


Design and Evaluation of a Personal Robot Playing a Self-Management for Children with Obesity

Abstract
:1. Introduction
- Develop a social robot architecture to deal with children with obesity.
- Validate the acceptability of social robots with children with obesity through a pilot study.
- Discuss the results obtained from the pilot study.
2. Related Works
3. Obesity Management System Design
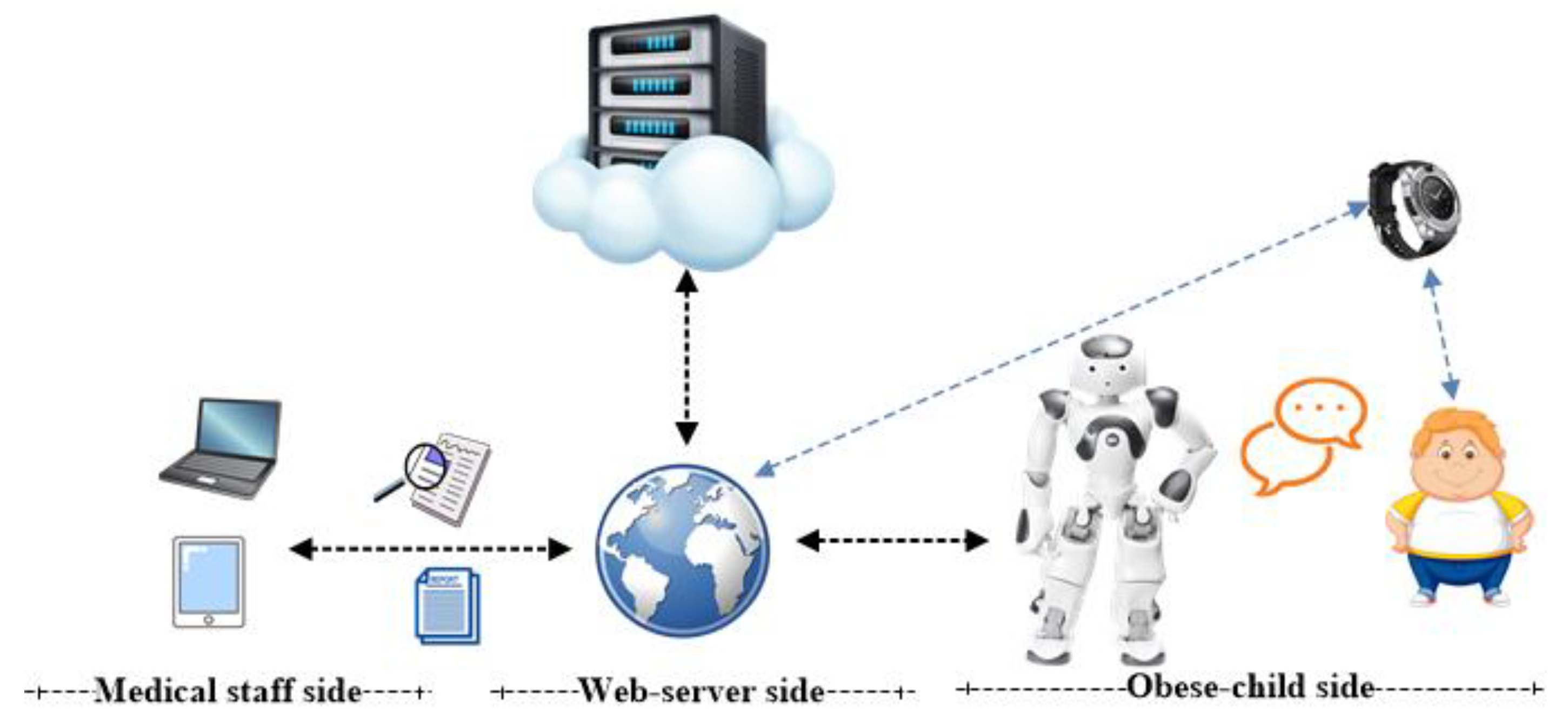
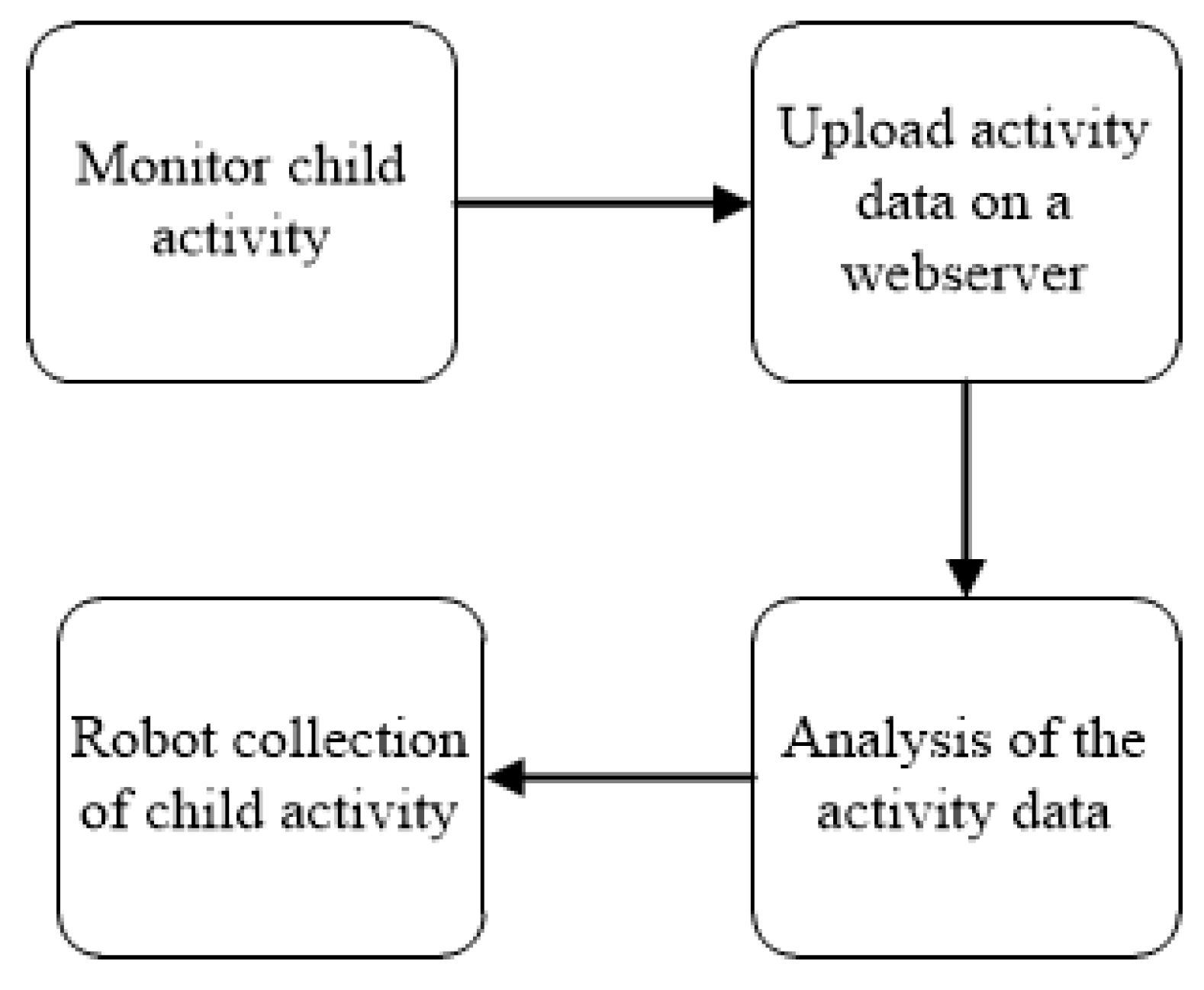
3.1. System Design
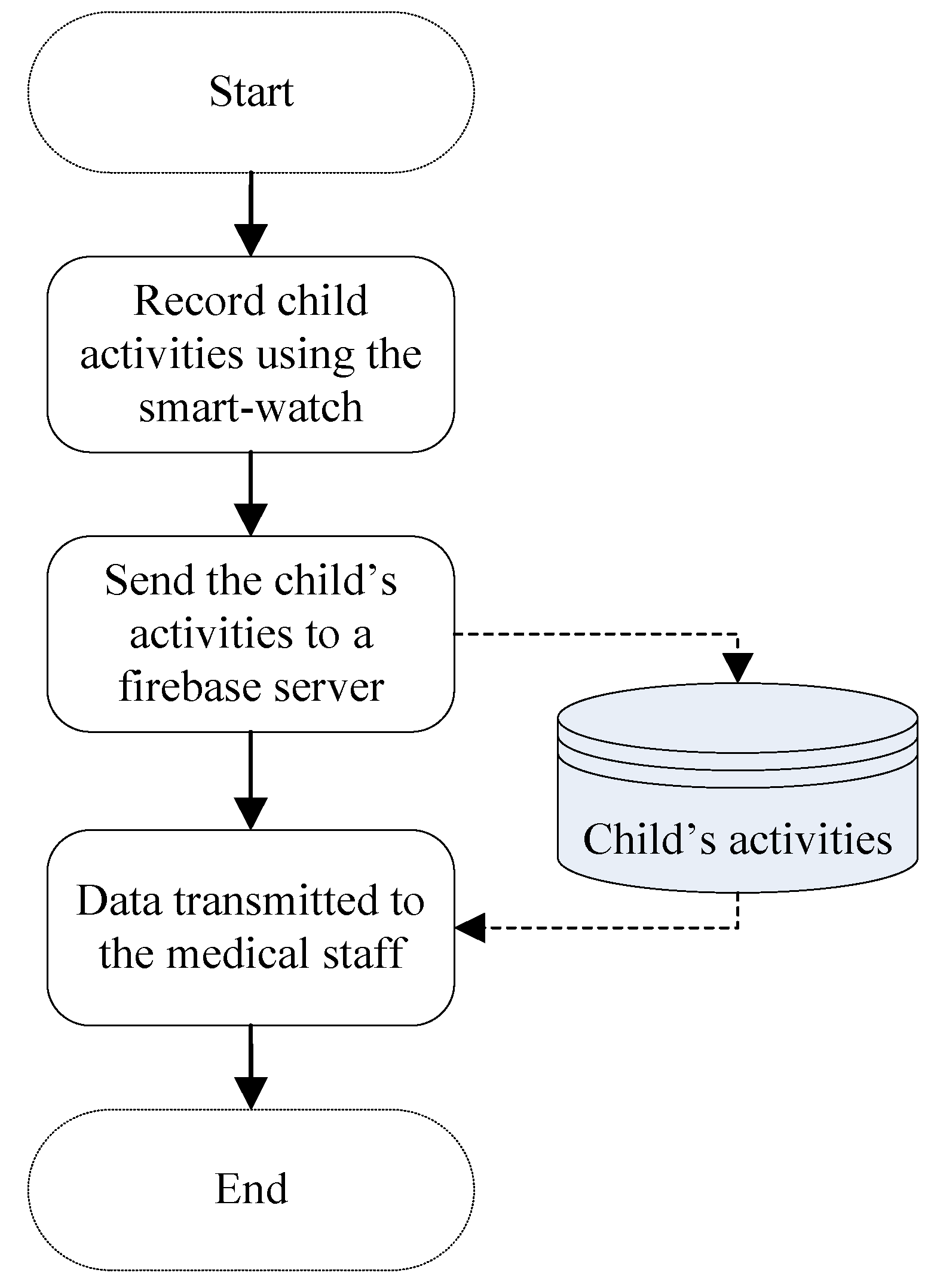
- Monitoring child-activity: This includes a smart-watch unit that incorporated an intelligent system that could monitor, record, and transmit the child’s activities during the daytime. The child’s general activities (active/inactive, number of steps, and the activity in the whole daytime) were collected and processed on the monitoring unit.
- Upload activity data on a webserver: The processed data were then transmitted to the firebase webserver to allow this data to be available for the medical staff and the robot system.
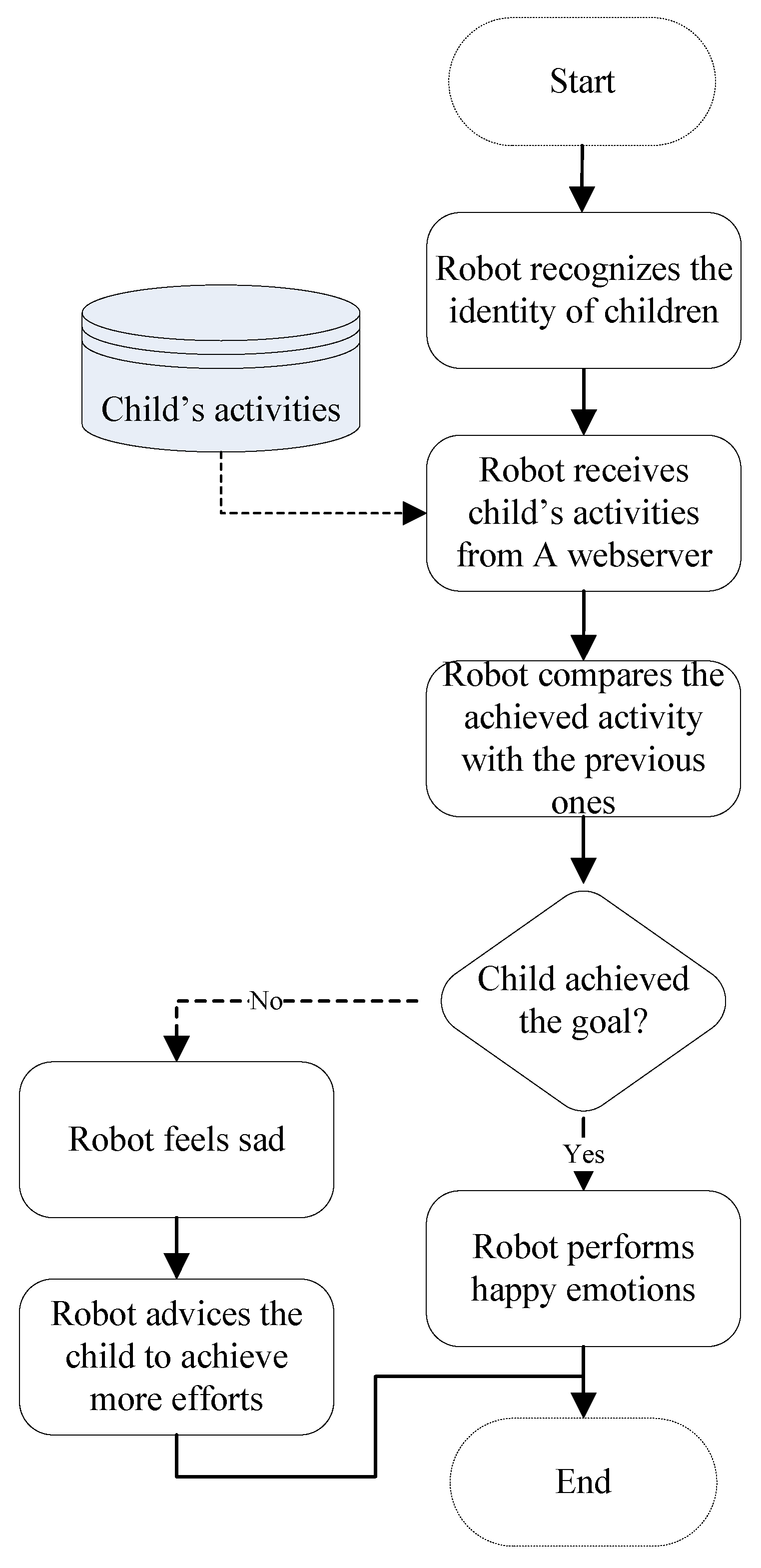
- Analyzing the collected data: The collected data were processed and analyzed according to the previous child’s activities recorded in the database and according to the child’s general status.
- Robot collection of child-activity: In this stage, the robot collected the analyzed data and interacted with the obese child.
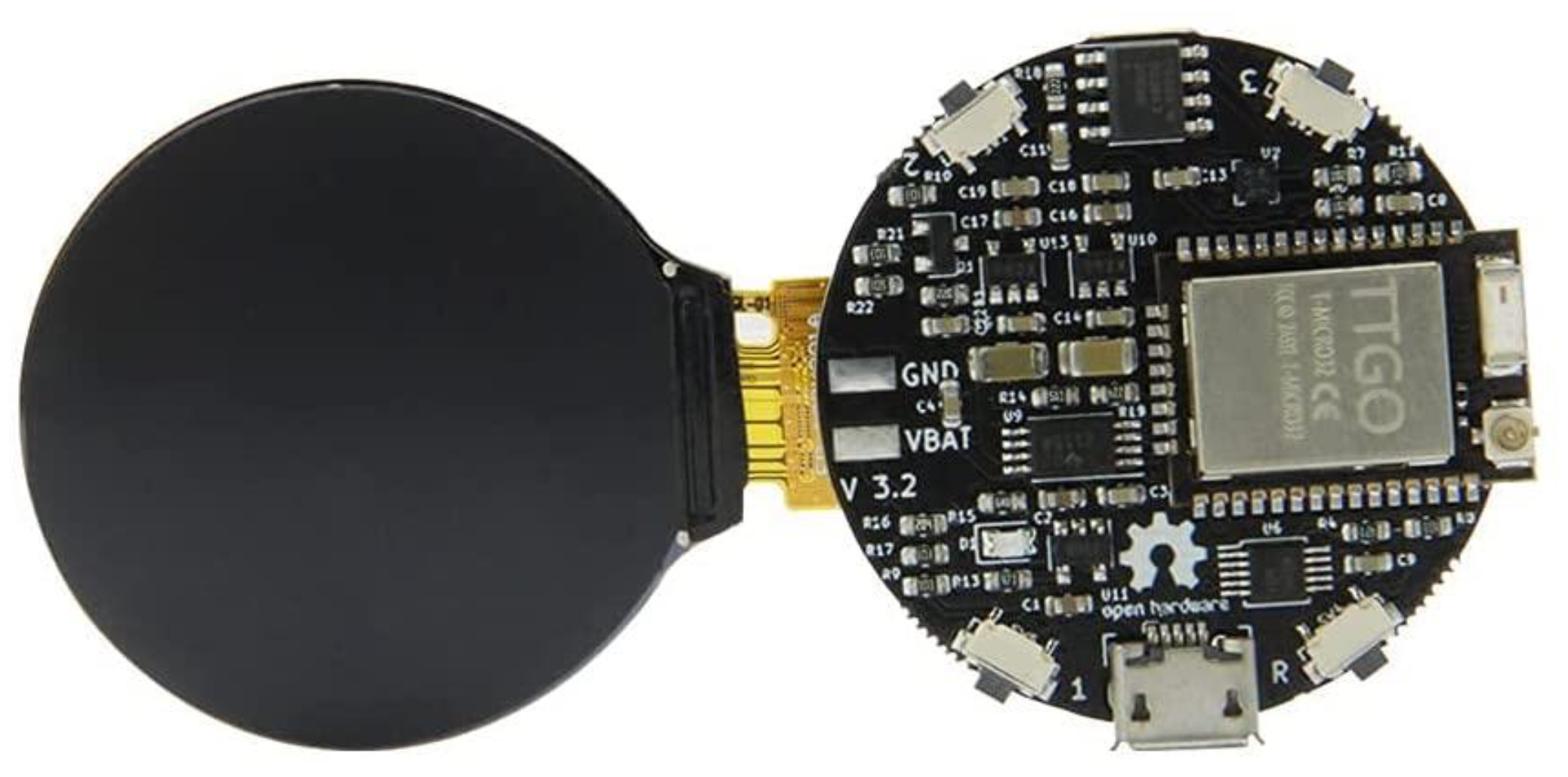
3.2. Hardware Design
- Active time refers to the total time the child is active in the daytime, where the child may be walking, playing, running, etc.
- Number of steps refers to the total number of steps that are accomplished by the child during the day.
- Inactive time refers to total time the child is inactive, for instance, sitting down, laying, etc.
- Sleep time refers to the total sleep time for the child during the day.
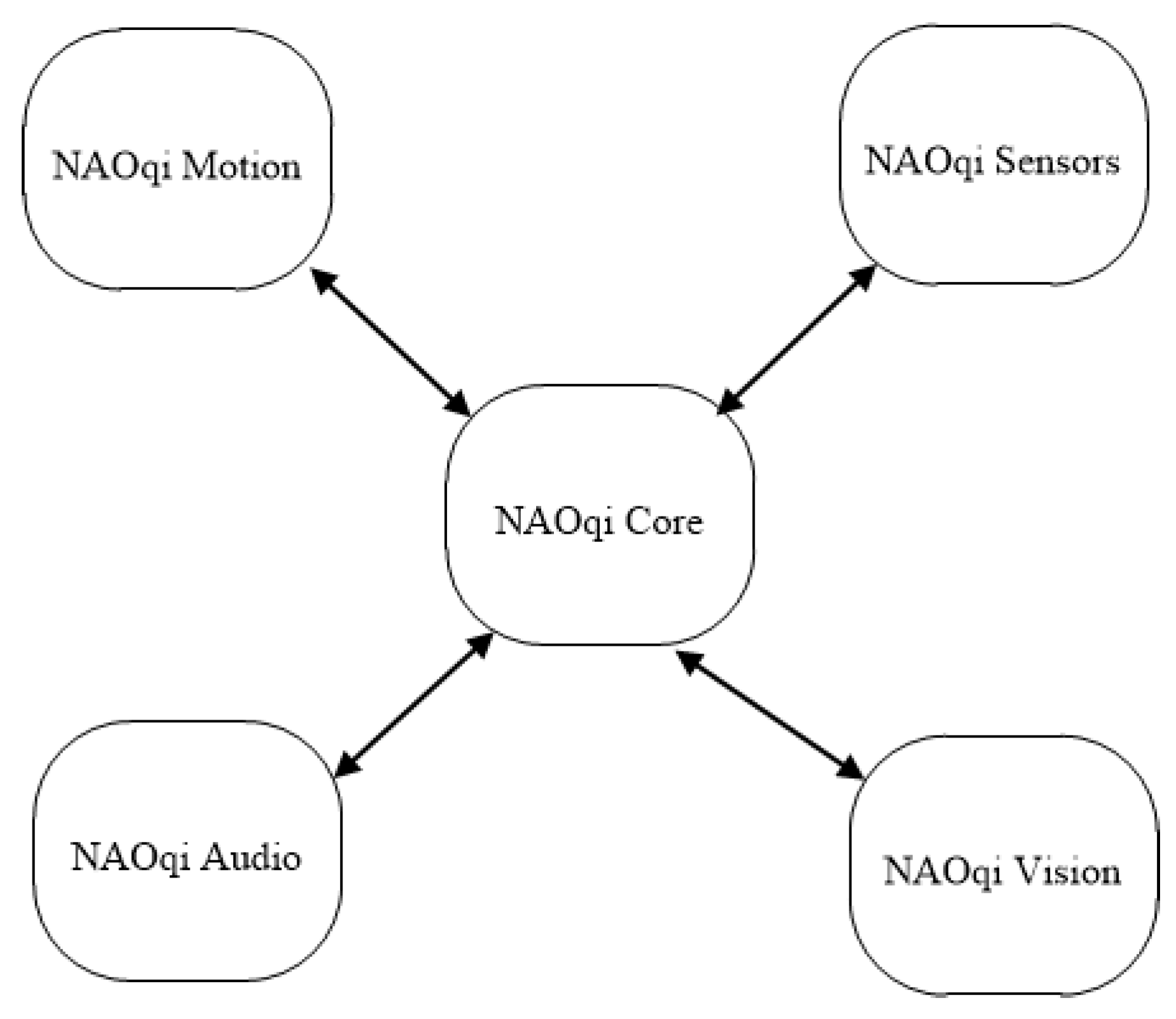
3.3. Software Architecture
- NAOqi Core: This includes a list of core modules where every module offers a set of methods. The developed robotic system employed a set of core modules that handle core operations, such as start and stop behaviors and managing connections between different modules.
- NAOqi Motion: This package involves several methods that allow the NAO robot to move and perform several actions. For instance, NAO moves hands when it interacts with the obese children. In addition, NAOqi Motion offers a set of functionalities that allow the NAO robot to perform navigation and movement.
- NAOqi Audio: This involves the audio software components of the NAO robot platform. In the proposed system, the NAO robot is able to interact with the obese child through a voice recognition system, where the NAO robot may communicate with the obese child using the Arabic language. This also includes the text-to-speech functions and speech recognition functions.
- NAOqi Vision: This contains a set of vision components for the NAO robot platform. The developed robot system is able to recognize the identity of a child using a face recognition application. This helps the robot to correctly retrieve the child’s activities during the last few days in order to perform the suitable action accordingly.
- NAOqi Sensors: This involves a set of modules that allows the developers to interact with the sensors available in the NAO robot. The NAO robot platform is equipped with a set of sensors, including the range-finder sensors that allow the robot to detect the presence of heading objects and tactile sensors that detect whenever the NAO robot is touched by the obese child.
4. Results
4.1. Participants Information
4.2. Experiment Design
4.3. System Evaluation
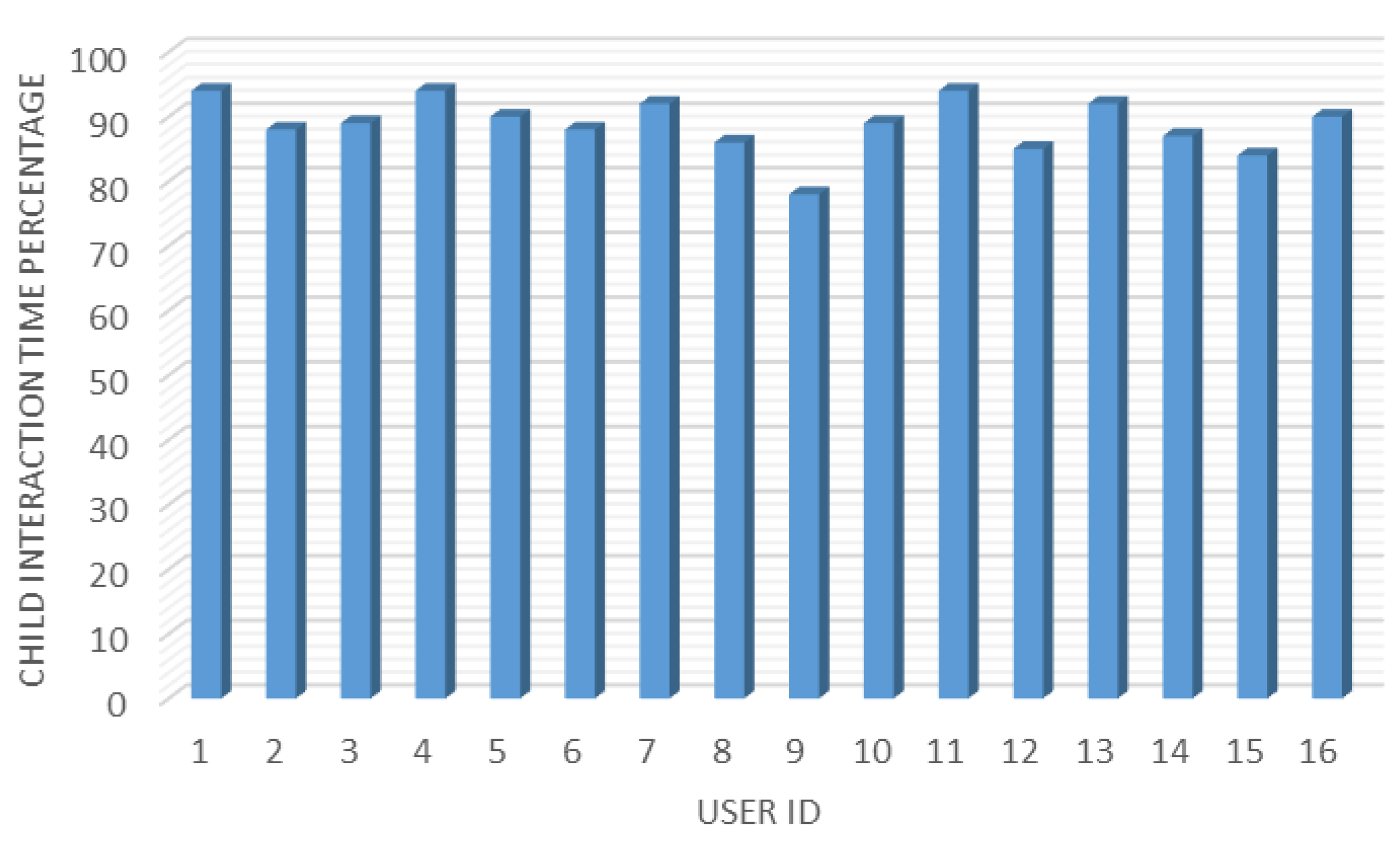
- Interaction time: This estimates the average interaction time between the obese children and the robot system. Total interaction time should offer positive feedback on the acceptability level of social robots (NAO robot platform in our case).
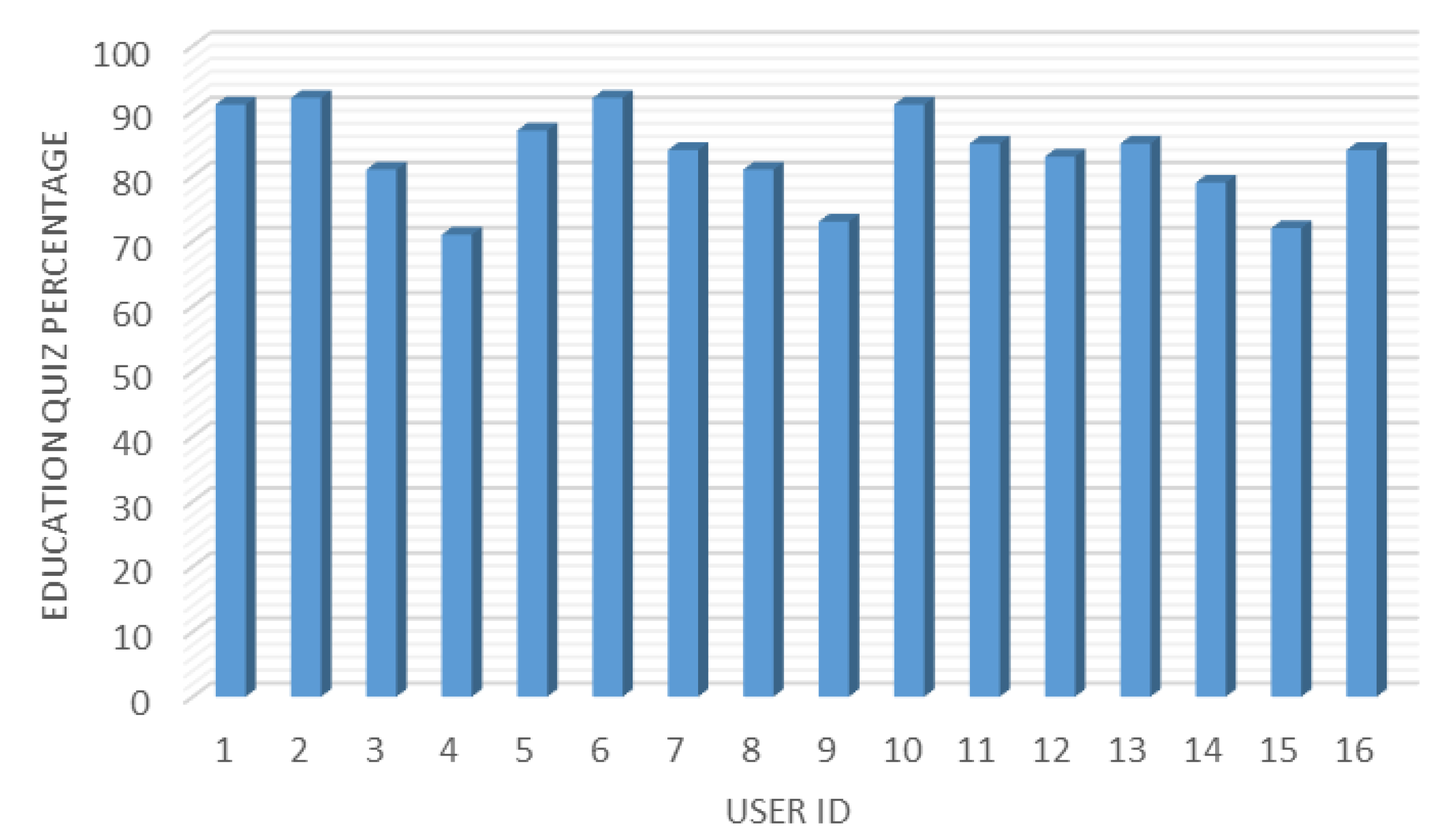
- Education quiz: This measures the average results obtained from the education quiz offered by the robot and the knowledge received by the obese children.
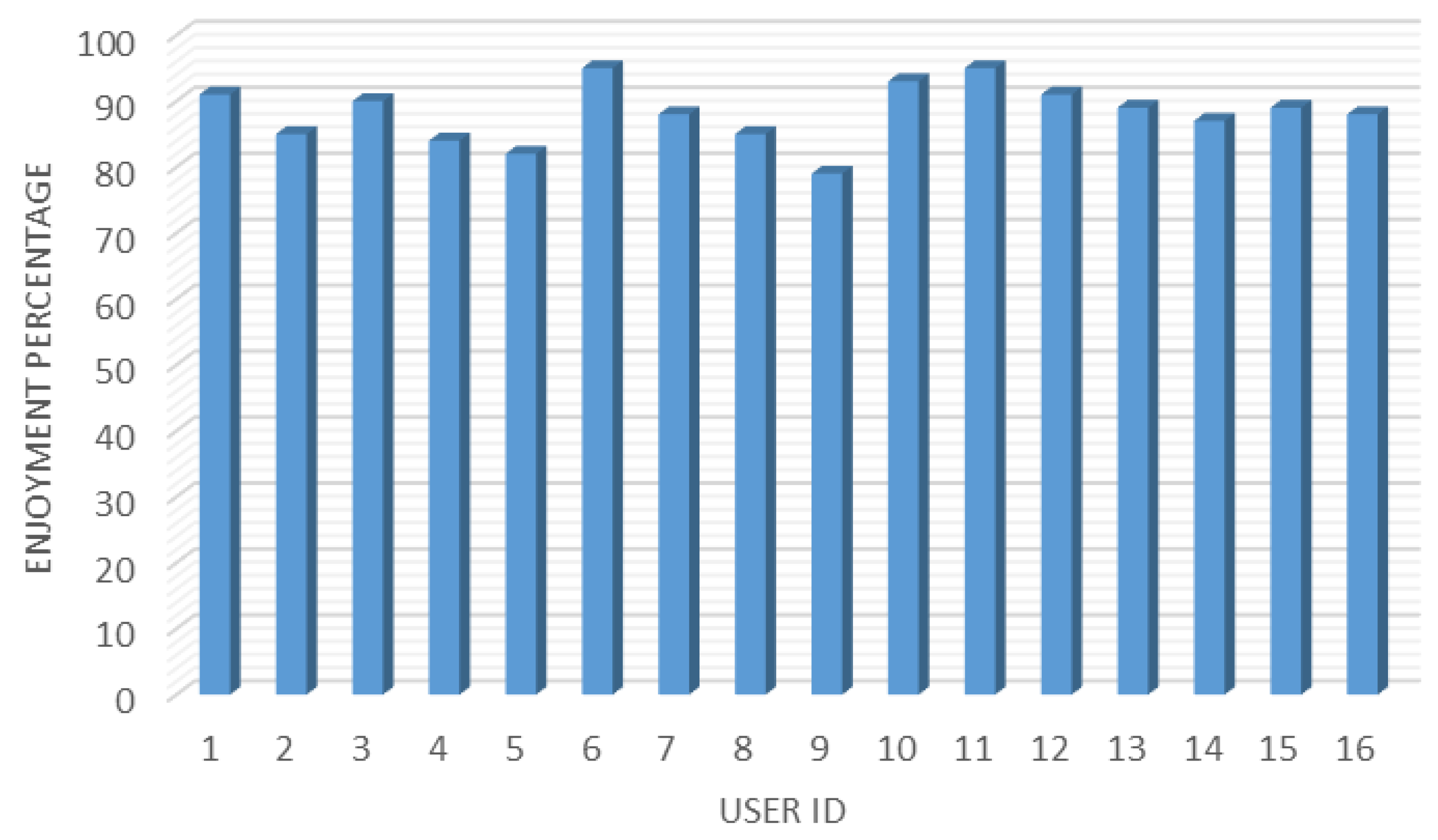
- Enjoyment: This indicates how often the obese child enjoyed interacting with the robot system. Hence, the enjoyment should offer a good indication of the obese children’s acceptability level of social robots.
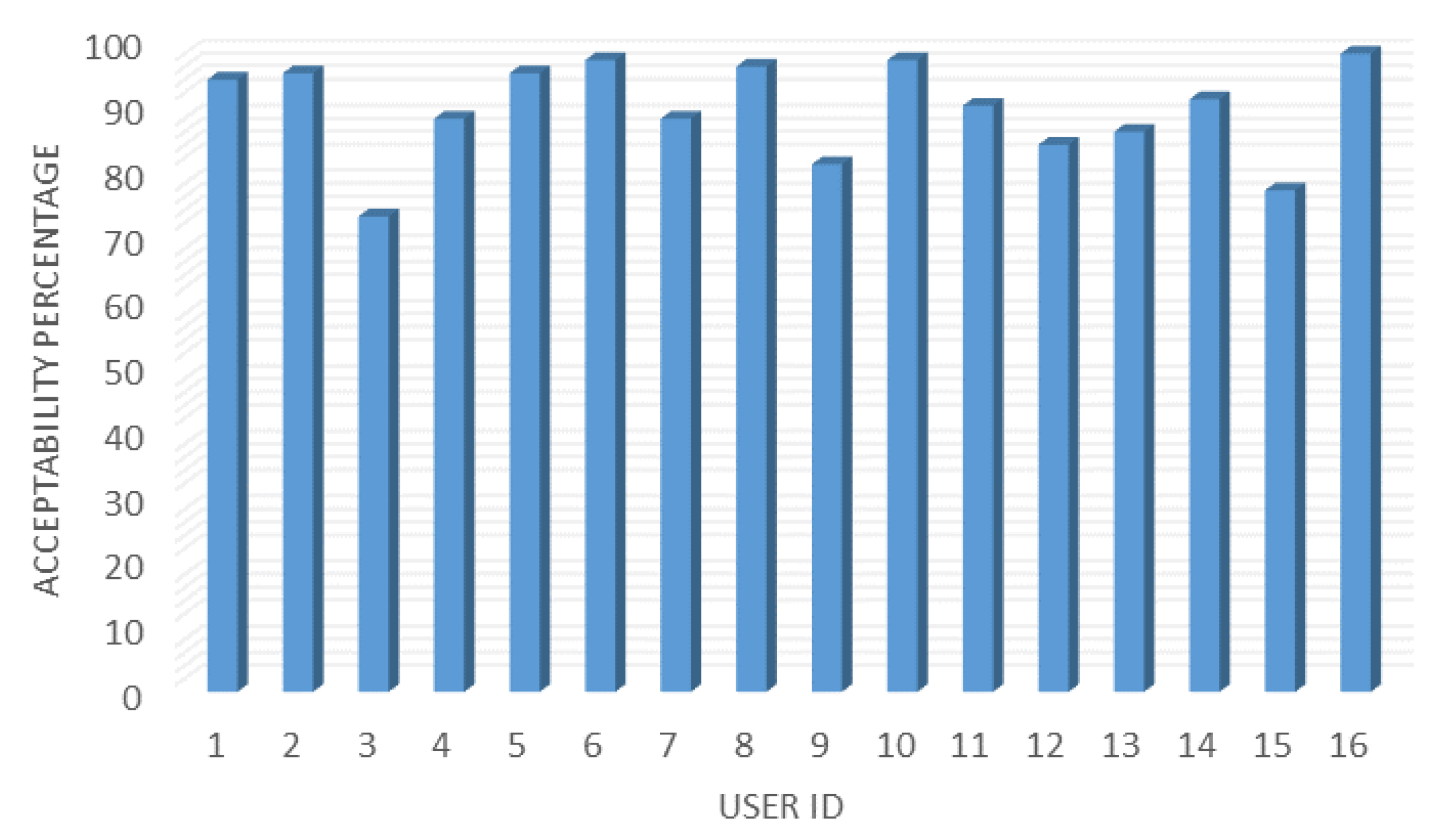
- Acceptability: This measures the average acceptability of the social robot platform by the obese children during the engagement sessions for the whole experiment time.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ferrara, L. Focus on Body Mass Index and Health Research; Nova Science Publishers: New York, NY, USA, 2006. [Google Scholar]
- Elflein, J. Overweight Prevalence by Age Worldwide 2019|Statista, Statista. 2022. Available online: https://www.statista.com/statistics/1065605/prevalence-overweight-people-worldwide-by-age/ (accessed on 20 September 2022).
- World Health Organization. Obesity and Overweight, Who.int. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 20 September 2022).
- Worldobesity.org. World Obesity Federation|Data. 2022. Available online: https://www.worldobesityday.org/assets/downloads/World_Obesity_Atlas_2022_WEB.pdf (accessed on 20 September 2022).
- Alqarni, S.M. A Review of Prevalence of Obesity in Saudi Arabia. J. Obes. Eat. Disord. 2016, 2, 2. [Google Scholar] [CrossRef]
- Yoon, K.; Kim, H. A short message service by cellular phone in type 2 diabetic patients for 12 months. Diabetes Res. Clin. Pract. 2008, 79, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.; Nguyen, X.; Lane, J.; Wang, P. Relationship Between Obesity and Diabetes in a US Adult Population: Findings from the National Health and Nutrition Examination Survey, 1999–2006. Obes. Surg. 2010, 21, 351–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckel, R.H.; Kahn, S.E.; Ferrannini, E.; Goldfine, A.B.; Nathan, D.M.; Schwartz, M.W.; Smith, R.J.; Smith, S.R. Obesity and Type 2 Diabetes: What Can Be Unified and What Needs to Be Individualized? J. Clin. Endocrinol. Metab. 2011, 96, 1654–1663. [Google Scholar] [CrossRef] [Green Version]
- Rössner, S. Obesity and type 2 diabetes. Pract. Diabetes Int. 2001, 18, 263–264. [Google Scholar] [CrossRef]
- Aljoudi, A.; Mwanri, L.; Al Dhaifallah, A. Childhood obesity in Saudi Arabia: Opportunities and challenges. Saudi J. Obes. 2015, 3, 2. [Google Scholar] [CrossRef]
- Alotaibi, M.; Istepanian, R.; Philip, N. A mobile diabetes management and educational system for type-2 diabetics in Saudi Arabia (SAED). mHealth 2016, 2, 33. [Google Scholar] [CrossRef] [Green Version]
- Liang, X.; Wang, Q.; Yang, X.; Cao, J.; Chen, J.; Mo, X.; Huang, J.; Wang, L.; Gu, D. Effect of mobile phone intervention for diabetes on glycaemic control: A meta-analysis. Diabet. Med. 2011, 28, 455–463. [Google Scholar] [CrossRef]
- Colmenarejo, G. Machine learning models to predict childhood and adolescent obesity: A review. Nutrients 2020, 12, 2466. [Google Scholar] [CrossRef]
- Su, J.; Dugas, M.; Guo, X.; Gao, G. Influence of Personality on mHealth Use in Patients with Diabetes: Prospective Pilot Study. JMIR Mhealth Uhealth 2020, 8, e17709. [Google Scholar] [CrossRef]
- Lee, M.; Park, C.; Park, S.; Lee, D.; Sung, J. Implementation and Evaluation of Gestational Diabetes Management Using Mobile Health Care Service—A Pilot Study. Diabetes 2018, 67, 708. [Google Scholar] [CrossRef]
- Triantafyllidis, A.; Alexiadis, A.; Elmas, D.; Votis, K.; Tzovaras, D. A Social Robot-Based Platform for Prevention of Childhood Obesity. In Proceedings of the International Conference on Bioinformatics and Bioengineering (BIBE), Athens, Greece, 28–30 October 2019; pp. 914–917. [Google Scholar]
- De Jong, C.; Kühne, R.; Peter, J.; van Straten, C.; Barco, A. Intentional acceptance of social robots: Development and validation of a self-report measure for children. Int. J. Hum.-Comput. Stud. 2020, 139, 102426. [Google Scholar] [CrossRef]
- Logan, D.E.; Breazeal, C.; Goodwin, M.S.; Jeong, S.; O’Connell, B.; Smith-Freedman, D.; Heathers, J.; Weinstock, P. Social Robots for Hospitalized Children. Pediatrics 2019, 144, e20181511. [Google Scholar] [CrossRef] [PubMed]
- De Jong, C.; Peter, J.; Kühne, R.; Barco, A. Children’s acceptance of social robots. Interact. Stud. 2019, 20, 393–425. [Google Scholar] [CrossRef]
- Hu, F.B.; Rimm, E.; Smith-Warner, S.A.; Feskanich, D.; Stampfer, M.J.; Ascherio, A.; Sampson, L.; Willett, W.C. Reproducibility and validity of dietary patterns assessed with a food-frequency questionnaire. Am. J. Clin. Nutr. 1999, 69, 243–249. [Google Scholar] [CrossRef] [Green Version]
- Janz, K.; Lutuchy, E.; Wenthe, P.; Levy, S. Measuring Activity in Children and Adolescents Using Self-Report. Med. Sci. Sport. Exerc. 2008, 40, 767–772. [Google Scholar] [CrossRef]
- Alexiadis, A.; Triantafyllidis, A.; Elmas, D.; Gerovasilis, G.; Votis, K.; Tzovaras, D. A Social Robot-based Platform towards Automated Diet Tracking. In Proceedings of the Conference on Computer Science and Information Systems (FedCSIS), Sofia, Bulgaria, 6–9 September 2020; pp. 11–14. [Google Scholar]
- Vrochidou, E.; Najoua, A.; Lytridis, C.; Salonidis, M.; Ferelis, V.; Papakostas, G.A. Social robot NAO as a self-regulating didactic mediator: A case study of teaching/learning numeracy. In Proceedings of the International Conference on Software, Telecommunications and Computer Networks (SoftCOM), Split, Croatia, 13–15 September 2018; pp. 1–5. [Google Scholar]
- Onyeulo, E.B.; Gandhi, V. What makes a social robot good at interacting with humans? Information 2020, 11, 43. [Google Scholar] [CrossRef] [Green Version]
- Filippini, C.; Perpetuini, D.; Cardone, D.; Merla, A. Improving Human–Robot Interaction by Enhancing NAO Robot Awareness of Human Facial Expression. Sensors 2021, 21, 6438. [Google Scholar] [CrossRef]
- Estévez, D.; Terrón-López, M.J.; Velasco-Quintana, P.J.; Rodríguez-Jiménez, R.M.; Álvarez-Manzano, V. A case study of a robot-assisted speech therapy for children with language disorders. Sustainability 2021, 13, 2771. [Google Scholar] [CrossRef]
- American Heart Association. American Heart Association Recommendations for Physical Activity in Adults and Kids, www.heart.org. 2022. Available online: https://www.heart.org/en/healthy-living/fitness/fitness-basics/aha-recs-for-physical-activity-in-adults (accessed on 20 September 2022).
- Best, K.; Ball, K.; Zarnowiecki, D.; Stanley, R.; Dollman, J. In search of consistent predictors of children’s physical activity. Int. J. Environ. Res. Public Health 2017, 14, 1258. [Google Scholar] [CrossRef]
- Charlier, N.; Zupancic, N.; Fieuws, S.; Denhaerynck, K.; Zaman, B.; Moons, P. Serious games for improving knowledge and self-management in young people with chronic conditions: A systematic review and meta-analysis. J. Am. Med. Inform. Assoc. 2015, 23, 230–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henkemans, O.A.B.; Bierman, B.P.; Janssen, J.; Looije, R.; Neerincx, M.A.; van Dooren, M.M.; de Vries, J.L.; van der Burg, G.J.; Huisman, S.D. Design and evaluation of a personal robot playing a self-management education game with children with diabetes type 1. Int. J. Hum.-Comput. Stud. 2017, 106, 63–76. [Google Scholar] [CrossRef] [Green Version]
- Edwards, J.; Waite-Jones, J.; Schwarz, T.; Swallow, V. Digital technologies for children and parents sharing self-management in childhood chronic or long-term conditions: A scoping review. Children 2021, 8, 1203. [Google Scholar] [CrossRef] [PubMed]
- Saxby, N.; Beggs, S.; Battersby, M.; Lawn, S. What are the components of effective chronic condition self-management education interventions for children with asthma, cystic fibrosis, and diabetes? A systematic review. Patient Educ. Couns. 2019, 102, 607–622. [Google Scholar] [CrossRef]
- Nabors, L.; Bernstein, J.; Winders, T.; Hart, M.; Toledano-Toledano, F. Needs assessment: Knowledge of self-management of asthma for children with co-morbid physical and intellectual disabilities: Brief report. J. Asthma 2021, 59, 712–718. [Google Scholar] [CrossRef]
- Qidwai, U.; Kashem, S.; Conor, O. Humanoid Robot as a Teacher’s Assistant: Helping Children with Autism to Learn Social and Academic Skills. J. Intell. Robot. Syst. 2019, 98, 759–770. [Google Scholar] [CrossRef]
- Arent, K.; Kruk-Lasocka, J.; Niemiec, T.; Szczepanowski, R. Social robot in diagnosis of autism among preschool children. In Proceedings of the International Conference on Methods and Models in Automation and Robotics (MMAR), Miedzyzdroje, Poland, 26–29 August 2019; pp. 652–656. [Google Scholar]
- Kaptein, F.; Kiefer, B.; Cully, A.; Celiktutan, O.; Bierman, B.; Rijgersberg-Peters, R.; Broekens, J.; Van Vught, W.; Van Bekkum, M.; Demiris, Y.; et al. A Cloud-based Robot System for Long-term Interaction: Principles, Implementation, Lessons Learned. ACM Trans. Hum.-Robot. Interact. 2022, 11, 1–27. [Google Scholar] [CrossRef]
- Cañete Yaque, R.; Svarrer Larsen, H.; Peralta Alvarez, M. Pepe: An adaptive robot that helps children with autism to plan and self-manage their day. In 11th International Conference on the Internet of Things; ACM: New York, NY, USA, 2021. [Google Scholar]
- Alotaibi, M.; Alnajjar, F.; Cappuccio, M.; Khalid, S.; Alhmiedat, T.; Mubin, O. Efficacy of Emerging Technologies to Manage Childhood Obesity. Diabetes Metab. Syndr. Obes. Targets Ther. 2022, 15, 1227–1244. [Google Scholar] [CrossRef]
- Kidd, C.D.; Breazeal, C. Effect of a robot on user perceptions. In Proceedings of the 2004 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS) (IEEE Cat. No.04CH37566), Sendai, Japan, 28 September–2 October 2004; Volume 4, pp. 3559–3564. [Google Scholar]
- Ferrari, E.; Robins, B.; Dautenhahn, K. Therapeutic and educational objectives in robot assisted play for children with autism. In Proceedings of the RO-MAN 2009—The 18th IEEE International Symposium on Robot and Human Interactive Communication, Toyama, Japan, 27 September–2 October 2009; pp. 108–114. [Google Scholar]
- Köse, H.; Uluer, P.; Akalın, N.; Yorgancı, R.; Özkul, A.; Ince, G. The Effect of Embodiment in Sign Language Tutoring with Assistive Humanoid Robots. Int. J. Soc. Robot. 2015, 7, 537–548. [Google Scholar] [CrossRef]
- Demiris, Y. Knowing when to assist: Developmental issues in lifelong assistive robotics. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009. [Google Scholar]
- Vygotsky, L.S. Mind in Society: The Development of Higher Psychological Processes; Harvard University Press: Cambridge, MA, USA, 1980. [Google Scholar]
- Al-Taee, M.; Al-Nuaimy, W.; Muhsin, Z.; Al-Ataby, A. Robot Assistant in Management of Diabetes in Children Based on the Internet of Things. IEEE Internet Things J. 2017, 4, 437–445. [Google Scholar] [CrossRef]
- Neggers, M.M.E.; Ruijten, P.A.M.; Cuijpers, R.H. Investigating Experiences with a Robot Teaching Children Self-Management: A Field Trial. In Proceedings of the 2021 30th IEEE International Conference on Robot & Human Interactive Communication (RO-MAN), Vancouver, BC, Canada, 8–12 August 2021; pp. 592–597. [Google Scholar]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Children # | Gender | Age | Weight | Length | Overweight % |
|---|---|---|---|---|---|
| 1 | M | 7 | 41 | 119 | 28.9 |
| 2 | F | 8 | 43 | 122 | 28.8 |
| 3 | M | 7 | 45 | 118 | 32.3 |
| 4 | M | 10 | 53 | 144 | 25.6 |
| 5 | M | 9 | 52 | 142 | 26.2 |
| 6 | F | 7 | 38 | 114 | 29.2 |
| 7 | M | 8 | 38 | 120 | 26.4 |
| 8 | F | 10 | 52 | 148 | 23.7 |
| 9 | M | 7 | 36 | 116 | 26.8 |
| 10 | M | 8 | 45.5 | 123 | 30.1 |
| 11 | M | 8 | 43 | 121 | 29.4 |
| 12 | M | 9 | 43 | 126 | 27.1 |
| 13 | F | 10 | 52 | 146 | 24.4 |
| 14 | M | 7 | 41.5 | 116 | 30.8 |
| 15 | F | 8 | 42.5 | 123 | 28.1 |
| 16 | M | 10 | 56.6 | 152 | 24.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhmiedat, T.; Alotaibi, M. Design and Evaluation of a Personal Robot Playing a Self-Management for Children with Obesity. Electronics 2022, 11, 4000. https://doi.org/10.3390/electronics11234000
Alhmiedat T, Alotaibi M. Design and Evaluation of a Personal Robot Playing a Self-Management for Children with Obesity. Electronics. 2022; 11(23):4000. https://doi.org/10.3390/electronics11234000
Chicago/Turabian StyleAlhmiedat, Tareq, and Mohammed Alotaibi. 2022. "Design and Evaluation of a Personal Robot Playing a Self-Management for Children with Obesity" Electronics 11, no. 23: 4000. https://doi.org/10.3390/electronics11234000