
A Convolutional Block Base Architecture for Multiclass Brain Tumor Detection Using Magnetic Resonance Imaging

Abstract
:1. Introduction
- We introduce a convolutional-block-based architecture for the detection and classification of multiclass brain tumors using MRI scans. This modular approach is pivotal in addressing the complexities of brain tumor manifestations, especially in scenarios with subtle and nuanced visual distinctions.
- To address the challenges of data heterogeneity, our study incorporates three distinct, publicly accessible multiclass datasets: Dataset 1 [38], Dataset 2 [39], and Dataset 3 [40]. The model demonstrates its adaptability and reliability across these datasets, with an average accuracy rate of 97.85%, thus showcasing its potential in various diagnostic scenarios.
- Our research proposes an automated, data-driven approach to improve both the efficiency and accuracy of the diagnostic process. This method effectively addresses the limitations inherent in traditional diagnostic techniques, such as the invasive nature of biopsies and potential errors in manual MRI scan interpretation.
- In a comparative analysis with state-of-the-art models such as VGG16, VGG19, MobileNetv2, and ResNet50, our proposed model outperforms in key performance metrics like accuracy, precision, and recall. It achieves a mean average precision (mAP) value of 99.03% on Dataset 1 [38], 99.93% on Dataset 2 [39], and 99.70% on Dataset 3 [40]. These high mAP scores further validate the model’s precision in detecting tumor instances across varied datasets, underscoring its effectiveness and reliability in brain tumor diagnostics.
2. Related Work
3. Methodology
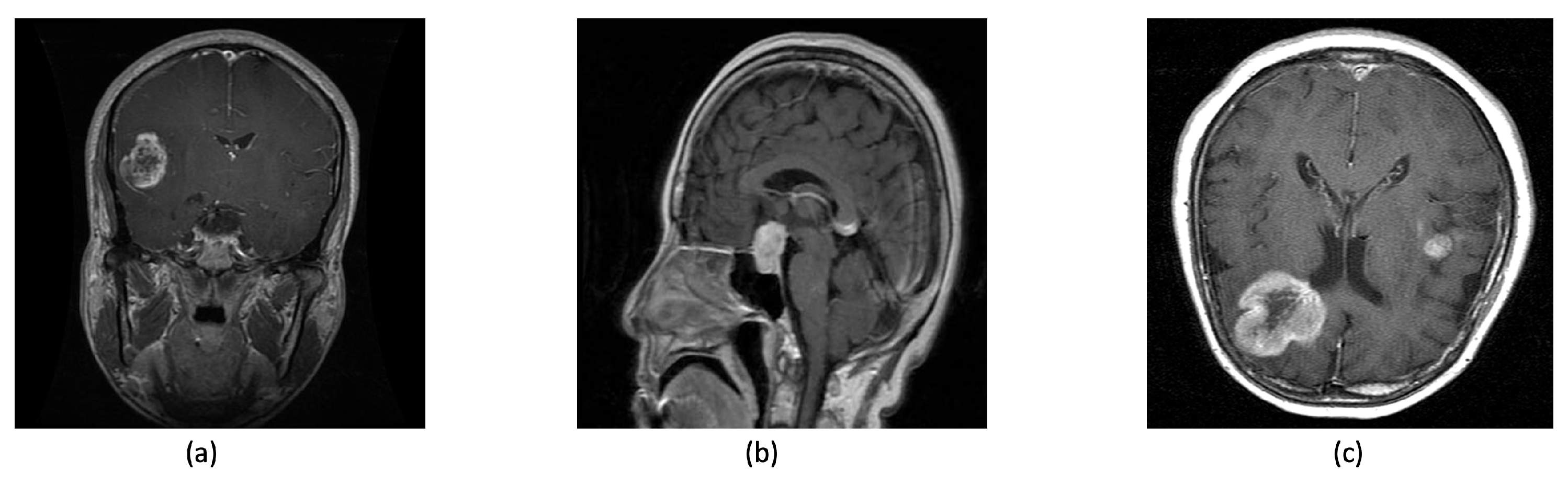
3.1. Dataset Collection
Image Rescaling and Normalization
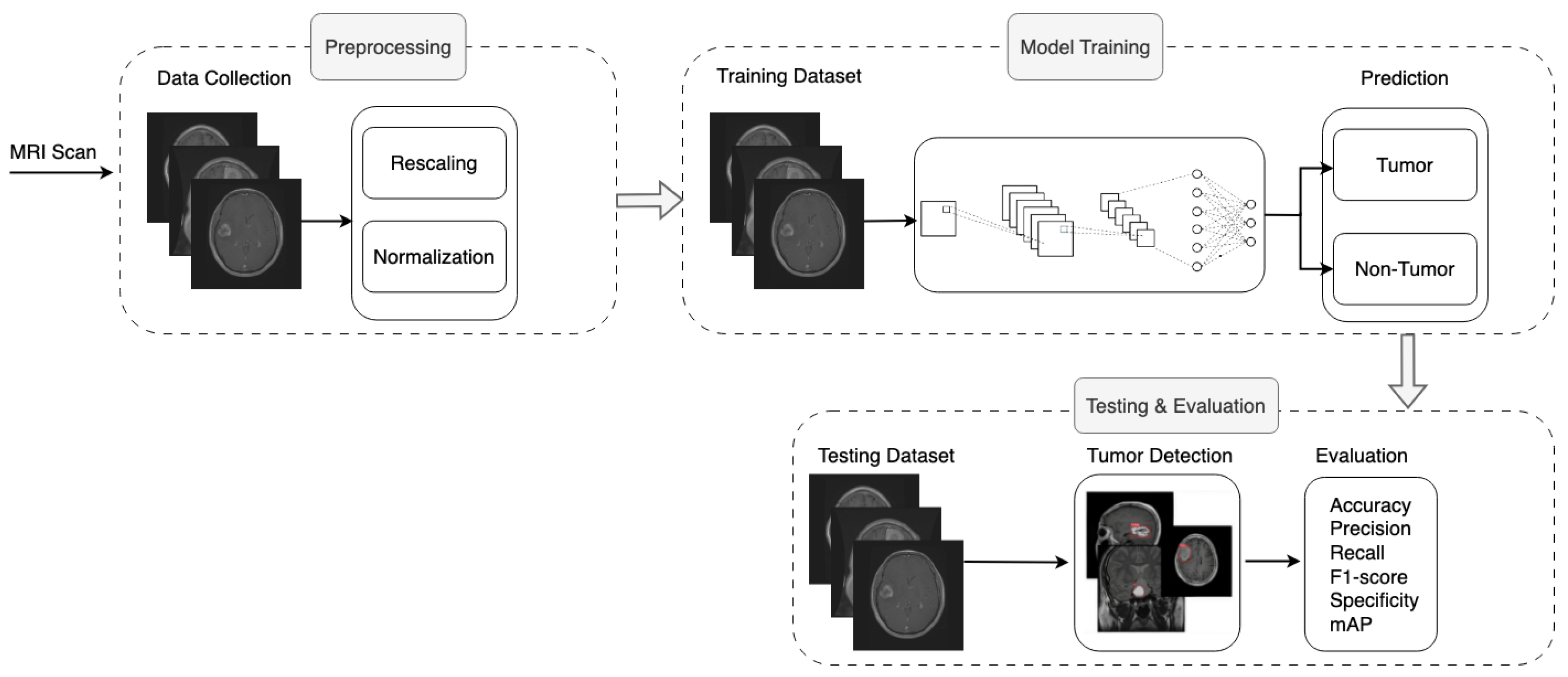
3.2. Proposed Methodology
| Algorithm 1 Pseudocode of the proposed model | |
| Require: , , | |
| 1: | Define Sequential model |
| 2: | |
| 3: | for i in do |
| 4: | if then |
| 5: | Add Conv2D layer with i filters, kernel size , and |
| 6: | else |
| 7: | Add Conv2D layer with i filters, kernel size |
| 8: | end if |
| 9: | Add MaxPool2D layer with pool size |
| 10: | Add BatchNormalization layer |
| 11: | end for |
| 12: | Add GlobalAveragePooling2D layer |
| 13: | Add Dense layer with 128 neurons and ReLU activation |
| 14: | Add Dense layer with “Number of Classes” neurons and Softmax activation |
| 15: | CompileAdam optimizer, loss and accuracy |
3.3. Loss Function and Optimization Strategy
4. Results
4.1. Key Performance Indicators (KPIs)
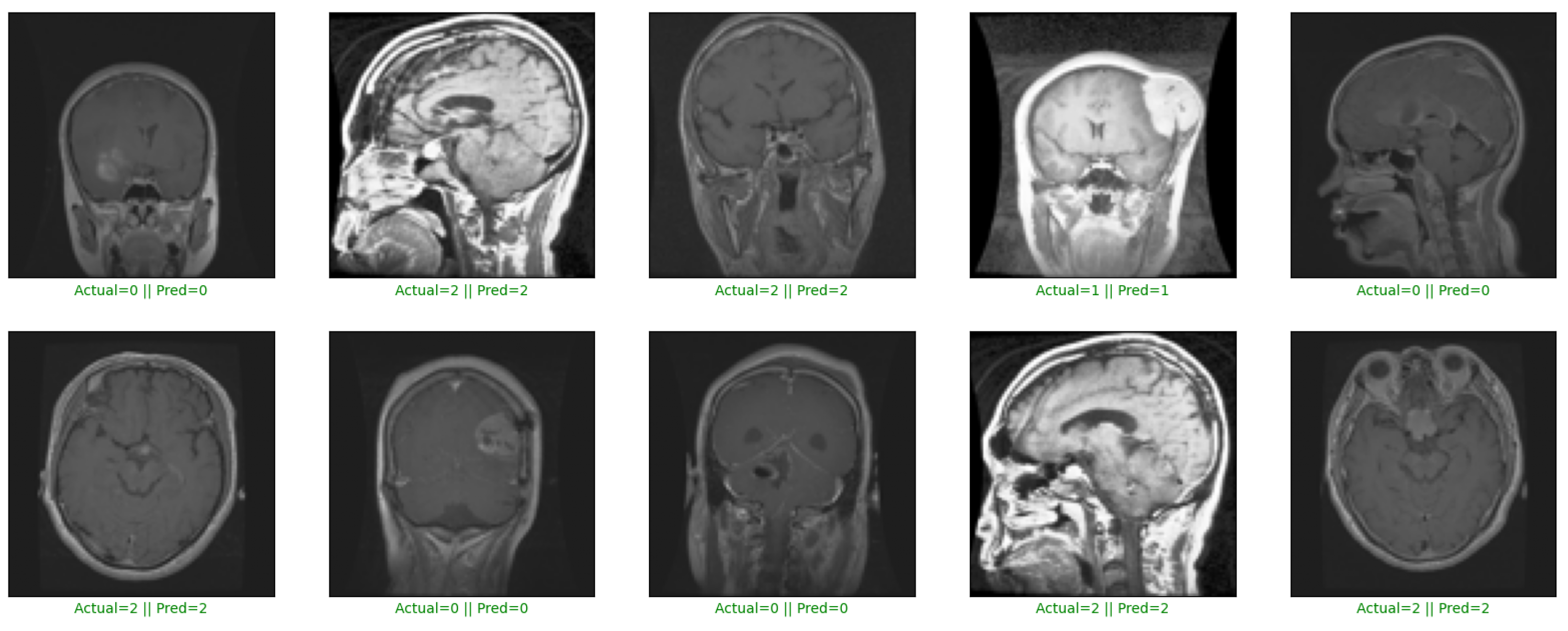
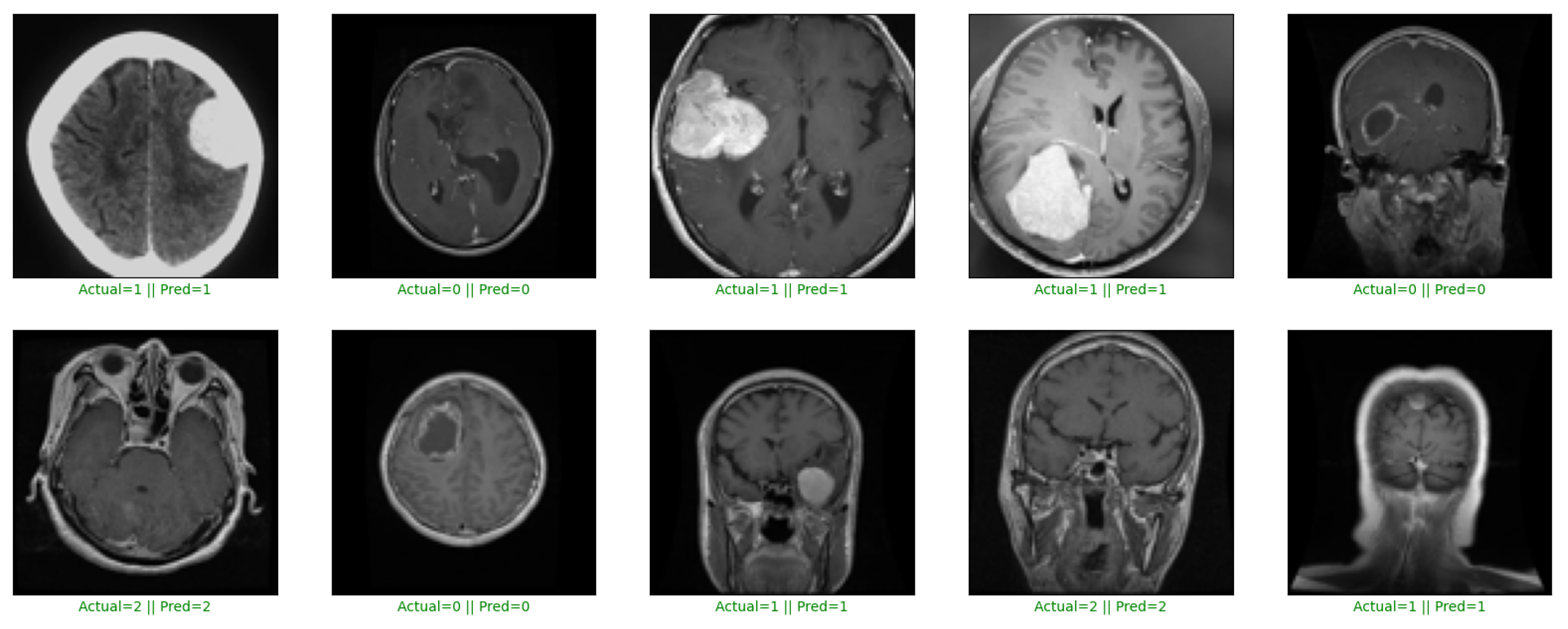
4.2. Experimental Result
4.2.1. Performance Results on Dataset 1
4.2.2. Performance Results on Dataset 2
4.2.3. Performance Results on Dataset 3
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gore, D.V.; Deshpande, V. Comparative study of various techniques using deep Learning for brain tumor detection. In Proceedings of the 2020 International Conference for Emerging Technology (INCET), Belgaum, India, 5–7 June 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 1–4. [Google Scholar]
- Gliomas and Its Symptoms and Causes; Johns Hopkins Medicine: Baltimore, MD, USA, 2022; Available online: https://www.hopkinsmedicine.org/health/conditions-and-diseases/gliomas (accessed on 10 September 2023).
- Pituitary Tumors—Symptoms and Causes; Mayo Clinic: Rochester, MN, USA, 2022; Available online: https://www.hopkinsmedicine.org/health/conditions-and-diseases/pituitary-tumors (accessed on 10 September 2023).
- Meningioma, Risk Its Symptoms; Johns Hopkins Medicine: Baltimore, MD, USA, 2022; Available online: https://www.hopkinsmedicine.org/health/conditions-and-diseases/meningioma (accessed on 10 September 2023).
- Rasheed, Z.; Ma, Y.K.; Ullah, I.; Ghadi, Y.Y.; Khan, M.Z.; Khan, M.A.; Abdusalomov, A.; Alqahtani, F.; Shehata, A.M. Brain tumor classification from MRI using image enhancement and convolutional neural network techniques. Brain Sci. 2023, 13, 1320. [Google Scholar] [CrossRef] [PubMed]
- McFaline-Figueroa, J.R.; Lee, E.Q. Brain tumors. Am. J. Med. 2018, 131, 874–882. [Google Scholar] [CrossRef] [PubMed]
- Payne, L.S.; Huang, P.H. The pathobiology of collagens in glioma. Mol. Cancer Res. 2013, 11, 1129–1140. [Google Scholar] [CrossRef] [PubMed]
- Wen, P.Y.; Kesari, S. Malignant gliomas in adults. N. Engl. J. Med. 2008, 359, 492–507. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Dwivedi, T. A simplified overview of World Health Organization classification update of central nervous system tumors 2016. J. Neurosci. Rural Pract. 2017, 8, 629–641. [Google Scholar] [CrossRef]
- Melmed, S. Pathogenesis of pituitary tumors. Nat. Rev. Endocrinol. 2011, 7, 257–266. [Google Scholar] [CrossRef]
- Rogers, L.; Barani, I.; Chamberlain, M.; Kaley, T.J.; McDermott, M.; Raizer, J.; Schiff, D.; Weber, D.C.; Wen, P.Y.; Vogelbaum, M.A. Meningiomas: Knowledge base, treatment outcomes, and uncertainties. A RANO review. J. Neurosurg. 2015, 122, 4–23. [Google Scholar] [CrossRef]
- Zhao, L.; Zhao, W.; Hou, Y.; Wen, C.; Wang, J.; Wu, P.; Guo, Z. An overview of managements in meningiomas. Front. Oncol. 2020, 10, 1523. [Google Scholar] [CrossRef]
- Holleczek, B.; Zampella, D.; Urbschat, S.; Sahm, F.; von Deimling, A.; Oertel, J.; Ketter, R. Incidence, mortality and outcome of meningiomas: A population-based study from Germany. Cancer Epidemiol. 2019, 62, 101562. [Google Scholar] [CrossRef]
- Perry, A. Meningiomas. In Practical Surgical Neuropathology: A Diagnostic Approach; Elsevier: Amsterdam, The Netherlands, 2018; pp. 259–298. [Google Scholar]
- Komaki, K.; Sano, N.; Tangoku, A. Problems in histological grading of malignancy and its clinical significance in patients with operable breast cancer. Breast Cancer 2006, 13, 249–253. [Google Scholar] [CrossRef]
- Grant, R.; Dowswell, T.; Tomlinson, E.; Brennan, P.M.; Walter, F.M.; Ben-Shlomo, Y.; Hunt, D.W.; Bulbeck, H.; Kernohan, A.; Robinson, T.; et al. Interventions to reduce the time to diagnosis of brain tumours. Cochrane Database Syst. Rev. 2020, 2020, CD013564. [Google Scholar] [CrossRef]
- Shehab, M.; Abualigah, L.; Shambour, Q.; Abu-Hashem, M.A.; Shambour, M.K.Y.; Alsalibi, A.I.; Gandomi, A.H. Machine learning in medical applications: A review of state-of-the-art methods. Comput. Biol. Med. 2022, 145, 105458. [Google Scholar] [CrossRef] [PubMed]
- Fernando, T.; Gammulle, H.; Denman, S.; Sridharan, S.; Fookes, C. Deep learning for medical anomaly detection–a survey. ACM Comput. Surv. (CSUR) 2021, 54, 1–37. [Google Scholar] [CrossRef]
- Frid-Adar, M.; Diamant, I.; Klang, E.; Amitai, M.; Goldberger, J.; Greenspan, H. GAN-based synthetic medical image augmentation for increased CNN performance in liver lesion classification. Neurocomputing 2018, 321, 321–331. [Google Scholar] [CrossRef]
- Ge, C.; Gu, I.Y.H.; Jakola, A.S.; Yang, J. Deep learning and multi-sensor fusion for glioma classification using multistream 2D convolutional networks. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 5894–5897. [Google Scholar]
- Ge, C.; Gu, I.Y.H.; Jakola, A.S.; Yang, J. Enlarged training dataset by pairwise GANs for molecular-based brain tumor classification. IEEE Access 2020, 8, 22560–22570. [Google Scholar] [CrossRef]
- Mzoughi, H.; Njeh, I.; Wali, A.; Slima, M.B.; BenHamida, A.; Mhiri, C.; Mahfoudhe, K.B. Deep multi-scale 3D convolutional neural network (CNN) for MRI gliomas brain tumor classification. J. Digit. Imaging 2020, 33, 903–915. [Google Scholar] [CrossRef] [PubMed]
- Dixit, A.; Nanda, A. An improved whale optimization algorithm-based radial neural network for multi-grade brain tumor classification. Vis. Comput. 2021, 38, 3525–3540. [Google Scholar] [CrossRef]
- Chan, H.P.; Hadjiiski, L.M.; Samala, R.K. Computer-aided diagnosis in the era of deep learning. Med. Phys. 2020, 47, e218–e227. [Google Scholar] [CrossRef]
- Lynch, C.J.; Liston, C. New machine-learning technologies for computer-aided diagnosis. Nat. Med. 2018, 24, 1304–1305. [Google Scholar] [CrossRef]
- Tanvir Rouf Shawon, M.; Shahariar Shibli, G.; Ahmed, F.; Saha Joy, S.K. Explainable Cost-Sensitive Deep Neural Networks for Brain Tumor Detection from Brain MRI Images considering Data Imbalance. arXiv 2023, arXiv:2308.00608. [Google Scholar] [CrossRef]
- Kayalibay, B.; Jensen, G.; van der Smagt, P. CNN-based segmentation of medical imaging data. arXiv 2017, arXiv:1701.03056. [Google Scholar]
- Matsoukas, C.; Haslum, J.F.; Söderberg, M.; Smith, K. Pretrained ViTs Yield Versatile Representations For Medical Images. arXiv 2023, arXiv:2303.07034. [Google Scholar]
- Tajbakhsh, N.; Shin, J.Y.; Gurudu, S.R.; Hurst, R.T.; Kendall, C.B.; Gotway, M.B.; Liang, J. Convolutional neural networks for medical image analysis: Full training or fine tuning? IEEE Trans. Med. Imaging 2016, 35, 1299–1312. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Huang, W.; Cao, S.; Yang, R.; Yang, W.; Yun, Z.; Wang, Z.; Feng, Q. Enhanced performance of brain tumor classification via tumor region augmentation and partition. PLoS ONE 2015, 10, e0140381. [Google Scholar] [CrossRef] [PubMed]
- David, D.; Arun, L. Classification of brain tumor type and grade using MRI texture and shape in a machine learning scheme. Artech J. Eff. Res. Eng. Technol. 2020, 1, 57–63. [Google Scholar]
- Pashaei, A.; Sajedi, H.; Jazayeri, N. Brain tumor classification via convolutional neural network and extreme learning machines. In Proceedings of the 2018 8th International Conference on Computer and Knowledge Engineering (ICCKE), Virtual, 25–26 October 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 314–319. [Google Scholar]
- Kaplan, K.; Kaya, Y.; Kuncan, M.; Ertunç, H.M. Brain tumor classification using modified local binary patterns (LBP) feature extraction methods. Med. Hypotheses 2020, 139, 109696. [Google Scholar] [CrossRef]
- Pinho, M.C.; Bera, K.; Beig, N.; Tiwari, P. MRI Morphometry in brain tumors: Challenges and opportunities in expert, radiomic, and deep-learning-based analyses. Brain Tumors 2021, 158, 323–368. [Google Scholar]
- Saeedi, S.; Rezayi, S.; Keshavarz, H.; R Niakan Kalhori, S. MRI-based brain tumor detection using convolutional deep learning methods and chosen machine learning techniques. BMC Med. Inform. Decis. Mak. 2023, 23, 16. [Google Scholar] [CrossRef]
- Abdusalomov, A.B.; Mukhiddinov, M.; Whangbo, T.K. Brain tumor detection based on deep learning approaches and magnetic resonance imaging. Cancers 2023, 15, 4172. [Google Scholar] [CrossRef]
- Ahuja, S.; Panigrahi, B.; Gandhi, T. Transfer learning based brain tumor detection and segmentation using superpixel technique. In Proceedings of the 2020 International Conference on Contemporary Computing and Applications (IC3A), Lucknow, India, 5–7 February 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 244–249. [Google Scholar]
- Muhammadd. Brain Tumor MRI Images; Kaggle: San Francisco, CA, USA, 2023; Available online: https://www.kaggle.com/datasets/muhammadd7/brain-tumor-mri-images (accessed on 10 January 2023).
- Nickparvar, M. Brain Tumor MRI Dataset; Kaggle: San Francisco, CA, USA, 2021. [Google Scholar] [CrossRef]
- Eldakrory, S. Brain Tumors MRI Images; Kaggle: San Francisco, CA, USA, 2023; Available online: https://www.kaggle.com/datasets/shadyeldakrory/shadyfinal3 (accessed on 10 January 2023).
- Soltaninejad, M.; Zhang, L.; Lambrou, T.; Allinson, N.; Ye, X. Multimodal MRI brain tumor segmentation using random forests with features learned from fully convolutional neural network. arXiv 2017, arXiv:1704.08134. [Google Scholar]
- Nguyen, H.T.; Le, T.T.; Nguyen, T.V.; Nguyen, N.T. Enhancing MRI brain tumor segmentation with an additional classification network. In Proceedings of the International MICCAI Brainlesion Workshop, Lima, Peru, 4 October 2020; Springer: Berlin/Heidelberg, Germany, 2020; pp. 503–513. [Google Scholar]
- Maurya, U.; Kalyan, A.K.; Bohidar, S.; Sivakumar, D.S. Detection and Classification of Glioblastoma Brain Tumor. arXiv 2023, arXiv:2304.09133. [Google Scholar]
- Balaji, G.; Sen, R.; Kirty, H. Detection and Classification of Brain tumors Using Deep Convolutional Neural Networks. arXiv 2022, arXiv:2208.13264. [Google Scholar]
- Siddique, M.A.B.; Sakib, S.; Khan, M.M.R.; Tanzeem, A.K.; Chowdhury, M.; Yasmin, N. Deep convolutional neural networks model-based brain tumor detection in brain MRI images. In Proceedings of the 2020 Fourth International Conference on I-SMAC (IoT in Social, Mobile, Analytics and Cloud) (I-SMAC), Palladam, India, 7–9 October 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 909–914. [Google Scholar]
- Hamran, A.; Vaeztourshizi, M.; Esmaili, A.; Pedram, M. Brain Tumor Detection using Convolutional Neural Networks with Skip Connections. arXiv 2023, arXiv:2307.07503. [Google Scholar]
- Karimi, D.; Gholipour, A. Improving calibration and out-of-distribution detection in deep models for medical image segmentation. IEEE Trans. Artif. Intell. 2022, 4, 383–397. [Google Scholar] [CrossRef] [PubMed]
- Fard, A.S.; Reutens, D.C.; Vegh, V. CNNs and GANs in MRI-based cross-modality medical image estimation. arXiv 2021, arXiv:2106.02198. [Google Scholar]
- Gumaei, A.; Hassan, M.M.; Hassan, M.R.; Alelaiwi, A.; Fortino, G. A hybrid feature extraction method with regularized extreme learning machine for brain tumor classification. IEEE Access 2019, 7, 36266–36273. [Google Scholar] [CrossRef]
- Swati, Z.N.K.; Zhao, Q.; Kabir, M.; Ali, F.; Ali, Z.; Ahmed, S.; Lu, J. Brain tumor classification for MR images using transfer learning and fine-tuning. Comput. Med. Imaging Graph. 2019, 75, 34–46. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.L.; Kakarla, J.; Isunuri, B.V.; Singh, M. Multi-class brain tumor classification using residual network and global average pooling. Multimed. Tools Appl. 2021, 80, 13429–13438. [Google Scholar] [CrossRef]
- Aamir, M.; Rahman, Z.; Dayo, Z.A.; Abro, W.A.; Uddin, M.I.; Khan, I.; Imran, A.S.; Ali, Z.; Ishfaq, M.; Guan, Y.; et al. A deep learning approach for brain tumor classification using MRI images. Comput. Electr. Eng. 2022, 101, 108105. [Google Scholar] [CrossRef]
- Dehkordi, A.A.; Hashemi, M.; Neshat, M.; Mirjalili, S.; Sadiq, A.S. Brain Tumor Detection and Classification Using a New Evolutionary Convolutional Neural Network. arXiv 2022, arXiv:2204.12297. [Google Scholar] [CrossRef]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Zou, Z.; Chen, K.; Shi, Z.; Guo, Y.; Ye, J. Object detection in 20 years: A survey. Proc. IEEE 2023, 111, 257–276. [Google Scholar] [CrossRef]
- Abd El Kader, I.; Xu, G.; Shuai, Z.; Saminu, S.; Javaid, I.; Salim Ahmad, I. Differential deep convolutional neural network model for brain tumor classification. Brain Sci. 2021, 11, 352. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Tumor Type | Total Size | Training Size | Validation Size | Testing Size | Label Distribution |
|---|---|---|---|---|---|---|
| Dataset 1 [38] | Glioma | 19,226 | 14,718 | 3680 | 828 | Glioma: 34.27% |
| Pituitary | Pituitary: 33.38% | |||||
| Meningioma | Meningioma 32.35% | |||||
| Dataset 2 [39] | Glioma | 5023 | 3293 | 824 | 906 | Glioma: 32.29% |
| Pituitary | Pituitary: 34.97% | |||||
| Meningioma | Meningioma 32.74% | |||||
| Dataset 3 [40] | Glioma | 19,226 | 13,686 | 2770 | 2770 | Glioma: 34.27% |
| Pituitary | Pituitary: 33.38% | |||||
| Meningioma | Meningioma 32.35% | |||||
| Total | - | 43,475 | 31,697 | 7274 | 4504 | - |
| Image Resolution Size | Time (in Seconds) | Resources Usage (in MByte) | Accuracy (%) | Precision (%) |
|---|---|---|---|---|
| 32 × 32 | 1185.6 | 7.8 | 92.02 | 92.29 |
| 50 × 50 | 1229.7 | 8.6 | 96.13 | 96.17 |
| 80 × 80 | 1328.8 | 9.4 | 96.25 | 96.37 |
| 100 × 100 | 1874.4 | 17.2 | 97.58 | 97.59 |
| 150 × 150 | 2339.3 | 20.9 | 97.22 | 97.36 |
| Layer Name | Output Size | Kernel Size | Strides | Activation | Number of Layers |
|---|---|---|---|---|---|
| Input | 100 × 100 × 3 | - | - | - | - |
| Conv2D | 98 × 98 × 32 | 3 × 3 | 1 × 1 | ReLU | 2 |
| BatchNormalization | - | - | - | - | 1 |
| MaxPool2D | 49 × 49 × 32 | 2 × 2 | 2 × 2 | - | 1 |
| Conv2D | 49 × 49 × 64 | 3 × 3 | 1 × 1 | ReLU | 3 |
| BatchNormalization | - | - | - | - | 1 |
| MaxPool2D | 24 × 24 × 64 | 2 × 2 | 2 × 2 | - | 1 |
| Conv2D | 24 × 24 × 128 | 3 × 3 | 1 × 1 | ReLU | 3 |
| BatchNormalization | - | - | - | - | 1 |
| MaxPool2D | 12 × 12 × 128 | 2 × 2 | 2 × 2 | - | 1 |
| Conv2D | 12 × 12 × 256 | 3 × 3 | 1 × 1 | ReLU | 2 |
| Conv2D | 12 × 12 × 512 | 3 × 3 | 1 × 1 | ReLU | 2 |
| GlobalAveragePooling | - | - | - | - | 1 |
| Dense | 128 | - | - | ReLU | 1 |
| Dropout | - | - | - | - | 1 |
| Dense | Number of Classes | - | - | Softmax | 1 |
| Model | Accuracy (%) | Precision (%) | Recall (%) | F1-Score (%) | Specificity (%) | mAP (%) | Memory (MByte) |
|---|---|---|---|---|---|---|---|
| VGG16 | 96.74 | 96.76 | 96.74 | 96.73 | 98.37 | 99.29 | 11.6 |
| VGG19 | 94.93 | 95.20 | 94.93 | 94.90 | 97.44 | 99.15 | 14.2 |
| MobileNet | 96.14 | 96.13 | 96.14 | 96.13 | 98.07 | 98.96 | 14.2 |
| EfficientNet | 58.57 | 60.02 | 58.57 | 58.72 | 79.33 | 68.69 | 14.2 |
| ResNet50 | 96.50 | 96.52 | 96.50 | 96.48 | 98.24 | 99.46 | 16.4 |
| Xception | 96.98 | 97.04 | 96.98 | 96.99 | 99.70 | 99.43 | 17.2 |
| DenseNet121 | 96.86 | 96.86 | 96.86 | 96.85 | 98.50 | 98.43 | 11.9 |
| Proposed Model | 97.58 | 97.59 | 97.58 | 97.58 | 98.80 | 99.03 | 17.2 |
| Model | Accuracy (%) | Precision (%) | Recall (%) | F1-Score (%) | Specificity (%) | mAP (%) | Memory (MByte) |
|---|---|---|---|---|---|---|---|
| VGG16 | 95.25 | 95.54 | 95.25 | 95.27 | 97.63 | 99.52 | 5.9 |
| VGG19 | 97.35 | 97.39 | 97.35 | 97.35 | 98.67 | 99.63 | 7.2 |
| MobileNet | 97.35 | 97.40 | 97.35 | 97.35 | 98.68 | 99.52 | 7.2 |
| EfficientNet | 38.19 | 24.84 | 38.19 | 29.08 | 69.09 | 45.23 | 7.2 |
| ResNet50 | 98.23 | 98.24 | 98.23 | 98.23 | 98.95 | 99.76 | 8.2 |
| Xception | 97.90 | 97.92 | 97.90 | 97.91 | 98.95 | 99.86 | 8.6 |
| DenseNet121 | 97.13 | 97.14 | 97.13 | 97.12 | 98.56 | 99.30 | 6.0 |
| Proposed Model | 98.79 | 98.81 | 98.79 | 98.79 | 99.39 | 99.93 | 8.9 |
| Model | Accuracy (%) | Precision (%) | Recall (%) | F1 Score (%) | Specificity (%) | mAP (%) | Memory (MByte) |
|---|---|---|---|---|---|---|---|
| VGG16 | 92.85 | 93.18 | 92.85 | 92.85 | 96.40 | 98.48 | 16.4 |
| VGG19 | 95.52 | 95.52 | 95.52 | 95.51 | 97.76 | 99.22 | 14.2 |
| MobileNet | 96.64 | 96.65 | 96.64 | 96.63 | 98.32 | 99.15 | 10.9 |
| EfficientNet | 70.65 | 70.56 | 70.65 | 70.60 | 85.34 | 78.10 | 13.4 |
| ResNet50 | 96.75 | 96.74 | 96.75 | 96.74 | 98.38 | 99.40 | 14.1 |
| Xception | 96.64 | 96.66 | 96.64 | 96.65 | 98.33 | 99.27 | 14.9 |
| DenseNet121 | 96.75 | 96.76 | 96.75 | 96.75 | 98.38 | 99.25 | 16.4 |
| Proposed Model | 97.18 | 97.19 | 97.18 | 97.18 | 98.59 | 99.70 | 10.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, M.A.; Park, H. A Convolutional Block Base Architecture for Multiclass Brain Tumor Detection Using Magnetic Resonance Imaging. Electronics 2024, 13, 364. https://doi.org/10.3390/electronics13020364
Khan MA, Park H. A Convolutional Block Base Architecture for Multiclass Brain Tumor Detection Using Magnetic Resonance Imaging. Electronics. 2024; 13(2):364. https://doi.org/10.3390/electronics13020364
Chicago/Turabian StyleKhan, Muneeb A., and Heemin Park. 2024. "A Convolutional Block Base Architecture for Multiclass Brain Tumor Detection Using Magnetic Resonance Imaging" Electronics 13, no. 2: 364. https://doi.org/10.3390/electronics13020364