [Google Scholar]
- Banerjee, A.; Nikumb, V.; Thakur, R. Health Problems among the Elderly: A Cross-Sectional Study. Ann. Med. Health Sci. Res. 2013, 3, 19. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.-H. Physical Health Status, Depression and Activities of Daily Living of the Low-income Elderly Living Alone in Metropolitan Areas. J. Korean Acad. Community Health Nurs. 2005, 16, 137–147. [Google Scholar]
- Gupta, H.L.; Yadav, M.; Sundarka, M.K.; Talwar, V.; Saini, M.; Garg, P. A study of prevalence of health problems in asymptomatic elderly individuals in Delhi. J. Assoc. Physicians India 2002, 50, 792–795. [Google Scholar]
- Benedetti, T.R.B.; Borges, L.J.; Petroski, E.L.; Gonçalves, L.H.T. Atividade física e estado de saúde mental de idosos. Rev. De Saude Publica 2008, 42, 302–307. [Google Scholar] [CrossRef] [Green Version]
- Morita, M.; Takamura, N.; Kusano, Y.; Abe, Y.; Moji, K.; Takemoto, T.I.; Aoyagi, K. Relationship between falls and physical performance measures among community-dwelling elderly women in Japan. Aging Clin. Exp. Res. 2005, 17, 211–216. [Google Scholar] [CrossRef]
- Duncan, P.W.; Weiner, D.K.; Chandler, J.; Studenski, S. Functional reach: A new clinical measure of balance. J. Gerontol. 1990, 45. [Google Scholar] [CrossRef]
- Maranesi, E.; Ghetti, G.; Rabini, R.A.; Fioretti, S. Functional reach test: Movement strategies in diabetic subjects. Gait Posture 2014, 39, 501–505. [Google Scholar] [CrossRef]
- Weiner, D.K.; Duncan, P.W.; Chandler, J.; Studenski, S.A. Functional Reach: A Marker of Physical Frailty. J. Am. Geriatr. Soc. 1992, 40, 203–207. [Google Scholar] [CrossRef]
- Pires, I.M.; Marques, G.; Garcia, N.M.; Pombo, N.; Flórez-Revuelta, F.; Spinsante, S.; Teixeira, M.C.; Zdravevski, E. Recognition of Activities of Daily Living and Environments Using Acoustic Sensors Embedded on Mobile Devices. Electronics 2019, 8, 1499. [Google Scholar] [CrossRef] [Green Version]
- Pires, I.M.; Garcia, N.M.; Pombo, N.; Flórez-Revuelta, F.; Spinsante, S.; Teixeira, M.C. Identification of activities of daily living through data fusion on motion and magnetic sensors embedded on mobile devices. Pervasive Mob. Comput. 2018. [Google Scholar] [CrossRef]
- Pires, I.M.; Teixeira, M.C.; Pombo, N.; Garcia, N.M.; Flórez-Revuelta, F.; Spinsante, S.; Goleva, R.; Zdravevski, E. Android Library for Recognition of Activities of Daily Living: Implementation Considerations, Challenges, and Solutions. Open Bioinform. J. 2018. [Google Scholar] [CrossRef] [Green Version]
- Pires, I.M.; Garcia, N.M.; Pombo, N.; Flórez-Revuelta, F.; Spinsante, S. Approach for the development of a framework for the identification of Activities of Daily Living using sensors in mobile devices. Sensors 2018, 18, 640. [Google Scholar] [CrossRef] [Green Version]
- Ponciano, V.; Pires, I.M.; Ribeiro, F.R.; Garcia, N.M.; Pombo, N.; Spinsante, S.; Crisóstomo, R. Smartphone-based automatic measurement of the results of the Timed-Up and Go test. In Proceedings of the 5th EAI International Conference on Smart Objects and Technologies for Social Good, Valencia, Spain, 25–27 September 2019. [Google Scholar]
- Pires, I.M.; Garcia, N.M.; Teixeira, M.C.C. Calculation of jump flight time using a mobile device. In Proceedings of the HEALTHINF 2015—8th International Conference on Health Informatics, Part of 8th International Joint Conference on Biomedical Engineering Systems and Technologies, BIOSTEC 2015, Lisbon, Portugal, 12–15 January 2015. [Google Scholar]
- Pires, I.M.; Felizardo, V.; Pombo, N.; Drobics, M.; Garcia, N.M.; Flórez-Revuelta, F. Validation of a method for the estimation of energy expenditure during physical activity using a mobile device accelerometer. J. Ambient Intell. Smart Environ. 2018. [Google Scholar] [CrossRef]
- Pires, I.M.; Andrade, M.; Garcia, N.M.; Crisóstomo, R.; Florez-Revuelta, F. Measurement of Heel-Rise Test Results using a Mobile Device. In Proceedings of the Doctoral Consortium—DCPhyCS, (PhyCS 2015), Angers, France, 11–13 February 2015; SciTePress: Setúbal, Portugal, 2015; pp. 9–18. [Google Scholar]
- Ponciano, V.; Pires, I.M.; Ribeiro, F.R.; Marques, G.; Garcia, N.M.; Pombo, N.; Spinsante, S.; Zdravevski, E. Is The Timed-Up and Go Test Feasible in Mobile Devices? A Systematic Review. Electronics 2020, 9, 528. [Google Scholar] [CrossRef] [Green Version]
- Pires, I.; Felizardo, V.; Pombo, N.; Garcia, N.M. Limitations of energy expenditure calculation based on a mobile phone accelerometer. In Proceedings of the 2017 International Conference on High Performance Computing and Simulation, HPCS, Genoa, Italy, 17–21 July 2017. [Google Scholar]
- Pires, I.M.; Garcia, N.M.; Pombo, N.; Flórez-Revuelta, F. Limitations of the use of mobile devices and smart environments for the monitoring of ageing people. In Proceedings of the ICT4AWE 2018—Proceedings of the 4th International Conference on Information and Communication Technologies for Ageing Well and e-Health, Funchal, Portugal, 22–23 March 2018. [Google Scholar]
- Zdravevski, E.; Lameski, P.; Trajkovik, V.; Chorbev, I.; Goleva, R.; Pombo, N.; Garcia, N.M. Automation in Systematic, Scoping and Rapid Reviews by an NLP Toolkit: A Case Study in Enhanced Living Environments BT—Enhanced Living Environments: Algorithms, Architectures, Platforms, and Systems. In Enhanced Living Environments; Ganchev, I., Garcia, N.M., Dobre, C., Mavromoustakis, C.X., Goleva, R., Eds.; Springer International Publishing: Cham, Germany, 2019; pp. 1–18. ISBN 978-3-030-10752-9. [Google Scholar]
- Fell, N.; True, H.H.; Allen, B.; Harris, A.; Cho, J.; Hu, Z.; Sartipi, M.; Place, K.K.; Salstrand, R. Functional measurement post-stroke via mobile application and body-worn sensor technology. mHealth 2019, 5, 47. [Google Scholar] [CrossRef] [PubMed]
- Mengarelli, A.; Cardarelli, S.; Strazza, A.; Di Nardo, F.; Fioretti, S.; Verdini, F. Validity of the Nintendo Wii Balance Board for the Assessment of Balance Measures in the Functional Reach Test. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1400–1406. [Google Scholar] [CrossRef] [PubMed]
- Arai, T.; Obuchi, S.; Shiba, Y. A novel clinical evaluation method using maximum angular velocity during knee extension to assess lower extremity muscle function of older adults. Arch. Gerontol. Geriatr. 2017, 73, 143–147. [Google Scholar] [CrossRef]
- D’Anna, C.; Scorza, A.; Schmid, M.; Orsini, F.; Andrea Sciuto, S.; Conforto, S.; Scena, S. A preliminary study on the validation of anautomatic measurement method for functional reach assessment by stereophotogrammetry. In Proceedings of the 2017 IEEE International Instrumentation and Measurement Technology Conference (I2MTC), Turin, Italy, 22–25 May 2017; IEEE: Torino, Italy, 2017; pp. 1–5. [Google Scholar]
- Williams, B.; Allen, B.; Hu, Z.; True, H.; Cho, J.; Harris, A.; Fell, N.; Sartipi, M. Real-time fall risk assessment using functional reach test. Int. J. Telemed. Appl. 2017, 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, A.; True, H.; Hu, Z.; Cho, J.; Fell, N.; Sartipi, M. Fall recognition using wearable technologies and machine learning algorithms. In Proceedings of the 2016 IEEE International Conference on Big Data (Big Data), Washington, DC, USA, 5–8 December 2016; pp. 3974–3976. [Google Scholar]
- Lin, C.C.; Chen, C.C.; Lin, P.S.; Lee, R.G.; Huang, J.S.; Tsai, T.H.; Chang, Y.C. Development of Home-Based Frailty Detection Device Using Wireless Sensor Networks. J. Med. Biol. Eng. 2016, 36, 168–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz-Muñoz, M.; González-Sánchez, M.; Cuesta-Vargas, A.I. Foot Dorsiflexion Velocity and Torque Variance Explained through Architectural and Electromyography Variables Comparing Elders and Stroke Survivors. J. Stroke Cerebrovasc. Dis. 2016, 25, 2295–2304. [Google Scholar] [CrossRef]
- Scena, S.; Steindler, R.; Ceci, M.; Zuccaro, S.M.; Carmeli, E. Computerized Functional Reach Test to Measure Balance Stability in Elderly Patients with Neurological Disorders. J. Clin Med. Res. 2016, 8, 715–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merchán-Baeza, J.A.; González-Sánchez, M.; Cuesta-Vargas, A. Mobile Functional Reach Test in People Who Suffer Stroke: A Pilot Study. Jmir Rehabil. Assist. Technol. 2015, 2, e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merchán-Baeza, J.A.; González-Sánchez, M.; Cuesta-Vargas, A.I. Comparison of kinematic variables obtained by inertial sensors among stroke survivors and healthy older adults in the Functional Reach Test: Cross-sectional study. Biomed. Eng. Online 2015, 14, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Carmeli, E.; Katz-Laurer, M.; Scena, S.; Kodesh, E.; Steindler, R. Functional reach test performance in distance and velocity—A pilot study. Eur. J. Physiother. 2014, 16, 168–172. [Google Scholar] [CrossRef]
- Merchán-Baeza, J.A.; González-Sánchez, M.; Cuesta-Vargas, A.I. Reliability in the parameterization of the functional reach test in elderly stroke patients: A pilot study. Biomed. Res. Int. 2014, 2014, 8–11. [Google Scholar] [CrossRef] [Green Version]
- Van den Heuvel, M.R.C.; Kwakkel, G.; Beek, P.J.; Berendse, H.W.; Daffertshofer, A.; van Wegen, E.E.H. Effects of augmented visual feedback during balance training in Parkinson’s disease: A pilot randomized clinical trial. Parkinsonism Relat. Disord. 2014, 20, 1352–1358. [Google Scholar] [CrossRef] [Green Version]
- Yalla, S.V.; Crews, R.T.; Fleischer, A.E.; Grewal, G.; Ortiz, J.; Najafi, B. An immediate effect of custom-made ankle foot orthoses on postural stability in older adults. Clin. Biomech. 2014, 29, 1081–1088. [Google Scholar] [CrossRef] [Green Version]
- Allen, B.; Derveloy, R.; Lowry, K.; Handley, H.; Fell, N.; Gasior, W.; Yu, G.; Sartipi, M. Evaluation of fall risk for post-stroke patients using bluetooth low-energy wireless sensor. In Proceedings of the 2013 IEEE Global Communications Conference (GLOBECOM), Atlanta, GA, USA, 9–13 December 2013; pp. 2598–2603. [Google Scholar] [CrossRef]
- Allen, B.; Derveloy, R.; Fell, N.; Gasior, W.; Yu, G.; Sartipi, M. Telemedicine assessment of fall risk using wireless sensors. In Proceedings of the 2013 IEEE International Conference on Sensing, Communications and Networking, SECON 2013, New Orleans, LA, USA, 24–27 June 2013; pp. 245–247. [Google Scholar] [CrossRef]
- Shin, S.; Sosnoff, J.J. Spinal cord injury and time to instability in seated posture. Arch. Phys. Med. Rehabil. 2013, 94, 1615–1620. [Google Scholar] [CrossRef]
- Itoh, T.; Kumagai, Y.; Morioka, I.; Mae, S.; Naka, T.; Uenishi, H.; Matsuoka, T. Development of a new instrument for evaluating leg motions using acceleration sensors (II). Environ. Health Prev. Med. 2012, 17, 205–212. [Google Scholar] [CrossRef] [Green Version]
- Pertille, A.; MacEdo, A.B.; Dibai Filho, A.V.; Rêgo, E.M.; Arrais, L.D.D.F.; Negri, J.R.; Teodori, R.M.H. Immediate effects of bilateral grade III mobilization of the talocrural joint on the balance of elderly women. J. Manip. Physiol. Ther. 2012, 35, 549–555. [Google Scholar] [CrossRef]
- Rajaratnam, B.S.; Tim, X.T.M.; Elsa, A.Y.H.; Ng, K.H.; Su, Y.; Wilson, W.Y.H.; Teo, S.T.S. Wii-rehab to enhance balance among patients with stroke. In i-CREATe 2011—International Convention on Rehabilitation Engineering and Assistive Technology; ACM: New York, NY, USA, 2011; pp. 258–260. [Google Scholar]
- Yamada, M.; Aoyama, T.; Nakamura, M.; Tanaka, B.; Nagai, K.; Tatematsu, N.; Uemura, K.; Nakamura, T.; Tsuboyama, T.; Ichihashi, N. The Reliability and Preliminary Validity of Game-Based Fall Risk Assessment in Community-Dwelling Older Adults. Geriatr. Nurs. 2011, 32, 188–194. [Google Scholar] [CrossRef]
- Costarella, M.; Monteleone, L.; Steindler, R.; Zuccaro, S.M. Decline of physical and cognitive conditions in the elderly measured through the functional reach test and the mini-mental state examination. Arch. Gerontol. Geriatr. 2010, 50, 332–337. [Google Scholar] [CrossRef]
- Katz-Leurer, M.; Fisher, I.; Neeb, M.; Schwartz, I.; Carmeli, E. Reliability and validity of the modified functional reach test at the sub-acute stage post-stroke. Disabil. Rehabil. 2009, 31, 243–248. [Google Scholar] [CrossRef]
- Batista, D.; Silva, H.; Fred, A. Experimental characterization and analysis of the BITalino platforms against a reference device. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Seogwipo, Korea, 11–15 July 2017; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2017; pp. 2418–2421. [Google Scholar]



{kind=link}
{kind=link}
| Study: | Health Problem: | Average of the Percentage of Population: | Number of Studies: |
|---|---|---|---|
| [8,9,10] | Cardiac problems | 29.2% | 3 |
| [3,9,11] | Cognitive impairment | 16.0% | 3 |
| [8,10] | Visual impairment | 45.4% | 2 |
| [3,11] | Depression | 13.7% | 2 |
| [11] | Sedentary | 93.5% | 1 |
| [3] | Chronic physical illness | 60.1% | 1 |
| [8] | Tobacco | 58.97% | 1 |
| [8] | Dental problems | 32.6% | 1 |
| [9] | Arthritis | 26.5% | 1 |
| [10] | Proteinuria | 22.2% | 1 |
| [12] | Falling prevalence | 21.1% | 1 |
| [10] | Pulmonary tuberculosis | 16% | 1 |
| [3] | Functional dependence | 15.7% | 1 |
| [8] | Diabetes | 12% | 1 |
| [10] | Glycosuria | 7.6% | 1 |
| [10] | Asthma | 4.5% | 1 |
| [10] | Urinary tract infection | 1.5% | 1 |
| Study | Year of Publication | Population | Purpose | Sensors Used | Diseases |
|---|---|---|---|---|---|
| Fell et al. [28] | 2019 | 35 patients (21 males, and 14 female) | Mobile health system for a support management system for patients with exercise plans or clinical measurement tools for healthcare providers | Accelerometer, gyroscope, and magnetometer | Stroke |
| Mengarelli et al. [29] | 2018 | 48 subjects aged between 21 and 26 years old | Comparison of the center of pressure data | Force sensors in Nintendo Wii Balance Board | Healthy patients |
| Arai et al. [30] | 2017 | 204 older adults aged between 73 and 85 years old | Examination of the utilities of maximum angular velocity assessment during knee extension | Gyroscope | Healthy patients |
| D’Anna et al. [31] | 2017 | 4 male subjects aged between 27 and 40 years old | Assessment of the validity of a measurement method for Functional Reach Test implementation | Cameras | Healthy patients |
| Williams et al. [32] | 2017 | 23 individuals (15 females and eight males) with an average age of 25.3 years old | Monitoring of the fall risk with Functional Reach Test | Accelerometer, gyroscope, and magnetometer | Stroke |
| Harris et al. [33] | 2016 | 14 subjects (7 males and seven females) aged between 22 to 50 years old | Measurement of fall risk | Gyroscope, and accelerometer | Stroke |
| Lin et al. [34] | 2016 | 309 individuals (178 females and 131 males) aged over 65 years old | Monitoring of the impact of the aging of elderly people | Pressure sensor | Healthy patients |
| Ruiz-Muñoz et al. [35] | 2016 | 28 participants (14 stroke survivors and 14 healthy) subjects) over 65 years old | Analysis of the relationship between electromyographic variables, tibialis anterior architecture, and functional variables during maximal isometric and isotonic foot dorsiflexion | Accelerometer and electromyography sensors | Balance impairment |
| Scena et al. [36] | 2016 | 80 patients, where 38 are males, and 42 are females | Measurement of distance, velocity, time length, arm direction and girdles translation during Functional Reach Test | Cameras | Neurological disorders |
| Merchán-Baeza et al. [37] | 2015 | Seven subjects over 65 years old | Analysis of the reliability in the Functional Reach Test parameters with mobile sensors | Accelerometer, gyroscope, and magnetometer | Stroke |
| Merchán-Baeza et al. [38] | 2015 | Ten subjects (6 females and four males) aged between 68 and 77 years old | Comparison of kinematic variables and analysis of the reliability of the kinematic measurements | Accelerometer | Stroke |
| Carmeli et al. [39] | 2014 | 73 subjects aged between 20 and 95 years old | Description of the difference in Functional Reach Test distance and velocity during different velocities, and description of the age-related differences associated distance and velocity | Cameras | Healthy patients |
| Merchán-Baeza et al. [40] | 2014 | 4 participants aged between 69 and 92 years old | Analysis of the reliability, sensitivity, and specificity | Accelerometer | Stroke |
| van den Heuvel et al. [41] | 2014 | 33 individuals with unknown age | Investigation of the effects of the balance training program | Accelerometer | Parkinson’s disease |
| Yalla et al. [42] | 2014 | 30 patients with an average age of 73 years old | Improvement of postural stability in older adults | Accelerometer, gyroscope, and magnetometer | Healthy patients |
| Allen et al. [43] | 2013 | Physical therapy students and stroke patients from Siskin Hospital | Measurement of fall risk | Accelerometer, gyroscope, and magnetometer | Stroke |
| Allen et al. [44] | 2013 | One patient with unknown age | Measurement of fall risk | Gyroscope, and accelerometer | Ischemic stroke |
| Shin et al. [45] | 2013 | 36 persons aged between 19 and 26 years old | Comparison of seated postural control in persons with spinal cord injury with age-related people | Force platform | Spinal Cord Injury |
| Itoh et al. [46] | 2012 | 30 subjects (9 males and 21 females with a minimum age of 63 years old | Calculation of the characteristics of the average acceleration of elderly people | Accelerometer | Healthy patients |
| Pertille et al. [47] | 2012 | 32 subjects aged between 65 and 80 years old | Monitoring of the effects of the treatment of bilateral grade III mobilization of the talocrural joint | Pressure platform | Bilateral grade III mobilization of the talocrural joint |
| Rajaratnam et al. [48] | 2011 | 12 individuals aged over 45 years old | Identification the effects of the use of the Wii Fit with conventional stroke rehabilitation | Force sensors in Nintendo Wii Balance Board | Hemiparetic stroke |
| Yamada et al. [49] | 2011 | 45 persons aged between 73 and 89 years old | Assessment of the fall risk with the Nintendo Wii Fit program | Pressure sensors | Parkinson’s disease or stroke |
| Costarella et al. [50] | 2010 | 50 subjects divided aged over 55 years old | Assessment of the physical and cognitive conditions | Pressure sensors | Healthy patients |
| Katz-Leurer et al. [51] | 2009 | 10 post-stroke patients with unknown age | Evaluation of the reliability of sitting balance, and the ability to change in reaching while sitting, and comparison of results from modified functional reach test and the Balance Master | Pressure sensors | Stroke |
| Features: | Interpretation: | Number of Studies: |
|---|---|---|
| mean speed | Dynamic Balance | 7 |
| mean acceleration | 4 | |
| maximum angular lumbosacral/thoracic displacement speed | 2 | |
| maximum lumbosacral/thoracic angular displacement | 2 | |
| maximum time of lumbosacral/thoracic angular displacement | 2 | |
| resultant displacement | 2 | |
| balance | 1 | |
| bent angle | 1 | |
| maximum acceleration | 1 | |
| maximum angular lumbosacral/thoracic displacement average acceleration | 1 | |
| maximum resultant acceleration | 1 | |
| maximum resultant speed | 1 | |
| maximum speed | 1 | |
| minimum acceleration | 1 | |
| minimum resultant acceleration | 1 | |
| minimum resultant speed | 1 | |
| initial position | 1 | |
| final position | 2 | |
| mean of stroke activity scale | 1 | |
| minimum speed | 1 | |
| distance | Quantitative | 12 |
| reaction time | 2 | |
| total time | 4 | |
| center-of-pressure path deviation | 1 | |
| maximum distance | 2 | |
| root mean square | 1 | |
| shuffles | 1 | |
| steps | 1 | |
| time return initial position | 1 | |
| trunk length | 1 | |
| angle | Raw statistic | 3 |
| pitch | 2 | |
| roll | 2 | |
| yaw | 2 | |
| absolute mean | 1 | |
| covariance | 1 | |
| mean | 1 | |
| mean cross rate | 1 | |
| mean trend | 1 | |
| quaternion | 1 | |
| range | 1 | |
| standard deviation | 1 | |
| variance | 1 | |
| zero-cross rate | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pires, I.M.; Garcia, N.M.; Zdravevski, E. Measurement of Results of Functional Reach Test with Sensors: A Systematic Review. Electronics 2020, 9, 1078. https://doi.org/10.3390/electronics9071078
Pires IM, Garcia NM, Zdravevski E. Measurement of Results of Functional Reach Test with Sensors: A Systematic Review. Electronics. 2020; 9(7):1078. https://doi.org/10.3390/electronics9071078
Chicago/Turabian StylePires, Ivan Miguel, Nuno M. Garcia, and Eftim Zdravevski. 2020. "Measurement of Results of Functional Reach Test with Sensors: A Systematic Review" Electronics 9, no. 7: 1078. https://doi.org/10.3390/electronics9071078