


System for Non-Contact and Multispectral Examination of Blood Supply to Cutaneous Tissue

Abstract
:1. Introduction
2. Materials and Methods
2.1. System Functional Description
2.2. System Operation Based on Timing Diagram
2.3. Adjustability of Illumination Device
2.4. Three-Channel Linear LED Driver
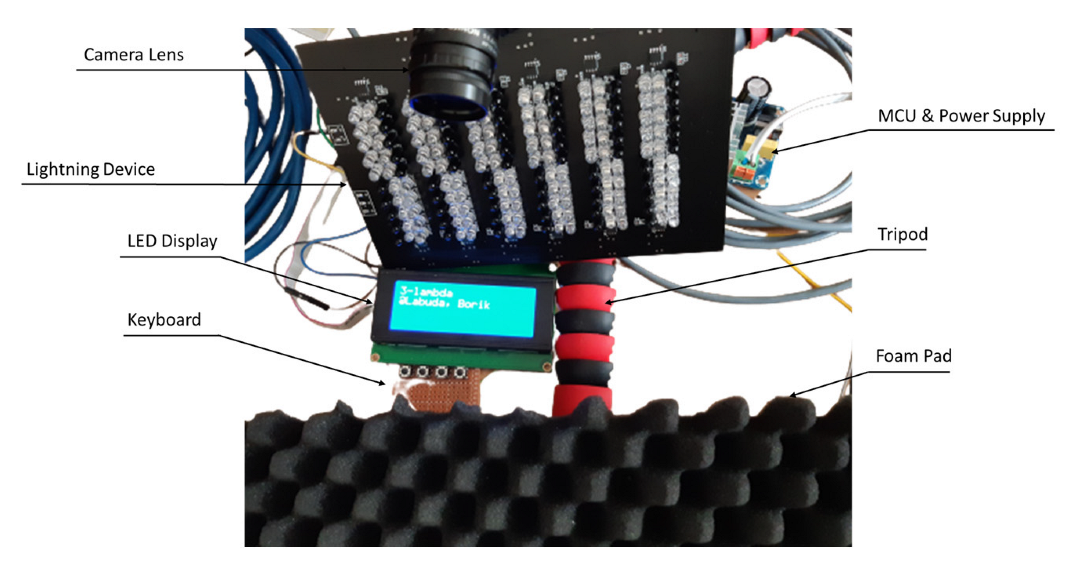
2.5. Testing of Illumination Device and Camera Setup
2.6. Software Calibration
3. Results
3.1. Testing the System Timing
3.2. Testing the System Transients
3.3. Measuring PPGI Data
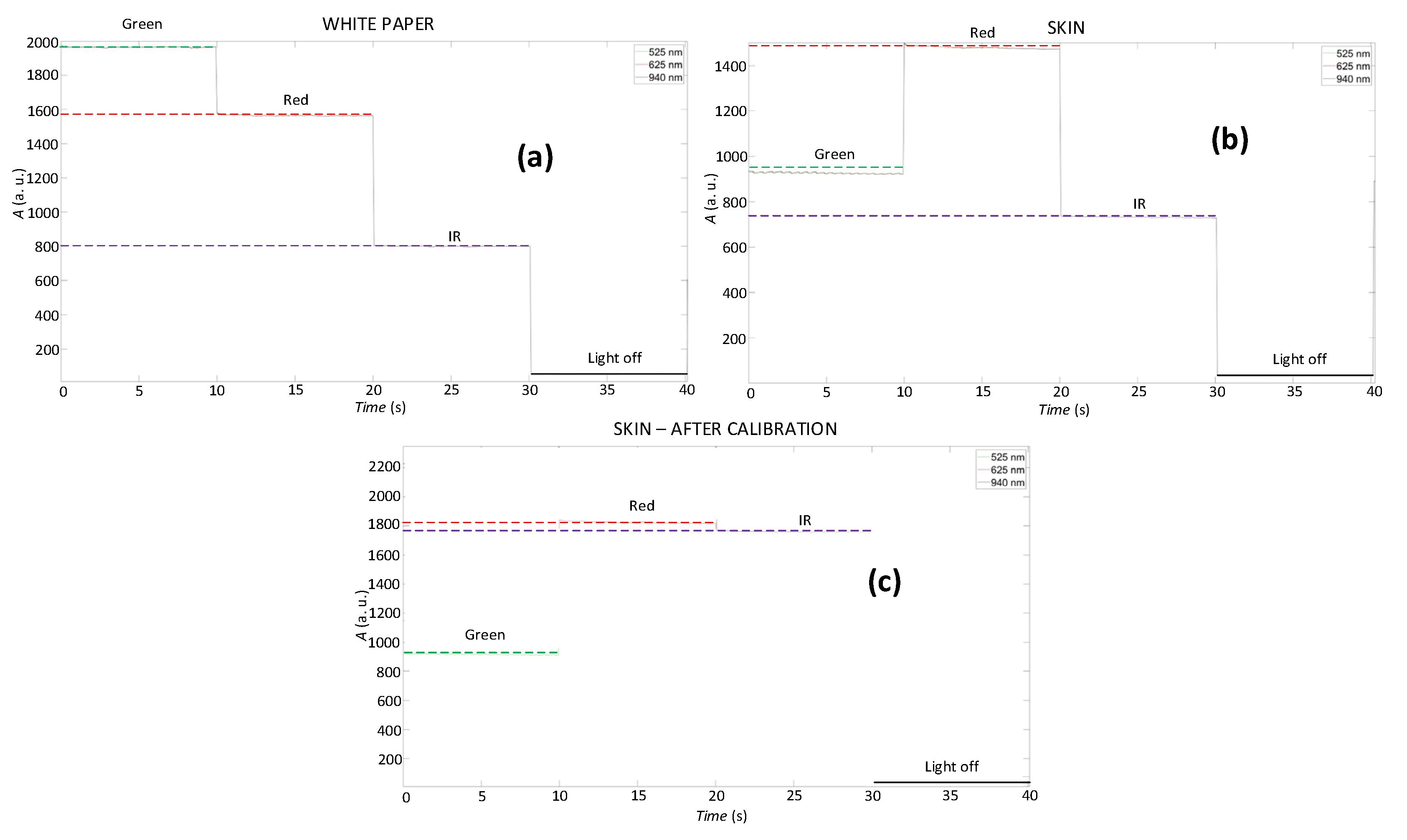
3.4. Amplitude Maps after Calibration
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rushmer, R.F.; Buettner, K.J.K.; Short, J.M.; Odland, G.F. The skin. Science 1966, 80, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Moretti, G. The blood vessels of the skin. In Normale und Pathologische Anatomie der Haut I.; Springer: Berlin/Heidelberg, Germany, 1968; pp. 491–623. [Google Scholar]
- Wong, R.; Geyer, S.; Weninger, W.; Guimberteau, J.; Wong, J.K. The dynamic anatomy and patterning of skin. Exp. Dermatol. 2016, 25, 92–98. [Google Scholar] [CrossRef]
- Korthuis, R.J. Skeletal muscle circulation. Colloq. Ser. Integr. Syst. Physiol. Mol. Funct. 2011, 3, 1–144. [Google Scholar] [CrossRef]
- Frink, M.; Hildebrand, F.; Krettek, C.; Brand, J.; Hankemeier, S. Compartment syndrome of the lower leg and foot. Clin. Orthop. Relat. Res. 2010, 468, 940–950. [Google Scholar] [CrossRef] [PubMed]
- Eberhardt, R.T.; Raffetto, J.D. Chronic venous insufficiency. Circulation 2014, 130, 333–346. [Google Scholar] [CrossRef] [PubMed]
- Yiu, E.M.; Kornberg, A.J. Duchenne muscular dystrophy. J. Paediatr. Child Health 2015, 51, 759–764. [Google Scholar] [CrossRef]
- Staessen, J.A.; Wang, J.; Bianchi, G.; Birkenhäger, W.H. Essential hypertension. Lancet 2003, 361, 1629–1641. [Google Scholar] [CrossRef]
- Bhatnagar, D.; Soran, H.; Durrington, P.N. Hypercholesterolaemia and its management. BMJ 2008, 337, a993. [Google Scholar] [CrossRef]
- Jiang, S.; Lu, W.; Zong, X.; Ruan, H.; Liu, Y. Obesity and hypertension. Exp. Ther. Med. 2016, 12, 2395–2399. [Google Scholar] [CrossRef]
- Deshpande, A.D.; Harris-Hayes, M.; Schootman, M. Epidemiology of diabetes and diabetes-related complications. Phys. Ther. 2008, 88, 1254–1264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosch, J.; Garcia-Pagán, J.C.; Feu, F.; Pizcueta, M.P. Portal hypertension. In Hepatobiliary Diseases; Springer: Berlin/Heidelberg, Germany, 1992; pp. 429–463. ISBN 9783642768040. [Google Scholar]
- Bereksi-Regiug, M.A.; Bereksi-Reguig, F.; Ali, A.N. A new system for measurement of the pulse transit time, the pulse wave velocity and its analysis. J. Mech. Med. Biol. 2017, 17, 1750010. [Google Scholar] [CrossRef]
- Podoleanu, A.G. Optical coherence tomography. J. Microsc. 2012, 247, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.V. Prospects of photoacoustic tomography. Med. Phys. 2008, 35, 5758–5767. [Google Scholar] [CrossRef]
- Such, O.; Acker, S.; Blazek, V. Mapped hemodynamic data acquisition by near infrared CCD imaging. In Proceedings of the 19th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Magnificent Milestones and Emerging Opportunities in Medical Engineering (Cat. No. 97CH36136), Chicago, IL, USA, 30 October–2 November 1997; Volume 2, pp. 637–639. [Google Scholar] [CrossRef]
- Wu, T.; Blazek, V.; Schmitt, H.J. Photoplethysmography imaging: A new noninvasive and noncontact method for mapping of the dermal perfusion changes. In Optical Techniques and Instrumentation for the Measurement of Blood Composition, Structure, and Dynamics; SPIE: Cergy, France, 2000; Volume 4163, pp. 62–70. [Google Scholar] [CrossRef]
- Hülsbusch, M.; Rembold, B. Ein bildgestütztes, funktionelles Verfahren zur optoelektronischen Erfassung der Hautperfusion. PhD Thesis, Lehrstuhl und Institut für Hochfrequenztechnik, Aachen, Germany, 2008. [Google Scholar]
- Borik, S.; Lyra, S.; Paul, M.; Antink, C.H.; Leonhardt, S.; Blazek, V. Photoplethysmography imaging: Camera performance evaluation by means of an optoelectronic skin perfusion phantom. Physiol. Meas. 2020, 41, 54001. [Google Scholar] [CrossRef] [PubMed]
- Blazek, V.; Dahlmanns, S.; Pereira, C.B.; Yu, X.; Blanik, N.; Leonhardt, S.; Blazek, C.R. Photoplethysmography Imaging and Common Optical Hybrid Imaging Modalities. In Multi-Modality Imaging; Springer: Cham, Switzerland, 2018; pp. 31–66. [Google Scholar] [CrossRef]
- Bergstrand, S.; Lindberg, L.G.; Ek, A.; Lindén, M.; Lindgren, M. Blood flow measurements at different depths using photoplethysmography and laser Doppler techniques. Ski. Res. Technol. 2009, 15, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Huelsbusch, M.; Blazek, V. Rhythmical Phenomena in Dermal Perfusion-Proved Assesment Strategies and new Discoveries. Adv. Electr. Electron. Eng. 2011, 4, 112–117. [Google Scholar]
- Huelsbusch, M.; Blazek, V. Contactless mapping of rhythmical phenomena in tissue perfusion using PPGI. In Medical Imaging 2002: Physiology and Function from Multidimensional Images; SPIE: Cergy, France, 2002; Volume 4683, pp. 110–117. [Google Scholar] [CrossRef]
- Blazek, C.; Blazek, V. Selected Clinical Applications of Functional PPGI Perfusion Mapping in Dermatology. In Studies in Skin Perfusion Dynamics; Springer: Berlin/Heidelberg, Germany, 2021; pp. 207–221. [Google Scholar] [CrossRef]
- Wieringa, F.P.; Mastik, F.; van der Steen, A.F.W. Contactless multiple wavelength photoplethysmographic imaging: A first step toward ‘SpO2 camera’ technology. Ann. Biomed. Eng. 2005, 33, 1034–1041. [Google Scholar] [CrossRef]
- Optosupply. OSG59A5111P, 525 nm LED. Technology Datasheet, Version. A.0. 2011. Available online: https://www.micros.com.pl/en/optoelectronics/ (accessed on 6 July 2022).
- Optosupply. OS6YKA5201P, 625 nm LED. Version A.0. 2011. Available online: http://www.optosupply.com/search/result.asp (accessed on 6 July 2022).
- Osram. SFH 4544, 940 nm LED. Version 1.6. 2021. Available online: https://www.osram.com/ecat/com/en/class_pim_web_catalog_103489/prd_pim_device_2219771/ (accessed on 6 July 2022).
- AIMTEC. Training Applications AMES100-277NZ Models & Specifications. 2017. Available online: https://aimtec.com/index.aspx?a=SerieUp.List&ConverterTypeId=&undefined_SeriesCurrent=undefined&undefined_SeriesWattage=undefined&SerieSearch=AMES100-277NZ (accessed on 6 July 2022).
- Technology, M. 3-Channel, 20mA, Linear LED Driver CL320. Version. DSFP-CL320A091508. 2017. Available online: https://www.microchip.com/en-us/product/CL320 (accessed on 6 July 2022).
- Panavision. Lee 250 Half White Diffusion filter & Lee 216 Full White Diffusion Filter. Version 1.0. 2022. Available online: https://leefilters.com/colour/250-half-white-diffusion/ (accessed on 6 July 2022).
- Blackfly®s. BFS-U3-28S5. Revised 1/29/2019. 2019. Available online: http://softwareservices.flir.com/BFS-U3-28S5/latest/Model/spec.html (accessed on 6 July 2022).
- Abay, T.Y.; Kyriacou, P.A. Photoplethysmography in oxygenation and blood volume measurements. In Photoplethysmography; Academic Press: Cambridge, MA, USA, 2022; pp. 147–188. [Google Scholar] [CrossRef]
- Angelopoulou, E. The Reflectance Spectrum of Human Skin. Technical Reports (CIS). MS-CIS-99-29. December 1999. Available online: https://repository.upenn.edu/cis_reports/584 (accessed on 6 July 2022).
- Cooksey, C.C.; Allen, D.W.; Tsai, B.K. Reflectance data set and variability study for human skin reflectance. In Proceedings of the 29th Session of the CIE, Washington DC, USA, 14–22 June 2019. [Google Scholar] [CrossRef]
- Chatterjee, S.; Budidha, K.; Kyriacou, P.A. Investigating the origin of photoplethysmography using a multiwavelength Monte Carlo model. Physiol. Meas. 2020, 41, 84001. [Google Scholar] [CrossRef]
- Kyriacou, P.A.; Allen, J. Photoplethysmography: Technology, Signal Analysis and Applications; Academic Press: Cambridge, MA, USA, 2021. [Google Scholar] [CrossRef]
- Halbritter, H.; Jäger, C.; Weber, R.; Schwind, M.; Möllmer, F. High-speed LED driver for ns-pulse switching of high-current LEDs. IEEE Photonics Technol. Lett. 2014, 26, 1871–1873. [Google Scholar] [CrossRef]
- Wang, Y.; Alonso, J.M.; Ruan, X. A review of LED drivers and related technologies. IEEE Trans. Ind. Electron. 2017, 64, 5754–5765. [Google Scholar] [CrossRef]
- Tian, G.; Qi, W.; Yan, Y.; Jiang, Y.Z. High power factor LED power supply based on SEPIC converter. Electron. Lett. 2014, 50, 1866–1868. [Google Scholar] [CrossRef]
- Yeon, J.-E.; Kim, D.-S.; Cho, K.; Kim, H.-J. A single stage flyback power supply unit for LED lighting applications. In Proceedings of the 2009 International Conference on Electrical and Electronics Engineering-ELECO, Bursa, Turkey, 5–8 November 2009; p. I-288. [Google Scholar] [CrossRef]
- Pollock, A.; Pollock, H.; Pollock, C. High efficiency LED power supply. IEEE J. Emerg. Sel. Top. Power Electron. 2015, 3, 617–623. [Google Scholar] [CrossRef]
- FLIR. FLIR Product Catalog List. Version 17-0713. 2017. Available online: https://www.flir.eu/ (accessed on 6 July 2022).
- Liu, H.; Wang, Y.; Wang, L.E.I. The effect of light conditions on photoplethysmographic image acquisition using a commercial camera. IEEE J. Transl. Eng. Health Med. 2014, 2, 1800811. [Google Scholar] [CrossRef] [PubMed]
- Cooksey, C.C.; Allen, D.W.; Tsai, B.K. Reference data set of human skin reflectance. J. Res. Natl. Inst. Stand. Technol. 2017, 122, 1. [Google Scholar] [CrossRef]






















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | Wavelength (nm) | IF (mA) | VF (V) | Radiance (mW/sr) | Half Angle (°) |
|---|---|---|---|---|---|
| OSG59A5111P *(1) | 525 (GREEN) | 50 | 3.1 | 260.8 | 8 |
| OS6YKA5201P *(2) | 625 (RED) | 75 | 2.3 | 543.9 | 8 |
| SFH4544 *(3) | 940 (IR) | 100 | 1.6 | 550 | 10 |
| Type of Power Supply Used | AMES100-24S277NZ 24V |
|---|---|
| Recommended AC input voltage | 85 V–305 V |
| DC output voltage | 24 V |
| Output current | 4.5 A |
| Wavelength (nm) | Quantum Efficiency (%) |
|---|---|
| 525 | 79% |
| 625 | 70% |
| 940 | 10% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Labuda, M.; Smondrk, M.; Babusiak, B.; Borik, S. System for Non-Contact and Multispectral Examination of Blood Supply to Cutaneous Tissue. Electronics 2022, 11, 2958. https://doi.org/10.3390/electronics11182958
Labuda M, Smondrk M, Babusiak B, Borik S. System for Non-Contact and Multispectral Examination of Blood Supply to Cutaneous Tissue. Electronics. 2022; 11(18):2958. https://doi.org/10.3390/electronics11182958
Chicago/Turabian StyleLabuda, Michal, Maros Smondrk, Branko Babusiak, and Stefan Borik. 2022. "System for Non-Contact and Multispectral Examination of Blood Supply to Cutaneous Tissue" Electronics 11, no. 18: 2958. https://doi.org/10.3390/electronics11182958