
Mixed Reality in Undergraduate Mental Health Education: A Systematic Review
 , , and
, , and
Abstract
:1. Introduction
1.1. Mixed Reality
1.2. Advantages of MR Use
1.3. Disadvantages of MR Use
2. Materials and Methods
2.1. General Description
2.2. Selection Criteria
2.3. Outcomes
2.4. Search Methodology
2.5. Data Collection and Analysis
2.6. Data Extraction and Management
2.7. Quality of Studies Included
2.8. Statistical Analysis
3. Results
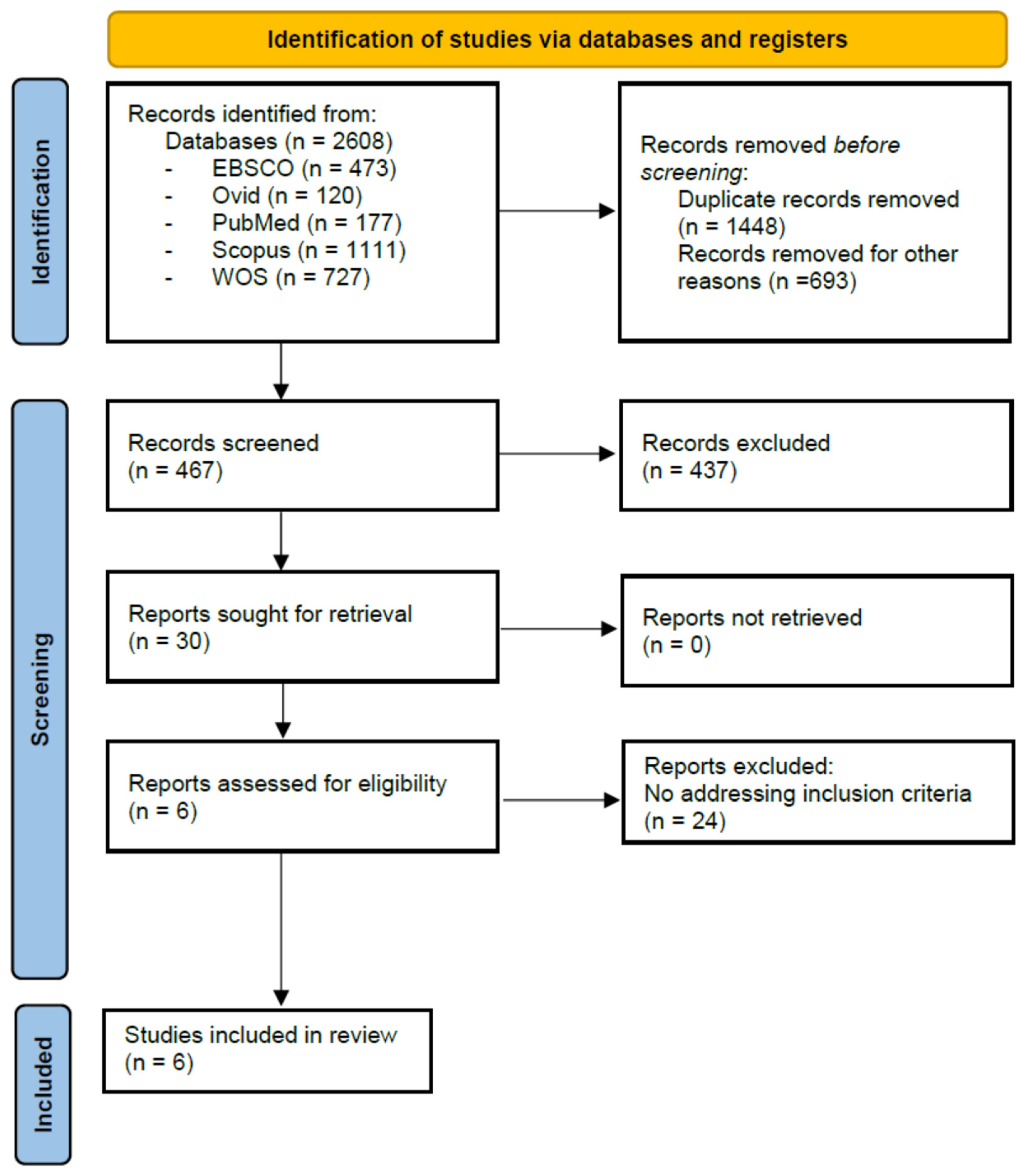
3.1. Study Selection and Inclusion
3.2. General Characteristics of the Studies Included
3.3. Assessment of Methodological Quality of Included Studies
3.4. Primary Outcomes
3.5. Secondary Outcomes
4. Discussion
4.1. MR Usefulness to Enhance Acquisition of Knowledge/Skills in Mental Health Education
4.2. MR Advantages and Disadvantages in Undergraduate Mental Health Education
5. Conclusions
5.1. Clinical and Researcher Implications
5.2. Limitations
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Car, L.T.; Kyaw, B.M.; Teo, A.; Fox, T.E.; Vimalesvaran, S.; Apfelbacher, C.; Kemp, S.; Chavannes, N. Outcomes, Measurement Instruments, and Their Validity Evidence in Randomized Controlled Trials on Virtual, Augmented, and Mixed Reality in Undergraduate Medical Education: Systematic Mapping Review. JMIR Serious Games 2022, 10, e29594. [Google Scholar]
- Zhang, J.; Yu, N.; Wang, B.; Lv, X. Trends in the use of augmented reality, virtual reality, and mixed reality in surgical research: A global bibliometric and visualized analysis. Indian J. Surg. 2022, 84, 52–69. [Google Scholar] [CrossRef] [PubMed]
- Milgram, P.; Kishino, F. A taxonomy of mixed reality visual displays. IEICE Trans. Inf. Syst. 1994, 77, 1321–1329. [Google Scholar]
- Ma, L.; Mor, S.; Anderson, P.L.; Baños, R.M.; Botella, C.; Bouchard, S.; Cárdenas-López, G.; Donker, T.; Fernández-Álvarez, J.; Lindner, P. Integrating virtual realities and psychotherapy: SWOT analysis on VR and MR based treatments of anxiety and stress-related disorders. Cogn. Behav. Ther. 2021, 50, 509–526. [Google Scholar] [CrossRef] [PubMed]
- Aruanno, B.; Garzotto, F. MemHolo: Mixed reality experiences for subjects with Alzheimer’s disease. Multimed. Tools Appl. 2019, 78, 13517–13537. [Google Scholar] [CrossRef]
- Gerup, J.; Soerensen, C.B.; Dieckmann, P. Augmented reality and mixed reality for healthcare education beyond surgery: An integrative review. Int. J. Med. Educ. 2020, 11, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Car, J.; Carlstedt-Duke, J.; Car, L.T.; Posadzki, P.; Whiting, P.; Zary, N.; Atun, R.; Majeed, A.; Campbell, J. Digital Health Education Collaboration Digital education in health professions: The need for overarching evidence synthesis. J. Med. Internet Res. 2019, 21, e12913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- John, B.; Kurian, J.C.; Fitzgerald, R.; Lian Goh, D.H. Students’ Learning Experience in a Mixed Reality Environment: Drivers and Barriers. Commun. Assoc. Inf. Syst. 2022, 50, 28. [Google Scholar] [CrossRef]
- Chen, L.; Day, T.W.; Tang, W.; John, N.W. Recent Developments and Future Challenges in Medical Mixed Reality. In Proceedings of the 2017 IEEE International Symposium on Mixed and Augmented Reality (ISMAR), Nantes, France, 9–13 October 2017; pp. 123–135. [Google Scholar]
- Hoffman, M.A. Microsoft Hololens development edition. Science 2016, 353, 876. [Google Scholar] [CrossRef]
- Stromberga, Z.; Phelps, C.; Smith, J.; Moro, C. Teaching with disruptive technology: The use of augmented, virtual, and mixed reality (HoloLens) for disease education. In Biomedical Visualisation; Springer: Cham, Switzerland, 2021; pp. 147–162. [Google Scholar]
- Brun, H.; Bugge, R.A.B.; Suther, L.; Birkeland, S.; Kumar, R.; Pelanis, E.; Elle, O.J. Mixed reality holograms for heart surgery planning: First user experience in congenital heart disease. Eur. Heart J.-Cardiovasc. Imaging 2019, 20, 883–888. [Google Scholar] [CrossRef] [Green Version]
- Ryan, G.V.; Callaghan, S.; Rafferty, A.; Higgins, M.F.; Mangina, E.; McAuliffe, F. Learning Outcomes of Immersive Technologies in Health Care Student Education: Systematic Review of the Literature. J. Med. Internet Res. 2022, 24, e30082. [Google Scholar] [CrossRef]
- Baratz, G.; Sridharan, P.S.; Yong, V.; Tatsuoka, C.; Griswold, M.A.; Wish-Baratz, S. Comparing learning retention in medical students using mixed-reality to supplement dissection: A preliminary study. Int. J. Med. Educ. 2022, 13, 107–114. [Google Scholar] [CrossRef]
- Al-Tikriti, M.; Al-Aubidy, K. Embedding Mixed-Reality Laboratories into E-Learning Systems for Engineering Education. J. Educ. Technol. 2013, 9, 25–35. [Google Scholar] [CrossRef]
- Arango-Lopez, J.; Ceron Valdivieso, C.C.; Collazos, C.A.; Gutierrez Vela, F.L.; Moreira, F. CREANDO: Tool for creating pervasive games to increase the learning motivation in higher education students. Telemat. Inf. 2019, 38, 62–73. [Google Scholar] [CrossRef]
- Brunzini, A.; Papetti, A.; Messi, D.; Germani, M. A comprehensive method to design and assess mixed reality simulations. Virtual Real. 2022, 26, 1257–1275. [Google Scholar] [CrossRef]
- Liang, C.; Start, C.; Boley, H.; Kamat, V.R.; Menassa, C.C.; Aebersold, M. Enhancing stroke assessment simulation experience in clinical training using augmented reality. Virtual Real. 2021, 25, 575–584. [Google Scholar] [CrossRef]
- Diemer, J.; Alpers, G.W.; Peperkorn, H.M.; Shiban, Y.; Mühlberger, A. The impact of perception and presence on emotional reactions: A review of research in virtual reality. Front. Psychol. 2015, 6, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, C.S.; Bailenson, J.N.; Welch, G.F. A Systematic Review of Social Presence: Definition, Antecedents, and Implications. Front. Robot. AI 2018, 5, 114. [Google Scholar] [CrossRef] [Green Version]
- Lombard, M.; Ditton, T. At the heart of it all: The concept of presence. J. Comput.-Mediat. Commun. 1997, 3, JCMC321. [Google Scholar] [CrossRef]
- Price, M.; Anderson, P. The role of presence in virtual reality exposure therapy. J. Anxiety Disord. 2007, 21, 742–751. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Vives, M.V.; Slater, M. From presence to consciousness through virtual reality. Nat. Rev. Neurosci. 2005, 6, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Miloff, A.; Lindner, P.; Hamilton, W.; Reuterskiöld, L.; Andersson, G.; Carlbring, P. Single-session gamified virtual reality exposure therapy for spider phobia vs. traditional exposure therapy: Study protocol for a randomized controlled non-inferiority trial. Trials 2016, 17, 60. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.L.; Foley, M.R. Transforming clinical education in obstetrics and gynecology: Gone is the day of the sage on the stage. Obstet. Gynecol. 2016, 127, 763–767. [Google Scholar] [CrossRef]
- Machleid, F.; Kaczmarczyk, R.; Johann, D.; Balčiūnas, J.; Atienza-Carbonell, B.; von Maltzahn, F.; Mosch, L. Perceptions of digital health education among European medical students: Mixed methods survey. J. Med. Internet Res. 2020, 22, e19827. [Google Scholar] [CrossRef]
- Beyoglu, D.; Hursen, C.; Nasiboglu, A. Use of mixed reality applications in teaching of science. Educ. Inf. Technol. 2020, 25, 4271–4286. [Google Scholar] [CrossRef]
- Kyaw, B.M.; Saxena, N.; Posadzki, P.; Vseteckova, J.; Nikolaou, C.K.; George, P.P.; Divakar, U.; Masiello, I.; Kononowicz, A.A.; Zary, N. Virtual reality for health professions education: Systematic review and meta-analysis by the digital health education collaboration. J. Med. Internet Res. 2019, 21, e12959. [Google Scholar] [CrossRef] [Green Version]
- Middeke, A.; Anders, S.; Raupach, T.; Schuelper, N. Transfer of clinical reasoning trained with a serious game to comparable clinical problems: A prospective randomized study. Simul. Healthc. 2020, 15, 75–81. [Google Scholar] [CrossRef]
- Boeldt, D.; McMahon, E.; McFaul, M.; Greenleaf, W. Using Virtual Reality Exposure Therapy to Enhance Treatment of Anxiety Disorders: Identifying Areas of Clinical Adoption and Potential Obstacles. Front. Psychiatry 2019, 10, 773. [Google Scholar] [CrossRef] [Green Version]
- Yoo, H.; Jang, J.; Oh, H.; Park, I. The potentials and trends of holography in education: A scoping review. Comput. Educ. 2022, 186, 104533. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G. Practical Statistics for Medical Research; CRC Press: Boca Raton, FL, USA, 1990. [Google Scholar]
- Pluye, P.; Gagnon, M.; Griffiths, F.; Johnson-Lafleur, J. A scoring system for appraising mixed methods research, and concomitantly appraising qualitative, quantitative and mixed methods primary studies in mixed studies reviews. Int. J. Nurs. Stud. 2009, 46, 529–546. [Google Scholar] [CrossRef]
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.; Griffiths, F.; Nicolau, B. Mixed methods appraisal tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Abdullah, J.; Mohd-Isa, W.; Samsudin, M.A. Virtual reality to improve group work skill and self-directed learning in problem-based learning narratives. Virtual Real. 2019, 23, 461–471. [Google Scholar] [CrossRef]
- Aguinaga-Ontoso, I.; Guillen-Aguinaga, L.; Guillen-Aguinaga, S. Evaluation of Mixed reality in undergraduate nursing education. A systematic review. Eur. J. Public Health 2021, 31, iii456–iii457. [Google Scholar] [CrossRef]
- Allcoat, D.; Hatchard, T.; Azmat, F.; Stansfield, K.; Watson, D.; von Muhlenen, A. Education in the Digital Age: Learning Experience in Virtual and Mixed Realities. J. Educ. Comput. Res. 2021, 59, 795–816. [Google Scholar] [CrossRef]
- Antoniou, P.E.; Dafli, E.; Arfaras, G.; Bamidis, P.D. Versatile mixed reality medical educational spaces; requirement analysis from expert users. Pers. Ubiquitous Comput. 2017, 21, 1015–1024. [Google Scholar] [CrossRef]
- Baños, R.M.; Herrero, R.; Vara, M.D. What is the Current and Future Status of Digital Mental Health Interventions? Span. J. Psychol. 2022, 25, e5. [Google Scholar] [CrossRef]
- Bellamy, E.; Whitehead, B.; Ansell, H. Opportunities for augmented reality in clinical simulation education. Nurs. Times 2022, 118, 43–46. [Google Scholar]
- Bi, T.; Lyons, R.; Fox, G.; Muntean, G.-M. Improving Student Learning Satisfaction by Using an Innovative DASH-Based Multiple Sensorial Media Delivery Solution. IEEE Trans. Multimed. 2021, 23, 3494–3505. [Google Scholar] [CrossRef]
- Birt, J.; Stromberga, Z.; Cowling, M.; Moro, C. Mobile mixed reality for experiential learning and simulation in medical and health sciences education. Information 2018, 9, 31. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.-J.; Chen, Y.-C.; Lee, M.-Y.; Wang, C.-H.; Sung, H.-C. Effects of three-dimensional holograms on the academic performance of nursing students in a health assessment and practice course: A pretest-intervention-posttest study. Nurse Educ. Today 2021, 106, 105081. [Google Scholar] [CrossRef]
- Cochrane, T.; Aiello, S.; Cook, S.; Aguayo, C.; Wilkinson, N. MESH360: A framework for designing MMR-enhanced clinical simulations. Res. Learn. Technol. 2020, 28, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Cochrane, T.; Narayan, V.; Birt, J. Special collection on mobile mixed reality 2019 update. Res. Learn. Technol. 2020, 28, 1–5. [Google Scholar] [CrossRef]
- Collins, E.; Ditzel, L. Standardised Holographic Patients: An Evaluation of Their Role in Developing Clinical Reasoning Skills. Stud. Health Technol. Inform. 2021, 284, 148–152. [Google Scholar] [PubMed]
- Denholm, J.A.; Protopsaltis, A.; de Freitas, S. The Value of Team-Based Mixed-Reality (TBMR) Games in Higher Education. Int. J. Game-Based Learn. 2013, 3, 18–33. [Google Scholar] [CrossRef] [Green Version]
- Frost, J.; Delaney, L.; Fitzgerald, R. Exploring the application of mixed reality in Nurse education. BMJ Simul. Technol. Enhanc Learn. 2020, 6, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Habak, S.; Bennett, J.; Davies, A.; Davies, M.; Christensen, H.; Boydell, K.M. Edge of the Present: A Virtual Reality Tool to Cultivate Future Thinking, Positive Mood and Wellbeing. Int. J. Environ. Res. Public. Health 2021, 18, 140. [Google Scholar] [CrossRef]
- Kang, J.; Lindgren, R.; Planey, J. Exploring emergent features of student interaction within an embodied science learning simulation. Multimodal Technol. Interact. 2018, 2, 39. [Google Scholar] [CrossRef] [Green Version]
- Lertbumroongchai, K.; Saraubon, K.; Nilsook, P. The social-emotional learning process to develop practicing skills for hands-on students. Int. J. Inf. Educ. Technol. 2020, 10, 597–602. [Google Scholar] [CrossRef]
- Martinez-Cerda, J.; Torrent-Sellens, J.; Gonzalez-Gonzalez, I. Promoting collaborative skills in online university: Comparing effects of games, mixed reality, social media, and other tools for ICT-supported pedagogical practices. Behav. Inf. Technol. 2018, 37, 1055–1071. [Google Scholar] [CrossRef]
- Rushton, M.A.; Drumm, I.A.; Campion, S.P.; O’Hare, J.J. The Use of Immersive and Virtual Reality Technologies to Enable Nursing Students to Experience Scenario-Based, Basic Life Support Training-Exploring the Impact on Confidence and Skills. Comput. Inform. Nurs. 2020, 38, 281–293. [Google Scholar] [CrossRef]
- Sonntag, D.; Bodensiek, O. How mixed reality shifts visual attention and success in experimental problem solving. Phys. Rev. Phys. Educ. Res. 2022, 18, 023101. [Google Scholar] [CrossRef]
- Stretton, T.; Cochrane, T.; Narayan, V. Exploring mobile mixed reality in healthcare higher education: A systematic review. Res. Learn. Technol. 2018, 26, 2131. [Google Scholar] [CrossRef] [Green Version]
- Tang, Y.M.; Au, K.M.; Lau, H.C.W.; Ho, G.T.S.; Wu, C.H. Evaluating the effectiveness of learning design with mixed reality (MR) in higher education. Virtual Real. 2020, 24, 797–807. [Google Scholar] [CrossRef]
- Taylor, S.; Soneji, S. Bioinformatics and the Metaverse: Are We Ready? Front. Bioinform 2022, 2, 863676. [Google Scholar] [CrossRef]
- Usmani, S.S.; Sharath, M.; Mehendale, M. Future of mental health in the metaverse. Gen. Psychiatr. 2022, 35, e100825. [Google Scholar] [CrossRef] [PubMed]
- Chuah, J.H.; Lok, B.; Black, E. Applying mixed reality to simulate vulnerable populations for practicing clinical communication skills. IEEE Trans. Vis. Comput. Graph. 2013, 19, 539–546. [Google Scholar] [CrossRef]
- Essmiller, K.; Asino, T.I.; Ibukun, A.; Alvarado-Albertorio, F.; Chaivisit, S.; Do, T.; Kim, Y. Exploring mixed reality based on self-efficacy and motivation of user. Res. Learn. Technol. 2020, 28, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Frost, J.; Chipchase, L.; Kecskes, Z.; D’Cunha, N.M.; Fitzgerald, R. Research in Brief: Exploring Perceptions of Needs for the Same Patient Across Disciplines Using Mixed Reality: A Pilot Study. Clin Simul. Nurs 2020, 43, 21–25. [Google Scholar] [CrossRef]
- Murphy, K.M. Working with Avatars and High Schoolers to Teach Qualitative Methods to Undergraduates. LEARNing Landsc. 2019, 12, 183–203. [Google Scholar] [CrossRef]
- Na, H.; Park, S.; Dong, S.-Y. Mixed Reality-Based Interaction between Human and Virtual Cat for Mental Stress Management. Sensors 2022, 22, 1159. [Google Scholar] [CrossRef]
- Perryman, T.; Sandefur, C.; Morris, C.T. Developing Interpersonal and Counseling Skills Through Mixed-Reality Simulation in Communication Sciences and Disorders. Perspect. ASHA Spec. Interest Groups 2021, 6, 416–428. [Google Scholar] [CrossRef]
- Emmelkamp, P.M.; Meyerbröker, K. Virtual reality therapy in mental health. Annu. Rev. Clin. Psychol. 2021, 17, 495–519. [Google Scholar] [CrossRef]
- Cai, Y.; Cao, Q. When VR Serious Games Meet Special Needs Education; Gaming Media and Social Effects; Springer: Singapore, 2021. [Google Scholar] [CrossRef]
- Coorey, G.; Figtree, G.A.; Fletcher, D.F.; Snelson, V.J.; Vernon, S.T.; Winlaw, D.; Grieve, S.M.; McEwan, A.; Yang, J.Y.H.; Qian, P. The health digital twin to tackle cardiovascular disease—A review of an emerging interdisciplinary field. NPJ Digit. Med. 2022, 5, 126. [Google Scholar] [CrossRef]
- Franco, M.; Monfort, C.; Piñas-Mesa, A.; Rincon, E. Could Avatar Therapy Enhance Mental Health in Chronic Patients? A Systematic Review. Electronics 2021, 10, 2212. [Google Scholar] [CrossRef]
- Rheu, M.; Jang, Y.; Peng, W. Enhancing healthy behaviors through virtual self: A systematic review of health interventions using avatars. Games Health J. 2020, 9, 85–94. [Google Scholar] [CrossRef]
- Andrade, A.D.; Anam, R.; Karanam, C.; Downey, P.; Ruiz, J.G. An overactive bladder online self-management program with embedded avatars: A randomized controlled trial of efficacy. Urology 2015, 85, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, Y.K.; Hughes, L.; Baabdullah, A.M.; Ribeiro-Navarrete, S.; Giannakis, M.; Al-Debei, M.; Dennehy, D.; Metri, B.; Buhalis, D.; Cheung, C.M.K.; et al. Metaverse beyond the hype: Multidisciplinary perspectives on emerging challenges, opportunities, and agenda for research, practice and policy. Int. J. Inf. Manag. 2022, 66, 102542. [Google Scholar] [CrossRef]
- Merkx, C.; Nawijn, J. Virtual reality tourism experiences: Addiction and isolation. Tour. Manag. 2021, 87, 104394. [Google Scholar] [CrossRef]
- Gorman, T.E.; Gentile, D.A.; Green, C.S. Problem gaming: A short primer. Am. J. Play 2018, 10, 309. [Google Scholar] [PubMed]
- Viglialoro, R.M.; Condino, S.; Turini, G.; Carbone, M.; Ferrari, V.; Gesi, M. Augmented Reality, Mixed Reality, and Hybrid Approach in Healthcare Simulation: A Systematic Review. Appl. Sci. 2021, 11, 2338. [Google Scholar] [CrossRef]
- Ziker, C.; Truman, B.; Dodds, H. Cross reality (XR): Challenges and opportunities across the spectrum. Innov. Learn. Environ. STEM High. Educ. Oppor. Chall. Look. Forw. 2021, 55–77. [Google Scholar]


{kind=link}
| Study | Publication Year | Country | Study Design |
|---|---|---|---|
| Chuah et al. [60] | 2013 | USA | Quantitative |
| Essmiller et al. [61] | 2020 | USA | Quantitative |
| Frost et al. [62] | 2020 | Australia | Qualitative |
| Murphy. [63] | 2019 | USA | Qualitative |
| Na et al. [64] | 2022 | Korea | Quantitative |
| Perryman et al. [65] | 2021 | USA | Mixed method |
| Study | Study Aim | Sample Size (Mean Age) | College Degree | Mental Health-Related Variable Targeted |
|---|---|---|---|---|
| Chuah et al. [60] | To apply MR to simulate a pediatric developmental exam. | 22 (25.45) | Health professions students (ten participants were undergraduate nursing students, seven were medical students, three were pediatrics residents, one was a graduate nursing student, and one was a physician’s assistant student). | Interaction with a virtual patient (pediatrics) and parents. |
| Essmiller et al. [61] | How to facilitate instruction and practice with MR to mitigate cognitive load. | 63 (not provided) | Not provided. | Motivation and self-efficacy. |
| Frost et al. [62] | To explore the perceptions of need after a visual assessment of the same patient using MR. | 13 (not provided) | Medicine (n = 3), nursing (n = 6), occupational therapy (n = 2), and dietetics (n = 2), in their last six months of training to get their college degree. | Perceptions of a virtual patient’s needs. |
| Murphy. [63] | A seminar focusing on youth participatory action research (YPAR), to teach qualitative research using MR. | 15 (not provided) | Not provided. | Ability to interact with younger students, interviewing them, and applying these skills to better develop qualitative research. |
| Na et al. [64] | To analyze the effect of stress reduction using an MR-based HAI. | 30 (21.7) | Not provided. | Induced mental stress. |
| Perryman et al. [65] | To investigate whether MR enhanced perceived application of the content and increased confidence in specific clinician counseling skills. | 29 (not provided) | Communication sciences and disorders (CSD) who had completed one full year of undergraduate. | Ability to apply clinical and counseling skills (e.g., delivering difficult news, paraphrasing, and normalizing difficult emotions). |
| Study | Training Using MR | Useful to Acquire Knowledge | Useful as Training in New Skills |
|---|---|---|---|
| Chuah et al. [60] | Interaction with a virtual patient (pediatrics) and parents to examine the effect of the object interaction interface on perception of the virtual child as a real child. | Not provided | Yes |
| Essmiller et al. [61] | Using Microsoft HoloLens, via three different activities: (a) a 3D AR gamewhere players defend their homes from a robotic invasion (Roboraid); (b) a Microsoft tutorial on how to use the HoloLens and (c) freeplay, where the participants are free to examine any content from the HoloLens, to explore and observe the engagement of the participants in the assigned activities. | Not provided | No |
| Frost et al. [62] | Participants were asked to spend a maximum of 15 min immersed in an application that displayed a holographic patient (Holopatient.), via Microsoft Hololens: a head mounted wearable holographic headset which permits human-computer interaction within an MR environment. | Not provided | Yes |
| Murphy. [63] | A 10-min training session on the SHOWeD protocol through a photovoice discussion in a classroom of the Mursion. MR was used in the interaction with five avatars that simulated five eighth-grade students, diverse in personality. | Not provided | Yes |
| Na et al. [64] | A 3 min training session using MR, with virtual animals (cats), with gestures and voice commands, using HoloLens (1st generation). | Not provided | Yes |
| Perryman et al. [65] | Utilizing an office environment with adult avatars, to simulate a meeting between a student clinician and a patient. There were two challenges: (1), two parents were presenting with the lead participant in a post assessment meeting for their 4-year-old son who was exhibiting social communication delays, language deficits, and atypical behaviors; and (2) the same two parents returned for follow-up consultation where participants’ objectives were to plan for intervention. | Not provided | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rincon, E.; Rodriguez-Guidonet, I.; Andrade-Pino, P.; Monfort-Vinuesa, C. Mixed Reality in Undergraduate Mental Health Education: A Systematic Review. Electronics 2023, 12, 1019. https://doi.org/10.3390/electronics12041019
Rincon E, Rodriguez-Guidonet I, Andrade-Pino P, Monfort-Vinuesa C. Mixed Reality in Undergraduate Mental Health Education: A Systematic Review. Electronics. 2023; 12(4):1019. https://doi.org/10.3390/electronics12041019
Chicago/Turabian StyleRincon, Esther, Irene Rodriguez-Guidonet, Paula Andrade-Pino, and Carlos Monfort-Vinuesa. 2023. "Mixed Reality in Undergraduate Mental Health Education: A Systematic Review" Electronics 12, no. 4: 1019. https://doi.org/10.3390/electronics12041019