
Medical Data Storage Model Based on an Alliance Chain

Abstract
:1. Introduction
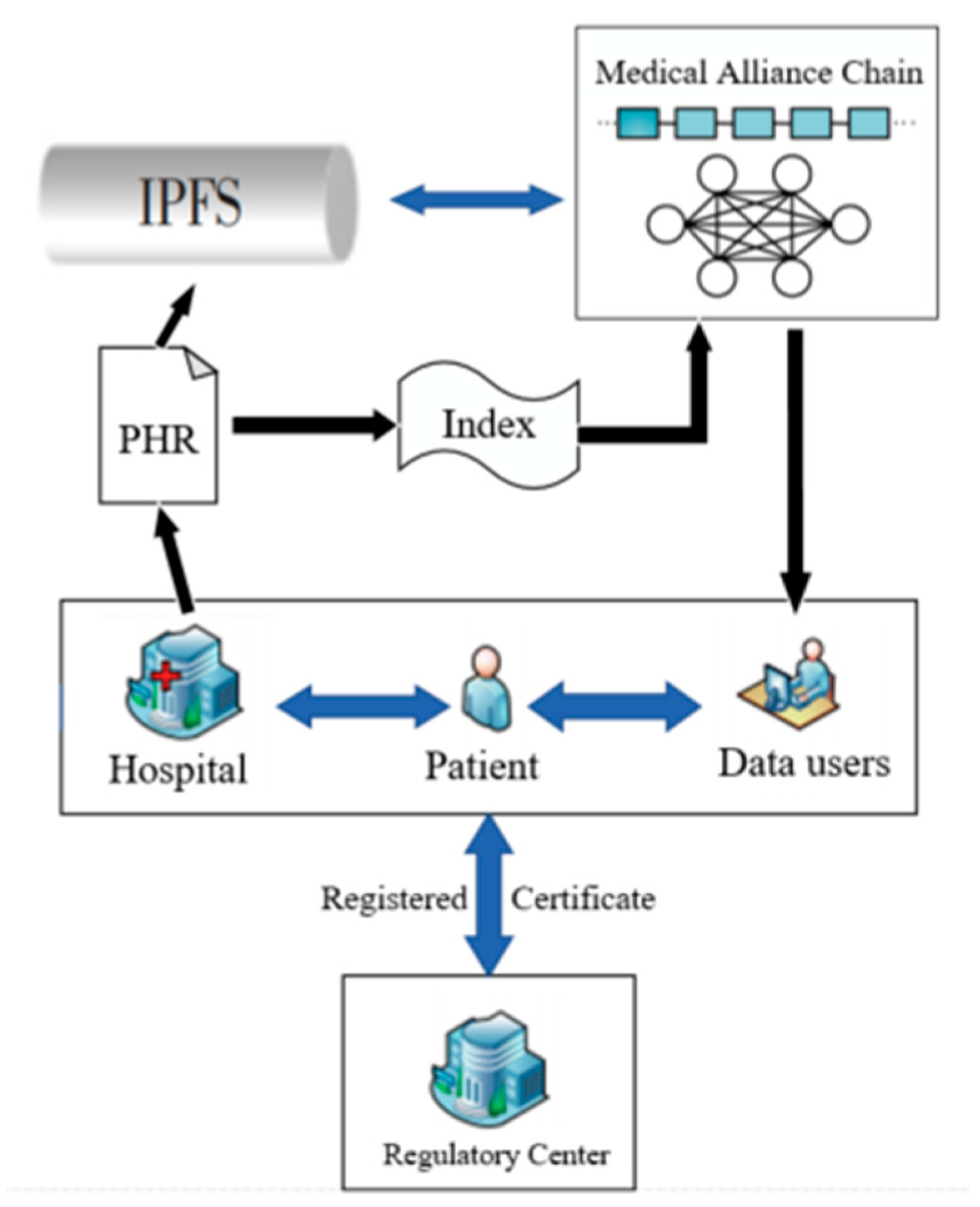
2. Medical Data Storage Model
2.1. Distance Algorithm
| Algorithm 1 Distance algorithm |
| Input: Initial node collection Threshold radius Number of groups Output: Initial groups 1: . ← {} 2: for (, ) 3: c ← () 4: . 5: 6: for 7: if 8: . 9: ←- 10: ←- 11: 12: 13: ← 14: . 15: |
2.2. Consensus Algorithm of the Medical Data Storage Model
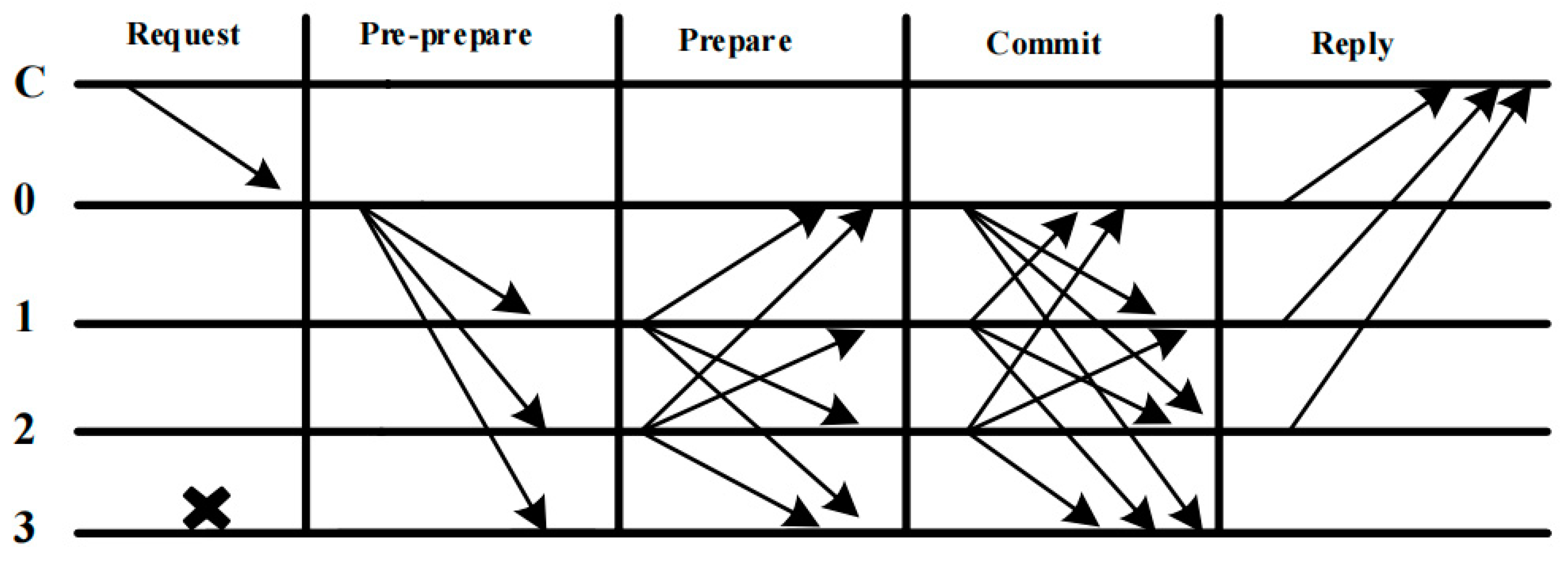
2.2.1. PBFT Consensus Algorithm
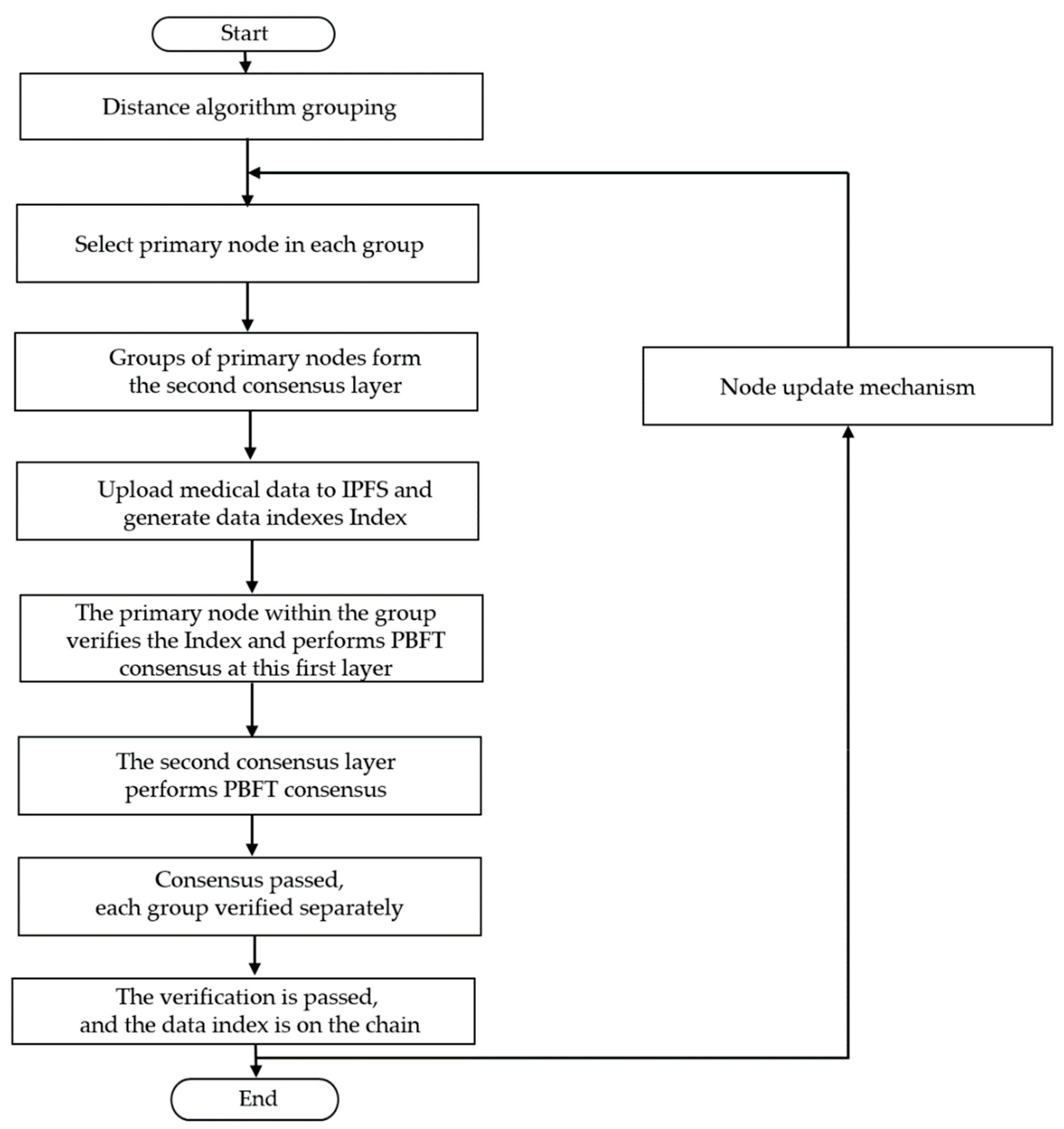
2.2.2. Consensus Mechanism for Medical Data Storage
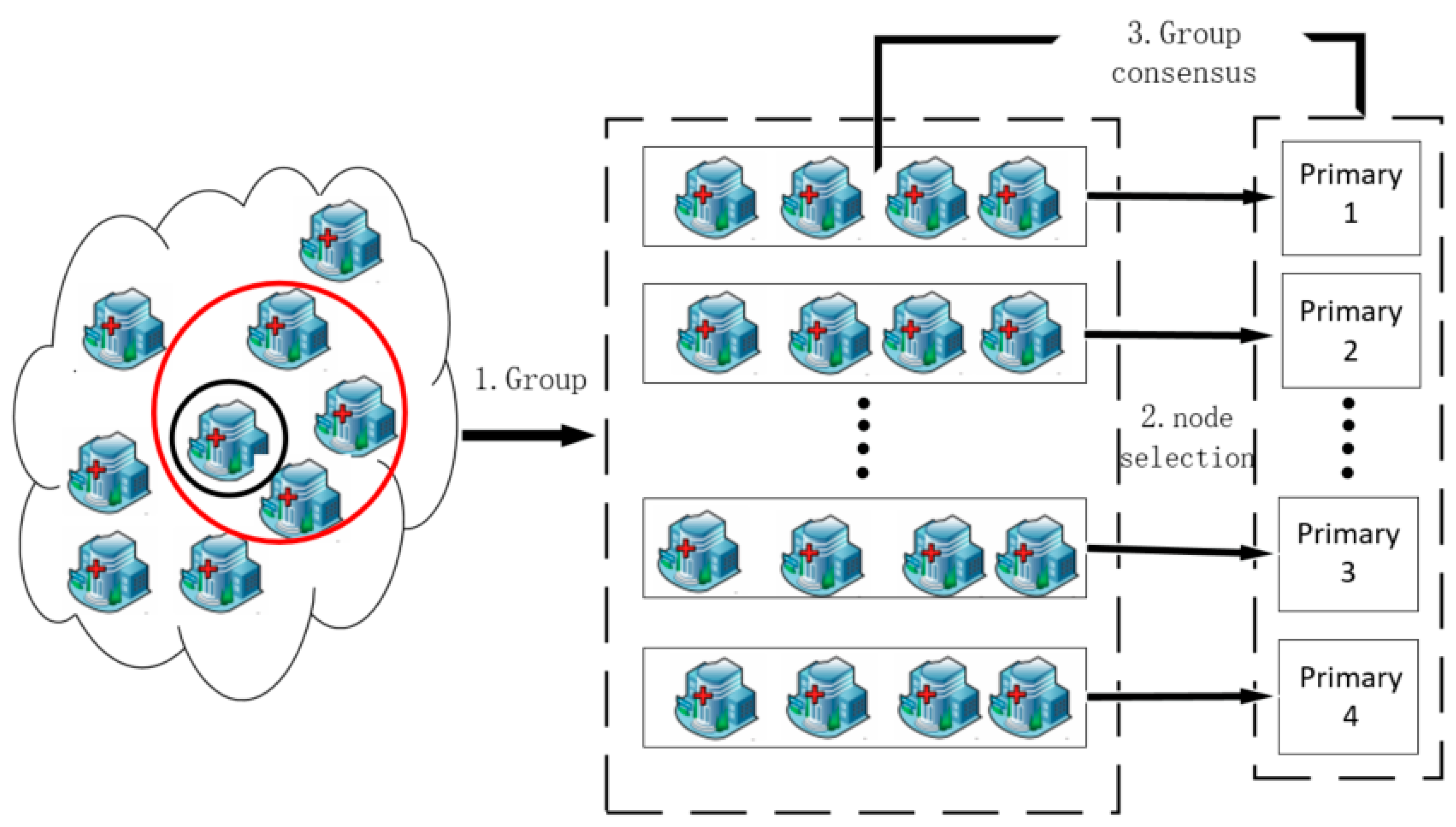
- Grouping: First, all medical nodes of the system are divided into M groups according to their distances within a fixed period T by the Distance algorithm. The specific cycle duration can be set appropriately according to the reality. The reason for regrouping medical nodes at intervals is to consider that the medical nodes of this model may change, which may affect the consensus efficiency. The generated master node ranking is fixed within a certain period and will only change due to master node replacement and the dynamic applications of medical nodes to join and exit.
- Election: In groups, in order to further improve communication efficiency and reduce the probability of malicious nodes becoming primary nodes, the selection of primary nodes adopts a distance ranking hybrid algorithm. The primary node election method adopted for the medical imaging blockchain platform is:Among them, is the final ranking result of the primary node, is the average distance, is the standard deviation of the distance, and is the comprehensive ranking of the hospital. and are different correction parameters set according to the change in the ranking value of medical institutions. 0 ≤ α, β ≤ 1. According to Formula (2), we calculate for each node in the group to other nodes, and when the same occurs, we calculate for each node in the group to other nodes according to Formula (3). The purpose of the distance ranking hybrid mechanism is to select a number of primary nodes that are closer to each other in each group, thus reducing the transmission delay of preparatory information in the consensus phase.
- Consensus: Assuming that there are Byzantine nodes in the node, when conducting sub-consensus groups, poll within the group. If there is a request from a medical node to upload medical data, upload this request to the current primary node of the group first; the primary node will sort and verify the request, generate a pre-prepared message, and then send the sorted pre-prepared message to other medical nodes in the group for the first PBFT consensus. When the primary consensus group consensus is performed, the block will be confirmed by the second PBFT consensus in the primary consensus group after passing the consensus verification process of the sub-consensus group. When the first PBFT consensus is successful, the master node T1 of the group will broadcast the generated pre-prepared message to the master nodes of other groups for the second PBFT consensus. During the consensus process, each master node broadcasts its own digital signature and collects the digital signatures of other master nodes, and when the consensus is passed, each master node will package all the collected signatures and requests and send them to the other hospital nodes in the group, respectively. After receiving the packaged message, the hospital node verifies the digital signature collection, executes the request content after the verification is passed, and updates the medical data to the local blockchain ledger so that the consensus is completed. Below is the pseudo-code of this Algorithm 2.
| Algorithm 2 Consensus |
| Input: Initial node collection Initial groups Request node client Collection of primary nodes Output: Consensus results res 1: (, . ) 2: ← 3: ← () 4: 5: ← (.)() 6: 7: ← () 8: 9: ( , ., ) 10: . 11: 12: |
- 4.
- Update: Most of the data of the medical imaging platform are stored in the server. If the master node hospital fails or goes down, the master node will be replaced to ensure the normal and efficient operation of the medical imaging platform. The node replacement mechanism is as follows: according to the result of the above election, the master node will be polled down in the master node ranking set according to the ranking result . If the rotating master node is also down, the rotation will continue down. The rotated master node will be removed from the consensus. In order to ensure fairness, if the master node is replaced within a fixed period , the set of the election will be recalculated so that all other nodes have the opportunity to become the master node to prevent a monopoly caused by a single node. When a new medical node wants to join, by calculating the average distance from the medical node to each node group, the smallest distance average node group is selected, and the new medical node is added to the small node group when there is no medical node data index up-link request in the node group. When a medical node wants to quit, the medical node that wants to quit sends a quit command to the primary node of the node group that the medical node wants to quit, and after verification, the medical node is deleted from the node group when the node group is free. At the same time, we can regroup after a fixed period . The specific period can be set according to the new hospitals and the actual demand to ensure the most efficient transmission efficiency and reduce the consensus delay and communication times.
3. Analysis and Evaluation
3.1. Security Analysis
3.1.1. Comparative Analysis
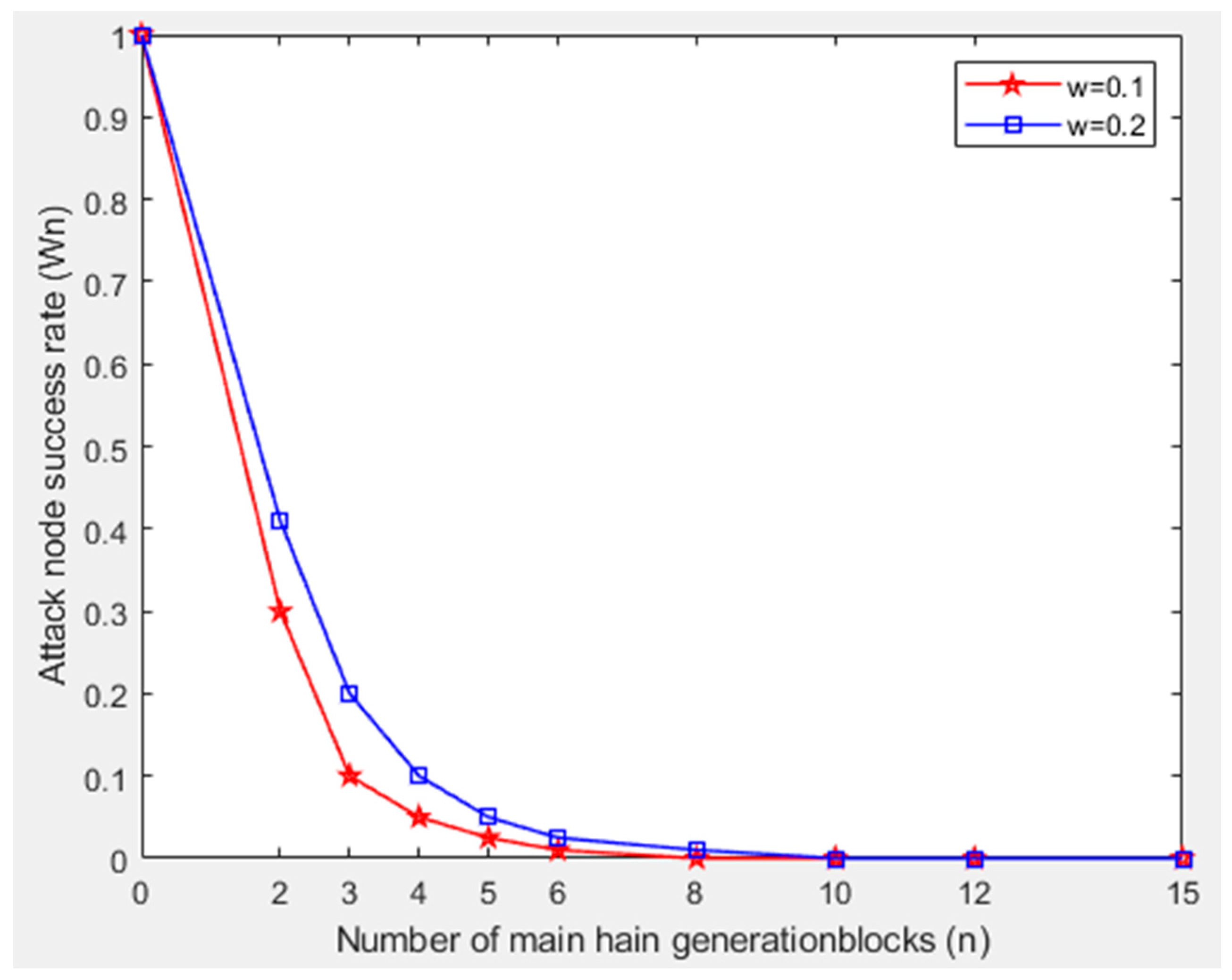
3.1.2. Security Analysis of Attack Blocks
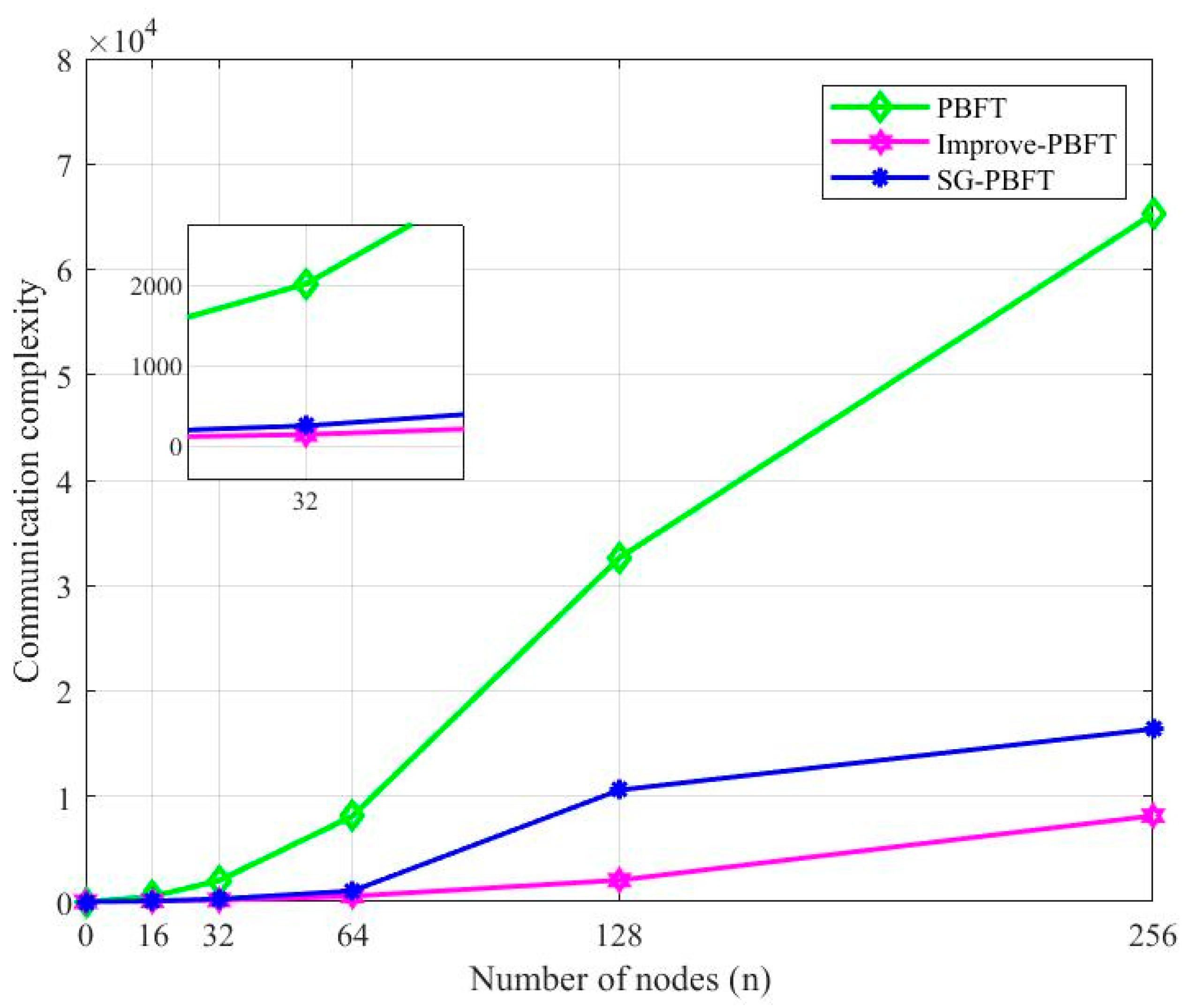
3.2. Analysis of Communication Complexity
4. Conclusions and Outlook
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Souiki, S.; Hadjila, M.; Moussaoui, D.; Ferdi, S.; Rais, S. M-Health Application for Managing a Patient’s Medical Record based on the Cloud: Design and Implementation. In Proceedings of the 2020 2nd International Workshop on Human-Centric Smart Environments for Health and Well-being (IHSH), Boumerdes, Algeria, 9–10 February 2021. [Google Scholar]
- Naumov, V.; Szarata, A.; Vasiutina, H. Simulating a Macrosystem of Cargo Deliveries by Road Transport Based on Big Data Volumes: A Case Study of Poland. Energies 2022, 15, 5111. [Google Scholar] [CrossRef]
- Thakur, N.; Han, C.Y. Indoor Localization for Personalized Ambient Assisted Living of Multiple Users in Multi-Floor Smart Environments. Big Data Cogn. Comput. 2021, 5, 42. [Google Scholar] [CrossRef]
- Hao, W.; Yujiao, S. Secure Cloud-Based EHR System Using Attribute-Based Cryptosystem and Blockchain. J. Med. Syst. 2018, 42, 152. [Google Scholar]
- Chen, W.; Zheng, Z. Blockchain Data Analysis: A Review of Status, Trends and Challenges. J. Comput. Res. Dev. 2018, 55, 1853–1870. [Google Scholar]
- Esposito, C.; Santis, A.D.; Tortora, G.; Chang, H.; Choo, K.-K.R. Blockchain: A Panacea for Healthcare Cloud-Based Data Security and Privacy? IEEE Cloud Comput. 2018, 5, 31–37. [Google Scholar] [CrossRef]
- Wang, H.; Liu, Y.; Cao, S.; Zhou, M. A medical data storage mechanism incorporating blockchain technology. Comput. Sci. 2020, 47, 285–291. [Google Scholar]
- Feng, T.; Jiao, Y.; Fang, J.; Tian, Y. Medical and Health Data Security Model Based on Consortium Blockchain. Comput. Sci. 2020, 47, 7. [Google Scholar]
- Azaria, A.; Ekblaw, A.; Vieira, T.; Lippman, A. MedRec: Using Blockchain for Medical Data Access and Permission Management. In Proceedings of the 2016 2nd International Conference on Open & Big Data, Vienna, Austria, 22–24 August 2016. [Google Scholar]
- Proof of Burn [EB/OL.]. Available online: https://en.bitcoin.it/wiki/Proofofburn (accessed on 10 April 2018).
- Zhang, L.; Li, Q. Research on Consensus Efficiency Based on Practical Byzantine Fault Tolerance. In Proceedings of the 2018 10th International Conference on Modelling, Identification and Control (ICMIC), Guiyang, China, 2–4 July 2018. [Google Scholar]
- Perez, A.O.; Domingo-Palaoag, T. Blockchain-based Model for Health Information Exchange: A Case for Simulated Patient Referrals Using an Electronic Medical Record. In IOP Conference Series: Materials Science and Engineering, Proceedings of the 5th International Conference on Information Technology and Digital Applications (ICITDA 2020), Yogyakarta, Indonesia, 13–14 November 2020; IOP Publishing: Yogyakarta, Indonesia, 2021; Volume 1077, p. 012059. [Google Scholar]
- Cheng, L.; Qi, Z.; Shi, J. EHR data security storage and sharing scheme based on blockchain. J. Nanjing Univ. Posts Telecommun. Nat. Sci. Ed. 2020, 40, 7. [Google Scholar]
- Feng, X.; Shi, Q.; Xie, Q.; Liu, L. An Efficient Privacy-preserving Authentication Model based on blockchain for VANETs. J. Syst. Archit. 2021, 117, 102158. [Google Scholar] [CrossRef]
- Xue, T.F.; Fu, Q.C.; Wang, C.; Wang, X.Y. A Medical Data Sharing Model via Blockchain. Zidonghua Xuebao/Acta Autom. Sin. 2017, 43, 1555–1562. [Google Scholar]
- MJalalzai, M.; Busch, C.; Richard, G.G. Consistent BFT Performance for Blockchains. In Proceedings of the 2019 49th Annual IEEE/IFIP International Conference on Dependable Systems and Networks—Supplemental Volume (DSN-S), Portland, OR, USA, 24–27 June 2019; pp. 17–18. [Google Scholar] [CrossRef]
- Li, M.; Wang, C.; Yan, L.; Wei, S. Research on the Application of Medical Big Data. In Proceedings of the 2019 14th International Conference on Computer Science & Education (ICCSE), Toronto, ON, Canada, 19–21 August 2019; pp. 478–482. [Google Scholar] [CrossRef]
- Gan, B.; Wu, Q.; Li, X.; Zhou, Y. Classification of Blockchain Consensus Mechanisms Based on PBFT Algorithm. In Proceedings of the 2021 International Conference on Computer Engineering and Application (ICCEA), Kunming, China, 25–27 June 2021; pp. 26–29. [Google Scholar] [CrossRef]
- Chen, H.; Yu, J.; Liu, F.; Cai, Z.; Xia, J. Archipelago: A Medical Distributed Storage System for Interconnected Health. In IEEE Internet Computing; IEEE: New York, NY, USA, 2020; Volume 24, pp. 28–38. [Google Scholar] [CrossRef]
- Snow, P.; Deery, B.; Lu, J.; Johnston, D.; Kirby, P.; Sprague, A.Y.; Byington, D. Business Processes Secured by Immutable Audit Trails on the Blockchain. Available online: https://bravenewcoin.com/insights/business-processes-secured-by-immutable-audit-trails-on-the-blockchain (accessed on 17 November 2014).
- Atreyapurapu, S.B.; Amarendra, K.; Alishah, M.M. Hyperledger Fabric based Medical Record Security. In Proceedings of the 2022 4th International Conference on Smart Systems and Inventive Technology (ICSSIT), Tirunelveli, India, 20–22 January 2022; pp. 223–228. [Google Scholar] [CrossRef]
- Xu, G.; Bai, H.; Xing, J.; Luo, T.; Xiong, N.N.; Cheng, X.; Liu, S.; Zheng, X. SG-PBFT: A secure and highly efficient distributed blockchain PBFT consensus algorithm for intelligent Internet of vehicles. J. Parallel Distrib. Comput. 2022, 164, 1–11. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Programs | Blockchain-Based | Consensus Mechanism | Focus on Medical Issues | Affiliate Chain |
|---|---|---|---|---|
| Factom [20] | No | None | No | No |
| MedRec [9] | Yes | POW | Yes | No |
| AMDSM [8] | Yes | DPOS + PBFT | Yes | No |
| This article | Yes | Improvement of PBFT | Yes | Yes |
| Pre-Prepare | Prepare | Commit | Total | ||||
|---|---|---|---|---|---|---|---|
| PBFT | n − 1 | N ∗ (n − 1) | N ∗ (n − 1) | 2n2 − n − 1 | |||
| SG-PBFT | n/2 − 1 | (n/2 − 1) ∗ (n/2 − 1) | n/2 − 1 | (n/2 − 1) ∗ (n/2 + 1) | |||
| The First Time | The Second Time | Total | |||||
| This article | (1 + 2n/k) ∗ (n/k − 1) | (k − 1) ∗ (2k + 1) | (k − 1) ∗ (2k + 1) +(1 + 2n/k) ∗ (n/k − 1) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, K.; Feng, W.; Zhang, Y.; Zhong, W.; Zheng, X. Medical Data Storage Model Based on an Alliance Chain. Electronics 2022, 11, 2495. https://doi.org/10.3390/electronics11162495
Chang K, Feng W, Zhang Y, Zhong W, Zheng X. Medical Data Storage Model Based on an Alliance Chain. Electronics. 2022; 11(16):2495. https://doi.org/10.3390/electronics11162495
Chicago/Turabian StyleChang, Kejia, Wenlong Feng, Yu Zhang, Wang Zhong, and Xiandong Zheng. 2022. "Medical Data Storage Model Based on an Alliance Chain" Electronics 11, no. 16: 2495. https://doi.org/10.3390/electronics11162495