
Detecting Breast Arterial Calcifications in Mammograms with Transfer Learning


Abstract
:1. Introduction
2. Literature Review
2.1. Previous Approaches
2.2. Previous Approaches Using Deep Learning
3. Methodology
3.1. Pre-Trained Models
3.1.1. VGG-19
3.1.2. ResNet50
3.1.3. DenseNet121
3.1.4. InceptionV3
3.1.5. Mobile Net
3.2. Dataset
3.3. Methods
3.4. Data Augmentation Settings
3.5. Transfer Learning Optimizations
3.6. Training of All Models
4. Results and Discussion
4.1. Results of Model
4.2. Verification of Results on Large Population
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; De Ferranti, S.; Després, J.-P.; Fullerton, H.J. Heart disease and stroke statistics—2016 update: A report from the American Heart Association. Circulation 2016, 133, e38–e360. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Theroux, P. Pathophysiology of coronary artery disease. Circulation 2005, 111, 3481–3488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoepf, U.J.; Becker, C.R.; Ohnesorge, B.M.; Yucel, E.K. CT of coronary artery disease. Radiology 2004, 232, 18–37. [Google Scholar] [CrossRef] [PubMed]
- Havaei, M.; Davy, A.; Warde-Farley, D.; Biard, A.; Courville, A.; Bengio, Y.; Pal, C.; Jodoin, P.-M.; Larochelle, H. Brain tumor segmentation with deep neural networks. Med. Image Anal. 2017, 35, 18–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castling, B.; Bhatia, S.; Ahsan, F. Mönckeberg’s arteriosclerosis: Vascular calcification complicating microvascular surgery. Int. J. Oral Maxillofac. Surg. 2015, 44, 34–36. [Google Scholar] [CrossRef] [PubMed]
- US Food and Drug Administration. FDA Approves First 3-D Mammography Imaging System; FDA: Silver Spring, MD, USA, 2011. [Google Scholar]
- Ge, J.; Chan, H.-P.; Sahiner, B.; Zhou, C.; Helvie, M.A.; Wei, J.; Hadjiiski, L.M.; Zhang, Y.; Wu, Y.-T.; Shi, J. Automated detection of breast vascular calcification on full-field digital mammograms. In Proceedings of the Medical Imaging 2008: Computer-Aided Diagnosis, San Diego, CA, USA, 16–21 February 2008; pp. 379–385. [Google Scholar]
- Marks, H. Breast Calcifications. WebMD. 27 August 2022. Available online: https://www.webmd.com/women/guide/breast-calcification-symptoms-causes-treatments (accessed on 30 December 2022).
- Molloi, S.; Mehraien, T.; Iribarren, C.; Smith, C.; Ducote, J.L.; Feig, S.A. Reproducibility of breast arterial calcium mass quantification using digital mammography. Acad. Radiol. 2009, 16, 275–282. [Google Scholar] [CrossRef] [Green Version]
- Mostafavi, L.; Marfori, W.; Arellano, C.; Tognolini, A.; Speier, W.; Adibi, A.; Ruehm, S.G. Prevalence of coronary artery disease evaluated by coronary CT angiography in women with mammographically detected breast arterial calcifications. PLoS ONE 2015, 10, e0122289. [Google Scholar] [CrossRef] [Green Version]
- Matsumura, M.E.; Maksimik, C.; Martinez, M.W.; Weiss, M.; Newcomb, J.; Harris, K.; Rossi, M.A. Breast artery calcium noted on screening mammography is predictive of high risk coronary calcium in asymptomatic women: A case control study. Vasa 2013, 42, 429–433. [Google Scholar] [CrossRef]
- Pecchi, A.; Rossi, R.; Coppi, F.; Ligabue, G.; Modena, M.G.; Romagnoli, R. Association of breast arterial calcifications detected by mammography and coronary artery calcifications quantified by multislice CT in a population of post-menopausal women. La Radiol. Med. 2003, 106, 305–312. [Google Scholar]
- Guo, X.; O’Neill, W.C.; Vey, B.; Yang, T.C.; Kim, T.J.; Ghassemi, M.; Pan, I.; Gichoya, J.W.; Trivedi, H.; Banerjee, I. SCU-Net: A deep learning method for segmentation and quantification of breast arterial calcifications on mammograms. Med. Phys. 2021, 48, 5851–5861. [Google Scholar] [CrossRef]
- Kataoka, M.; Warren, R.M.L.; Sala, E. How predictive is breast arterial calcification of cardiovascular disease and risk factors when found at screening mammography? Am. J. Roentgenol. 2006, 187, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Rotter, M.A.; Schnatz, P.F.; Currier, A.A., Jr.; O’Sullivan, D.M. Breast arterial calcifications (BACs) found on screening mammography and their association with cardiovascular disease. Menopause 2008, 15, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Iribarren, C.; Go, A.S.; Tolstykh, I.; Sidney, S.; Johnston, S.C.; Spring, D.B. Breast vascular calcification and risk of coronary heart disease, stroke, and heart failure. J. Women’s Health 2004, 13, 381–389. [Google Scholar] [CrossRef] [PubMed]
- AlGhamdi, M.; Abdel-Mottaleb, M.; Collado-Mesa, F. DU-Net: Convolutional network for the detection of arterial calcifications in mammograms. IEEE Trans. Med. Imaging 2020, 39, 3240–3249. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Ding, H.; Bidgoli, F.A.; Zhou, B.; Iribarren, C.; Molloi, S.; Baldi, P. Detecting cardiovascular disease from mammograms with deep learning. IEEE Trans. Med. Imaging 2017, 36, 1172–1181. [Google Scholar] [CrossRef] [PubMed]
- Al Ghamdi, M.; Li, M.; Abdel-Mottaleb, M.; Abou Shousha, M. Semi-supervised transfer learning for convolutional neural networks for glaucoma detection. In Proceedings of the ICASSP 2019-2019 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Brighton, UK, 12–17 May 2019; pp. 3812–3816. [Google Scholar]
- Hendriks, E.J.; De Jong, P.A.; van der Graaf, Y.; Willem, P.T.M.; van der Schouw, Y.T.; Beulens, J.W. Breast arterial calcifications: A systematic review and meta-analysis of their determinants and their association with cardiovascular events. Atherosclerosis 2015, 239, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Mazidi, N.; Roobottom, C.; Masala, G. Automatic Quantification of Breast Arterial Calcification on Mammographic Images. In Innovation in Medicine and Healthcare Systems, and Multimedia; Springer: New York, NY, USA, 2019; pp. 283–292. [Google Scholar]
- Nava, E.; Barba, I.; Sendra, F.; Gómez–Rebollo, C. Quantification of vascular calcifications on digitized mammograms. In International Workshop on Digital Mammography; Springer: New York, NY, USA, 2010; pp. 183–190. [Google Scholar]
- Cheng, E.; McLaughlin, S.; Megalooikonomou, V.; Bakic, P.R.; Maidment, A.D.; Ling, H. Learning-based vessel segmentation in mammographic images. In Proceedings of the IEEE International Conference on Healthcare Informatics, Imaging and Systems Biology, HISB 2011, San Jose, CA, USA, 26–29 July 2011; pp. 315–322. [Google Scholar]
- Cheng, J.-Z.; Chen, C.-M.; Cole, E.B.; Pisano, E.D.; Shen, D. Automated delineation of calcified vessels in mammography by tracking with uncertainty and graphical linking techniques. IEEE Trans. Med. Imaging 2012, 31, 2143–2155. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.-Z.; Chen, C.-M.; Shen, D. Identification of breast vascular calcium deposition in digital mammography by linear structure analysis. In Proceedings of the 2012 9th IEEE International Symposium on Biomedical Imaging (ISBI), Barcelona, Spain, 2–5 May 2012; pp. 126–129. [Google Scholar]
- Cheng, J.-Z.; Cole, E.B.; Pisano, E.D.; Shen, D. Detection of arterial calcification in mammograms by random walks. In Proceedings of the 27th International Conference, IPMI 2021, Virtual Event, 28–30 June 2021; pp. 713–724. [Google Scholar]
- Li, X.; Chen, H.; Qi, X.; Dou, Q.; Fu, C.-W.; Heng, P.-A. H-DenseUNet: Hybrid densely connected UNet for liver and tumor segmentation from CT volumes. IEEE Trans. Med. Imaging 2018, 37, 2663–2674. [Google Scholar] [CrossRef] [Green Version]
- Guan, S.; Khan, A.A.; Sikdar, S.; Chitnis, P.V. Fully dense UNet for 2-D sparse photoacoustic tomography artifact removal. IEEE J. Biomed. Health Inform. 2019, 24, 568–576. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Bentley, P.; Mori, K.; Misawa, K.; Fujiwara, M.; Rueckert, D. DRINet for medical image segmentation. IEEE Trans. Med. Imaging 2018, 37, 2453–2462. [Google Scholar] [CrossRef]
- Baheti, P. A Newbie-Friendly Guide to Transfer Learning. v7, 19 July 2022. [Google Scholar]
- Seldon. Transfer Learning for Machine Learning. Seldon, 29 June 2019. [Google Scholar]
- Sarkar, D.D. A Comprehensive Hands-on Guide to Transfer Learning with Real-World Applications in Deep Learning. Towards Data Science. 2018. Available online: https://towardsdatascience.com/a-comprehensive-hands-on-guide-to-transfer-learning-with-real-world-applications-in-deep-learning-212bf3b2f27a (accessed on 30 December 2022).
- Kaushik, A. Understanding the VGG19 Architecture, OpenGenus IQ: Computing Expertise & Legacy. 2022.
- Kaushik, A. Understanding ResNet50 architecture, OpenGenus IQ: Computing Expertise & Legacy. 2022.
- Boesch, G. Deep Residual Networks (ResNet, ResNet50)—Guide in 2022; Datagen: New York, NY, USA, 2022. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Feng, C.; Zhang, H.; Wang, S.; Li, Y.; Wang, H.; Yan, F. Structural damage detection using deep convolutional neural network and transfer learning. KSCE J. Civ. Eng. 2019, 23, 4493–4502. [Google Scholar] [CrossRef]
- Howard, A.G.; Zhu, M.; Chen, B.; Kalenichenko, D.; Wang, W.; Weyand, T.; Andreetto, M.; Adam, H. Mobilenets: Efficient convolutional neural networks for mobile vision applications. arXiv 2017, arXiv:1704.04861. [Google Scholar]
- Shah, D. The Essential Guide to Data Augmentation in Deep Learning. Available online: https://www.v7labs.com/blog/data-augmentation-guide (accessed on 19 July 2022).
- Fchollet: The Sequential Model. Keras, 4 December 2020.
- Brownlee, J. Difference Between a Batch and an Epoch in a Neural Network. Machine Learning Mastery, 20 July 2018. [Google Scholar]
- Doshi, S. Various Optimization Algorithms For Training Neural Network. Towards Data Science, 13 January 2019. [Google Scholar]
- Mayanglambam, G. Deep Learning Optimizers. Towards Data Science, 18 November 2020. [Google Scholar]
- Afaq, S.; Rao, S. Significance of epochs on training a neural network. Int. J. Sci. Technol. Res. 2020, 9, 485–488. [Google Scholar]
- Newcombe, R.G. Two-sided confidence intervals for the single proportion: Comparison of seven methods. Stat. Med. 1998, 17, 857–872. [Google Scholar] [CrossRef]
- Trimboli, R.M.; Codari, M.; Bert, A.; Carbonaro, L.A.; Maccagnoni, S.; Raciti, D.; Bernardi, D.; Clauser, P.; Losio, C.; Tagliafico, A.; et al. Breast arterial calcifications on mammography: Intra-and inter-observer reproducibility of a semi-automatic quantification tool. Radiol. Med. 2018, 123, 168–173. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Values |
|---|---|
| Rescale | 1/255 |
| Height shift | 0.2 |
| Width shift | 0.2 |
| Zoom | 0.2 |
| Shear | 0.2 |
| Rotation | 40 |
| Horizontal flip | True |
| Hyper-Parameters | Values |
|---|---|
| Batch size | 16 |
| Epochs | 400/600 |
| Optimizer | Adagrad |
| Learning rate | Default (0.001) |
| Loss function | Categorical Cross-entropy |
| VGG-19 | ResNet50 | Mobile Net | DenseNet-121 | Inception V3 | |
|---|---|---|---|---|---|
| Training time (avg.) ms/epoch | 9.733 | 8.673 | 7.533 | 8.631 | 7.640 |
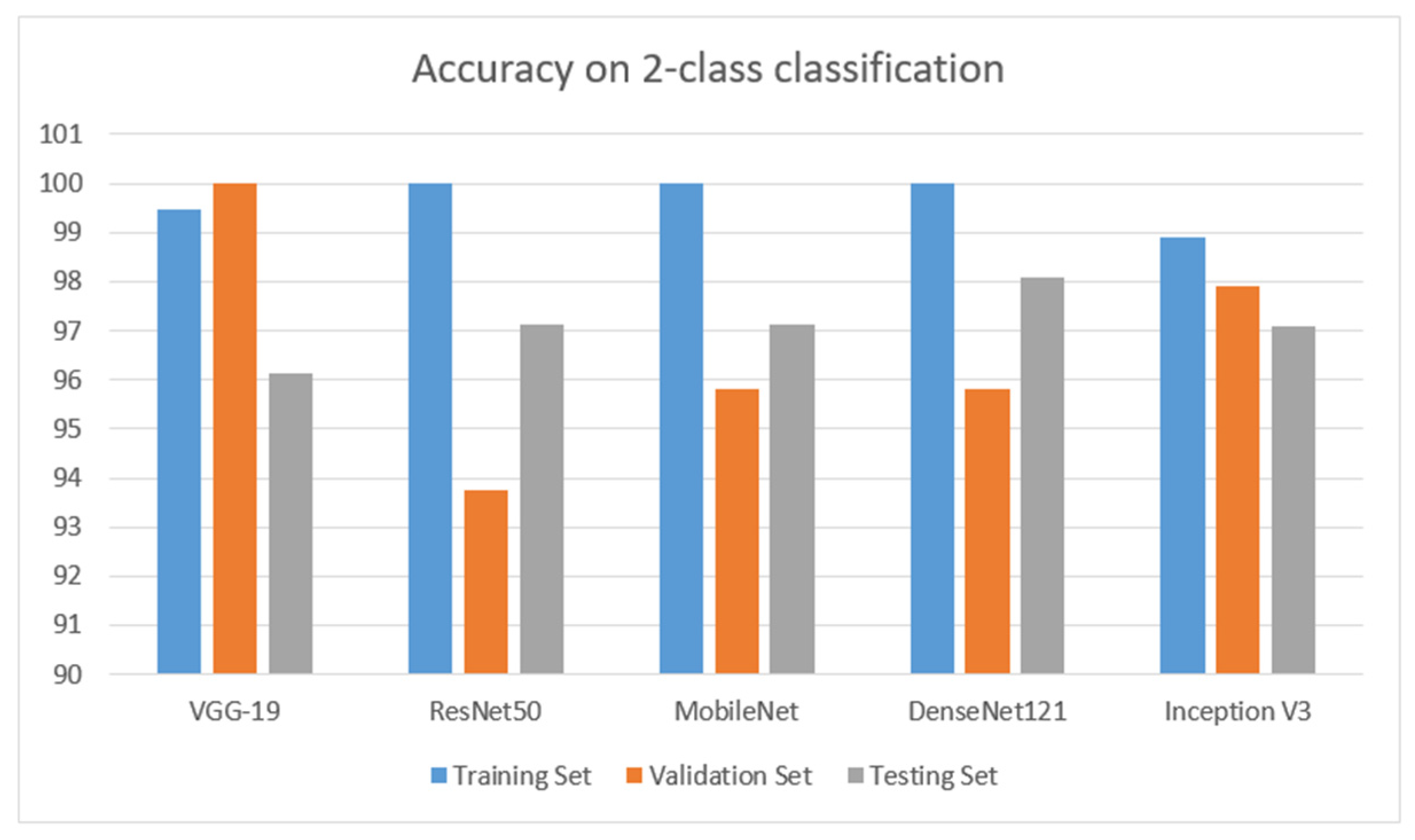
| Val. Accuracy (%) | 100 | 93.75 | 95.83 | 95.83 | 97.92 |
| Val. loss | 1.88 | 11.92 | 22.41 | 13.07 | 2.42 |
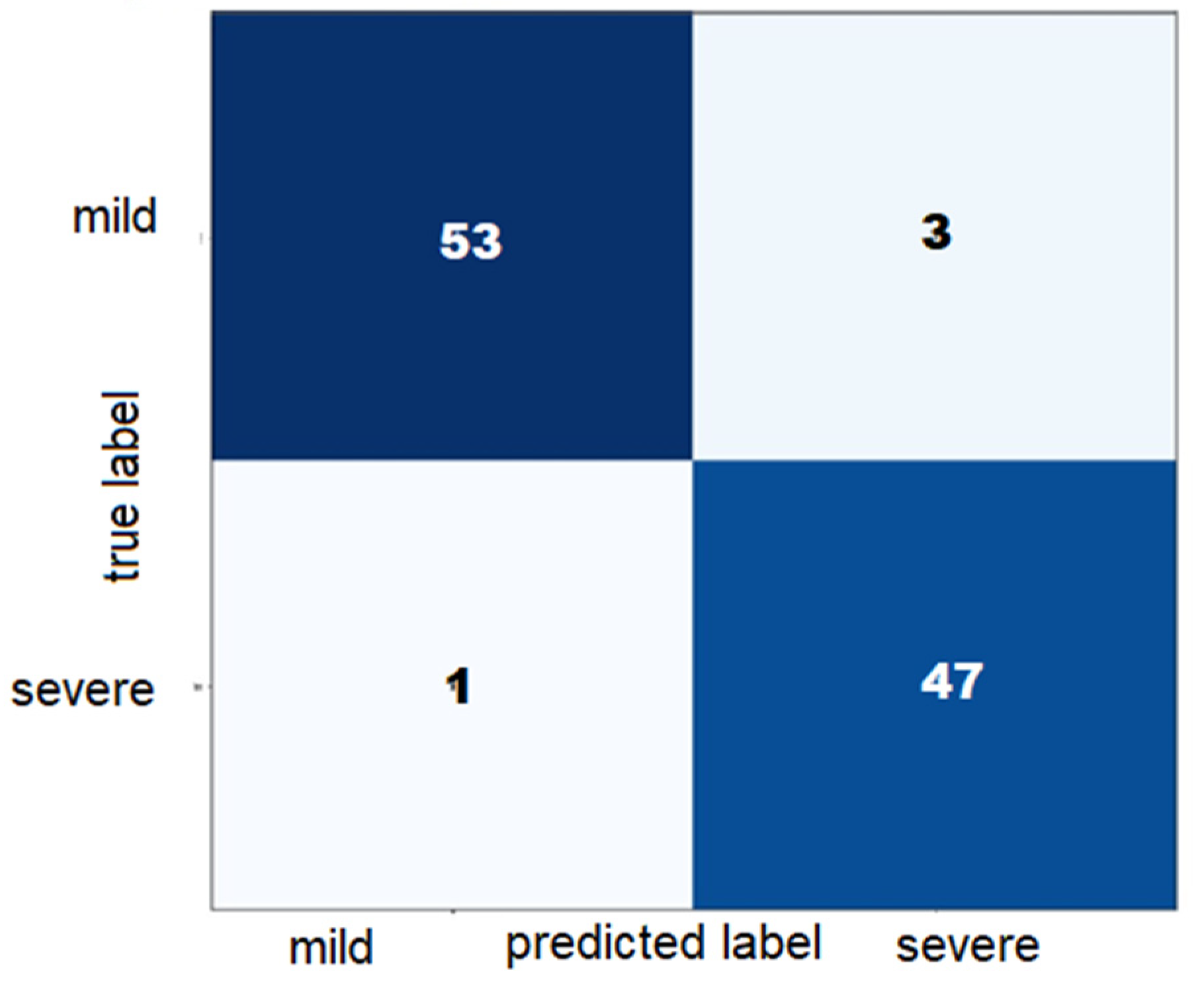
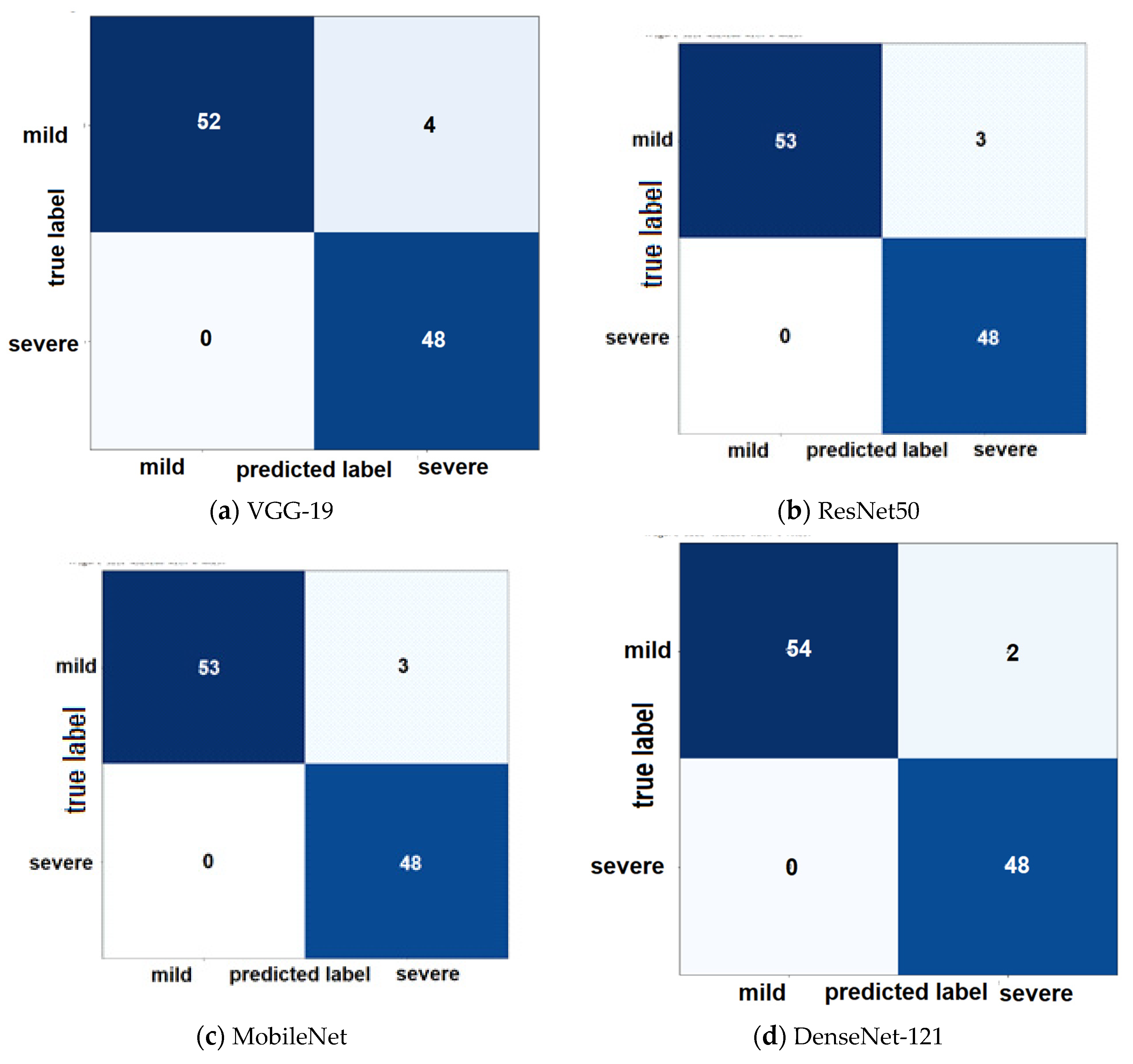
| Test Accuracy | 96.15 | 97.11 | 97.11 | 98.07 | 97.08 |
| Test Sensitivity (Recall) | 100 | 100 | 100 | 100 | 98 |
| Test Specificity | 93 | 95 | 95 | 96 | 95 |
| Test Precision | 92 | 94 | 94 | 96 | 94 |
| Figure No. | 6 | 7 | 8 | 9 | 10 |
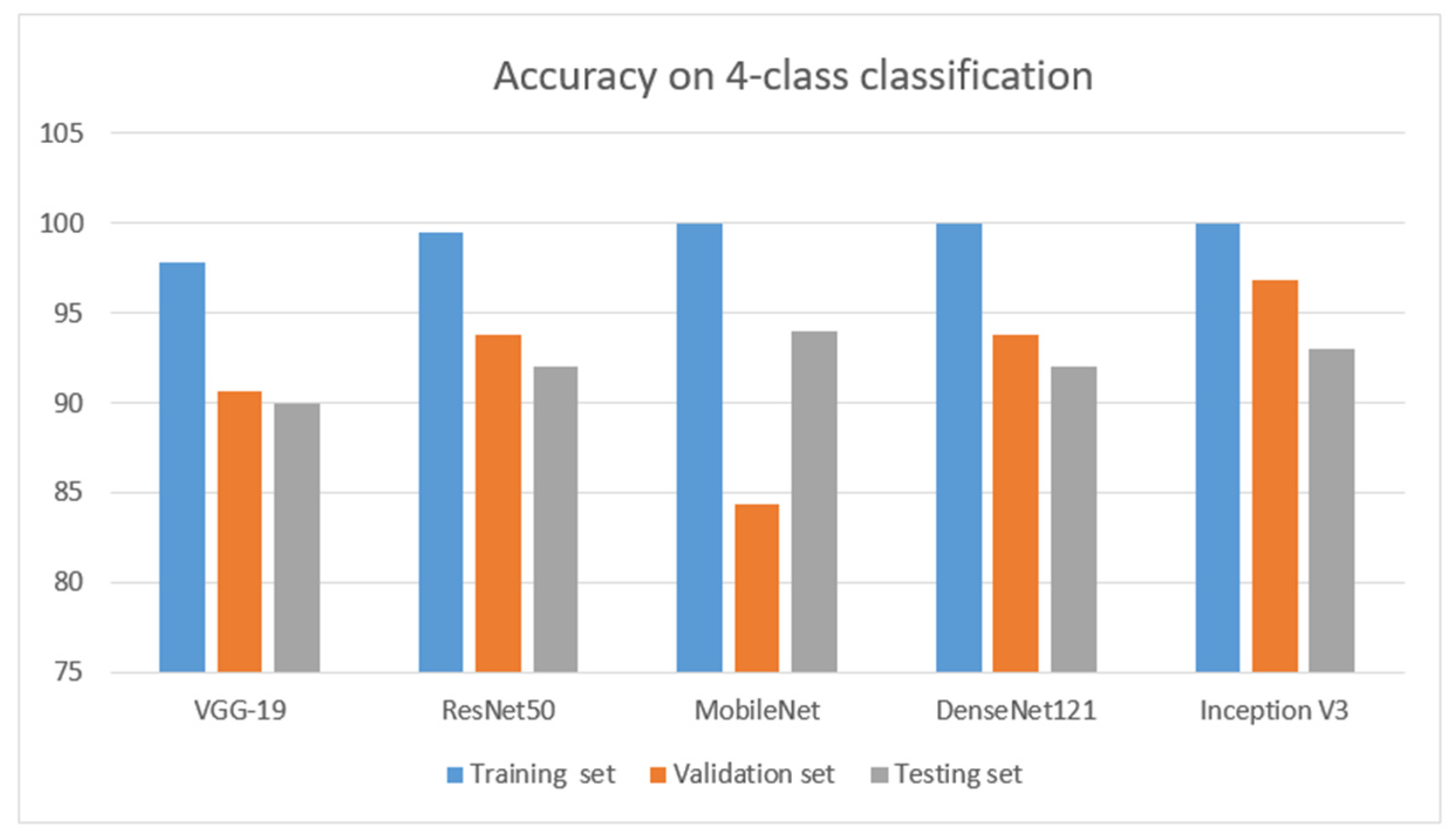
| Model | VGG-19 | ResNet50 | Mobile Net | DenseNet-121 | Inception V3 |
|---|---|---|---|---|---|
| Training time (avg.) ms/epoch | 9.733 | 8.676 | 6.523 | 7.598 | 7.588 |
| Val. Accuracy (%) | 90.62 | 93.75 | 84.38 | 93.75 | 96.88 |
| Val. loss | 42.05 | 7.45 | 58.84 | 43.20 | 13.49 |
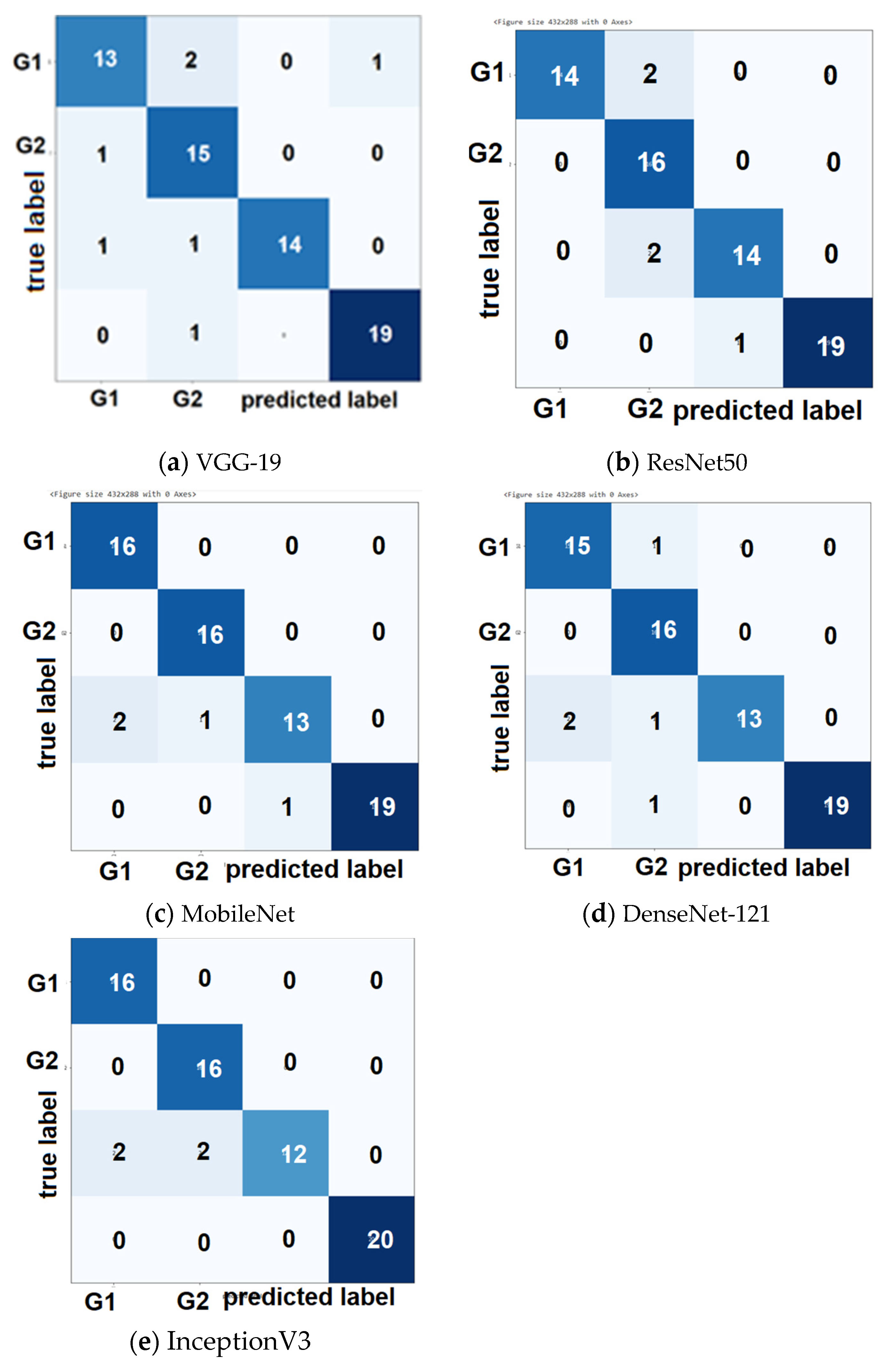
| Test Accuracy | 90 | 92 | 94 | 92 | 93 |
| Test Sensitivity | 89 | 93 | 94 | 93 | 94 |
| Test Precision | 90 | 93 | 94 | 93 | 94 |
| Reference | Objective | Classification Type | Method | Year | Accuracy % |
|---|---|---|---|---|---|
| [17] | Detect BACs in real time using mammograms | 2 class | Simple context U-net ( SCU-Net) | 2021 | 95 |
| [46] | Compute the quantity of BACs and also determine vessel calcification in the breast as a detector | 4 class | Remove the extra black space from the mammograms and apply different algorithms. | 2019 | 81.8 |
| [13] | Determine the performance of deep learning for vascular extraction | 2 class | A retrospective analysis was used to determine the performance of the 2 classes | 2020 | 98 |
| [18] | Detect the presence and severity of BACs from mammograms | 2 class | CNN | 2017 | 62.61 |
| [21] | Detect the presence and severity of 2 class BACs from mammograms | 2 class | A handcrafted method with medical imaging technique | 2019 | 82 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, R.; Masala, G.L. Detecting Breast Arterial Calcifications in Mammograms with Transfer Learning. Electronics 2023, 12, 231. https://doi.org/10.3390/electronics12010231
Khan R, Masala GL. Detecting Breast Arterial Calcifications in Mammograms with Transfer Learning. Electronics. 2023; 12(1):231. https://doi.org/10.3390/electronics12010231
Chicago/Turabian StyleKhan, Rimsha, and Giovanni Luca Masala. 2023. "Detecting Breast Arterial Calcifications in Mammograms with Transfer Learning" Electronics 12, no. 1: 231. https://doi.org/10.3390/electronics12010231