
An Integrated Support System for People with Intellectual Disability

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Related Work
2.1. Integrated Platforms
2.2. Mobile Sensor-Based Applications and Wearable Technologies
2.3. Smartphone Applications
- Soy Cappaz [53] is a mobile application for IID, available on Android worldwide in English and Spanish. It displays an opening screen with four main sections: (a) My Calendar, (b) Where Am I?, (c) My Tasks, and (d) I Need Help. The application helps with work tasks, answers questions, and provides guidance. It is also useful for daily activities such as using a microwave or catching a bus.
- MindMate [56] is an application designed to support individuals living with dementia and their caregivers. It offers features such as cognitive exercises, reminders, and mood tracking. The application also provides access to articles and information related to dementia care.
- MemoryWell [57] is a digital platform that helps create life stories for individuals with dementia. Caregivers and family members can use the application to build personalized narratives and share them with healthcare professionals to improve patient-centered care.
- Alzheimer’s Society’s Talking Point [58] is an online community and mobile application that allows people affected by dementia to connect, share their experiences, and seek support from others in similar situations.
- Elder 411 [59] is an application designed to provide practical advice and tips for caregivers of individuals with dementia. It covers a wide range of topics, including communication strategies, safety measures, and resources for additional support.
- Timeless [60] is an application that offers reminiscence therapy to people with dementia. It allows users to access a vast library of pictures, music, and videos from the past, which can stimulate memories and encourage conversations.
- CogniCare [61] is an application designed to help caregivers manage their daily responsibilities effectively. It provides tools for medication tracking, appointment reminders, and communication with other caregivers or family members.
- GPS SmartSole [62] has been designed for caregivers to monitor the location of individuals with dementia who wear a special shoe insole with a built-in GPS tracking system. It can be particularly useful in cases where the person tends to wander.
- PainChek [63] is an application designed to help healthcare professionals assess pain levels in individuals who may have difficulty communicating, such as those with advanced dementia.
- Puzzle Me [64] allows caregivers and their loved ones with dementia to solve puzzles together virtually, fostering a sense of engagement and connection.
3. Materials and Methods
3.1. Participating Users
- Reading ability: 18.8% very high, 12.5% above average, 6.3% below average, 31.3% very low, 31.3% incomplete
- Writing ability: 18.8% very high, 6.3% above average, 12.5% below average, 37.5% very low, 25% incomplete
- Speech: 12.5% very high, 31.3% above average, 25% below average, 25% very low, 6.3% incomplete
- Use of everyday vocabulary: 12.5% very high, 31.3% above average, 18.8% below average, 37.5% very low
- Self-care ability: 37.5% above average, 31.3% below average, 25% very low, 6.3% incomplete
- Assisted self-care skills: 25% very high, 31.3% above average, 37.5% below average, 6.3% very low
- Semi-skilled work: 6.3% above average, 18.8% below average, 25% very low, 50% incomplete
- Unskilled work without supervision: 18.8% above average, 25% below average, 37.5% very low, 18.8% incomplete
- Unskilled work with supervision: 18.8% very high, 25% above average, 31.3% below average, 18.8% very low, 6.3% incomplete
- Household chores: 25% above average, 31.3% below average, 37.5% very low, 6.3% incomplete
- Assisted household chores: 25% very high, 31.3% above average, 31.3% below average, 6.3% very low, 6.3% incomplete
- Autonomy: 12.5% very high, 25% above average, 25% below average, 31.3% very low, 6.3% incomplete
- Perception: 6.3% very high, 25% above average, 31.3% below average, 37.5% very low
- Cognitive abilities: 6.3% very high, 31.3% above average, 31.3% below average, 31.3% very low
- Concentration ability: 12.5% very high, 6.3% above average, 25% below average, 50% very low, 6.3% incomplete
- Memory: 12.5% very high, 6.3% above average, 31.3% below average, 43.8% very low, 6.3% incomplete
- Emotional maturity: 12.5% above average, 18.8% below average, 56.3% very low, 12.5% incomplete
- Motility: 18.8% very high, 43.8% above average, 25% below average, 6.3% very low, 6.3% incomplete
- Stereotyped movements: 25% above average, 25% below average, 31.3% very low, 18.8% incomplete
- Self-control: 50% below average, 50% very low
- Cooperation ability: 6.3% very high, 12.5% above average, 56.3% below average, 25% very low
- Participation in individual activities: 6.3% very high, 25% above average, 37.5% below average, 31.3% very low
- Participation in group activities: 6.3% very high, 18.8% above average, 56.3% below average, 6.3% very low, 12.5% incomplete
3.2. Content Recommendation and User Interfaces
- People with ID (adults and children), who are the key users of the recommendation system and may use it directly themselves, or with the aid of their relatives or/and caregivers;
- Their close relatives, i.e., parents and family, who have access to view their personal data registered to the system;
- The caregivers that represent the professional carers—occupational therapists who are allowed to access and modify the preferences, location, biomedical, and medication data of the people with ID that they have under their provision.
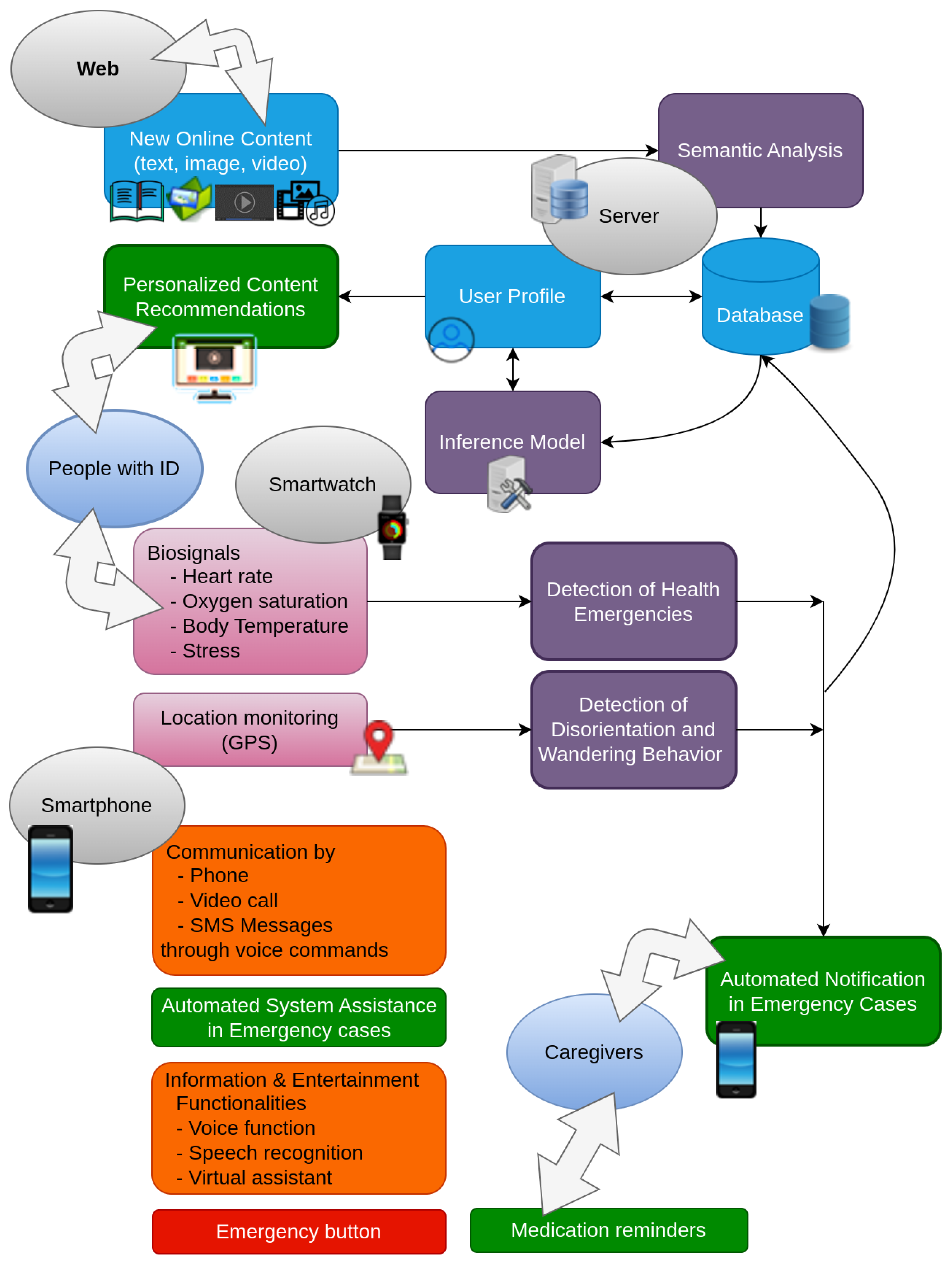
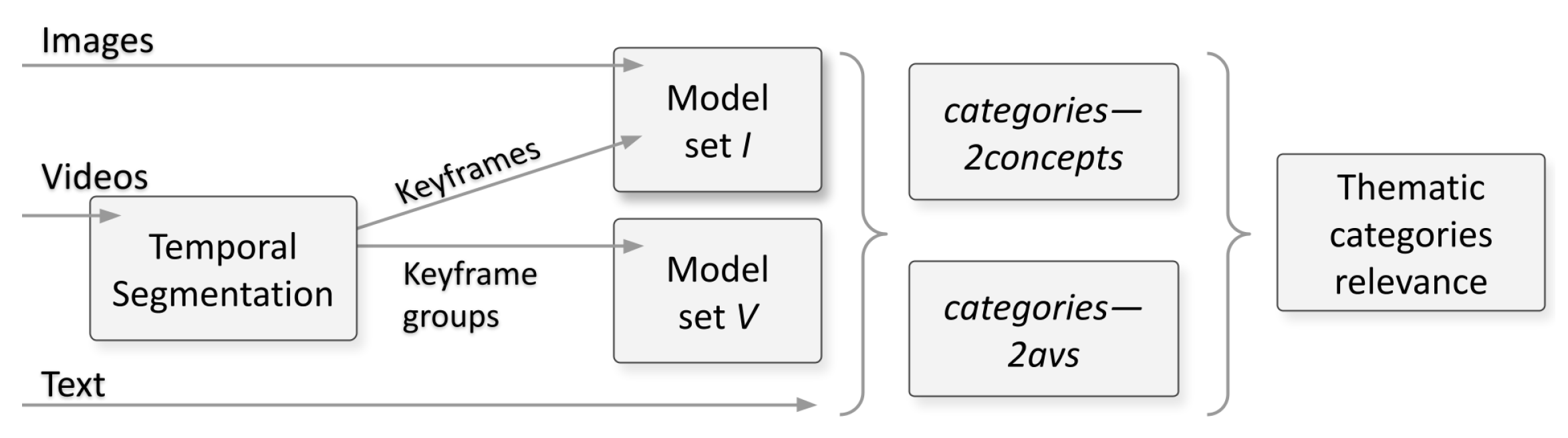
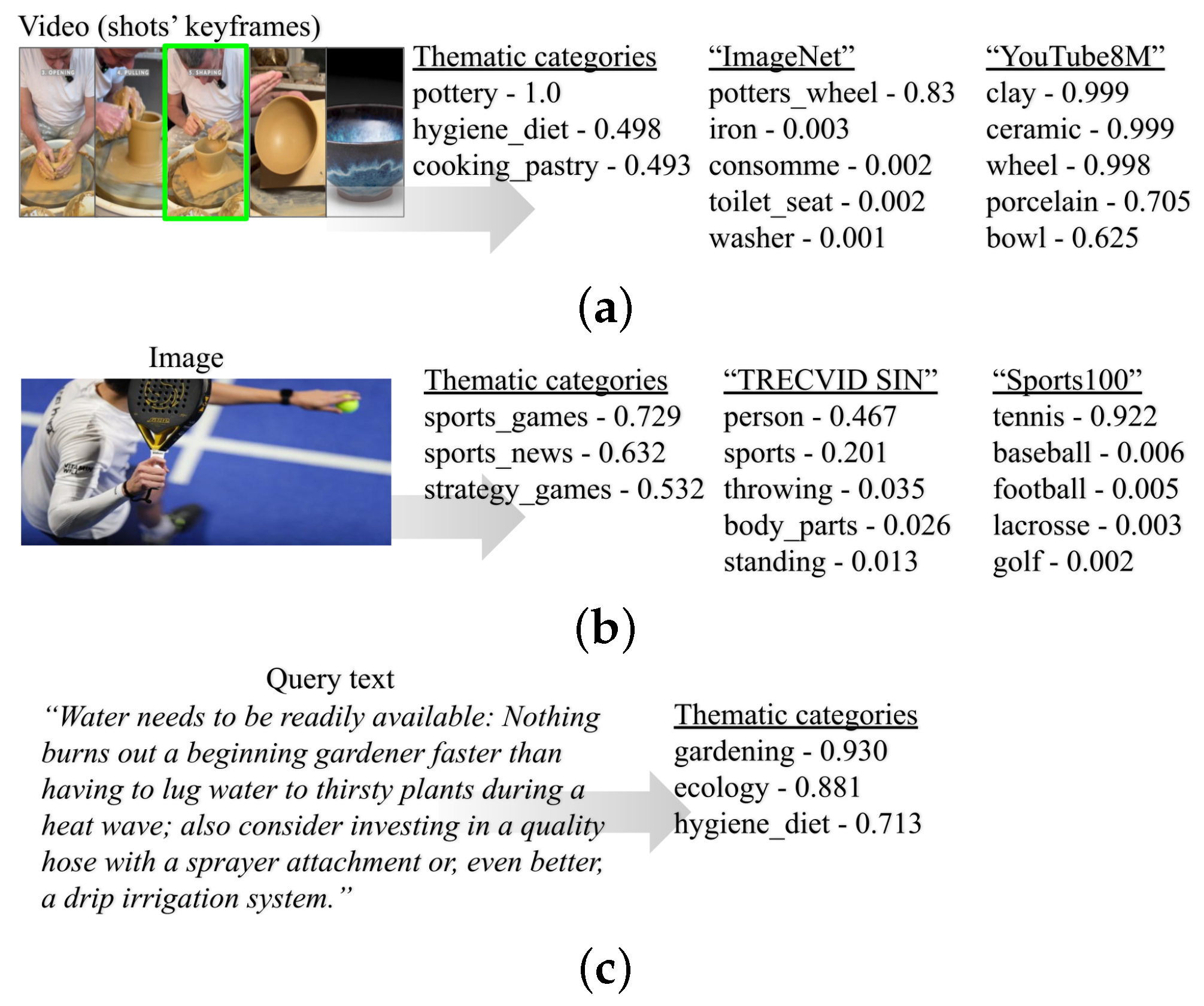
3.2.1. Content Semantic Analysis
3.2.2. Inference Model
- The approach of [74] deals with a mobile phone application, where the user is limited to a single screen, which does not constitute a web-based interface.
- The content concerns textual news items in Ref. [74], as opposed to our system, where the content is multi-modal and derived from several different sources.
- The most important difference concerns the target users, which, in our case, constitute IID that are characterized by special behaviors, e.g., they might have opened a webpage for a long time, without being concentrated on the content itself.
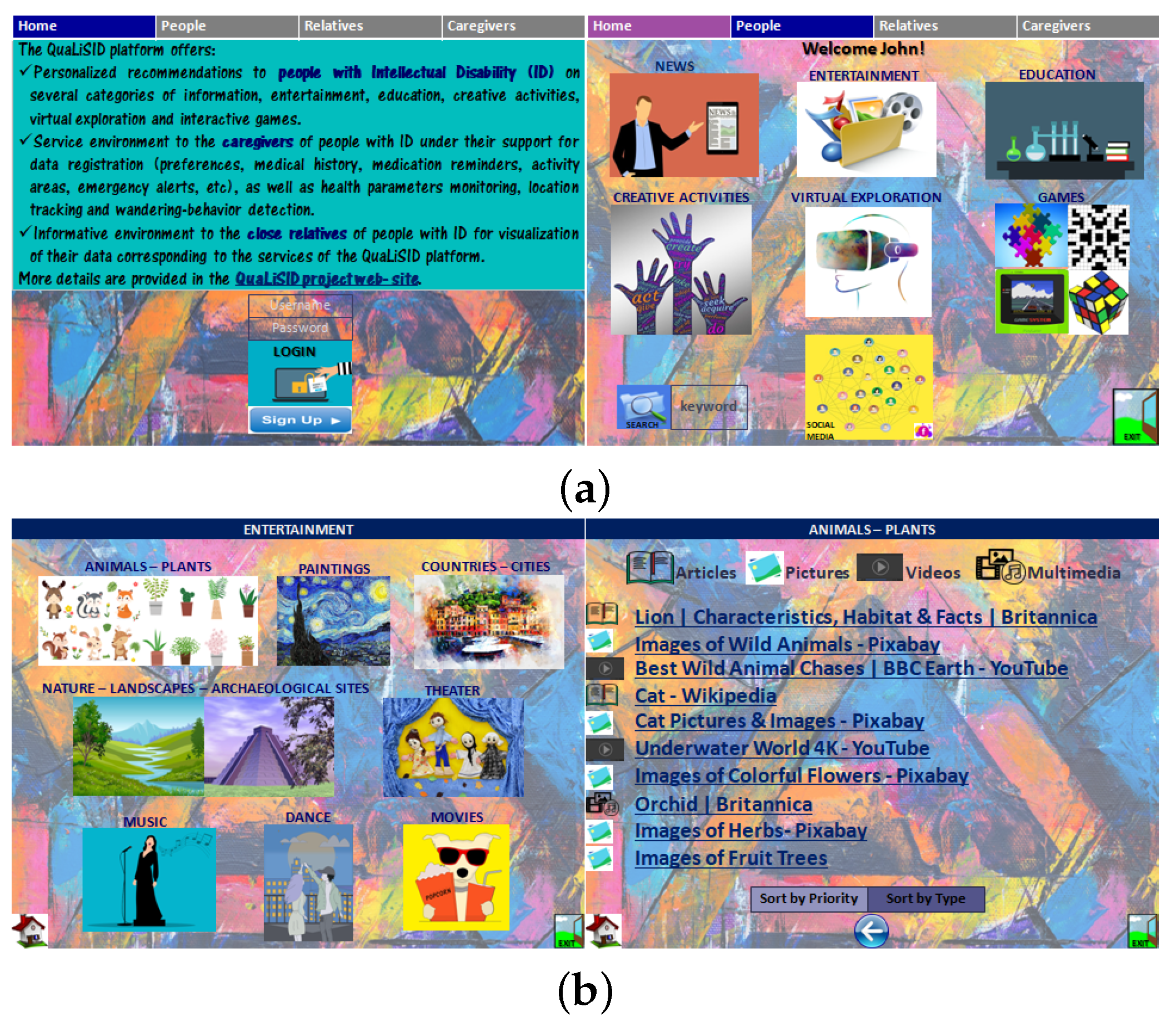
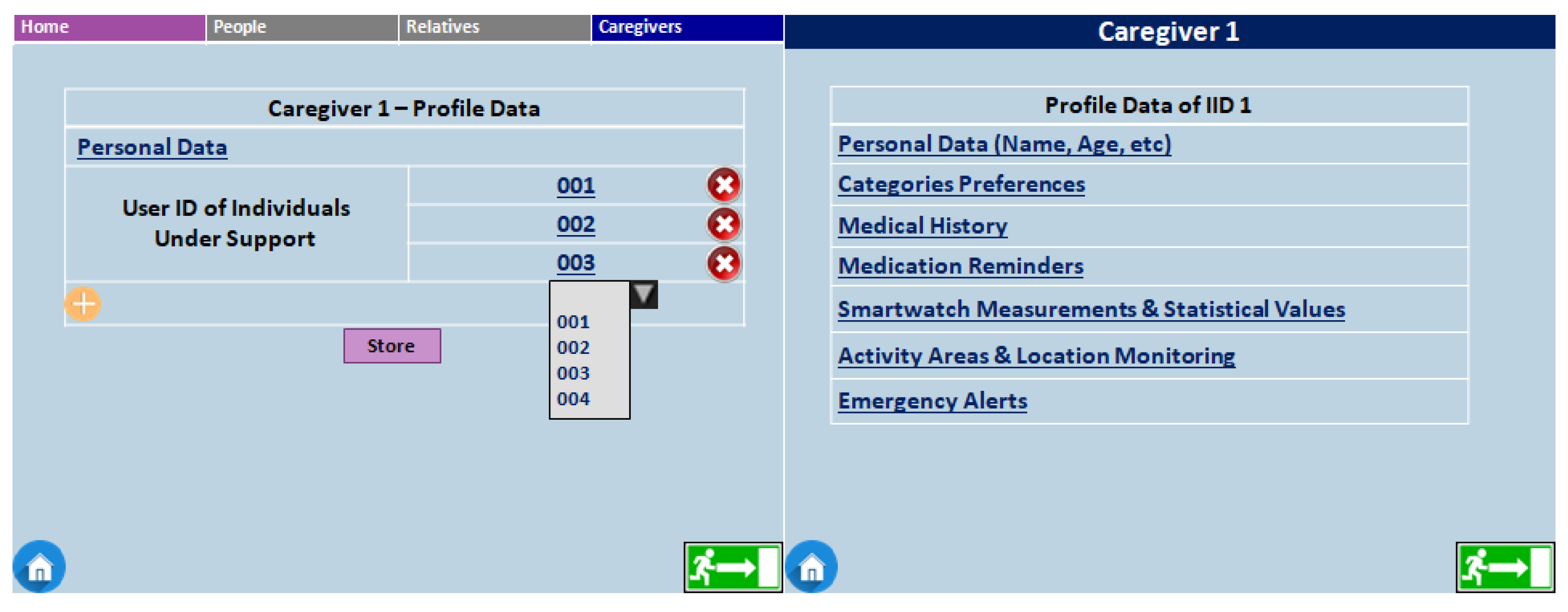
3.2.3. Web-Based User Interface
- The detailed preferences of the supported people, which the caregivers can anytime alter, in case they believe that the system’s automatic updates do not follow the actual individualized degrees of preference.
- The medical history, including reports and medical imaging modalities, which the therapists are allowed to (optionally) store in the system’s database.
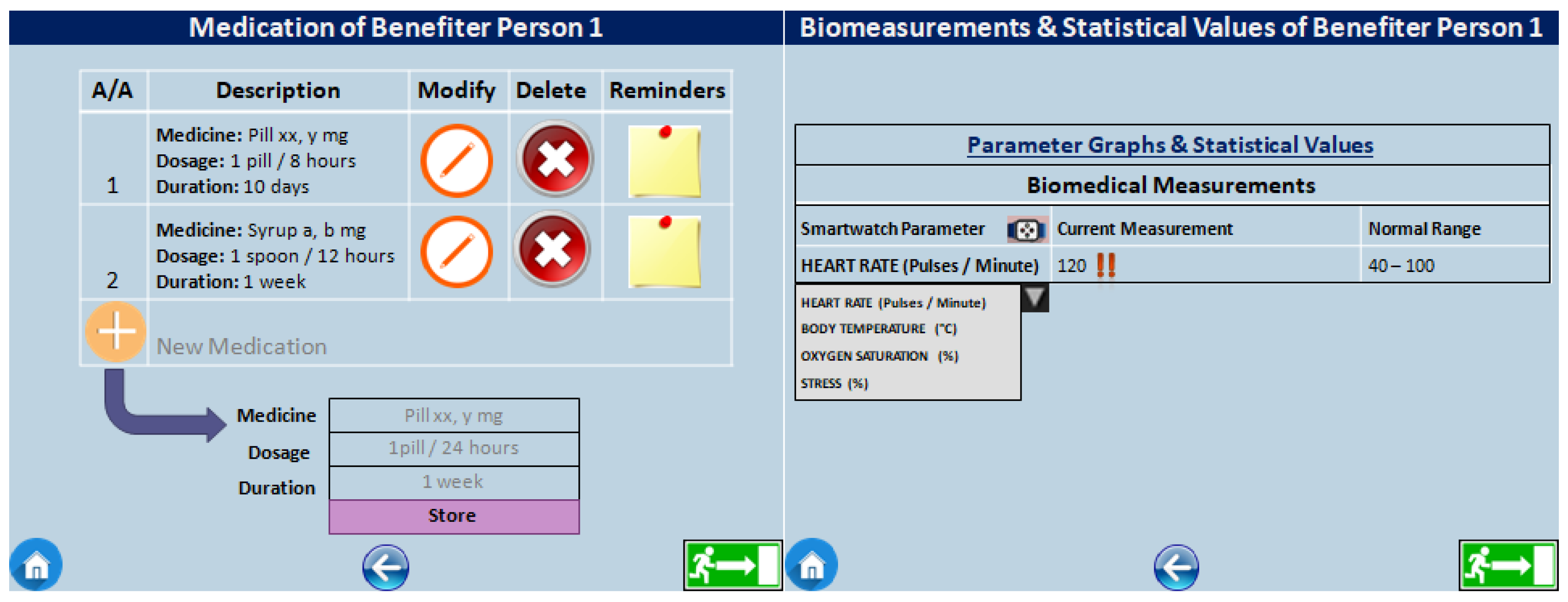
- The current medication of a specific benefiter with ID that the caregivers can store in the platform (Figure 6—left). In addition, through the button of ’Reminders’, they can specify as well as modify when/if it is necessary and schedule the time intervals of the corresponding reminders hat are sent to the people under their provision.
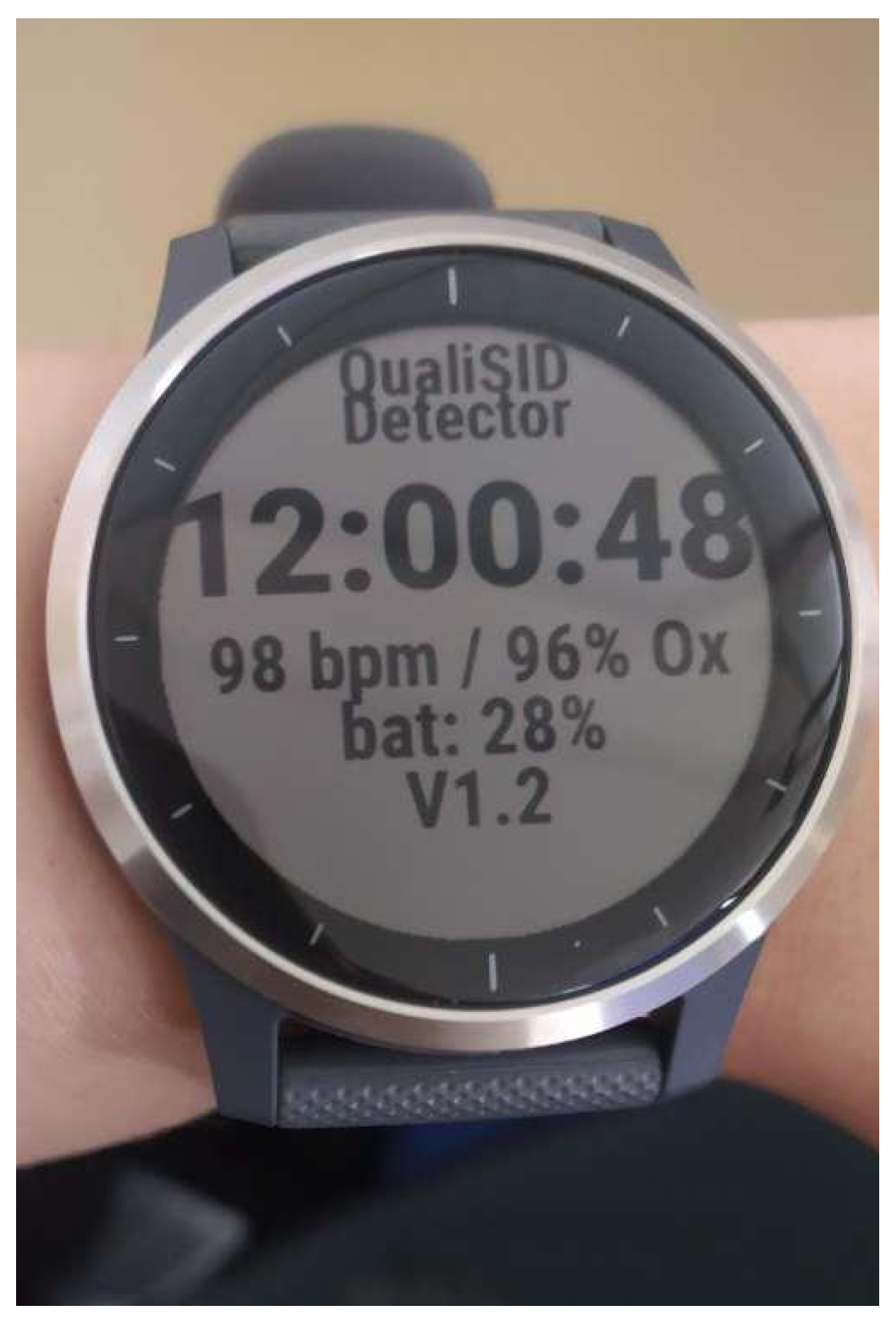
- The current values of biomeasurements monitored by the smartwatch, i.e., heart rate, oxygen saturation, body temperature, and stress level, which the carers can view at any time (Figure 6—right).
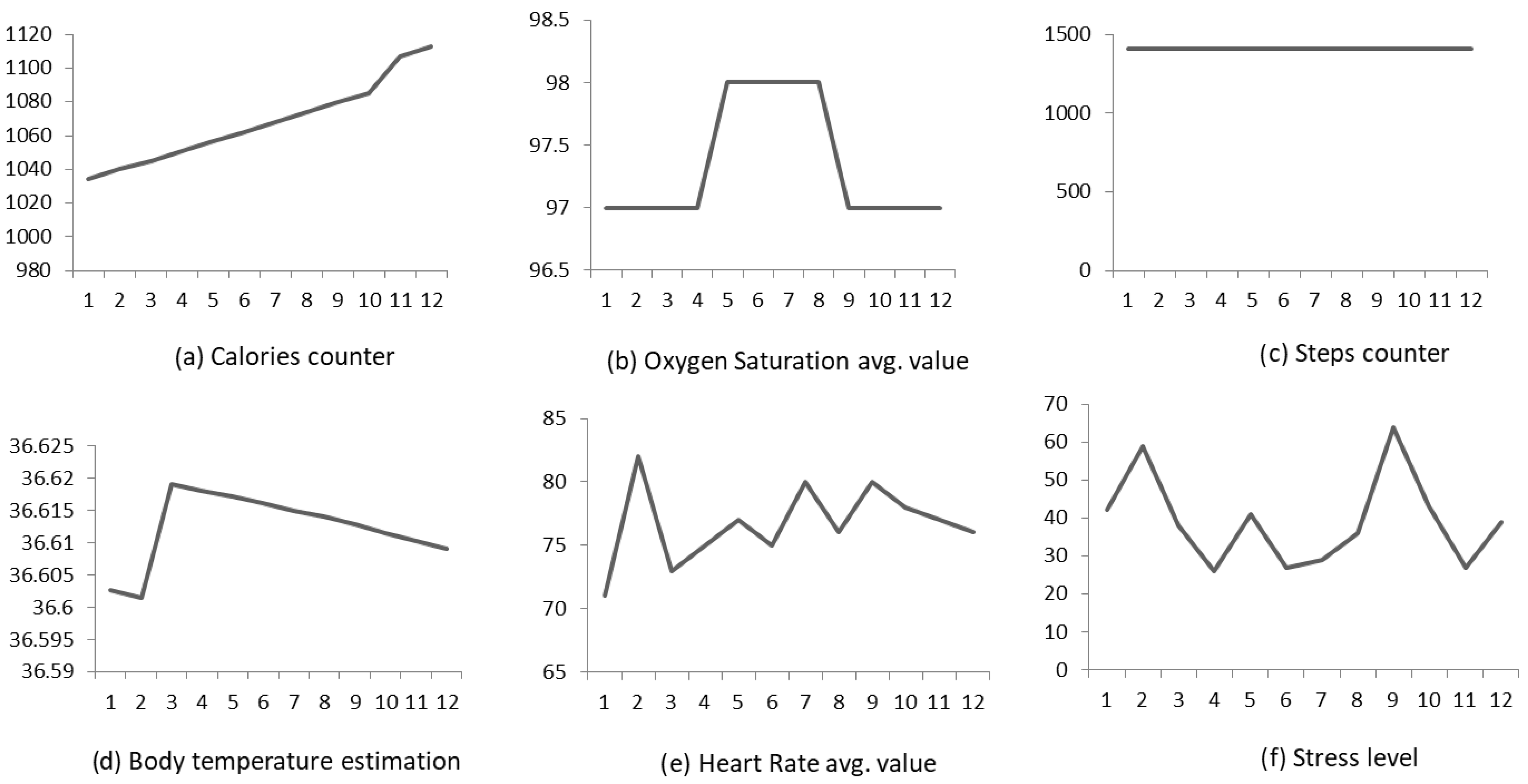
- The daily and weekly statistical reports of health parameters, namely specific statistical metrics, such as mean, maximum, and minimum values, etc., which are constantly calculated by means of the received time series of the heart rate, oxygen saturation, body temperature, and stress level, along with the respective time-series graphs (Figure 7).
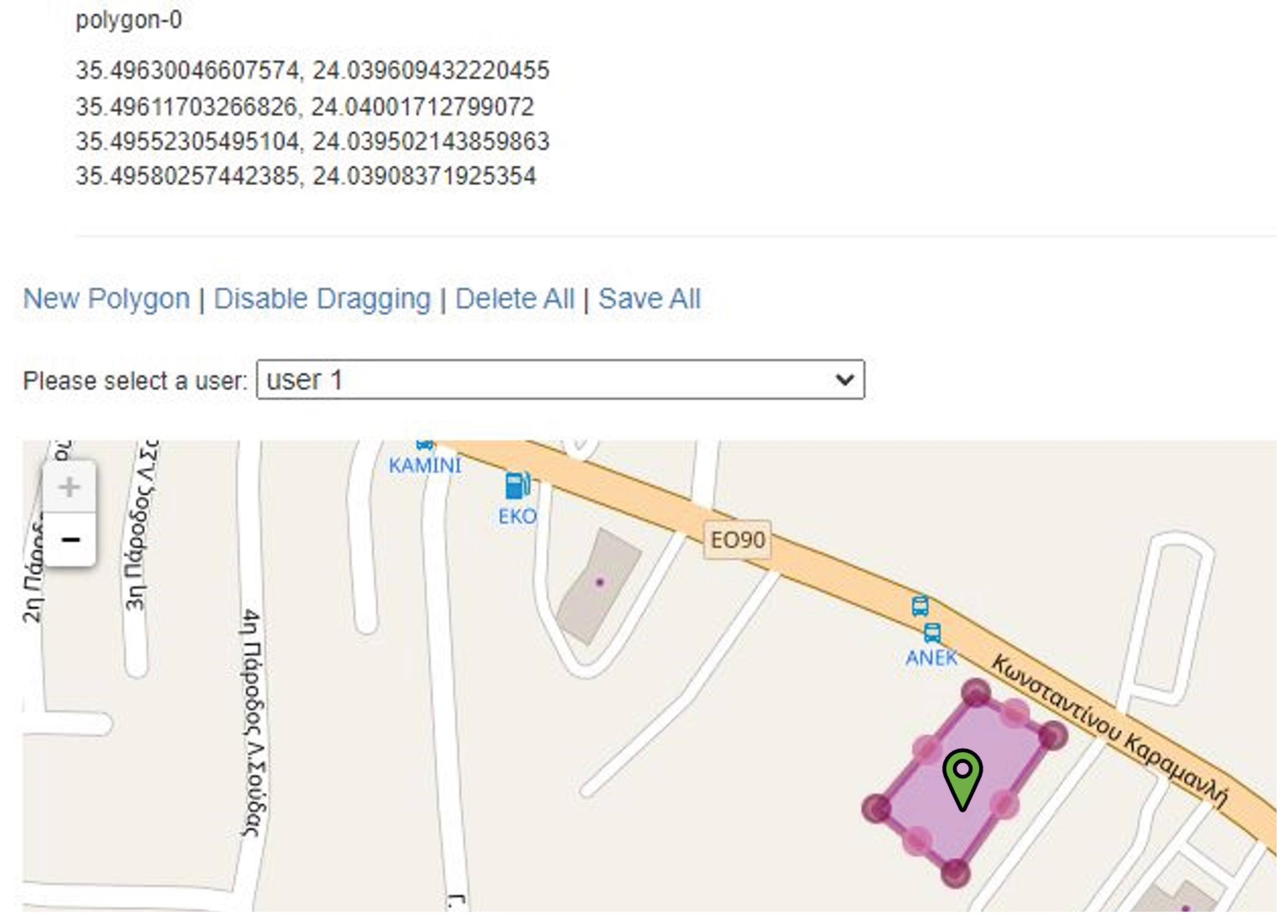
- The current location parameters are monitored by the smartphone’s GPS, which the carers can view anytime. Additionally, the caregivers are able to specify and change—directly on the map—the polygons that represent the individual safety areas of movement and activities for people with ID, namely geofences.
- The health and disorientation-related emergency incidents that are automatically detected by the system, along with the corresponding alerts. The carer can, at any time, view the recorded alerts, fill in additional data, as well as register new emergency incidents.
3.3. Mobile Applications
3.3.1. Detection of Health Emergencies
3.3.2. Detection of Disorientation and Wandering Behavior
3.3.3. Smartphone Application
- 1.
- People with ID:
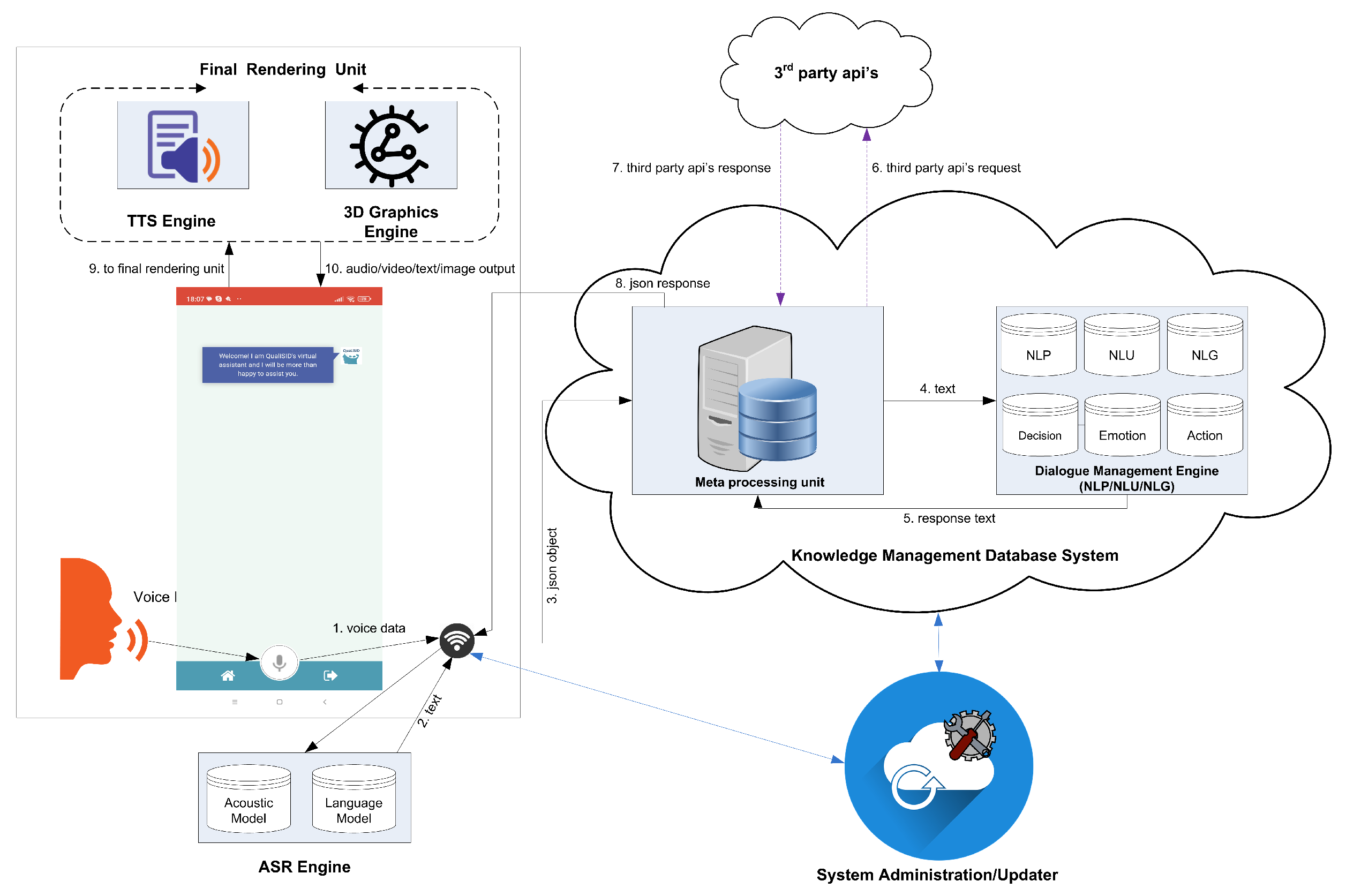
- Information, such as encyclopedia subjects, points of interest, weather forecasts, answers to short questions, etc., and entertainment, i.e., videos, pictures, music, radio, etc., through oral request (voice function and speech recognition) and the response of the virtual assistant.
- Communication with caregivers, relatives, and friends by phone calls and SMS messages through voice commands.
- System support and assistance in emergency cases through the automatic start of video calls with the responsible carers and/or voice instructions.
- Medication and other (such as lunchtime) reminders by the virtual assistant.
- Weather forecast notifications and alerts for upcoming bad and extreme weather conditions.
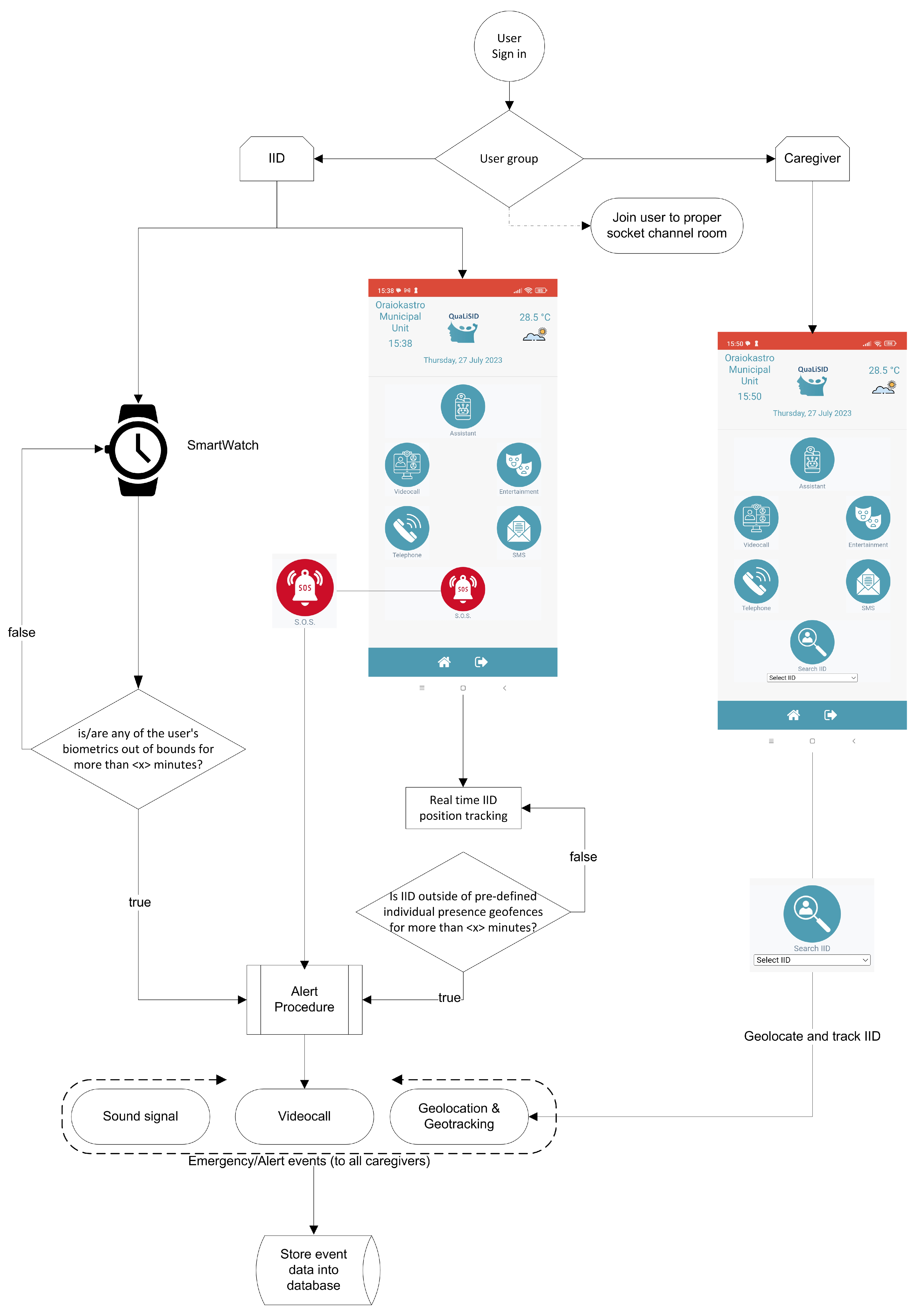
- S.O.S. (emergency) button for pressing in urgent situations related to health issues, disorientation, or other circumstances where the individual with ID feels uncomfortable.
- 2.
- Caregivers:
- Automated sound alerts for notification in emergency cases related to health issues that have been detected through the smartwatch monitoring of biomeasurements, i.e., heart rate, oxygen saturation, body temperature, and stress level.
- Automated sound alerts for notification in emergency cases related to disorientation and/or wandering behavior through the location monitoring from the smartphone’s GPS, when the individuals with ID have been located out of the safety zones (geofences).
- Alerts for upcoming bad weather conditions, in order to protect the individuals under their care who might be in potential danger.
- Automatic video call between the caregiver and the individual in an emergency situation and opening of the map where IID’s current location is depicted.
- Specification of geofences that constitute the individualized safe activities areas for the supported IID through the mobile user interface.
- Specification of automated sending of medication reminders to the supported IID, their carers, and families through the mobile user interface.
4. Experimental Results
4.1. Content Recommendation Service
- 1.
- User 1: This user has a mild ID. He understood the scope of the test and could use the web-based platform with assistance at the beginning, performing the task well while being very concentrated during the process. The user selected items according to his original preferences (e.g., paintings and crafts) and others not marked as High in the questionnaire (e.g., animals and plants). He used the system’s recommended ability to increase the font size of textual elements. Based on his selected content items, the updated preferences in his profile were maintained in four categories, while changed in the other four (reduced in three and increased in one, as depicted in Table 4).
- 2.
- User 4: This user has a severe ID. He used the web-based platform with assistance, performing the task pretty well. This user mostly selected items according to his initial preferences (Table 4), and he could read to a minimal extent; he chose to look mostly at pictures and videos. In the beginning, it was difficult for him to push buttons, while he could not concentrate and tended to speak during the testing. Based on his selected content items, the updated preferences in his profile were maintained in two categories and changed in the other six (fell in six) (Table 4).
- 3.
- User 12: This user has a moderate ID. She also used the web-based platform with assistance, responding very well during the process. She mostly selected items according to her original preferences (Table 4) and also chose to look mostly at pictures and videos. She is communicative; she could concentrate but also tended to speak while performing the testing. Based on her selected content items, the updated preferences in her profile were maintained in five categories and changed in the other three (reduced in two and increased in one—see Table 4).
4.2. Health and Location-Related Alerts
- 40 pulses/minute < Heart Rate < 100 pulses/minute.
- 95% < Oxygen Saturation < 100%.
- 35.7 °C < Body Temperature < 37.2 °C.
- 0% < Stress Level < 75%.
4.3. Smartphone Application
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Scandurra, V.; Emberti Gialloreti, L.; Barbanera, F.; Scordo, M.R.; Pierini, A.; Canitano, R. Neurodevelopmental disorders and adaptive functions: A study of children with autism spectrum disorders (ASD) and/or attention deficit and hyperactivity disorder (ADHD). Front. Psychiatry 2019, 10, 673. [Google Scholar] [CrossRef] [PubMed]
- Nair, R.; Mo, C.; Dutt, A.; Hagopian, L.; Singh, A.; Du, M. Significant regional inequalities in the prevalence of intellectual disability and trends from 1990 to 2019: A systematic analysis of GBD 2019. Epidemiol. Psychiatr. Sci. 2022, 21, 701. [Google Scholar] [CrossRef]
- des Portes, V. Intellectual disability. Handb. Clin. Neurol. 2020, 174, 113–126. [Google Scholar] [CrossRef] [PubMed]
- Apostolidis, K.; Mezaris, V.; Papadogiorgakim, M.; Bei, E.S.; Livanos, G.; Zervakis, M.E. Content and Other Resources Recommendations for Individuals with Intellectual Disability: A Review. Electronics 2022, 11, 3472. [Google Scholar] [CrossRef]
- Boot, F.H.; Dinsmore, J.; Khasnabis, C.; MacLachlan, M. Intellectual Disability and Assistive Technology: Opening the GATE Wider. Front. Public Health 2017, 22, 10. [Google Scholar] [CrossRef]
- Daly Lynn, J.; Rondón-Sulbarán, J.; Quinn, E.; Ryan, A.; McCormack, B.; Martin, S. A systematic review of electronic assistive technology within supporting living environments for people with dementia. Dementia 2019, 18, 2371–2435. [Google Scholar] [CrossRef]
- Cohen-Mansfield, J.; Creedon, M.A.; Malone, T.B.; Kirkpatrick, M.J., III; Dutra, L.A.; Herman, R.P. Electronic memory aids for community-dwelling elderly persons: Attitudes, preferences, and potential utilization. J. Appl. Gerontol. 2005, 24, 3–20. [Google Scholar] [CrossRef]
- Gitlin, L.N.; Schemm, R.L.; Landsberg, L.; Burgh, D. Factors predicting assistive device use in the home by older people following rehabilitation. J. Aging Health 1996, 8, 554–575. [Google Scholar] [CrossRef]
- Scherer, M.J. Assessing the benefits of using assistive technologies and other supports for thinking, remembering and learning. Disabil. Rehabil. 2005, 27, 731–739. [Google Scholar] [CrossRef]
- Thorpe, J.R.; Ronn-Andersen, K.V.; Bień, P.; Özkil, A.G.; Forchhammer, B.H.; Maier, A.M. Pervasive assistive technology for people with dementia: A UCD case. Healthc. Technol. Lett. 2016, 3, 297–302. [Google Scholar] [CrossRef]
- Papadogiorgaki, M.; Mezaris, V.; Grammalidis, N.; Grigoriadis, K.; Bei, E.S.; Livanos, G.; Zervakis, M.E. Quality of life support system for people with intellectual disability. In Proceedings of the 13th ACM International Conference on Pervasive Technologies Related to Assistive Environments (PETRA 2020), Corfu, Greece, 30 June–3 July 2020; pp. 1–6. [Google Scholar]
- Moreno, M.T.; Sans, J.C.; Fosch, M.T.C. Behavioral and cognitive interventions with digital devices in subjects with intellectual disability: A systematic review. Front. Psychiatry 2021, 12, 108797–108816. [Google Scholar]
- ELPIDA Project. E-Learning Platform for Intellectual Disability Awareness. Available online: http://elpida-project.eu/index.php/en/ (accessed on 26 August 2023).
- ENABLE Project. From Culture of Caring to Culture of Enabling: Co-Produce Services for People with Intellectual Disability. Association for Research and Training on Integration in Europe (ARFIE). Available online: https://arfie.info/2017/12/08/enable-project (accessed on 26 August 2023).
- Wyeth, P.; Summerville, J.; Adkins, B. Stomp: An interactive platform for people with intellectual disabilities. In Proceedings of the 8th International Conference on Advances in Computer Entertainment Technology (ACE’11), New Orleans, LA, USA, 26–27 October 2011; pp. 1–8. [Google Scholar] [CrossRef]
- Puspitasari, W.; Ummah, K.; F, P.A. Kidea: An innovative computer technology to improve skills in children with intelectual disability using kinect sensor. In Proceedings of the 2013 IEEE International Conference on Industrial Engineering and Engineering Management, Bangkok, Thailand, 10–13 December 2013. [Google Scholar] [CrossRef]
- Colomo-Palacios, R.; Paniagua-Martín, F.; García-Crespo, Á.; Ruiz-Mezcua, B. Technology enhanced learning for people with intellectual disabilities and cerebral paralysis: The MAS platform. In Proceedings of the Technology Enhanced Learning, Quality of Teaching and Educational Reform: First International Conference, TECH-EDUCATION, Athens, Greece, 19–21 May 2010; Springer: Berlin/Heidelberg, Germany, 2010; pp. 11–17. [Google Scholar]
- IDPLIVING. IDP Living Training. Available online: https://idpliving-platform.eu/en/home/ (accessed on 26 August 2023).
- LudoMinga. LudoMinga—A Serious Games-Based Platform. 2023. Available online: https://ludominga-aff09.firebaseapp.com/ (accessed on 26 August 2023).
- Watfern, C.; Heck, C.; Rule, C.; Baldwin, P.; Boydell, K.M. Feasibility and Acceptability of a Mental Health Website for Adults with an Intellectual Disability: Qualitative Evaluation. JMIR Ment. Health 2019, 6, 11–17. [Google Scholar] [CrossRef] [PubMed]
- MySigns—An App to Facilitate Mental Health Assessment of People with Intellectual Disability. Department of Developmental Disability Neurophsychiatry (3DN). Available online: https://www.3dn.unsw.edu.au/projects/mysigns-app-facilitate-mental-health-assessment-people-intellectual-disability (accessed on 26 August 2023).
- The NET. ERGASIAMOU.GR: Job Search Platform for People with Intellectual Disabilities. 2022. Available online: https://todiktyo.org/en/ergasiamou-gr-job-search-platform-for-people-with-intellectual-disabilities/ (accessed on 26 August 2023).
- Inclusion International. The International Network of People with Intellectual Disabilities and Their Families. Available online: https://inclusion-international.org/ (accessed on 26 August 2023).
- PUZZLE Project. Puzzle—Developing Easy to Read Formats for People with Intellectual Disabilities. Erasmus+ KA2—Cooperation for Innovation and the Exchange of Good Practices. 2015. Available online: https://www.puzzle-project.eu/index.php/el/ (accessed on 26 August 2023).
- EPIC. Hedland Disability Services. Available online: https://www.empoweringpeople.org.au/disability-support-services (accessed on 26 August 2023).
- DEP. Disability E-Learning Platform Supports People with Intellectual Disabilities in Albania. 2020. Available online: https://www.cei.int/news/8971/disability-e-learning-platform-supports-people-with-intellectual-disabilities-in-albania (accessed on 26 August 2023).
- Anagnostopoulos, I.; Anagnostopoulos, C.N.; Vlachogiannis, E.; Gavalas, D.; Tsekouras, G.E. Adaptive and Personalized Multimedia Content Delivery for Disabled Users in Internet TV. Signal Image Video Process. 2010, 4, 273–287. [Google Scholar] [CrossRef]
- Rohani, D.A.; Lopategui, A.Q.; Tuxen, N.; Faurholt-Jepsen, M.; Kessing, L.V.; Bardram, J.E. MUBS: A Personalized Recommender System for Behavioral Activation in Mental Health. In Proceedings of the 2020 CHI Conference on Human Factors in Computing Systems (CHI’20), Honolulu, HI, USA, 25–30 April 2020; pp. 1–13. [Google Scholar] [CrossRef]
- van Schrojenstein Lantman-De Valk, H.M.; Metsemakers, J.F.; Haveman, M.J.; Crebolder, H.F. Health problems in people with intellectual disability in general practice: A comparative study. Fam. Pract. 2000, 17, 405–407. [Google Scholar] [CrossRef] [PubMed]
- Vijayan, V.; Connolly, J.P.; Condell, J.; McKelvey, N.; Gardiner, P. Review of wearable devices and data collection considerations for connected health. Sensors 2021, 21, 5589. [Google Scholar] [CrossRef] [PubMed]
- Edwards, J.; Mold, F.E.; Knivett, D.; Boulter, P.; Firn, M.; Carey, N. Quality improvement of physical health monitoring for people with intellectual disabilities: An integrative review. J. Intellect. Disabil. Res. 2017, 62, 199–216. [Google Scholar] [CrossRef]
- Dibia, V. FOQUS: A Smartwatch Application for Individuals with ADHD and Mental Health Challenges. In Proceedings of the 18th International ACM SIGACCESS Conference on Computers and Accessibility, Reno, NV, USA, 22–25 October 2016; pp. 311–312. [Google Scholar]
- Varma, G.; Chauhan, R.; Singh, M.; Singh, D. Pre-emption of affliction severity using HRV measurements from a smart wearable; case-study on SARS-Cov-2 symptoms. Sensors 2020, 20, 7068. [Google Scholar] [CrossRef]
- King, C.E.; Sarrafzadeh, M. A survey of smartwatches in remote health monitoring. J. Healthc. Inform. Res. 2018, 2, 1–24. [Google Scholar] [CrossRef]
- Breda, J.; Patel, S. Intuitive and Ubiquitous Fever Monitoring Using Smartphones and Smartwatches. arXiv 2021, arXiv:2106.11855. [Google Scholar]
- Solomon, O.; Lawlor, M.C. Beyond V40. 31: Narrative phenomenology of wandering in autism and dementia. Cult. Med. Psychiatry 2018, 42, 206–243. [Google Scholar] [CrossRef]
- Lin, Q.; Zhang, D.; Chen, L.; Ni, H.; Zhou, X. Managing elders’ wandering behavior using sensors-based solutions: A survey. Int. J. Gerontol. 2014, 8, 49–55. [Google Scholar] [CrossRef]
- Martino-Saltzman, D.; Blasch, B.B.; Morris, R.D.; McNeal, L.W. Travel behavior of nursing home residents perceived as wanderers and nonwanderers. Gerontologist 1991, 31, 666–672. [Google Scholar] [CrossRef] [PubMed]
- Algase, D.L. Wandering: A dementia-compromised behavior. J. Gerontol. Nurs. 1999, 25, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Fillekes, M.P.; Giannouli, E.; Kim, E.K.; Zijlstra, W.; Weibel, R. Towards a comprehensive set of GPS-based indicators reflecting the multidimensional nature of daily mobility for applications in health and aging research. Int. J. Health Geogr. 2019, 18, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Solanas, A.; Martinez-Balleste, A.; Perez-Martinez, P.A.; de la Pena, A.F.; Ramos, J. m-Carer: Privacy-aware monitoring for people with mild cognitive impairment and dementia. IEEE J. Sel. Areas Commun. 2013, 31, 19–27. [Google Scholar] [CrossRef]
- Lin, Q.; Zhang, D.; Huang, X.; Ni, H.; Zhou, X. Detecting wandering behavior based on GPS traces for elders with dementia. In Proceedings of the 2012 12th International Conference on Control Automation Robotics & Vision (ICARCV), Guangzhou, China, 5–7 December 2012; pp. 672–677. [Google Scholar]
- De Joode, E.; Van Heugten, C.; Verhey, F.; Van Boxtel, M. Effectiveness of an electronic cognitive aid in patients with acquired brain injury: A multicentre randomised parallel-group study. Neuropsychol. Rehabil. 2013, 23, 133–156. [Google Scholar] [CrossRef]
- Hart, T.; Buchhofer, R.; Vaccaro, M. Portable electronic devices as memory and organizational aids after traumatic brain injury: A consumer survey study. J. Head Trauma Rehabil. 2004, 19, 351–365. [Google Scholar] [CrossRef]
- Jamieson, M.; Cullen, B.; McGee-Lennon, M.; Brewster, S.; Evans, J. Technological memory aid use by people with acquired brain injury. Neuropsychol. Rehabil. 2017, 27, 919–936. [Google Scholar] [CrossRef]
- Álvarez-Dardet, S.M.; Lara, B.L.; Pérez-Padilla, J. Older adults and ICT adoption: Analysis of the use and attitudes toward computers in elderly Spanish people. Comput. Hum. Behav. 2020, 110, 106377. [Google Scholar] [CrossRef]
- Wong, D.; Sinclair, K.; Seabrook, E.; McKay, A.; Ponsford, J. Smartphones as assistive technology following traumatic brain injury: A preliminary study of what helps and what hinders. Disabil. Rehabil. 2017, 39, 2387–2394. [Google Scholar] [CrossRef]
- Anderson, S.; Araten-Bergman, T.; Steel, G. Adults with intellectual disabilities as users of social media: A scoping review. Br. J. Learn. Disabil. 2023, 8, 928. [Google Scholar] [CrossRef]
- Pew Research Center. Mobile Fact Sheet. 2021. Available online: http://www.pewinternet.org/fact-sheet/mobile/ (accessed on 26 August 2023).
- Putzer, G.J.; Park, Y. Are physicians likely to adopt emerging mobile technologies? Attitudes and innovation factors affecting smartphone use in the Southeastern United States. Perspect. Health Inf. Manag. Am. Health Inf. Manag. Assoc. 2012, 9, 288. [Google Scholar]
- Shinohara, K.; Wobbrock, J.O. In the shadow of misperception: Assistive technology use and social interactions. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Vancouver, BC, Canada, 7–12 May 2011; pp. 705–714. [Google Scholar]
- Conte, M.J.; Gomes Ferreira, M.G.; García Ramírez, A.R. An AAC Mobile-Based Application for People with Intellectual Disability: A Case Study in Brazil. Adv.-Hum.-Comput. Interact. 2020, 2020, 2707. [Google Scholar] [CrossRef]
- Soy Cappaz Mobile Application. 2022. Available online: https://play.google.com/store/apps/details?id=com.mapfre.soycappaz&hl=es_AR (accessed on 26 August 2023).
- Borblik, J.; Shabalina, O.; Kultsova, M.; Pidoprigora, A.; Romanenko, R. Assistive technology software for people with intellectual or development disabilities: Design of user interfaces for mobile applications. In Proceedings of the 2015 6th International Conference on Information, Intelligence, Systems and Applications (IISA), London, UK, 7–9 September 2015; pp. 1–6. [Google Scholar] [CrossRef]
- Viamigo. Available online: https://www.viamigo.be/en/ (accessed on 26 August 2023).
- Mindmate. Your All-in-One App to Keep Your Mind & Body Healthy. 2021. Available online: https://www.mindmate-app.com/ (accessed on 26 August 2023).
- Memorywell. 2021. Available online: https://www.memorywell.com/ (accessed on 26 August 2023).
- AppAdvice. Talking Point. 2021. Available online: https://appadvice.com/app/alzheimers-societys-talking-point-forum/651419467 (accessed on 26 August 2023).
- AppAdvice. Elder 411. 2021. Available online: https://appadvice.com/app/elder-411-senior-caregiving-made-easier-with-doctor-marion/337794946 (accessed on 26 August 2023).
- Timeless. 2019. Available online: https://www.timeless.care (accessed on 26 August 2023).
- Play, G. CogniCare 411. 2022. Available online: https://play.google.com/store/apps/details?id=com.cognihealth.cognicare (accessed on 26 August 2023).
- SmartSole, G. When They Wander, You’ll Never Wonder. 2023. Available online: https://www.gpssmartsole.com/ (accessed on 26 August 2023).
- PainChek. Pain Assessment Tool. 2023. Available online: https://www.painchek.com/ (accessed on 26 August 2023).
- Play, G. Puzzle Me. 2018. Available online: https://play.google.com/store/apps/details?id=com.mirpkg.PuzzleMeFree (accessed on 26 August 2023).
- Blanco-Fernandez, Y.; Pazosarias, J.J.; Gil-Solla, A.; Ramos-Cabrer, M.; Lopez-Nore, M. Providing entertainment by content-based filtering and semantic reasoning in intelligent recommender systems. IEEE Trans. Consum. Electron. 2008, 54, 727–735. [Google Scholar] [CrossRef]
- Van den Oord, A.; Dieleman, S.; Schrauwen, B. Deep content-based music recommendation. In Proceedings of the 26th International Conference on Neural Information Processing Systems (NIPS’13), Berlin, Germany, 7–10 August 2013; Volume 24, pp. 2643–2651, ISBN 9781632660244. [Google Scholar]
- Grammatikopoulou, A.; Grammalidis, N.; Papadogiorgaki, M.; Zervakis, M. A platform for health emergency warning and wandering behaviour detection supporting people with Intellectual Disability. In Proceedings of the 15th International Conference on Pervasive Technologies Related to Assistive Environments, Paris, France, 14–16 June 2022; pp. 694–699. [Google Scholar]
- Schalock, R.L.; Luckasson, R.; Tassé, M.J. Defining, diagnosing, classifying, and planning supports for people with intellectual disability: An emerging consensus. Siglo Cero 2021, 52, 29–36. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Diseases (ICD-11). 2014. Available online: https://icd.who.int/en (accessed on 26 August 2023).
- Ke, X.; Liu, J. Intellectual disability. In IACAPAP e-Textbook of Child and Adolescent Mental Health; International Association for Child and Adolescent Psychiatry and Allied Professions: Geneva, Switzerland, 2012; pp. 1–25. [Google Scholar]
- Buntinx, W.H.E.; Schalock, R.L. Models of Disability, Quality of Life, and Individualized Supports: Implications for Professional Practice in Intellectual Disability. J. Policy Pract. Intellect. Disabil. 2010, 7, 283–294. [Google Scholar] [CrossRef]
- Association, W.M. World medical association declaration of helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Elbadrawy, A.; Karypis, G. User-Specific Feature-Based Similarity Models for Top-n Recommendation of New Items. ACM Trans. Intell. Syst. Technol. (TIST) 2015, 6, 495. [Google Scholar] [CrossRef]
- Papadogiorgaki, M.; Papastathis, V.; Nidelkou, E.; Waddington, S.; Bratu, B.; Ribiere, M.; Kompatsiaris, I. Two-Level Automatic Adaptation of a Distributed User Profile for Personalized News Content Delivery. Int. J. Digit. Multimed. Broadcast. Spec. Issue Pers. Mob. Multimed. Broadcast. 2008, 6, 1–21. [Google Scholar] [CrossRef]
- Photodentro. Digital School II: Expanding and Exploiting the Digital Educational Platform, the OER Repositories and the Interactive Textbooks. 2021. Available online: http://photodentro.edu.gr/aggregator/?lang=en (accessed on 26 August 2023).
- Travel All over Greece. Explore Greece. Available online: https://www.allovergreece.com/index.php?lang=en (accessed on 26 August 2023).
- Pixabay. Stunning Royalty-Free Images & Royalty-Free Stock. Available online: https://pixabay.com/ (accessed on 26 August 2023).
- Pexels. The Best Free Stock Photos, Royalty Free Images & Videos Shared by Creators. Available online: https://www.pexels.com/ (accessed on 26 August 2023).
- YouTube. YouTube Videos. Available online: https://www.youtube.com/ (accessed on 26 August 2023).
- Google Arts & Culture. Explore a Virtual Gallery. Available online: https://artsandculture.google.com/ (accessed on 26 August 2023).
- Wikimedia. Wikimedia Commons. Available online: https://commons.wikimedia.org/wiki/Main_Page (accessed on 26 August 2023).
- Openbook. Available online: https://www.openbook.gr/ (accessed on 26 August 2023).
- Airpano. A Virtual Journey around the World. Available online: https://www.airpano.com/ (accessed on 26 August 2023).
- Papadogiorgaki, M.; Apostolidis, K.; Livanos, G.; Bei, E.S.; Zafeiris, S.; Klado, G.A.; Mezaris, V.; Zervakis, M.E. A Content Recommendation Platform for People with Intellectual Disability. In Proceedings of the 14th International Conference on Ubiquitous and Future Networks (PETRA 2020), 3rd International Workshop on Artificial Intelligence for Information, Communications, and Applications (AIICA 2023), Athens, Greece, 14–16 April 2022. [Google Scholar]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Adv. Neural Inf. Process. Syst. 2012, 25, 298. [Google Scholar] [CrossRef]
- Zhou, B.; Lapedriza, A.; Khosla, A.; Oliva, A.; Torralba, A. Places: A 10 million image database for scene recognition. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 40, 1452–1464. [Google Scholar] [CrossRef] [PubMed]
- Abu-El-Haija, S.; Kothari, N.; Lee, J.; Natsev, P.; Toderici, G.; Varadarajan, B.; Vijayanarasimhan, S. Youtube-8m: A large-scale video classification benchmark. arXiv 2016, arXiv:1609.08675. [Google Scholar]
- Moumtzidou, A.; Dimou, A.; Gkalelis, N.; Vrochidis, S.; Mezaris, V.; Kompatsiaris, Y. ITI-CERTH participation to TRECVID 2015. In Proceedings of the TREC Video Retrieval Evaluation, New York, NY, USA, 14–19 July 2015. [Google Scholar]
- Kaggle. Kaggle Datasets. 2023. Available online: https://www.kaggle.com/datasets/gpiosenka/sports-classification (accessed on 26 August 2023).
- Souček, T.; Lokoč, J. Transnet v2: An effective deep network architecture for fast shot transition detection. arXiv 2020, arXiv:2008.04838. [Google Scholar]
- Gkalelis, N.; Daskalakis, D.; Mezaris, V. ViGAT: Bottom-up event recognition and explanation in video using factorized graph attention network. IEEE Access 2022, 10, 108797–108816. [Google Scholar] [CrossRef]
- Xie, S.; Sun, C.; Huang, J.; Tu, Z.; Murphy, K. Rethinking spatiotemporal feature learning: Speed-accuracy trade-offs in video classification. In Proceedings of the European Conference on Computer Vision (ECCV), Basel, Switzerland, 4–8 April 2018; pp. 305–321. [Google Scholar]
- Caba Heilbron, F.; Escorcia, V.; Ghanem, B.; Carlos Niebles, J. Activitynet: A large-scale video benchmark for human activity understanding. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Berlin, Germany, 15–18 December 2015; pp. 961–970. [Google Scholar]
- Galanopoulos, D.; Mezaris, V. Are all combinations equal? Combining textual and visual features with multiple space learning for text-based video retrieval. In Proceedings of the European Conference on Computer Vision, Tel Aviv, Israel, 23–27 October 2022; Springer: Berlin/Heidelberg, Germany, 2022; pp. 627–643. [Google Scholar]
- Reimers, N.; Gurevych, I. Sentence-bert: Sentence embeddings using siamese bert-networks. arXiv 2019, arXiv:1908.10084. [Google Scholar]
- Xu, J.; Mei, T.; Yao, T.; Rui, Y. Msr-vtt: A large video description dataset for bridging video and language. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, London, UK, 14–20 June 2016; pp. 5288–5296. [Google Scholar]
- Li, Y.; Song, Y.; Cao, L.; Tetreault, J.; Goldberg, L.; Jaimes, A.; Luo, J. TGIF: A new dataset and benchmark on animated GIF description. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, London, UK, 14–20 June 2016; pp. 4641–4650. [Google Scholar]
- Wang, X.; Wu, J.; Chen, J.; Li, L.; Wang, Y.F.; Wang, W.Y. Vatex: A large-scale, high-quality multilingual dataset for video-and-language research. In Proceedings of the 2019 IEEE/CVF International Conference on Computer Vision (ICCV), Seoul, Republic of Korea, 27 October–2 November 2019; pp. 4581–4591. [Google Scholar]
- Awad, G.; Butt, A.A.; Curtis, K.; Fiscus, J.; Godil, A.; Lee, Y.; Delgado, A.; Zhang, J.; Godard, E.; Chocot, B.; et al. Evaluating multiple video understanding and retrieval tasks at trecvid 2021. In Proceedings of the 2021 TREC Video Retrieval Evaluation, Grenoble, France, 3–7 June 2021. [Google Scholar]
- Buller, M.J.; Tharion, W.J.; Cheuvront, S.N.; Montain, S.J.; Kenefick, R.W.; Castellani, J.; Latzka, W.A.; Roberts, W.S.; Richter, M.; Jenkins, O.C.; et al. Estimation of human core temperature from sequential heart rate observations. Physiol. Meas. 2013, 34, 781. [Google Scholar] [CrossRef]
- Buller, M.J.; Tharion, W.J.; Duhamel, C.M.; Yokota, M. Real-time core body temperature estimation from heart rate for first responders wearing different levels of personal protective equipment. Ergonomics 2015, 58, 1830–1841. [Google Scholar] [CrossRef]
- Looney, D.P.; Buller, M.J.; Gribok, A.V.; Leger, J.L.; Potter, A.W.; Rumpler, W.V.; Tharion, W.J.; Welles, A.P.; Friedl, K.E.; Hoyt, R.W. Estimating resting core temperature using heart rate. J. Meas. Phys. Behav. 2018, 1, 79–86. [Google Scholar] [CrossRef]
- Dong, C.; Liu, Y.; Lumpkin, R.; Lankhorst, M.; Chen, D.; McWilliams, J.C.; Guan, Y. A scheme to identify loops from trajectories of oceanic surface drifters: An application in the Kuroshio Extension region. J. Atmos. Ocean. Technol. 2011, 28, 1167–1176. [Google Scholar] [CrossRef]
- Channell, M.M.; Loveall, S.J.; Conners, F.A. Strengths and weaknesses in reading skills of youth with intellectual disabilities. Res. Dev. Disabil. 2013, 34, 776–787. [Google Scholar] [CrossRef]
- Koritsas, S.; Iacono, T. Secondary conditions in people with developmental disability. Am. J. Intellect. Dev. Disabil. 2011, 116, 36–47. [Google Scholar] [CrossRef] [PubMed]
- Apache. Http Server Project. 2023. Available online: https://httpd.apache.org (accessed on 26 August 2023).
- Mariadb Server The Open Source Relational Database. 2023. Available online: https://mariadb.org (accessed on 26 August 2023).
- Node.js. Open-Source, Cross-Platform JavaScript Runtime Environment. 2023. Available online: https://nodejs.org (accessed on 26 August 2023).
- PHP. A Popular General-Purpose Scripting Language that Is Especially Suited to Web Development. 2023. Available online: https://www.php.net/ (accessed on 26 August 2023).
- Pluralsight. JavaScript. 2023. Available online: https://www.javascript.com/ (accessed on 26 August 2023).
- Mozilla. HTML: HyperText Markup Language. 2023. Available online: https://developer.mozilla.org/en-US/docs/Web/HTML (accessed on 26 August 2023).
- Mozilla. CSS: Cascading Style Sheets. 2023. Available online: https://developer.mozilla.org/en-US/docs/Web/CSS (accessed on 26 August 2023).
- Mozilla. Progressive Web Apps. 2023. Available online: https://developer.mozilla.org/en-US/docs/Web/Progressive_web_apps (accessed on 26 August 2023).
- Visual Crossing Weather. Visual Crossing Weather API. 2023. Available online: https://www.visualcrossing.com (accessed on 26 August 2023).
- API. MediaWiki API. 2023. Available online: https://www.mediawiki.org/wiki/MediaWiki (accessed on 26 August 2023).
- Youtube. Youtube Data API. 2023. Available online: https://developers.google.com/youtube/v3 (accessed on 26 August 2023).
- Nominatim. Open-Source Geocoding with OpenStreetMap Data. 2023. Available online: https://nominatim.org (accessed on 26 August 2023).
- OpenStreetMaps. OpenStreetMaps. 2023. Available online: https://www.openstreetmap.org (accessed on 26 August 2023).
- Leaflet. Leaflet Library. 2023. Available online: https://leafletjs.com (accessed on 26 August 2023).
- Mozilla. Automated Speech Recognition (ASR) Text To Speech & Web Speech API. 2023. Available online: https://developer.mozilla.org/en-US/docs/Web/API/Web_Speech_API (accessed on 26 August 2023).
- Google Places. Google Places API. 2023. Available online: https://developers.google.com/maps/documentation/places/web-service/overview (accessed on 26 August 2023).
- OpenStreetMap. OpenStreetMap—Points of Interest. 2023. Available online: https://wiki.openstreetmap.org/wiki/Points_of_interest (accessed on 26 August 2023).
- Munir, M.; Setiawan, W.; Prasetyo Nugroho, E.; Kusnendar, J.; Prasetya Wibawa, A. The Effectiveness of Multimedia in Education for Special Education (MESE) to Improve Reading Ability and Memorizing for Children with Intellectual Disability. Int. J. Emerg. Technol. Learn. 2018, 13, 254–263. [Google Scholar] [CrossRef]
- Begara Iglesias, O.; Gómez Sánchez, L.E.; Alcedo Rodríguez, M.A. Do young people with Asperger syndrome or intellectual disability use social media and are they cyberbullied or cyberbullies in the same way as their peers? Psicothema 2019, 31, 30–37. [Google Scholar] [CrossRef]
- Web Content Accessibility Guidelines (WCAG) International Standard. Available online: https://www.w3.org/WAI/standards-guidelines/wcag/ (accessed on 26 August 2023).
- Rabin, J.; McCathieNevile, C. Mobile Web Best Practices 1.0. Basic Guidelines. W3C Recommendation 29 July 2008. Available online: https://www.w3.org/TR/mobile-bp/ (accessed on 26 August 2023).
- Grahma. Open Seizure Detector. 2023. Available online: https://www.openseizuredetector.org.uk/ (accessed on 26 August 2023).
- Gillott, A.; Standen, P. Levels of anxiety and sources of stress in adults with autism. J. Intellect. Disabil. 2007, 11, 359–370. [Google Scholar] [CrossRef] [PubMed]
- The Media Futurist. Great Concept With Unfulfilled Promises: The Omron HeartGuide Blood Pressure Smartwatch Review. 2023. Available online: https://medicalfuturist.com/omron-heartguide-blood-pressure-smartwatch-review/ (accessed on 26 August 2023).
- Kultsova, M.; Potseluico, A.; Zhukova, I.; Skorikov, A.; Romanenko, R. A Two-Phase Method of User Interface Adaptation for People with Special Needs. In Creativity in Intelligent Technologies and Data Science; Kravets, A., Shcherbakov, M., Kultsova, M., Groumpos, P., Eds.; Springer: Berlin/Heidelberg, Germany, 2017; Volume 754, pp. 805–821. [Google Scholar] [CrossRef]
- Resta, E.; Brunone, L.; D’Amico, F.; Desideri, L. Evaluating a Low-Cost Technology to Enable People with Intellectual Disability or Psychiatric Disorders to Initiate and Perform Functional Daily Activities. Int. J. Environ. Res. Public Health 2021, 18, 9659. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, S.M.; Pescatello, L.S.; Bhat, A.N. Current perspectives on physical activity and exercise recommendations for children and adolescents with autism spectrum disorders. Phys. Ther. 2014, 94, 875–889. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| General Categories | Detailed Categories |
|---|---|
| News | Timeliness and Weather Forecast, Politics, Celebrities, Decoration and Fashion, Culture and Art, Sports, Environment, Architecture and Technology, Hygiene and Diet, World News |
| Entertainment | Music, Movies, Dance, Theater, Paintings, Nature and Landscapes and Archaeological Sites, Countries and Cities, Animals and Plants |
| Education | History and Archaeology and Culture, Mathematics, Physics and Astronomy, People and Society and Ecology and Environment, Internet and IT, Biology, Chemistry, Vocational Guidance, Geography and Geology, Language and Writing and Reading, Foreign Languages, Literature, Theater and Art History, Music Theory |
| Creative Activities | Gymnastic and Dance, Pottery, Cooking and Pastry, Gardening, Knitting, Technology Usage, Painting and Crafts, Musical Instruments |
| Interactive Games | Assembling-Games and Puzzles, Number Games, Crossword Games, Riddles and Quizzes, Scientific-Fantasy, Adventure, Strategy, Sport Games |
| Virtual Exploration | Museums and Temples and Monuments, City Attractions, Natural Landscapes, Art and Technology Exhibitions |
| Module/Unit | Voice-Controlled Virtual Assistant | Emergencies & Alerts | Support & Assistance | Communication |
|---|---|---|---|---|
| Weather | ✓ | ✓ | ||
| Music | ✓ | |||
| Radio | ✓ | |||
| Video | ✓ | |||
| Useful | ✓ | |||
| Advices-ITs | ✓ | |||
| Entertainment | ✓ | |||
| Phone calls | ✓ | ✓ | ✓ | |
| SMS | ✓ | ✓ | ||
| Points of interest | ✓ | |||
| Encyclopedia | ✓ | |||
| Short answers | ✓ | |||
| Chat | ✓ | |||
| Reminders (general) | ✓ | ✓ | ||
| Reminders (medication) | ✓ | ✓ | ||
| S.O.S. Button | ✓ | |||
| Video calls | ✓ | ✓ | ||
| Sound Alerts | ✓ | |||
| Automated Speech Recognition (ASR) | ✓ | |||
| Text To Speech (TTS) | ✓ | |||
| Open Street Maps | ✓ | |||
| IID geo-tracking | ✓ | ✓ | ||
| Geolocation | ✓ | ✓ | ||
| Geocoding | ✓ | ✓ | ||
| Geofences | ✓ | |||
| IID biometric data tracker | ✓ | ✓ |
| Data | Source |
|---|---|
| User’s geographic location | PWA + Smart Device GPS unit |
| Voice input | User |
| Weather | Visual Crossing Weather API [114] |
| Wikipedia | MediaWiki API [115] |
| Youtube | Youtube Data API [116] |
| Geolocation (direct and reverse) | Nominatim—Open-source geocoding with OpenStreetMap data [117] |
| Maps | OpenStreetMaps [118] and Leaflet library [119] |
| Biometrics | SmartWatch |
| Automated Speech Recognition (ASR) Text To Speech | Web Speech API [120] |
| Points of Interest (POIs) | Google places API [121], OSM [122] |
| User-ID | Timeliness & Weather-Forecast | Sports | Animals & Plants | Music | Movies | Internet & IT | Cooking & Pastry | Painting & Crafts |
|---|---|---|---|---|---|---|---|---|
| 1 | I: High | I: Medium | I: Medium | I: High | I: High | I: High | I: Medium | I: High |
| U: High | U: Medium | U: High | U: Medium | U: Medium | U: High | U: Low | U: High | |
| 4 | I: Medium | I: High | I: High | I: High | I: High | I: High | I: High | I: High |
| U: Low | U: Medium | U: High | U: Medium | U: High | U: Medium | U: Medium | U: Medium | |
| 12 | I: Low | I: High | I: High | I: High | I: Low | I: High | I: High | I: High |
| U: Low | U: Medium | U: High | U: High | U: Medium | U: High | U: High | U: Medium |
| User-ID | Timeliness & Weather-Forecast | Sports | Animals & Plants | Music | Movies | Internet & IT | Cooking & Pastry | Painting & Crafts |
|---|---|---|---|---|---|---|---|---|
| 1 | R (15 items): 1–15 | R (10 items): 16–25 | R (10 items): 31–40 | R (15 items): 46–60 | R (15 items): 61–75 | R (15 items): 76–90 | R (10 items): 91–100 | R (15 items): 106–120 |
| S: 12, 13, 14, 1, 2, 3, 5, 15 | S: 20, 17, 22, 23, 24, 18 | S: 32, 35, 36, 37, 38, 39, 40, 31, 33, 34 | S: 46, 47, 48, 49, 53 | S: 61, 62, 63, 64, 65, 66, 73 | S: 79, 80, 76, 77, 78, 84, 85, 86, 81, 88 | S: 97 | S: 107, 108, 114, 109, 111, 110, 112, 113, 117 | |
| U: 12, 13, 14, 1, 2, 3, 5, 15, 4, 7, 8, 9, 6, 10, 11 | U: 20, 17, 22, 23, 24, 18, 19, 29, 28, 30 | U: 32, 35, 36, 37, 38, 39, 40, 31, 33, 34, 41, 45, 42, 43, 44 | U: 46, 47, 48, 49, 53, 51, 56, 58, 60, 59 | U: 61, 62, 63, 64, 65, 66, 73, 67, 68, 69 | U: 79, 80, 76, 77, 78, 84, 85, 86, 81, 88, 82, 83, 87, 89, 90 | U: 97, 93, 100, 99, 104 | U: 107, 108, 114, 109, 111, 110, 112, 113, 117, 115, 116, 106, 118, 119, 120 | |
| 4 | R (10 items): 1–10 | R (15 items): 16–30 | R (15 items): 31–45 | R (15 items): 46–60 | R (15 items): 61–75 | R (15 items): 76–90 | R (15 items): 91–105 | R (15 items): 106–120 |
| S: 5, 8 | S: 16, 22, 19, 25, 27 | S: 38, 39, 40, 41, 42, 43, 44, 45, 32, 37 | S: 50, 47, 52 | S: 65, 61, 62, 64, 66, 67, 68, 70 | S: 79, 80, 85 | S: 98, 99, 103, 104 | S: 115, 116, 109, 110, 118 | |
| U: 5, 8, 4, 7, 13 | U: 16, 22, 19, 25, 27, 17, 18, 20, 29, 30 | U: 38, 39, 40, 41, 42, 43, 44, 45, 32, 37, 34, 35, 36, 31, 33 | U: 50, 47, 52, 54, 56, 57, 58, 60, 46, 49 | U: 65, 61, 62, 64, 66, 67, 68, 70, 69, 71, 72, 73, 74, 75, 63 | U: 79, 80, 85, 82, 83, 84, 81, 78, 89, 90 | U: 98, 99, 103, 104, 91, 92, 96, 101, 105, 102 | U: 115, 116, 109, 110, 118, 108, 111, 112, 113, 120 | |
| 12 | R (5 items): 1–5 | R (15 items): 16–30 | R (15 items): 31–45 | R (15 items): 46–60 | R (5 items): 61–65 | R (15 items): 76–90 | R (15 items): 91–105 | R (15 items): 106–120 |
| S: 3, 4, 5 | S: 18, 22, 19, 20, 25 | S: 35, 37, 32, 31, 33, 34, 38, 39, 40, 41 | S: 60, 58, 56, 52, 53, 50, 59, 57, 49, 48, 54 | S: 62, 64, 65, 61, 63 | S: 76, 78, 77, 79, 80, 83, 85, 90 | S: 91, 93, 94, 96, 98, 100, 101, 105 | S: 119, 106, 107, 113, 118 | |
| U: 3, 4, 5, 8, 13 | U: 18, 22, 19, 20, 25, 17, 21, 22, 27, 30 | U: 35, 37, 32, 31, 33, 34, 38, 39, 40, 41, 36, 42, 43, 44, 45 | U: 60, 58, 56, 52, 53, 50, 59, 57, 49, 48, 54, 55, 51, 46, 47 | U: 62, 64, 65, 61, 63, 66, 69, 67, 68, 72 | U: 76, 78, 77, 79, 80, 83, 85, 70 | U: 91, 93, 94, 96, 98, 100, 101, 105, 97, 92, 95, 99, 103, 104, 102 | U: 119, 106, 107, 113, 118, 108, 110, 111, 112, 114 |
| Support System for People with Intellectual Disability | Information-News Features | Education-Training Features | Socialization Features | Entertainment Features | Games | Content Recommendations | Disorientation-Wandering Detection | Health Monitoring & Emergencies Detection | Medication Reminders | Weather & Other Notifications | S.O.S. Button | Virtual Assistant |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MUBS [28] | ✓ | ✓ | ✓ | ✓ | ||||||||
| FOQUS [32] | ✓ | ✓ | ||||||||||
| m-Carer [41] | ✓ | |||||||||||
| Soy Cappaz [53] | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||
| Viamigo [55] | ✓ | ✓ | ||||||||||
| MindMate [56] | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||
| Timeless [60] | ✓ | ✓ | ✓ | ✓ | ||||||||
| GPS SmartSole [62] | ✓ | |||||||||||
| Puzzle Me [64] | ✓ | |||||||||||
| OAED [42] | ✓ | ✓ | ||||||||||
| Healthy Mind [20] | ✓ | |||||||||||
| MySigns [21] | ✓ | ✓ | ||||||||||
| Puzzle [24] | ✓ | ✓ | ||||||||||
| ELPIDA [13] | ✓ | ✓ | ||||||||||
| ENABLE [14] | ✓ | ✓ | ✓ | |||||||||
| Stomp [15] | ✓ | ✓ | ✓ | |||||||||
| KIDEA [16] | ✓ | ✓ | ||||||||||
| MAS [17] | ✓ | ✓ | ✓ | |||||||||
| IDPLIVING [18] | ✓ | ✓ | ||||||||||
| LudoMinga [19] | ✓ | ✓ | ||||||||||
| IPTV [27] | ✓ | ✓ | ✓ | |||||||||
| MemoryWell [57] | ✓ | ✓ | ||||||||||
| ERGASIAMOU [22] | ✓ | |||||||||||
| Inclusion [23] | ✓ | ✓ | ||||||||||
| QuaLiSID | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papadogiorgaki, M.; Grammalidis, N.; Grammatikopoulou, A.; Apostolidis, K.; Bei, E.S.; Grigoriadis, K.; Zafeiris, S.; Livanos, G.; Mezaris, V.; Zervakis, M.E. An Integrated Support System for People with Intellectual Disability. Electronics 2023, 12, 3803. https://doi.org/10.3390/electronics12183803
Papadogiorgaki M, Grammalidis N, Grammatikopoulou A, Apostolidis K, Bei ES, Grigoriadis K, Zafeiris S, Livanos G, Mezaris V, Zervakis ME. An Integrated Support System for People with Intellectual Disability. Electronics. 2023; 12(18):3803. https://doi.org/10.3390/electronics12183803
Chicago/Turabian StylePapadogiorgaki, Maria, Nikos Grammalidis, Athina Grammatikopoulou, Konstantinos Apostolidis, Ekaterini S. Bei, Kostas Grigoriadis, Stylianos Zafeiris, George Livanos, Vasileios Mezaris, and Michalis E. Zervakis. 2023. "An Integrated Support System for People with Intellectual Disability" Electronics 12, no. 18: 3803. https://doi.org/10.3390/electronics12183803