
Efficient Perineural Invasion Detection of Histopathological Images Using U-Net


Abstract
:1. Introduction
- ✓
- A deep learning-based method is proposed to efficiently detect PNI region with a relatively small amount of data with various types of cancers. The proposed method can learn a neural network model without detailed labels for the nerve and tumor cells. Labeling cells requires intensive and time-consuming labor from well-trained physicians. Instead, only the boundary lines between those cells are used to learn the models.
- ✓
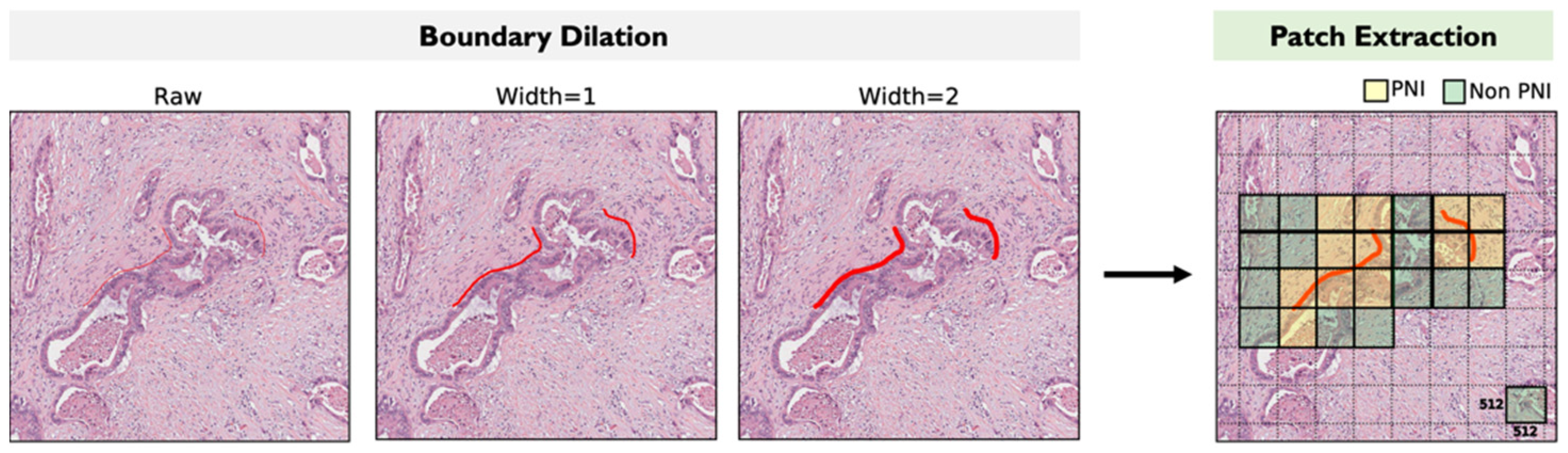
- A boundary dilation method and a loss combination technique are proposed to improve the detection performance of PNI. The expanded regions by the proposed dilation method help model the visual transitional patterns from the nerve to the tumor cells. A new loss function is also proposed to better learn the neural network model. Experimental results confirm that the proposed method effectively improves PNI detection performance from 0.188 to 0.275.
- ✓
- We validate that the proposed method can be utilized in many other medical problems that are involved with boundary detection tasks. According to the experimental results for nontumor and nerve cells boundary detection, the proposed method is effective for general boundary detection, and it showed improved detection performance from 0.551 to 0.693.
2. Related Work
3. Methods
3.1. Proposed Boundary Dilation Method
3.2. End-to-End PNI Detection and Segmentation with Combined Loss
4. Experimental Results
4.1. Dataset
4.2. Implementation Details
4.3. Evaluation Metric
4.4. Qualitative and Quantitative Results
4.5. Additional Experiments: Normal Nerve Detection
5. Discussion and Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Liebig, C.; Ayala, G.; Wilks, J.A.; Berger, D.H.; Albo, D. Perineural Invasion in Cancer: A Review of the Literature. Cancer 2009, 115, 3379–3391. [Google Scholar] [CrossRef] [PubMed]
- Brown, I.S. Pathology of Perineural Spread. J. Neurol. Surg. B Skull Base 2016, 77, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holthoff, E.R.; Jeffus, S.K.; Gehlot, A.; Stone, R.; Erickson, S.W.; Kelly, T.; Quick, C.M.; Post, S.R. Perineural Invasion Is an Independent Pathologic Indicator of Recurrence in Vulvar Squamous Cell Carcinoma. Am. J. Surg. Pathol. 2015, 39, 1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunn, M.; Morgan, M.B.; Beer, T.W. Perineural Invasion: Identification, Significance, and a Standardized Definition. Dermatol. Surg. 2009, 35, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Deng, S.; Yan, L.; Gu, J.; Li, J.; Wu, K.; Cai, K. Perineural Invasion Is Associated with Poor Prognosis of Colorectal Cancer: A Retrospective Cohort Study. Int. J. Colorectal Dis. 2020, 35, 1067–1075. [Google Scholar] [CrossRef] [PubMed]
- Schmitd, L.B.; Beesley, L.J.; Russo, N.; Bellile, E.L.; Inglehart, R.C.; Liu, M.; Romanowicz, G.; Wolf, G.T.; Taylor, J.M.G.; D’Silva, N.J. Redefining Perineural Invasion: Integration of Biology with Clinical Outcome. Neoplasia 2018, 20, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Fagan, J.J.; Collins, B.; Barnes, L.; D’Amico, F.; Myers, E.N.; Johnson, J.T. Perineural Invasion in Squamous Cell Carcinoma of the Head and Neck. Arch. Otolaryngol. Neck Surg. 1998, 124, 637–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, A.S.; Parameshwaran, V.; Beltran, L.; Fisher, G.; North, B.V.; Greenberg, D.; Soosay, G.; Møller, H.; Scardino, P.; Cuzick, J.; et al. Should Reporting of Peri-Neural Invasion and Extra Prostatic Extension Be Mandatory in Prostate Cancer Biopsies? Correlation with Outcome in Biopsy Cases Treated Conservatively. Oncotarget 2018, 9, 20555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deepthi, G.; Shyam, N.D.V.N.; Kumar, G.K.; Narayen, V.; Paremala, K.; Preethi, P. Characterization of Perineural Invasion in Different Histological Grades and Variants of Oral Squamous Cell Carcinoma. J. Oral Maxillofac. Pathol. JOMFP 2020, 24, 57. [Google Scholar] [PubMed]
- Fu, Y.; Zhang, X.; Ding, Z.; Zhu, N.; Song, Y.; Zhang, X.; Jing, Y.; Yu, Y.; Huang, X.; Zhang, L.; et al. Worst Pattern of Perineural Invasion Redefines the Spatial Localization of Nerves in Oral Squamous Cell Carcinoma. Front. Oncol. 2021, 11, 4973. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhu, H.; Wang, S.H.; Zhang, Y.D. A Review of Deep Learning on Medical Image Analysis. Mob. Netw. Appl. 2021, 26, 351–380. [Google Scholar] [CrossRef]
- Shen, D.; Wu, G.; Suk, H., II. Deep Learning in Medical Image Analysis. Annu. Rev. Biomed. Eng. 2017, 19, 221–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jha, A.; Yang, H.; Deng, R.; Kapp, M.E.; Fogo, A.B.; Huo, Y. Instance Segmentation for Whole Slide Imaging: End-to-End or Detect-Then-Segment. J. Med. Imaging 2020, 8, 014001. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Gkioxari, G.; Dollár, P.; Girshick, R. Mask R-CNN. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 42, 386–397. [Google Scholar] [CrossRef] [PubMed]
- Feng, R.; Liu, X.; Chen, J.; Chen, D.Z.; Gao, H.; Wu, J. A Deep Learning Approach for Colonoscopy Pathology WSI Analysis: Accurate Segmentation and Classification. IEEE J. Biomed. Health Inform. 2021, 25, 3700–3708. [Google Scholar] [CrossRef] [PubMed]
- Nirschl, J.J.; Janowczyk, A.; Peyster, E.G.; Frank, R.; Margulies, K.B.; Feldman, M.D.; Madabhushi, A. A Deep-Learning Classifier Identifies Patients with Clinical Heart Failure Using Whole-Slide Images of H&E Tissue. PLoS ONE 2018, 13, e0192726. [Google Scholar]
- Ahmed, S.; Shaikh, A.; Alshahrani, H.; Alghamdi, A.; Alrizq, M.; Baber, J.; Bakhtyar, M. Transfer Learning Approach for Classification of Histopathology Whole Slide Images. Sensors 2021, 21, 5361. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Chen, H.; Gan, C.; Lin, H.; Dou, Q.; Tsougenis, E.; Huang, Q.; Cai, M.; Heng, P.A. Weakly Supervised Deep Learning for Whole Slide Lung Cancer Image Analysis. IEEE Trans. Cybern. 2020, 50, 3950–3962. [Google Scholar] [CrossRef] [PubMed]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Singapore, 18–22 September 2022; Springer: Cham, Switzerland, 2015; Volume 9351, pp. 234–241. [Google Scholar]
- PAIP 2021 Challenge. Available online: https://paip2021.grand-challenge.org/ (accessed on 9 April 2021).
- Nateghi, R.; Pourakpour, F. Perineural Invasion Detection in Multiple Organ Cancer Based on Deep Convolutional Neural Network. arXiv 2021, arXiv:2110.12283. [Google Scholar]
- Han, C.H.; Kwak, J.T. A Hybrid Computational Pathology Method for the Detection of Perineural Invasion Junctions. In Medical Imaging 2022: Digital and Computational Pathology; SPIE: Bellingham, WA, USA, 2022; Volume 12039, pp. 215–219. Available online: http://lps3.doi.org.libproxy.dgist.ac.kr/10.1117/12.2610756 (accessed on 4 April 2022).
- Tan, M.; Le, Q.V. EfficientNet: Rethinking Model Scaling for Convolutional Neural Networks. In Proceedings of the 36th International Conference on Machine Learning, ICML 2019, Long Beach, CA, USA, 9–15 June 2019; International Machine Learning Society (IMLS): Long Beach, CA, USA, 2019; Volume 2019, pp. 10691–10700. [Google Scholar]
- Deng, J.; Dong, W.; Socher, R.; Li, L.-J.; Li, K.; Li, F.-F. ImageNet: A Large-Scale Hierarchical Image Database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; IEEE: New York, NY, USA, 2010; pp. 248–255. [Google Scholar]
- Paszke, A.; Gross, S.; Massa, F.; Lerer, A.; Bradbury, G.J.; Chanan, G.; Killeen, T.; Lin, Z.; Gimelshein, N.; Antiga, L.; et al. PyTorch: An Imperative Style, High-Performance Deep Learning Library. In Advances in Neural Information Processing Systems 32 (NeurIPS 2019); Curran Associates Inc.: Red Hook, NY, USA, 2019; pp. 8024–8035. [Google Scholar]
- Lakubovskii, P. Segmentation Models with Pretrained Backbones: Keras and TensorFlow Keras. Available online: https://github.com/qubvel/segmentation_models (accessed on 13 April 2022).
- Ström, P.; Kartasalo, K.; Ruusuvuori, P.; Grönberg, H.; Samaratunga, H.; Delahunt, B.; Tsuzuki, T.; Egevad, L.; Eklund, M. Detection of Perineural Invasion in Prostate Needle Biopsies with Deep Neural Networks. arXiv 2020, arXiv:2004.01589. [Google Scholar]
- Lee, S.; Park, Y.; Park, J.; Jang, G.-J.; Kim, H. Multi-target Learning on asymmetric U-Net for PNI boundary detection. In Proceedings of the 9th International Conference on Big Data Applications and Services (BIGDAS), Jeju Island, Korea, 20–23 October 2021; Volume 9, pp. 127–131. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PNI Detection | F1-Score | ||
|---|---|---|---|
| Segmentation Loss Only | Combined Loss (Width = 1) | Combined Loss (Width = 2) | |
| Segmentation loss (width = 1) | 0.1877 | 0.2509 | 0.2566 |
| Segmentation loss (width = 2) | 0.1878 | 0.2489 | 0.2747 |
| PNI Detection | F1-Score | ||
|---|---|---|---|
| Segmentation Loss Only | Combined Loss (Width = 1) | Combined Loss (Width = 2) | |
| Segmentation loss (width = 1) | 0.5511 | 0.5299 | 0.5752 |
| Segmentation loss (width = 2) | 0.6571 | 0.5602 | 0.6930 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, Y.; Park, J.; Jang, G.-J. Efficient Perineural Invasion Detection of Histopathological Images Using U-Net. Electronics 2022, 11, 1649. https://doi.org/10.3390/electronics11101649
Park Y, Park J, Jang G-J. Efficient Perineural Invasion Detection of Histopathological Images Using U-Net. Electronics. 2022; 11(10):1649. https://doi.org/10.3390/electronics11101649
Chicago/Turabian StylePark, Youngjae, Jinhee Park, and Gil-Jin Jang. 2022. "Efficient Perineural Invasion Detection of Histopathological Images Using U-Net" Electronics 11, no. 10: 1649. https://doi.org/10.3390/electronics11101649