
Improving Humanization through Metaverse-Related Technologies: A Systematic Review
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. General Description
2.2. Selection Criteria
2.3. Outcomes
2.4. Search Methodology
2.5. Data Collection and Analysis
2.6. Data Extraction and Management
2.7. Quality of Included Studies
2.8. Statistical Analysis
3. Results
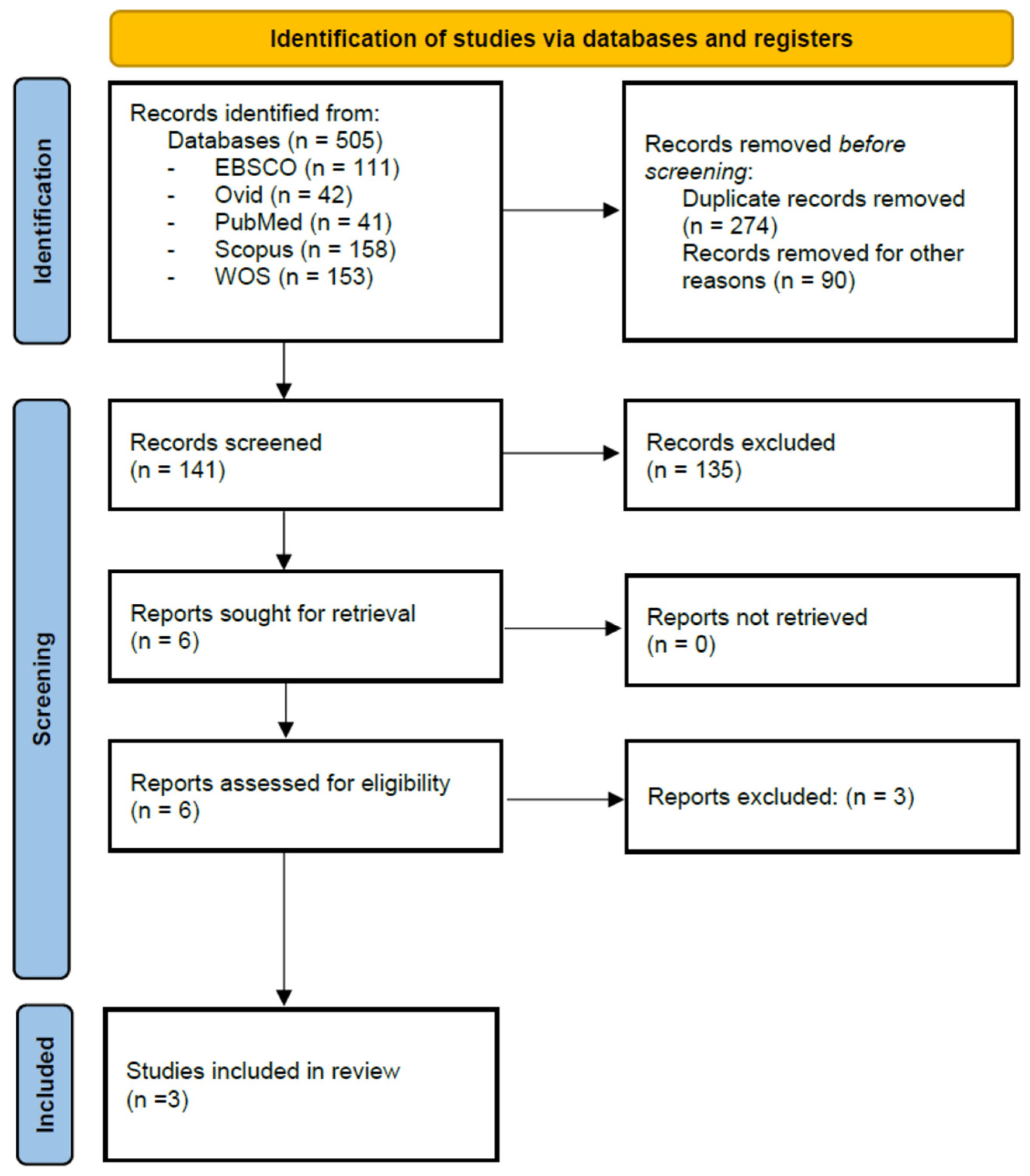
3.1. Study Selection and Inclusion
3.2. General Characteristics of the Studies Included
3.3. Assessment of the Methodological Quality of the Studies Included
3.4. Primary Outcomes
3.5. Secondary Outcomes
4. Discussion
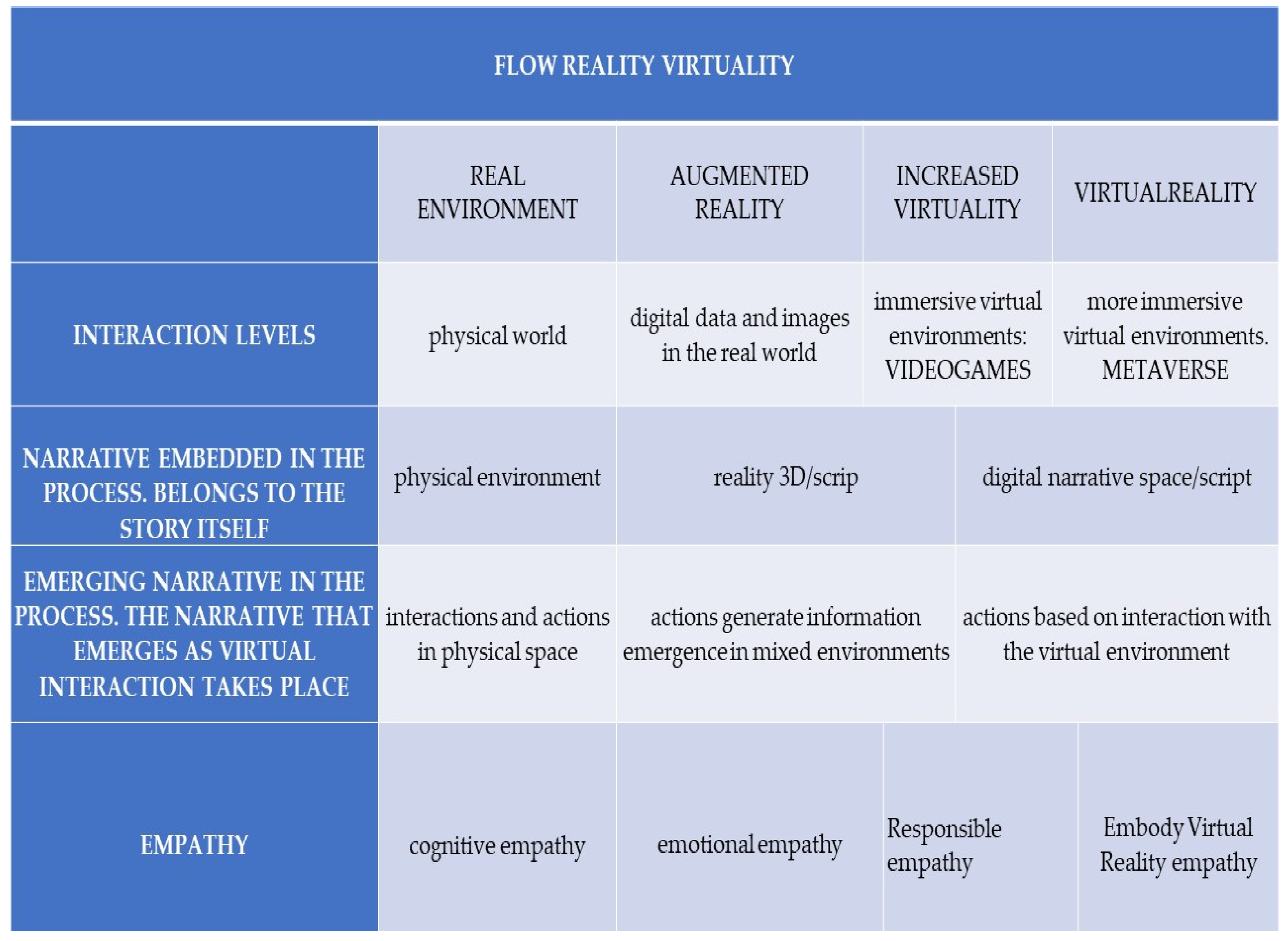
4.1. The Usefulness of Metaverse-Related Technologies in Enhancing Humanization Skills
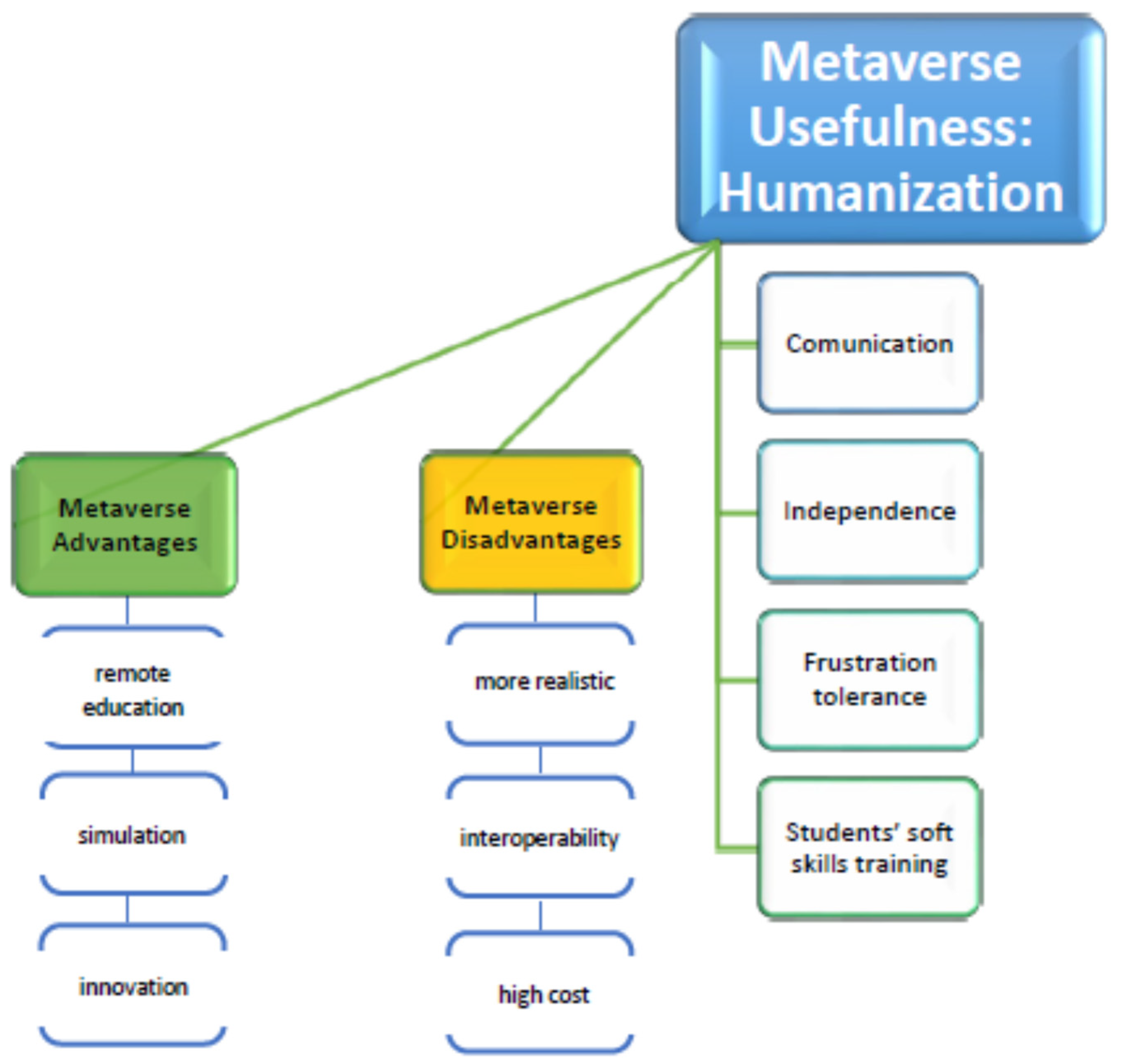
4.2. Advantages and Disadvantages of Metaverse-Related Technologies in Health Education
5. Conclusions
- (1)
- There is not sufficient empirical evidence to be able to confirm that Metaverse-related technologies are an effective type of technology to increase the acquisition of humanization skills in the healthcare sphere; result k of these studies focused on this topic;
- (2)
- Taking into account the different MR techniques developed with participants, numerous strengths and weaknesses should be addressed in order to successfully develop Metaverse-related strategies in healthcare education.
Limitations
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Umenai, T.; Wagner, M.; Page, L.; Faundes, A.; Rattner, D.; Dias, M.; Tyrrell, M.; Hotimsky, S.; Haneda, K.; Onuki, D.; et al. Conference agreement on the definition of humanization and humanized care. Int. J. Gynecol. Obstet. 2001, 75, S3–S4. [Google Scholar] [CrossRef]
- Lafaurie, M.; Perdomo, A.; Tocora, J.; González, M.C.; Barbosa, R.; Amaya, M.; Castelblanco, M.; Garzón, J.; Hincapié, S.; Huertas, L.; et al. La humanización en salud: Reflexiones de docentes, estudiantes y personal administrativo de una facultad de odontología. Rev. Salud Bosque 2018, 8, 97–105. [Google Scholar] [CrossRef]
- Casate, J.C.; Corrêa, A.K. A humanização do cuidado na formação dos profissionais de saúde nos cursos de graduação. Rev. Esc. Enferm. USP 2012, 46, 219–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busch, I.M.; Moretti, F.; Travaini, G.; Wu, A.W.; Rimondini, M. Humanization of Care: Key Elements Identified by Patients, Caregivers, and Healthcare Providers. A Systematic Review. Patient 2019, 12, 461–474. [Google Scholar] [CrossRef] [PubMed]
- Gálvez Herrer, M.; Gómez García, J.; Martín Delgado, M.; Ferrero Rodríguez, M.; Miembros del Proyecto HU-CI. Humanización de la Sanidad y Salud Laboral: Implicaciones, estado de la cuestión y propuesta del Proyecto HU-CI. Med. Segur. Trab. 2017, 63, 103–119. [Google Scholar]
- Pasche, D.; Passos, E.; Hennington, E. Cinco anos da política nacional de humanização: Trajetória de uma política pública. Ciênc. Saúde Coletiva 2015, 16, 4541–4548. [Google Scholar] [CrossRef] [Green Version]
- Starfield, B. Is Patient-Centered Care the Same as Person-Focused Care? Perm. J. 2011, 15, 63–69. [Google Scholar] [CrossRef] [Green Version]
- Frampton, S.B.; Guastello, S. Time to Embrace a New Patient-Centered Care Rallying Cry: “Why Not?”. Patient 2014, 7, 231–233. [Google Scholar] [CrossRef] [Green Version]
- van Mol, M.M.C.; Brackel, M.; Kompanje, E.J.O.; Gijsbers, L.; Nijkamp, M.D.; Girbes, A.R.J.; Bakker, J. Joined forces in person-centered care in the intensive care unit: A case report from the Netherlands. J. Compassionate Health Care 2016, 3, 5. [Google Scholar] [CrossRef] [Green Version]
- Bastos, S.; de Oliveira, H.; Moreira, M.; Azevedo, L. Soft-Digital Skills in Higher Education Curricula: HEI’s 5.0. In Proceedings of the 18th European Conference on e-Learning, Copenhagen, Denmark, 7–8 November 2019. [Google Scholar] [CrossRef]
- Prades, J.; Coll-Ortega, C.; Dal Lago, L.; Goffin, K.; Javor, E.; Lombardo, C.; de Munter, J.; Ponce, J.; Regge, D.; Salazar, R.; et al. Use of information and communication technologies (ICTs) in cancer multidisciplinary team meetings: An explorative study based on EU healthcare professionals. BMJ Open 2022, 12, e051181. [Google Scholar] [CrossRef]
- Cabero-Almenara, J.; Valencia-Ortiz, R.; Llorente-Cejudo, C. Ecosistemas de tecnologías emergentes: Realidad aumentada, virtual y mixta. Tecnol. Cienc. Educ. 2022, 23, 7–22. [Google Scholar] [CrossRef]
- Yang, Y.; Siau, K.; Xie, W.; Sun, Y. Smart Health: Intelligent Healthcare Systemsin the Metaverse, Artificial Intelligence, and Data Science Era. JOEUC 2022, 34, 1–14. [Google Scholar] [CrossRef]
- Almarzouqi, A.; Aburayya, A.; Salloum, S.A. Prediction of User’s Intention to Use Metaverse System in Medical Education: A Hybrid SEM-ML Learning Approach. IEEE Access 2022, 10, 43421–43434. [Google Scholar] [CrossRef]
- Tlili, A.; Huang, R.; Shehata, B.; Liu, D.; Zhao, J.; Metwally, A.H.S.; Wang, H.; Denden, M.; Bozkurt, A.; Lee, L.-H.; et al. Is Metaverse in education a blessing or a curse: A combined content and bibliometric analysis. Smart Learn. Environ. 2022, 9, 24. [Google Scholar] [CrossRef]
- Kye, B.; Han, N.; Kim, E.; Park, Y.; Jo, S. Educational applications of metaverse: Possibilities and limitations. J. Educ. Eval. Health Prof. 2021, 18, 32. [Google Scholar] [CrossRef] [PubMed]
- Prasetyo, J. Masruroh the Future of Post-Covid-19 Health Services using Metaverse Technology. J. Nurs. Pract. 2022, 6, 93–99. [Google Scholar] [CrossRef]
- Andrews, A. Serious Games for Psychological Health Education. In Virtual and Mixed Reality; Shumaker, R., Ed.; Springer: Berlin/Heidelberg, Germany, 2011; Volume 6774, pp. 3–10. [Google Scholar] [CrossRef]
- Chan, S.; Cao, Q.; Chen, J.; Cai, Y. Evaluation of Serious Games for Special Needs Education. In When VR Serious Games Meet Special Needs Education; Cai, Y., Cao, Q., Eds.; Springer: Singapore, 2021; pp. 113–127. [Google Scholar] [CrossRef]
- Li, Y.; Li, X.; Zhu, D.; Guo, H. Cultivation of the Students’ Critical Thinking Ability in Numerical Control Machining Course Based on the Virtual Simulation System Teaching Method. IEEE Access 2020, 8, 173584–173598. [Google Scholar] [CrossRef]
- Zwart, D.; van Luit, J.E.H.; Goei, S.L. Empowering Vocational Math Teachers by Using Digital Learning Material (DLM) with Workplace Assignments. In Simulation and Serious Games for Education. Gaming Media and Social Effects; Cai, Y., Goei, S., Trooster, W., Eds.; Springer: Singapore, 2017; pp. 81–97. [Google Scholar] [CrossRef]
- Viteri, F. EDUCACIÓN Y TECNOLOGÍA: Visión filosófica de la tecnología hasta llegar a su humanización por medio de la educación. Sophia Colección Filos. Educ. 2011, 11, 175–196. Available online: https://dspace.ups.edu.ec/handle/123456789/9392 (accessed on 30 December 2022).
- López, J. Educación en el Metaverso: ¿cómo Serían las Clases en el Mundo Virtual y qué Beneficios Tendría? La Republica. 12 November 2022. Available online: https://login.bucm.idm.oclc.org/login?url=https://www.proquest.com/newspapers/educación-en-el-metaverso-cómo-serían-las-clases/docview/2735718164/se2?accountid=14514 (accessed on 30 December 2022).
- Thomason, J. Metaverse, token economies, and non-communicable diseases. Glob. Health J. 2022, 6, 164–167. [Google Scholar] [CrossRef]
- Farjami, S.; Nakahira, K.; Fukumura, Y.; Taguchi, R.; Fukumura, Y. W-02 problem-based learning for materials science education in metaverse. JSEE Ann. Conf. Int. Sess. Proc. 2011, 20–23. [Google Scholar] [CrossRef]
- Fox, J.; Ahn, S.J.; Janssen, J.H.; Yeykelis, L.; Segovia, K.Y.; Bailenson, J.N. Avatars Versus Agents: A Meta-Analysis Quantifying the Effect of Agency on Social Influence. Hum. –Comput. Interact. 2014, 30, 401–432. [Google Scholar] [CrossRef]
- Chase, C.C.; Chin, D.B.; Oppezzo, M.A.; Schwartz, D.L. Teachable Agents and the Protégé Effect: Increasing the Effort Towards Learning. J. Sci. Educ. Technol. 2009, 18, 334–352. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G. Practical Statistics for Medical Research; CRC Press: Boca Raton, FL, USA, 1990. [Google Scholar]
- Pluye, P.; Gagnon, M.; Griffiths, F.; Johnson-Lafleur, J. A scoring system for appraising mixed methods research, and concomitantly appraising qualitative, quantitative and mixed methods primary studies in mixed studies reviews. Int. J. Nurs. Stud. 2009, 46, 529–546. [Google Scholar] [CrossRef] [PubMed]
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.; Griffiths, F.; Nicolau, B. Mixed methods appraisal tool (MMAT), version 2018. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Silva, A.B.; De Assumpção, A.M.B.; Filha, I.G.D.A.; Regadas, C.T.; De Castro, M.C.; Silva, C.R.A.; Assumpção, M.R.; Dos Santos, R.C.B.; Silvério, T.O.; Dos Santos, P.B.; et al. Cross-cultural adaptation of the zero mothers die (ZMD-app) in Brazil: Contributing to digital health with the approach on care centred for E-pregnant woman. Rev. Bras. Saude Matern. Infantil. 2019, 19, 751–762. [Google Scholar] [CrossRef] [Green Version]
- Burrai, F.; Othman, S.; Brioni, E.; Micheluzzi, V.; Luppi, M.; Apuzzo, L.; Delli Zotti, G.B.; La Manna, G. Effects of Virtual Reality in Patients Undergoing Dialysis: Study Protocol. Holist. Nurs. Pract. 2019, 33, 327–337. [Google Scholar] [CrossRef]
- Caballero-Galilea, M.; Martínez-Miguel, E.; Gonzalo, J.C.F.; Abbad, R.S.d.l.C.; Alonso, M.R. Digitized Prenatal Newsletter: Impact on Obstetric Patient Satisfaction and Loyalty. Int. J. Environ. Res. Public Health 2022, 19, 2773. [Google Scholar] [CrossRef]
- Castillo-Parra, S.; Bacigalupo-Araya, J.; García-Vallejos, G.; Ramírez-Lazcano, C.; Collado-Quezada, C.; Lorca-Nachar, A. Teachers’ voices seeking humanized teaching in nursing: Virtual experiences during the pandemic. Texto E Contexto Enferm. 2022, 31, e20210207. [Google Scholar] [CrossRef]
- Hallqvist, J. The making of a professional digital caregiver: Personalisation and friendliness as practices of humanisation. Med. Humanit. 2022, 48, 347–356. [Google Scholar] [CrossRef]
- Jiménez-Rodríguez, D.; Pérez-Heredia, M.; Jurado, M.D.M.M.; Pérez-Fuentes, M.D.C.; Arrogante, O. Improving Humanization Skills through Simulation-Based Computers Using Simulated Nursing Video Consultations. Healthcare 2021, 10, 37. [Google Scholar] [CrossRef] [PubMed]
- Todres, L.; Galvin, K.T.; Holloway, I. The humanization of healthcare: A value framework for qualitative research. Int. J. Qual. Stud. Health Well-Being 2009, 4, 68–77. [Google Scholar] [CrossRef]
- Shin, E.; Kim, J.H. The Metaverse and Video Games: Merging Media to Improve Soft Skills Training. J. Internet Comput. Serv. 2021, 23, 69–76. [Google Scholar] [CrossRef]
- Yimsawat, C.; Mangkhang, C.; Phuwanatwichit, T.; Anansuchatkul, B. An instructional innovation to strengthen comprehensive humanization for higher education students: Soft Skills for the digital society. J. Educ. Naresuan Univ. 2022, 24, 15–24. [Google Scholar] [CrossRef]
- Thomason, J. MetaHealth-How will the Metaverse Change Health Care? J. Metaverse 2021, 1, 13–16. [Google Scholar]
- Wang, G.; Badal, A.; Jia, X.; Maltz, J.S.; Mueller, K.; Myers, K.J.; Niu, C.; Vannier, M.; Yan, P.; Yu, Z.; et al. Development of metaverse for intelligent healthcare. Nat. Mach. Intell. 2022, 4, 922–929. [Google Scholar] [CrossRef]
- Ryan, G.V.; Callaghan, S.; Rafferty, A.; Higgins, M.F.; Mangina, E.; McAuliffe, F. Learning Outcomes of Immersive Technologies in Health Care Student Education: Systematic Review of the Literature. J. Med. Internet Res. 2022, 24, e30082. [Google Scholar] [CrossRef] [PubMed]
- Brunzini, A.; Papetti, A.; Messi, D.; Germani, M. A comprehensive method to design and assess mixed reality simulations. Virtual Real. 2022, 26, 1257–1275. [Google Scholar] [CrossRef]
- Liang, C.-J.; Start, C.; Boley, H.; Kamat, V.R.; Menassa, C.C.; Aebersold, M. Enhancing stroke assessment simulation experience in clinical training using augmented reality. Virtual Real. 2020, 25, 575–584. [Google Scholar] [CrossRef]
- Gerup, J.; Soerensen, C.B.; Dieckmann, P. Augmented reality and mixed reality for healthcare education beyond surgery: An integrative review. Int. J. Med. Educ. 2020, 11, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Perryman, T.; Sandefur, C.; Morris, C.T. Developing Interpersonal and Counseling Skills Through Mixed-Reality Simulation in Communication Sciences and Disorders. Perspect. ASHA Spéc. Interes. Groups 2021, 6, 416–428. [Google Scholar] [CrossRef]
- Al-Tikriti, M.; Al-Aubidy, K. Embedding Mixed-Reality Laboratories into E-Learning Systems for Engineering Education. J. Educ. Technol. 2013, 9, 25–35. [Google Scholar] [CrossRef]
- Car, J.; Carlstedt-Duke, J.; Car, L.T.; Posadzki, P.; Whiting, P.; Zary, N.; Atun, R.; Majeed, A.; Campbell, J. Digital Health Education Collaboration Digital education in health professions: The need for overarching evidence synthesis. J. Med. Internet Res. 2019, 21, e12913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baratz, G.; Sridharan, P.S.; Yong, V.; Tatsuoka, C.; Griswold, M.A.; Wish-Baratz, S. Comparing learning retention in medical students using mixed-reality to supplement dissection: A preliminary study. Int. J. Med. Educ. 2022, 13, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Coorey, G.; Figtree, G.A.; Fletcher, D.F.; Snelson, V.J.; Vernon, S.T.; Winlaw, D.; Grieve, S.M.; McEwan, A.; Yang, J.Y.H.; Qian, P. The health digital twin to tackle cardiovascular disease—A review of an emerging interdisciplinary field. NPJ Digit. Med. 2022, 5, 126. [Google Scholar] [CrossRef] [PubMed]
- Franco, M.; Monfort, C.; Piñas-Mesa, A.; Rincon, E. Could Avatar Therapy Enhance Mental Health in Chronic Patients? A Systematic Review. Electronics 2021, 10, 2212. [Google Scholar] [CrossRef]
- Coll, M.P.; Viding, E.; Rütgen, M.; Silani, G.; Lamm, C.; Catmur, C.; Bird, G. Are we really measuring empathy? Proposal for a new measurement framework. Neurosci. Biobehav. Rev. 2017, 83, 132–139. [Google Scholar] [CrossRef] [Green Version]
- Suazo, I.; Pérez-Fuentes, M.D.C.; Jurado, M.D.M.M.; Martínez, M.; Márquez, M.D.M.S.; Martín, A.B.B.; Sisto, M.; Linares, J.J.G. Moral Sensitivity, Empathy and Prosocial Behavior: Implications for Humanization of Nursing Care. Int. J. Environ. Res. Public Health 2020, 17, 8914. [Google Scholar] [CrossRef]
- Jolliffe, D.; Farrington, D.P. Development and validation of the Basic Empathy Scale. J. Adolesc. 2006, 29, 589–611. [Google Scholar] [CrossRef]
- Jo, H.; Kim, S. Moral Sensitivity, Empathy and Perceived Ethical Climate of Psychiatric Nurses Working in the National Mental Hospitals. J. Korean Acad. Psychiatr. Ment. Health Nurs. 2017, 26, 204–215. [Google Scholar] [CrossRef] [Green Version]
- Wong, A.M.F. Beyond burnout: Looking deeply into physician distress. Can. J. Ophthalmol. 2020, 55, 7–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubio-Tamayo, J.L.; Gértrudix Barrio, M. Realidad Virtual (HMD) e Interacción desde la Perspectiva de la Construcción Narrativa y la Comunicación: Propuesta Taxonómica. Econ. Digit. Impacto Medios 2016, 14, 1–24. [Google Scholar] [CrossRef] [Green Version]
- Milgram, P.; Kishino, F. A Taxonomy of Mixed Reality Visual Displays. IEICE Trans. Inf. Syst. 1994, 12, 1321–1329. Available online: http://vered.rose.utoronto.ca/people/paul_dir/IEICE94/ieice.htm (accessed on 30 December 2022).
- Hindmarsh, J.; Fraser, M.; Heath, C.; Benford, S. Virtually Missing the Point: Configuring CVEs for Object-Focused Interaction Collaborative Virtual Environments: Digital Places and Spaces for Interaction; Springer: London, UK, 2001. [Google Scholar] [CrossRef] [Green Version]
- Blasco, P. Literature and movies for medical students. Fam. Med. 2001, 33, 426–428. [Google Scholar] [PubMed]
- Mejía-Rivera, O. Literature and cinema in the training of doctors and medical humanities. Acta Med. Colomb. 2019, 44, 25–29. [Google Scholar] [CrossRef] [Green Version]
- Darbyshire, D.; Baker, P. A systematic review and thematic analysis of cinema in medical education. Med. Humanit. 2012, 38, 28–33. [Google Scholar] [CrossRef]
- Gorin, V. From Empathy to Shame: The Use of Virtual Reality by Humanitarian Organisations. In Making Humanitarian Crises. Palgrave Studies in the History of Emotions; Edgar, B.L., Gorin, V., Martín-Moruno, D., Eds.; Palgrave Macmillan: Cham, Switzerlasnd, 2022. [Google Scholar] [CrossRef]
- Bertrand, P.; Guegan, J.; Robieux, L.; McCall, C.A.; Zenasni, F. Learning Empathy Through Virtual Reality: Multiple Strategies for Training Empathy-Related Abilities Using Body Ownership Illusions in Embodied Virtual Reality. Front. Robot. AI 2018, 5, 26. [Google Scholar] [CrossRef] [Green Version]
- Petkova, V.I.; Ehrsson, H.H. If I were you: Perceptual illusion of body swapping. PLoS ONE 2008, 3, e3832. [Google Scholar] [CrossRef] [Green Version]
- Maselli, A.; Slater, M. The building blocks of the full body ownership illusion. Front. Hum. Neurosci. 2013, 7, 83. [Google Scholar] [CrossRef] [Green Version]
- Chuah, J.H.; Lok, B.; Black, E. Applying mixed reality to simulate vulnerable populations for practicing clinical communication skills. IEEE Trans. Vis. Comput. Graph. 2013, 19, 539–546. [Google Scholar] [CrossRef]
- Viglialoro, R.M.; Condino, S.; Turini, G.; Carbone, M.; Ferrari, V.; Gesi, M. Augmented Reality, Mixed Reality, and Hybrid Approach in Healthcare Simulation: A Systematic Review. Appl. Sci. 2021, 11, 2338. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Publication Year | Country | Study Design |
|---|---|---|---|
| Castillo-Parra et al. [35] | 2022 | Chile | Qualitative |
| Hallqvist [36] | 2022 | Sweden | Qualitative |
| Jiménez-Rodríguez et al. [37] | 2021 | Spain | Mixed Methods |
| Study | Study Aim | Sample Size (Mean Age) | Targeted Participants |
|---|---|---|---|
| Castillo-Parra et al. [35] | To describe the experience of implementing the online training labeled “Humanization of the training processes in nursing, care for all”, as well as to analyze their interventions in the online forum. | 12 (Not provided) | Professors from a nursing school |
| Hallqvist [36] | To examine how a digital caregiver is humanized through the health-enhancing approaches of personalization and friendliness for use in older patients. | Not provided/Not provided | Researchers from computing science fields and researchers within occupational therapy and nursing fields |
| Jiménez-Rodríguez et al. [37] | To examine the effects of virtual simulation-based training on developing and cultivating humanization abilities in undergraduate nursing students. | 60 (23.83) | 3rd-year students, degree in nursing |
| Study | Training Using Metaverse-Related Technologies | Useful in Enhancing Humanization Skills |
|---|---|---|
| Castillo-Parra et al. [35] | Six case studies concern virtual training, supported by the reading of texts, reviews of web pages, audiovisual materials, and simulated situations, encouraging debate and observations in the forum. | Not provided |
| Hallqvist [36] | Different types of events, lasting a total of 50 h, such as a user study with two researchers and two user study participants, meetings, seminars, public events (lectures, theme days), and social events. | Not provided |
| Jiménez-Rodríguez et al. [37] | A virtual platform of online video conferences provided by the university (Blackboard Collaborate Launcher TM) was used to develop six simulated scenarios focusing on basic healthcare at patients’ homes. | Not provided |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonzalez-Moreno, M.; Andrade-Pino, P.; Monfort-Vinuesa, C.; Piñas-Mesa, A.; Rincon, E. Improving Humanization through Metaverse-Related Technologies: A Systematic Review. Electronics 2023, 12, 1727. https://doi.org/10.3390/electronics12071727
Gonzalez-Moreno M, Andrade-Pino P, Monfort-Vinuesa C, Piñas-Mesa A, Rincon E. Improving Humanization through Metaverse-Related Technologies: A Systematic Review. Electronics. 2023; 12(7):1727. https://doi.org/10.3390/electronics12071727
Chicago/Turabian StyleGonzalez-Moreno, Maria, Paula Andrade-Pino, Carlos Monfort-Vinuesa, Antonio Piñas-Mesa, and Esther Rincon. 2023. "Improving Humanization through Metaverse-Related Technologies: A Systematic Review" Electronics 12, no. 7: 1727. https://doi.org/10.3390/electronics12071727