Author Contributions
Conceptualization, I.W. and A.K.M.; methodology, I.W.; software, I.W.; validation, A.K.M. and G.S.; formal analysis, I.W.; investigation, I.W.; writing—original draft preparation, I.W.; writing—review and editing, A.K.M., M.J. and P.C.; supervision, A.K.M., G.S., P.C., M.J., Z.L. and E.J.; Funding acquisition, Z.L. and E.J.; project administration, A.K.M. and G.S. All authors have read and agreed to the published version of the manuscript.
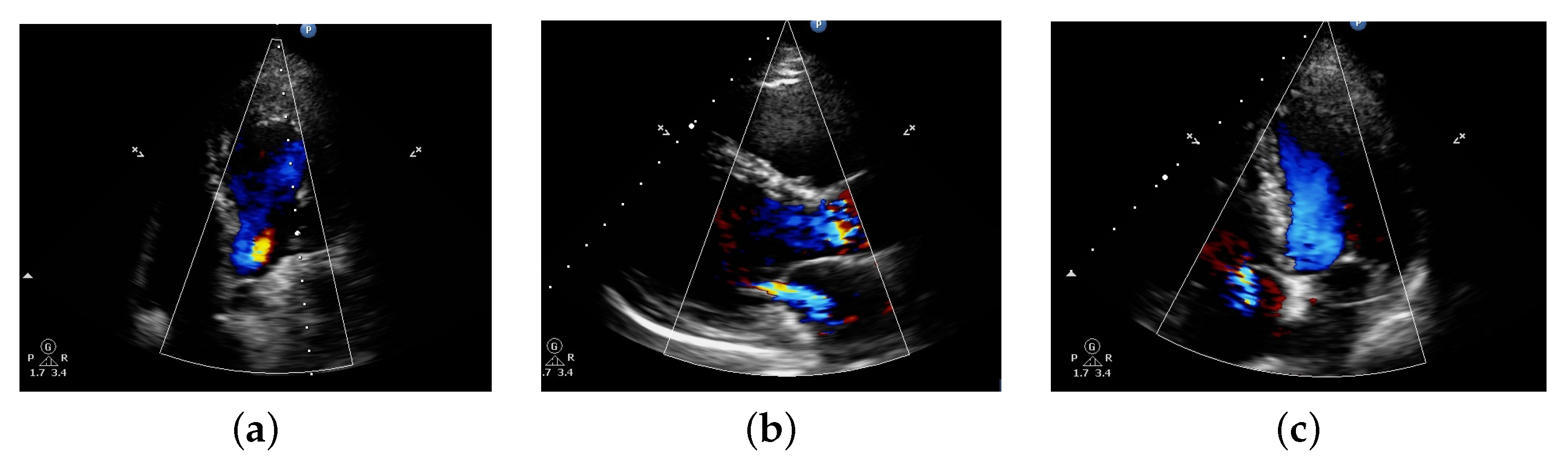
Figure 1.
Diagram showing Doppler echo from dataset collected of patient having (a) Aortic Regurgitation (AR), (b) Mitral Regurgitation (MR), and (c) Tricuspid Regurgitation (TR) abnormalities respectively.
Figure 1.
Diagram showing Doppler echo from dataset collected of patient having (a) Aortic Regurgitation (AR), (b) Mitral Regurgitation (MR), and (c) Tricuspid Regurgitation (TR) abnormalities respectively.
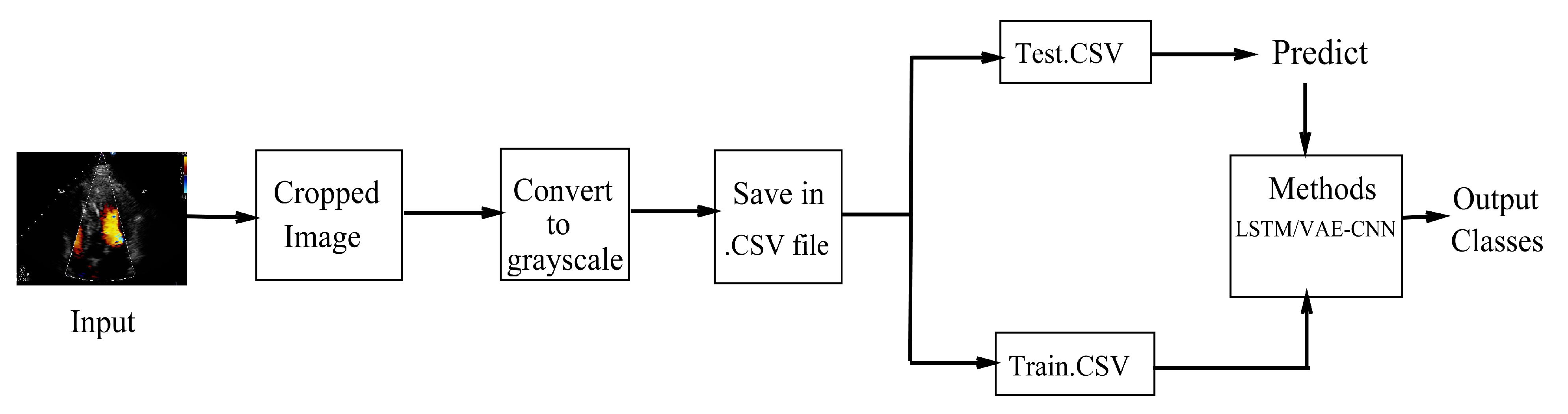
Figure 2.
An overall flow chart showing the working methodologies used in our scheme.
Figure 2.
An overall flow chart showing the working methodologies used in our scheme.
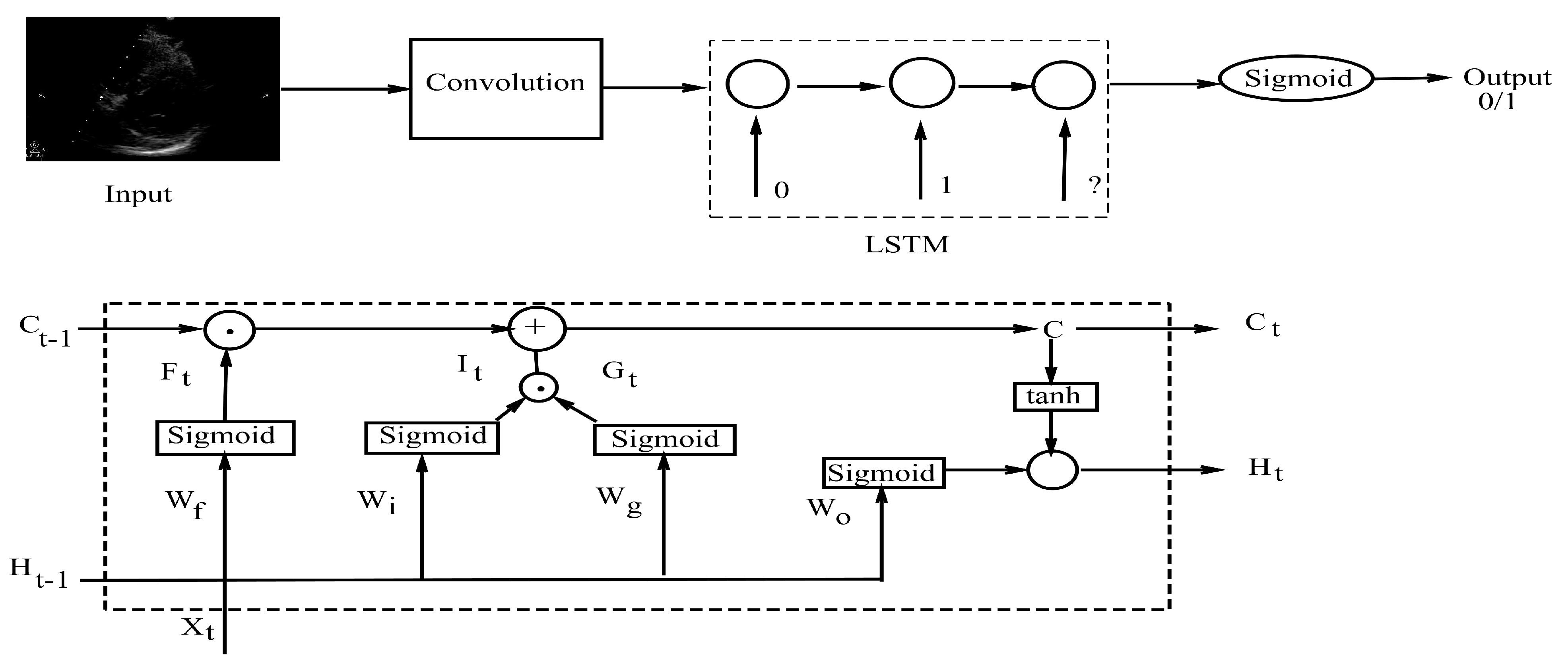
Figure 3.
Long Short Term Memory (LSTM) diagram with an overall flowchart of how the model works where an input image is passed to a convolution layer, then it is forwarded to the architecture whereby images are classified based on the previous and present classification.
Figure 3.
Long Short Term Memory (LSTM) diagram with an overall flowchart of how the model works where an input image is passed to a convolution layer, then it is forwarded to the architecture whereby images are classified based on the previous and present classification.
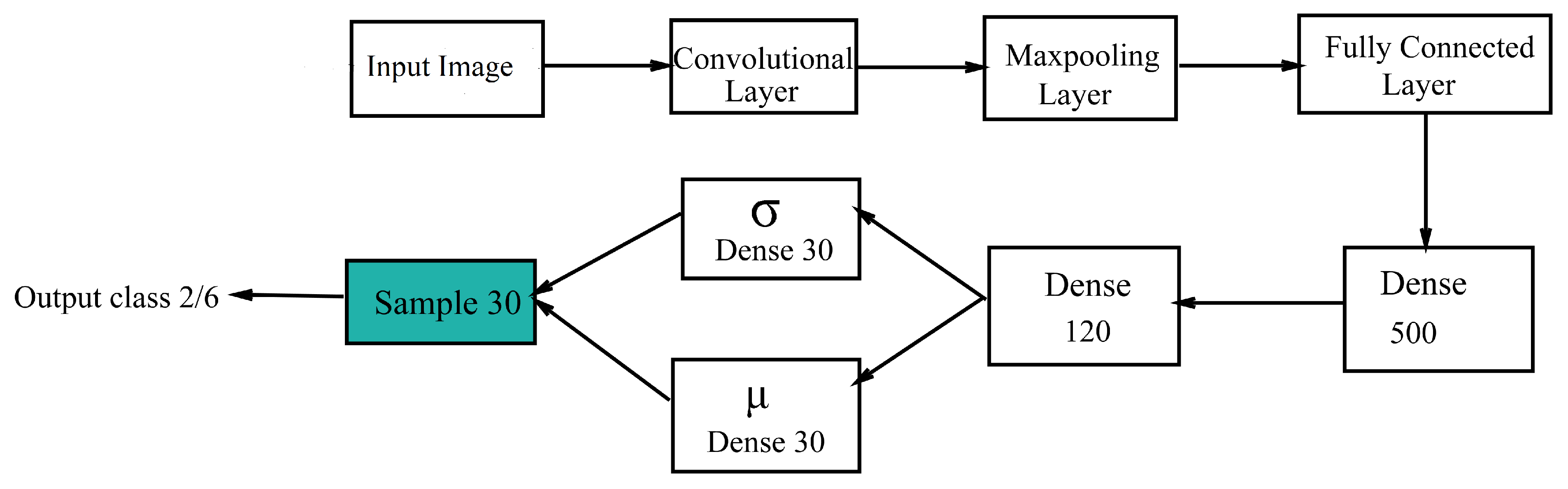
Figure 4.
Variational Autoencoder + Convolutional Neural Network (VAE-CNN) flowchart.
Figure 4.
Variational Autoencoder + Convolutional Neural Network (VAE-CNN) flowchart.
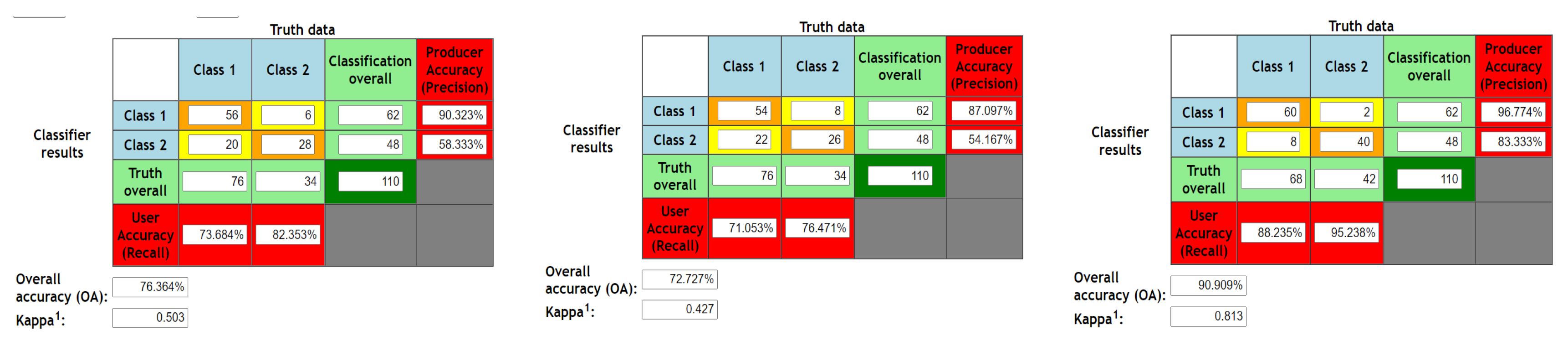
Figure 5.
Confusion matrix for validation phase of 2D images for SVM, LSTM and VAE3CNN respectively.
Figure 5.
Confusion matrix for validation phase of 2D images for SVM, LSTM and VAE3CNN respectively.
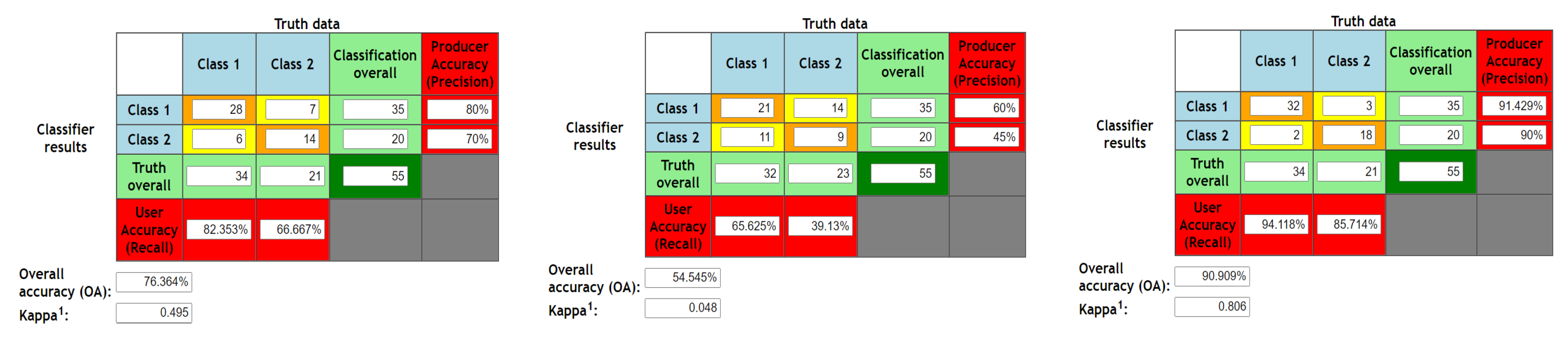
Figure 6.
Confusion matrix for testing phase of 2D images for SVM, LSTM and VAE-CNN respectively.
Figure 6.
Confusion matrix for testing phase of 2D images for SVM, LSTM and VAE-CNN respectively.
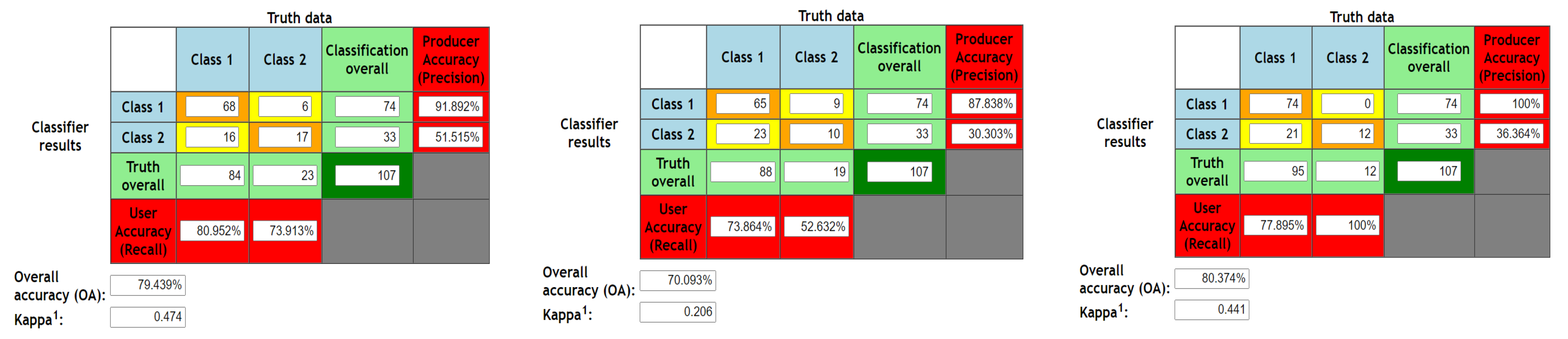
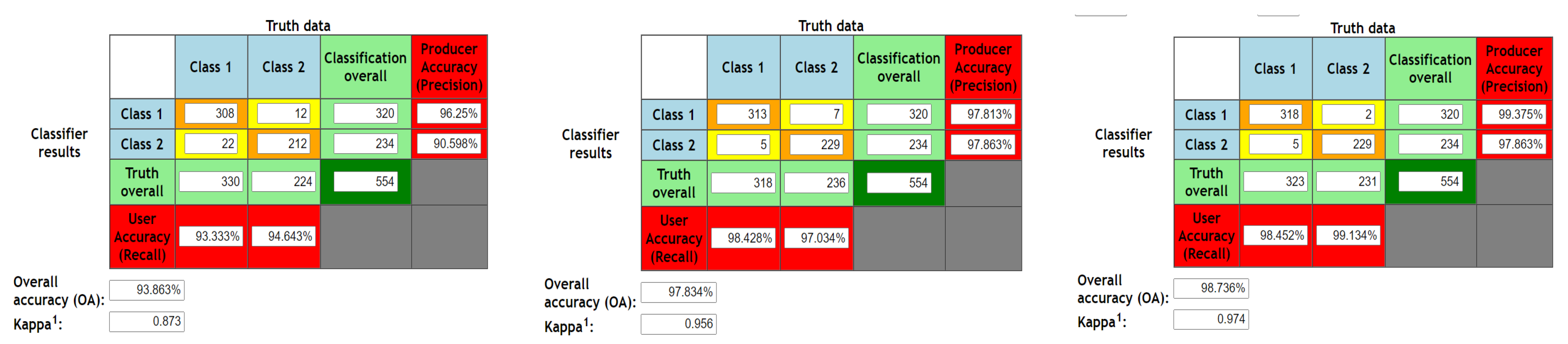
Figure 7.
Confusion matrix for Validation phase of 3D Doppler images for SVM, LSTM and VAE-CNN respectively.
Figure 7.
Confusion matrix for Validation phase of 3D Doppler images for SVM, LSTM and VAE-CNN respectively.
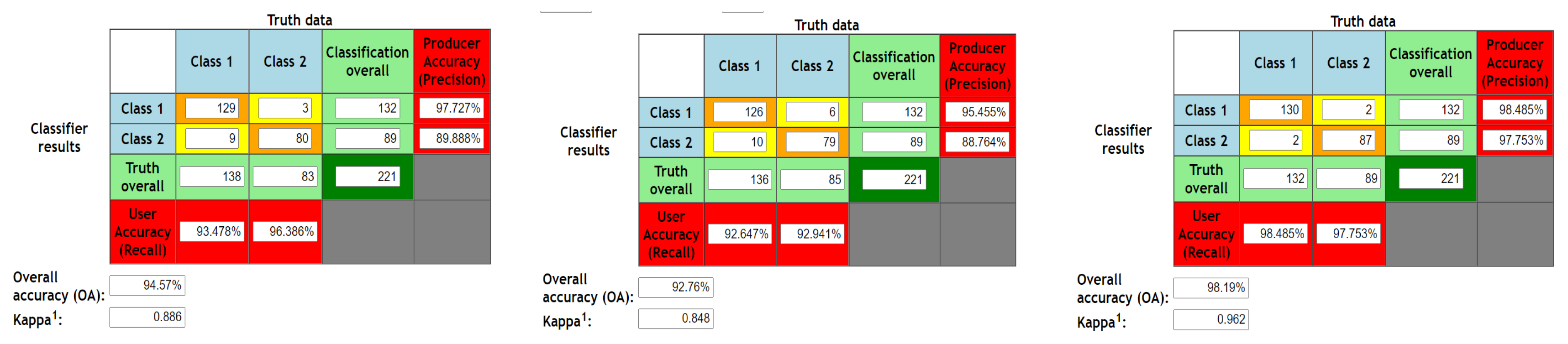
Figure 8.
Confusion matrix for testing phase of 3D Doppler images for SVM, LSTM and VAE-CNN respectively.
Figure 8.
Confusion matrix for testing phase of 3D Doppler images for SVM, LSTM and VAE-CNN respectively.
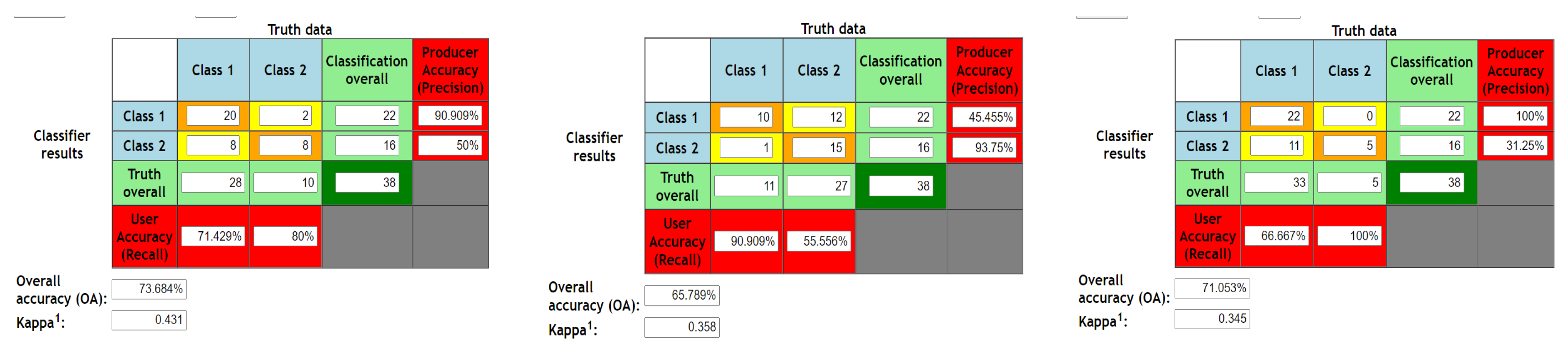
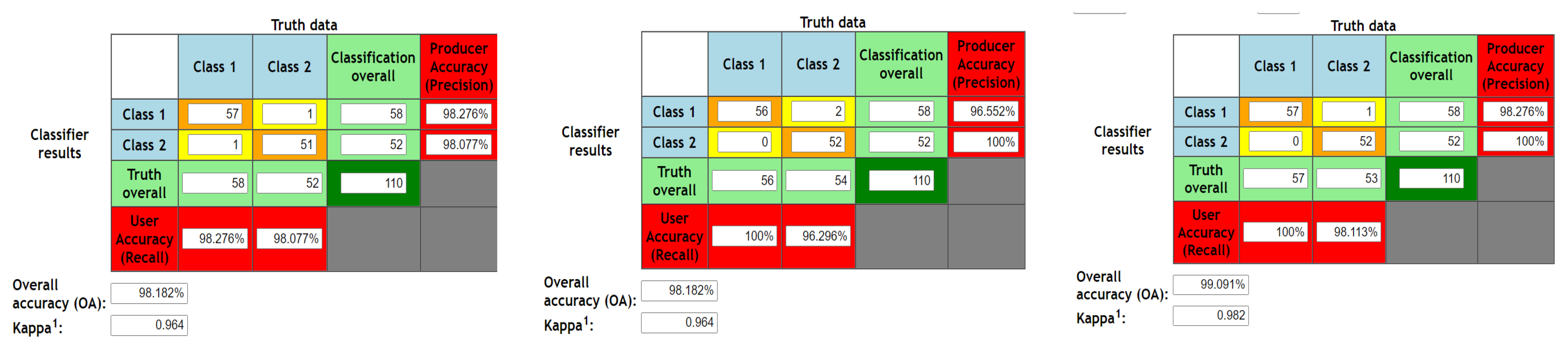
Figure 9.
Confusion matrix for 2 fold cross validation of 2D images for SVM, LSTM and VAE-CNN respectively.
Figure 9.
Confusion matrix for 2 fold cross validation of 2D images for SVM, LSTM and VAE-CNN respectively.
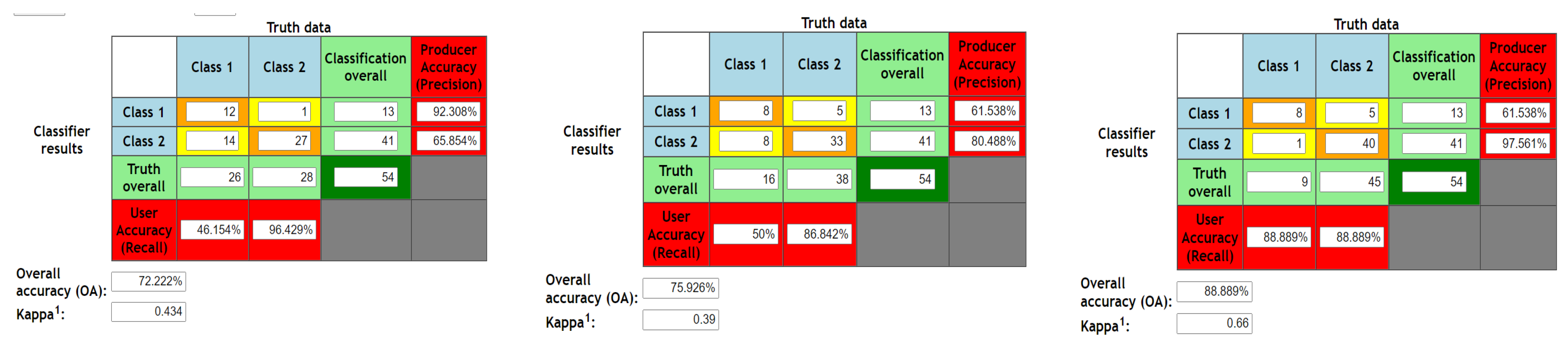
Figure 10.
Confusion matrix for 5 fold cross validation of 2D images for SVM, LSTM and VAE-CNN respectively.
Figure 10.
Confusion matrix for 5 fold cross validation of 2D images for SVM, LSTM and VAE-CNN respectively.
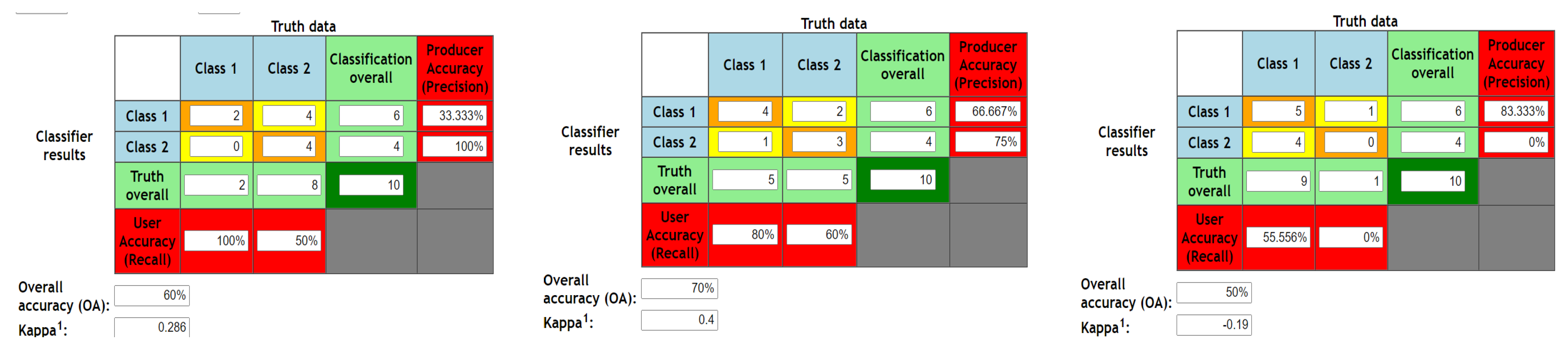
Figure 11.
Confusion matrix for 10 fold cross validation of 2D images for SVM, LSTM and VAE-CNN respectively.
Figure 11.
Confusion matrix for 10 fold cross validation of 2D images for SVM, LSTM and VAE-CNN respectively.
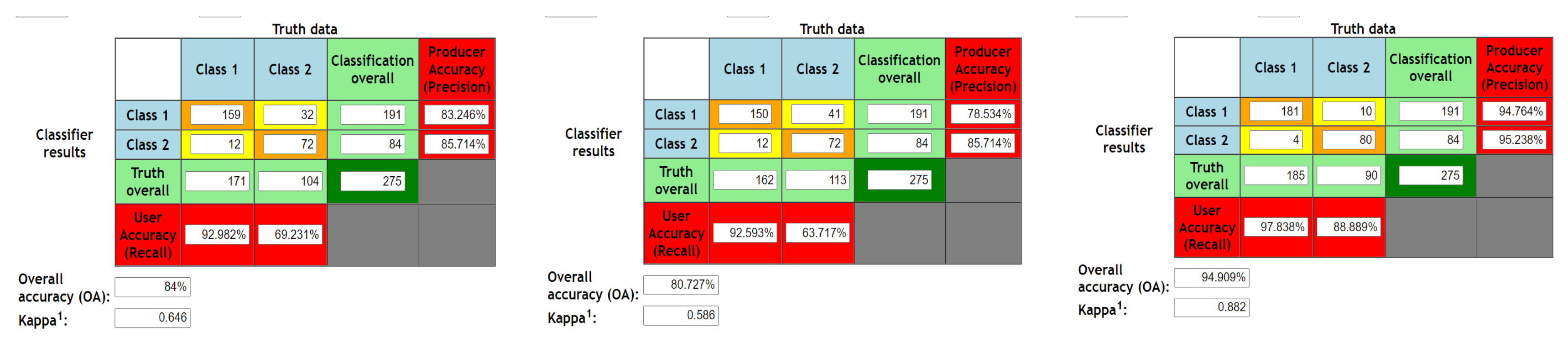
Figure 12.
Confusion matrix for 2 fold cross validation of 3D Doppler images for SVM, LSTM and VAE-CNN respectively.
Figure 12.
Confusion matrix for 2 fold cross validation of 3D Doppler images for SVM, LSTM and VAE-CNN respectively.
Figure 13.
Confusion matrix for 5 fold cross validation of 3D Doppler images for SVM, LSTM and VAE-CNN respectively.
Figure 13.
Confusion matrix for 5 fold cross validation of 3D Doppler images for SVM, LSTM and VAE-CNN respectively.
Figure 14.
Confusion matrix for 10 fold cross validation of 3D Doppler images for SVM, LSTM and VAE-CNN respectively.
Figure 14.
Confusion matrix for 10 fold cross validation of 3D Doppler images for SVM, LSTM and VAE-CNN respectively.
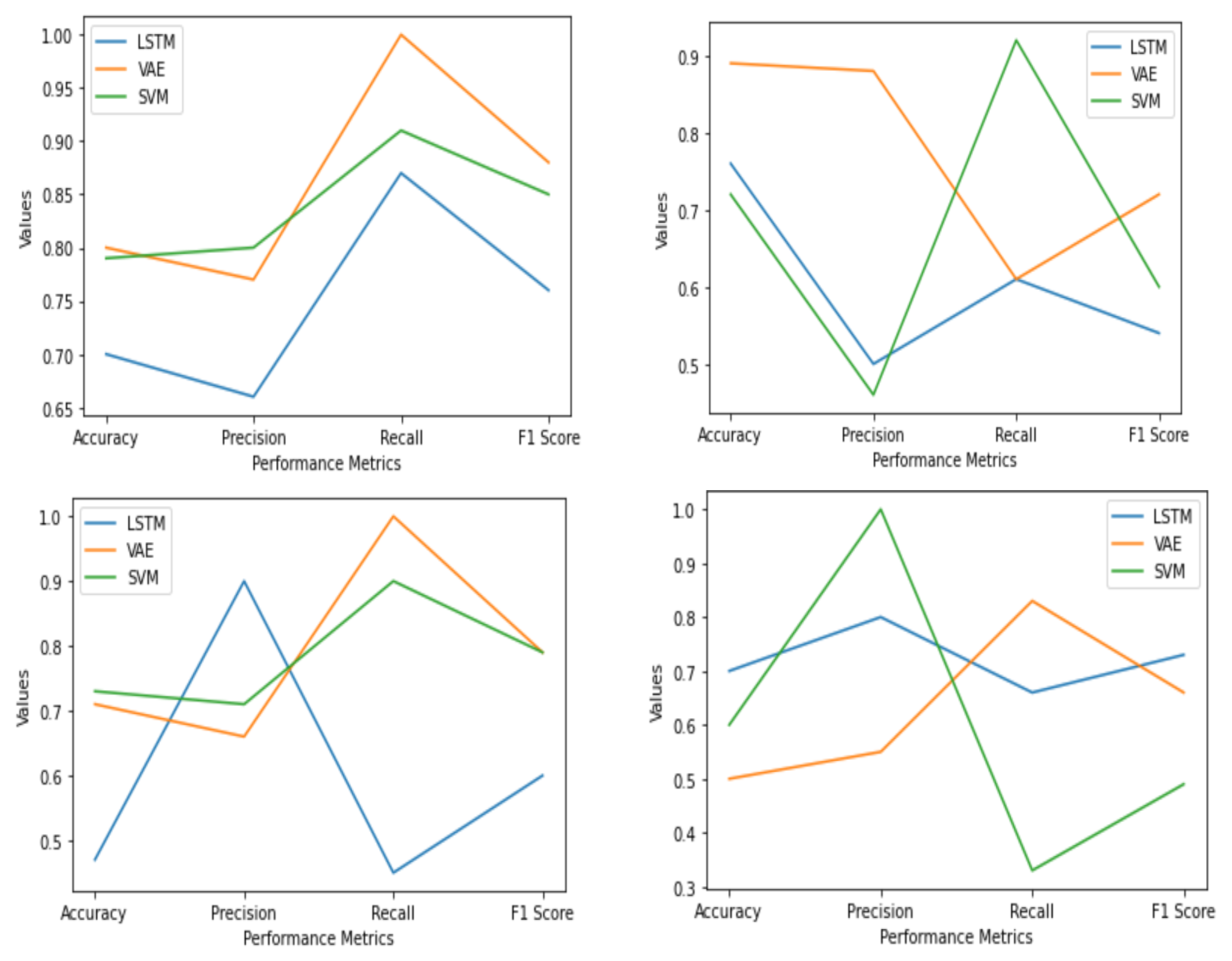
Figure 15.
Graph plotted for validation phase of 2D image and color doppler and testing phase of 2D image and color doppler respectively, without k fold cross validation.
Figure 15.
Graph plotted for validation phase of 2D image and color doppler and testing phase of 2D image and color doppler respectively, without k fold cross validation.
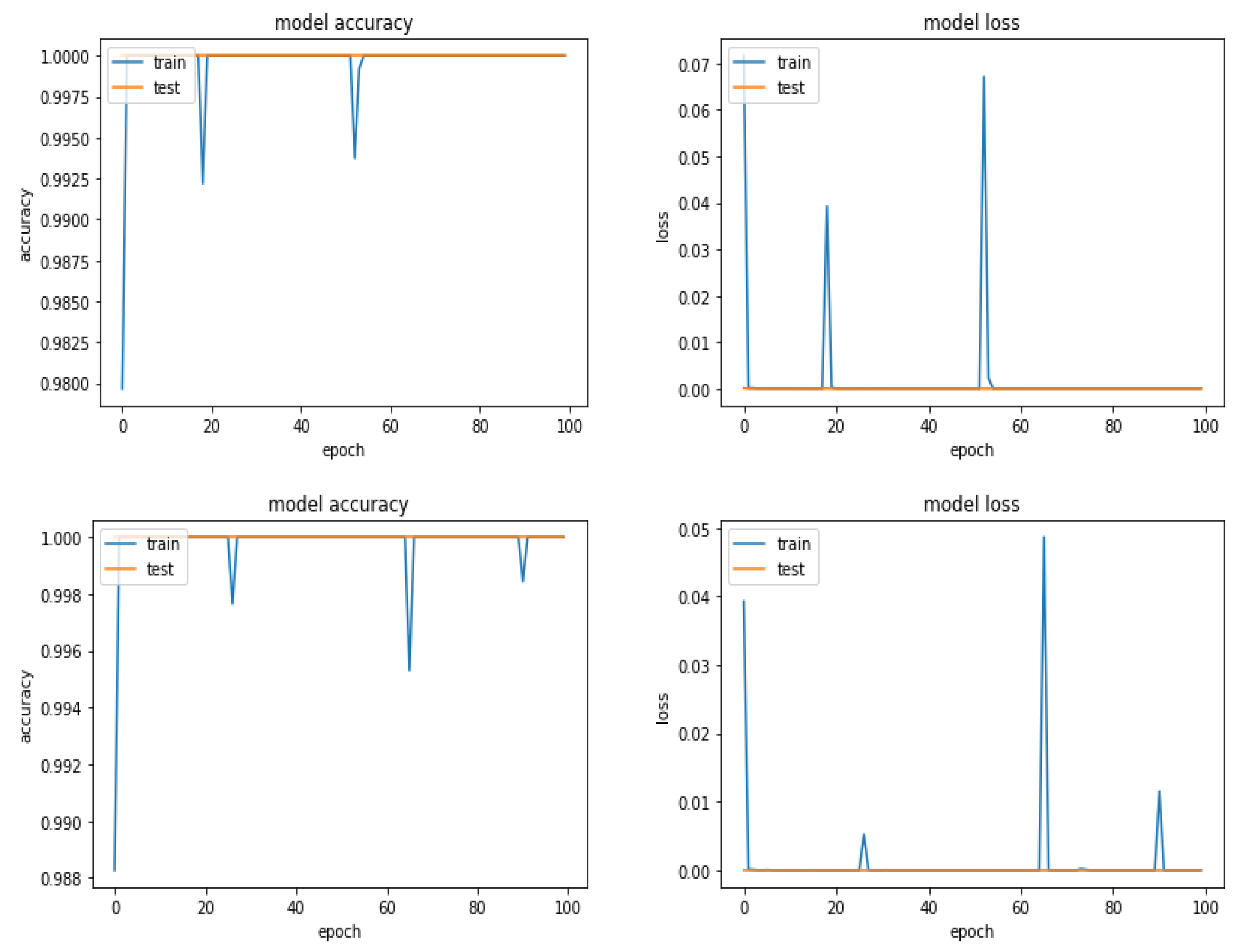
Figure 16.
Accuracy and Loss for LSTM and VAE-CNN for two-class classification for training and validation phase respectively.
Figure 16.
Accuracy and Loss for LSTM and VAE-CNN for two-class classification for training and validation phase respectively.
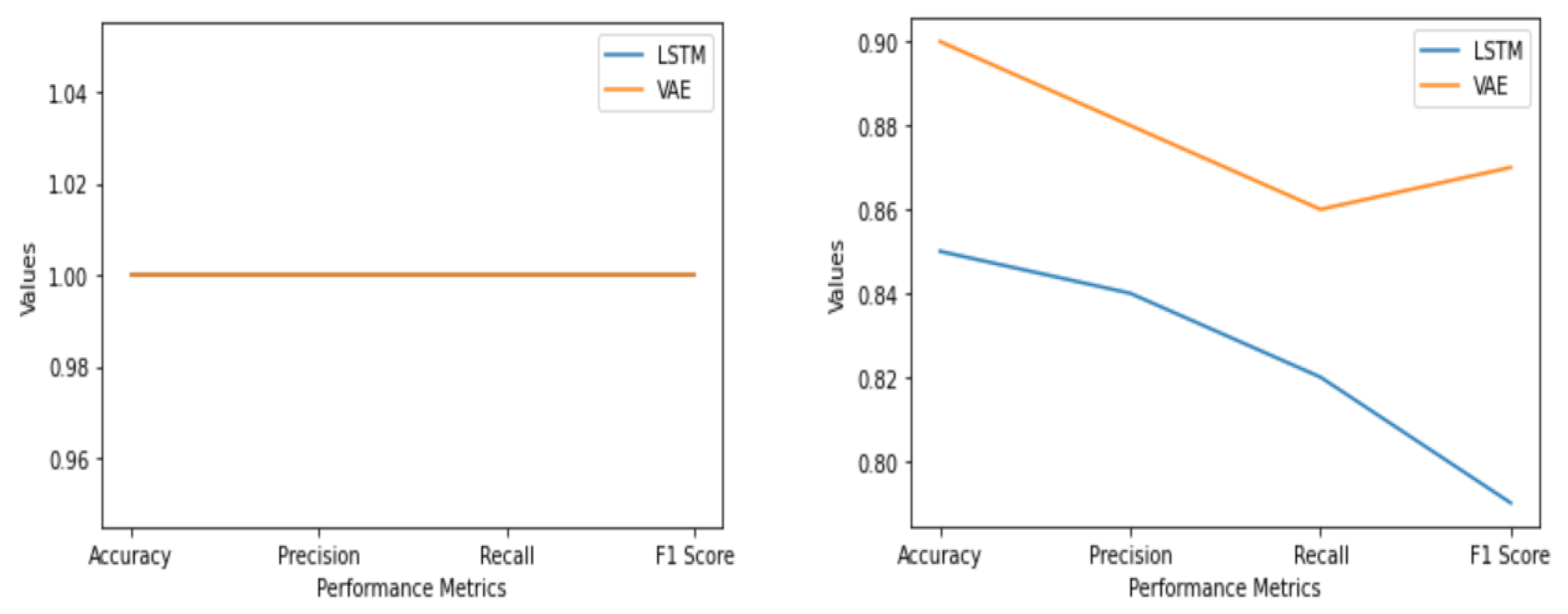
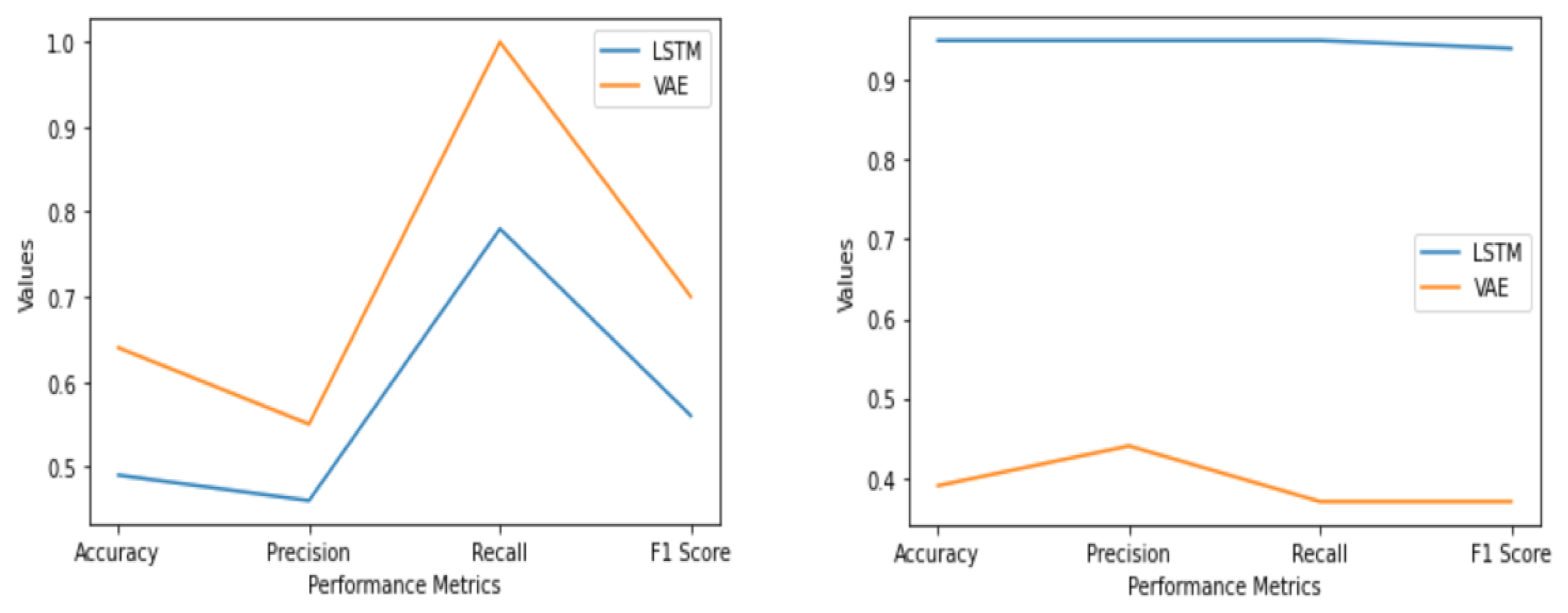
Figure 17.
Validation phase for two-class and six-class and testing phase for two-class and six-class respectively.
Figure 17.
Validation phase for two-class and six-class and testing phase for two-class and six-class respectively.
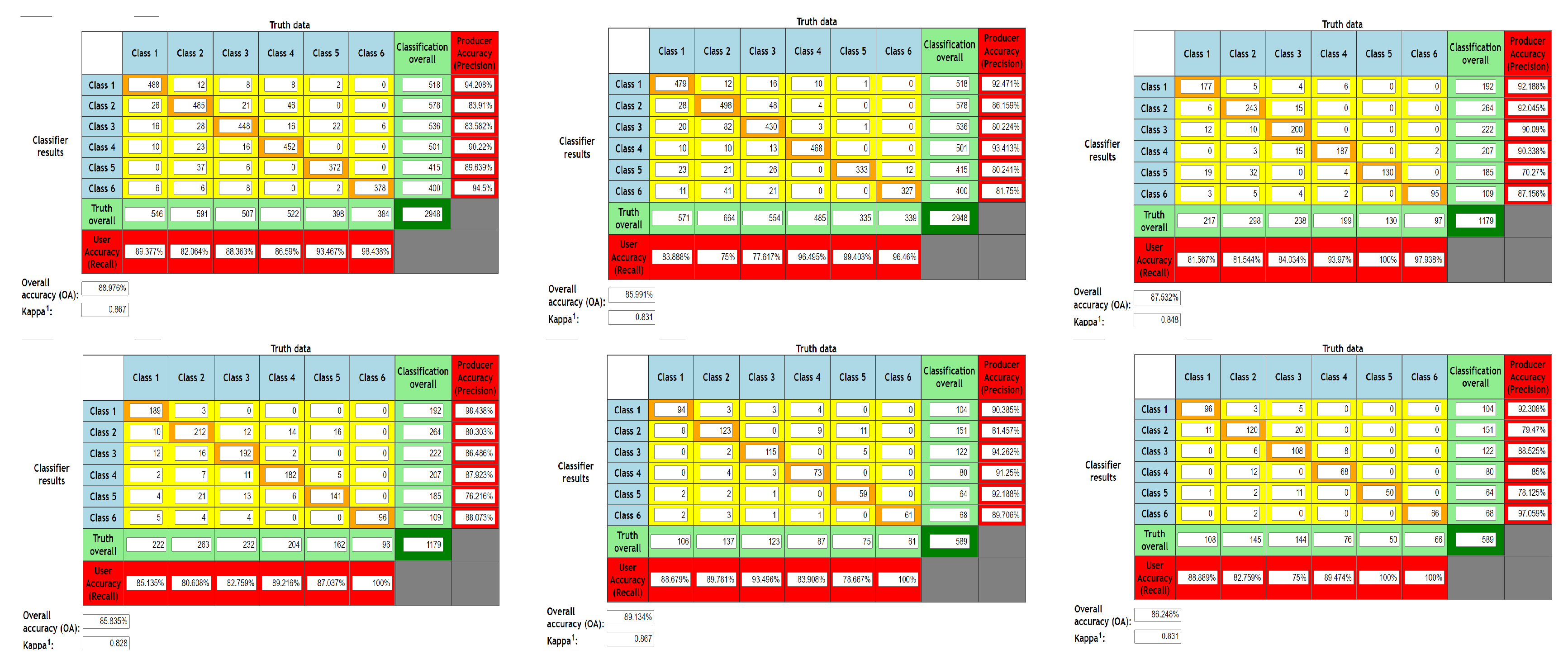
Figure 18.
Confusion matrix for 2-fold, 5-fold and 10-fold cross validation for LSTM and VAE-CNN, respectively.
Figure 18.
Confusion matrix for 2-fold, 5-fold and 10-fold cross validation for LSTM and VAE-CNN, respectively.
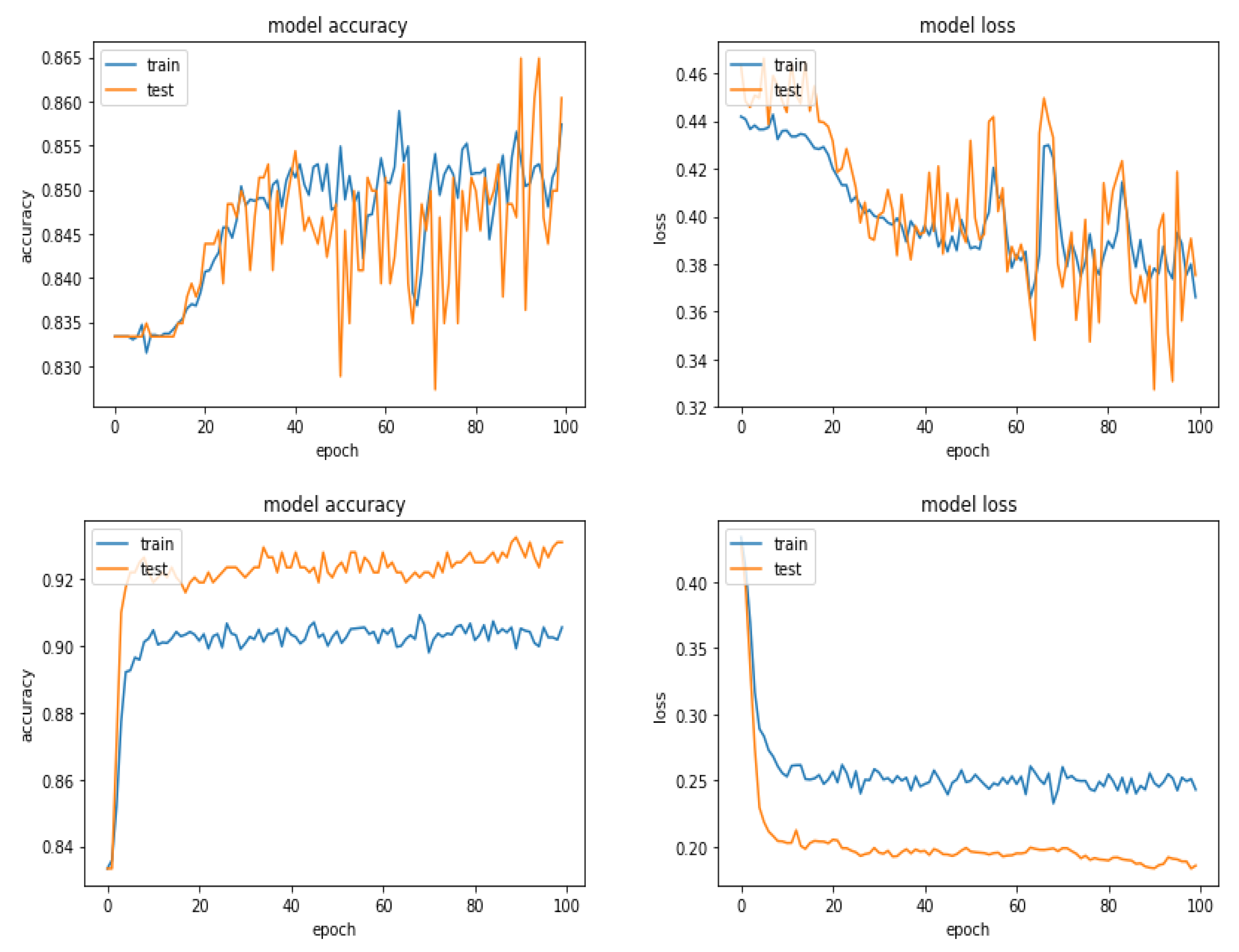
Figure 19.
Accuracy and Loss for LSTM and VAE-CNN for six-class classification for training and validation phase, respectively.
Figure 19.
Accuracy and Loss for LSTM and VAE-CNN for six-class classification for training and validation phase, respectively.
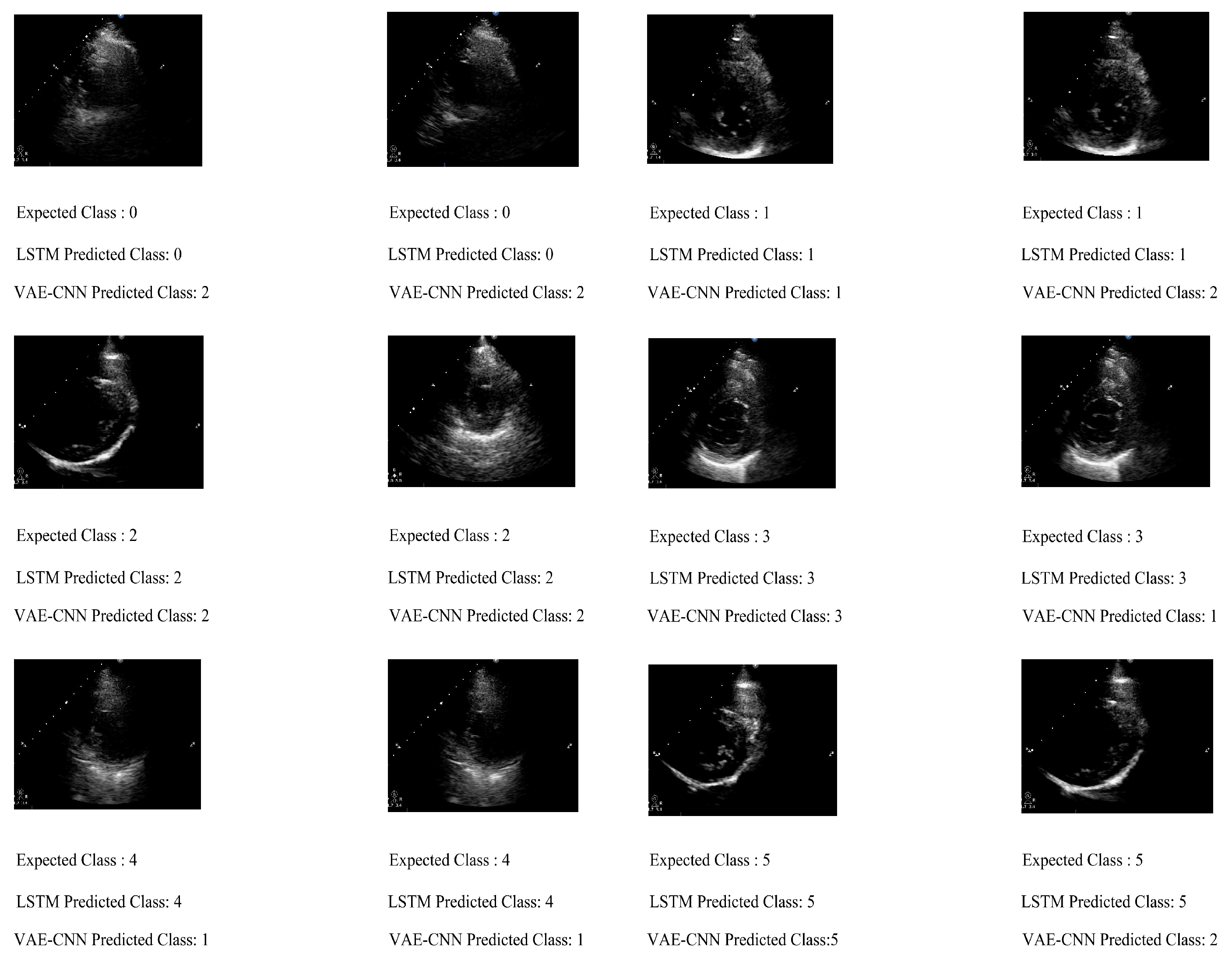
Figure 20.
Output of expected and predicted class for six-class classification using generaliza-tion approach.
Figure 20.
Output of expected and predicted class for six-class classification using generaliza-tion approach.
Table 1.
Architecture for LSTM and VAE-CNN.
Table 1.
Architecture for LSTM and VAE-CNN.
| Method | Layer Number | Layer Name | Layer Properties |
|---|
| LSTM | 1 | Input layer | Size |
| | 2 | Covolutional layer | filter size, stride = 2, output size= |
| | 3 | Flatten | 36,963 |
| | 4 | LSTM model | 126 units |
| | 5 | Dropout | 50 % dropout |
| | 6 | Fully connected layer | 50 |
| | 7 | Rectified Linear units | Rectified Linear Units |
| | 8 | Sigmoid/Softmax | Sigmoid/Softmax |
| | 9 | Classification output | 2 (normal or abnormal) and 6 (types of regurgitations) |
| VAE-CNN | 1 | Input image | |
| | 2 | Convolutional layer | filter size, stride = 2 |
| | 3 | Rectified Linear Units | Rectified Linear Units |
| | 4 | Dropout | 50 % dropout rate |
| | 5 | Max pooling | stride = 2, output size = |
| | 6 | Dropout | 50 % dropout rate |
| | 7 | Fully Connected | 9075 |
| | 8 | Fully Connected | 500 |
| | 9 | Fully Connected | 100 |
| | 10 | Fully Connected | Sample vector, 30 (Standard deviation), 30 (Mean) |
| | 11 | Fully Connected | 30 |
| | 12 | Sigmoid/Softmax | Sigmoid/Softmax |
| | 13 | Classification layer | 2 (normal or abnormal) and 6 (types of regurgitations) |
Table 2.
Output for 2D images and 3D Doppler images.
Table 2.
Output for 2D images and 3D Doppler images.
| Echo Format | 3D Doppler Images | 2D Images |
|---|
| Methodologies | LSTM | VAE-CNN | SVM | LSTM | VAE-CNN | SVM |
|---|
| Training Accuracy | 0.94 | 0.96 | 0.77 | 0.64 | 1 | 0.80 |
| Validation (labelled data) | Accuracy | 0.76 | 0.89 | 0.72 | 0.70 | 0.80 | 0.79 |
| | Precision | 0.50 | 0.88 | 0.46 | 0.66 | 0.77 | 0.80 |
| | Recall | 0.61 | 0.61 | 0.92 | 0.87 | 1 | 0.91 |
| | F1 Score | 0.54 | 0.72 | 0.60 | 0.76 | 0.88 | 0.85 |
| Testing (unlabelled) | Accuracy | 0.70 | 0.50 | 0.60 | 0.47 | 0.71 | 0.73 |
| | Precision | 0.80 | 0.55 | 1 | 0.90 | 0.66 | 0.71 |
| | Recall | 0.66 | 0.83 | 0.33 | 0.45 | 1 | 0.90 |
| | F1 Score | 0.73 | 0.66 | 0.49 | 0.60 | 0.79 | 0.79 |
| Testing 2 fold | Accuracy | 0.80 | 0.94 | 0.84 | 0.97 | 0.98 | 0.94 |
| | Precision | 0.92 | 0.97 | 0.92 | 0.97 | 0.99 | 0.96 |
| | Recall | 0.78 | 0.94 | 0.83 | 0.98 | 0.98 | 0.93 |
| | F1 Score | 0.84 | 0.95 | 0.87 | 0.97 | 0.98 | 0.94 |
| Testing 5 fold | Accuracy | 0.72 | 0.91 | 0.76 | 0.92 | 0.99 | 0.96 |
| | Precision | 0.71 | 0.88 | 0.73 | 0.95 | 0.98 | 0.97 |
| | Recall | 0.87 | 0.96 | 0.90 | 0.92 | 0.98 | 0.94 |
| | F1 Score | 0.78 | 0.91 | 0.80 | 0.93 | 0.98 | 0.98 |
| Testing 10 fold | Accuracy | 0.54 | 0.92 | 0.76 | 0.98 | 0.98 | 0.98 |
| | Precision | 0.65 | 0.94 | 0.80 | 0.96 | 0.98 | 0.98 |
| | Recall | 0.60 | 0.91 | 0.82 | 1 | 1 | 0.98 |
| | F1 Score | 0.62 | 0.92 | 0.80 | 0.97 | 0.98 | 0.98 |
Table 3.
Statistical test for comparing methodologies without k fold cross validation.
Table 3.
Statistical test for comparing methodologies without k fold cross validation.
| Type of Image | Methods | Paired T-Test (Validation) | Paired T-Test (Testing) |
|---|
| 2D image | SVM vs. LSTM | 0.493 | 0.00014 |
| | SVM vs. VAE-CNN | 0.042 | 0.153 |
| 3D Color Doppler | SVM vs. LSTM | 0.048 | 0.0005 |
| | SVM vs. VAE-CNN | 0.0003 | 0.0005 |
Table 4.
Confusion matrix for two-class (normal or abnormal) classification.
Table 4.
Confusion matrix for two-class (normal or abnormal) classification.
| Methodologies | LSTM | VAE-CNN |
|---|
| | 0 | 1 | 0 | 1 |
| Validation phase | 0 | 132 | 0 | 132 | 0 |
| | 1 | 0 | 111 | 0 | 111 |
| Testing phase | 0 | 191 | 52 | 243 | 0 |
| | 1 | 220 | 76 | 191 | 105 |
| Testing 2 fold | 0 | 812 | 0 | 805 | 7 |
| | 1 | 0 | 672 | 5 | 667 |
| Testing 5 fold | 0 | 323 | 0 | 321 | 2 |
| | 1 | 0 | 270 | 1 | 269 |
| Testing 10 fold | 0 | 182 | 0 | 181 | 1 |
| | 1 | 0 | 114 | 2 | 112 |
Table 5.
Confusion matrix for validation and testing into six-class (type of regurgitation) classification.
Table 5.
Confusion matrix for validation and testing into six-class (type of regurgitation) classification.
| Methodologies | LSTM | VAE-CNN |
|---|
| | 0 | 1 | 2 | 3 | 4 | 5 | 0 | 1 | 2 | 3 | 4 | 5 |
| Validation Phase | 0 | 73 | 3 | 0 | 5 | 0 | 0 | 77 | 0 | 0 | 4 | 0 | 0 |
| | 1 | 5 | 83 | 3 | 8 | 0 | 0 | 0 | 90 | 1 | 8 | 0 | 0 |
| | 2 | 0 | 4 | 80 | 9 | 0 | 0 | 0 | 11 | 82 | 0 | 0 | 0 |
| | 3 | 4 | 2 | 3 | 74 | 0 | 0 | 0 | 0 | 6 | 77 | 0 | 0 |
| | 4 | 3 | 0 | 4 | 10 | 62 | 0 | 6 | 2 | 4 | 3 | 64 | 0 |
| | 5 | 13 | 6 | 6 | 0 | 0 | 56 | 0 | 8 | 6 | 8 | 0 | 59 |
| Testing Phase | 0 | 89 | 4 | 0 | 3 | 0 | 0 | 20 | 9 | 67 | 0 | 0 | 0 |
| | 1 | 3 | 178 | 2 | 1 | 5 | 0 | 45 | 80 | 22 | 30 | 10 | 2 |
| | 2 | 0 | 0 | 134 | 0 | 0 | 0 | 15 | 10 | 95 | 14 | 0 | 0 |
| | 3 | 0 | 0 | 0 | 126 | 0 | 0 | 0 | 48 | 0 | 56 | 22 | 0 |
| | 4 | 0 | 0 | 2 | 12 | 87 | 0 | 0 | 60 | 0 | 12 | 29 | 0 |
| | 5 | 0 | 0 | 0 | 0 | 0 | 91 | 0 | 23 | 36 | 15 | 0 | 17 |
Table 6.
Output for Video 2 (normal or abnormal) and six-class (types of regurgitation).
Table 6.
Output for Video 2 (normal or abnormal) and six-class (types of regurgitation).
| Echo Format | Video 2 Class | Video 6 Class |
|---|
| Methodologies | LSTM | VAE-CNN | LSTM | VAE-CNN |
|---|
| Training Accuracy | 1 | 1 | 0.86 | 0.93 |
| Validation | Accuracy | 1 | 1 | 0.85 | 0.90 |
| | Precision | 1 | 1 | 0.84 | 0.88 |
| | Recall | 1 | 1 | 0.82 | 0.86 |
| | F1 Score | 1 | 1 | 0.79 | 0.87 |
| Testing | Accuracy | 0.49 | 0.64 | 0.95 | 0.39 |
| | Precision | 0.46 | 0.55 | 0.95 | 0.44 |
| | Recall | 0.78 | 1 | 0.95 | 0.37 |
| | F1 Score | 0.56 | 0.70 | 0.94 | 0.37 |
| Testing 2 fold | Accuracy | 1 | 0.99 | 0.88 | 0.85 |
| | Precision | 1 | 0.99 | 0.89 | 0.85 |
| | Recall | 1 | 0.99 | 0.89 | 0.88 |
| | F1 Score | 1 | 0.99 | 0.89 | 0.86 |
| Testing 5 fold | Accuracy | 1 | 0.99 | 0.87 | 0.85 |
| | Precision | 1 | 0.99 | 0.86 | 0.86 |
| | Recall | 1 | 0.99 | 0.89 | 0.87 |
| | F1 Score | 1 | 0.99 | 0.87 | 0.86 |
| Testing 10 fold | Accuracy | 1 | 0.98 | 0.89 | 0.86 |
| | Precision | 1 | 0.98 | 0.89 | 0.86 |
| | Recall | 1 | 0.98 | 0.89 | 0.89 |
| | F1 Score | 1 | 0.98 | 0.89 | 0.87 |
Table 7.
LSTM precision, recall and F1 Score for validation and testing phase for six-class classification.
Table 7.
LSTM precision, recall and F1 Score for validation and testing phase for six-class classification.
| No | Precision | Validation | Testing | Recall | Validation | Testing | F1 Score | Validation | Testing |
|---|
| 1 | P0 | 0.74 | 0.96 | R0 | 0.90 | 0.92 | F0 | 0.70 | 0.93 |
| 2 | P1 | 0.82 | 0.97 | R1 | 0.83 | 0.94 | F1 | 0.82 | 0.95 |
| 3 | P2 | 0.83 | 0.97 | R2 | 0.86 | 1 | F2 | 0.84 | 0.98 |
| 4 | P3 | 0.69 | 0.88 | R3 | 0.89 | 1 | F3 | 0.77 | 0.93 |
| 5 | P4 | 1 | 0.95 | R4 | 0.78 | 0.86 | F4 | 0.87 | 0.90 |
| 6 | P5 | 1 | 1 | R5 | 0.66 | 1 | F5 | 0.79 | 1 |
Table 8.
VAE-CNN precision, recall and F1 Score for validation and testing phase for six-class classification.
Table 8.
VAE-CNN precision, recall and F1 Score for validation and testing phase for six-class classification.
| No | Precision | Validation | Testing | Recall | Validation | Testing | F1 Score | Validation | Testing |
|---|
| 1 | P0 | 0.92 | 0.25 | R0 | 0.95 | 0.20 | F0 | 0.94 | 0.22 |
| 2 | P1 | 0.81 | 0.34 | R1 | 0.90 | 0.42 | F1 | 0.85 | 0.36 |
| 3 | P2 | 0.82 | 0.43 | R2 | 0.88 | 0.70 | F2 | 0.84 | 0.53 |
| 4 | P3 | 0.77 | 0.44 | R3 | 0.92 | 0.44 | F3 | 0.89 | 0.44 |
| 5 | P4 | 1 | 0.47 | R4 | 0.81 | 0.28 | F4 | 0.89 | 0.37 |
| 6 | P5 | 1 | 0.89 | R5 | 0.72 | 0.18 | F5 | 0.84 | 0.30 |


 ,
, 























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}