1. Introduction
The number of dangerous diseases has increased in recent years due to demographic shifts in developing and developed countries [
1]. Despite advances in medical techniques, effective treatments for dementia and Alzheimer’s disease remain elusive, except for some drugs that delay the diseases’ progression. Therefore, early diagnosis plays an important role in stopping the progression of the diseases to their advanced stages [
1,
2]. Some of the severe chronic conditions that have attracted much attention in the field of mental health are dementia and Alzheimer’s diseases because of their widespread prevalence among the elderly and their harmful effects on the elderly’s cognitive abilities to conduct daily activities normally. Dementia is the loss or impairment of memory to conduct healthy mental abilities due to age or disease; it is characterised by changes in the mind and behavioural disturbance or stroke. It is a syndrome that includes impaired memory, behaviour and thinking and the loss of ability to perform daily activities [
3,
4]. According to the reports of the World Health Organization (WHO), about 47 million people suffer from dementia around the world, and the number is rapidly increasing annually; the number of sufferers could reach 82 million people by 2030. The underlying causes of dementia are neurodegeneration and weak brain connectivity, which lead to poor decision-making; the non-neurodegenerative mechanisms result in vascular dementia. Alzheimer’s disease (AD) is one of the most common and prevalent types of dementia and accounts for 60% to 70% of dementia cases. Age is the direct cause of AD, especially in people over the age of 65. AD has a more noticeable prevalence among women than men. However, AD aetiology has not yet been identified. The main hypotheses are based on the accumulation of extracellular A
peptides and the accumulation of hyperphosphorylated tau proteins inside brain cells. These two structures are biomarkers called amyloid plaques (an accumulation of beta-amyloid fragments between neurons) and tangles (intracellular accumulations of tau protein in the form of twisted fibrils). A biomarker is a measure or indicator of the brain’s biological state. Biomarkers appear early before clinical symptoms appear [
5]. Thus, as a histopathological procedure, the accumulation of amyloid plaques and neurofibrillary tangles is responsible for neuronal damage and death [
6,
7], thereby leading to progressive memory loss with physiological changes in thinking and behaviour. Dementia and Alzheimer’s are multifactorial diseases that occur independently from physiological aging parameters, such as diet, sleep disturbances, environmental factors, sedentary lifestyle and genetic predisposition.
AD is one of the main causes of intellectual disability among the elderly worldwide. At the onset of AD, a combination of psychological and mental evaluation occurs, such as that involving tau protein and cerebrovascular amyloid protein, to find synapses, brain plaques and neuronal degeneration. There are measures to assess cognitive and mental decline in the elderly, such as tacrine for the level of symptoms and assessment of genetic history to identify Down syndrome [
8,
9]. AD is then evaluated by a brain imaging called Pittsburgh Compound B (PIB), which is based on n-positron emission tomography (PET); it is considered for the early detection and monitoring of AD [
10,
11]. Subsequently, the AD Neuroimaging Initiative (ADNI) is established; it standardises image formats with psychological and intellectual tests to monitor the effectiveness of treatment and early detection of disease. There is an urgent need to identify biomarkers that can detect histological changes in the brain, which may indicate neurological disorders, such as atrophy and amyloid plaques; these changes may represent early signs of dementia, and AD can be predicted. Thus, biomarkers help us differentiate between dementia and AD and predict them early. In recent years, researchers have provided biomarkers in the form of neuroimaging techniques, such as MRI, single-photon emission computed tomography (SPECT) and Positron Emission Tomography (PET), which had a prominent role in the early diagnosis of both dementia and Alzheimer’s [
12]. Diagnosing the soft tissues of the brain and distinguishing them from healthy tissues are essential for the early prediction of dementia and AD. Manually extracting features from MRI images or medical records requires a great deal of time and effort from experts. Similarities between soft and healthy tissues in MRI make manual diagnosis more prone to errors [
13]. Therefore, this paper aimed to evaluate the use of machine learning algorithms on the Open Access Series of Imaging Studies (OASIS) dataset for the early prediction of dementia and the use of deep learning algorithms and hybrid techniques between deep and machine learning on MRI dataset for the early prediction of AD and for differentiating disease stages and severity from mild to moderate to severe. Machine learning, deep learning and hybrid and pattern analysis technologies serve as powerful tools for building predictive models based on MRI images and medical records for computer-aided diagnosis. Deep learning techniques extract deep representative feature maps without the need for manual feature representation. All results are more effective, consistent, less likely to create bias and proven to be effective in diagnosing dementia and AD compared with manual approaches.
Duc et al. introduced a deep learning-based method for assessing Mini-Mental State Examination (MMSE) through resting-state functional Magnetic Resonance Imaging (rs-fMRI); the system yielded good results for the diagnosis of AD [
14]. Li et al. presented a deep learning model and validated the diagnosis of 2146 cases of magnetic resonance imaging to predict the progression of mild cognitive impairment (MCI) to AD dementia [
15]. Francesco et al. introduced deep learning techniques to evaluate an EEG dataset to distinguish Creutzfeldt–Jakob disease from other dementias. The method is based on the extraction of time frequencies from EEG by continuous wavelet transform (CWT) algorithm and measuring complex EEG signals through permutation entropy (PE) [
16]. Amoroso et al. applied the random forest technique to select the most important features extracted from the dataset that contains four classes, namely, HC, AD, MCI and cMCI, and their classification by DNN techniques [
17]. Popuri et al. presented a model calculating the FDG-PET DAT score (FPDS) as a score between 0 and 1 for the diagnosis of dementia of Alzheimer’s type (DAT) [
18]. Raza et al. introduced a system for diagnosing AD and monitoring similar diseases through machine learning techniques [
19]. Aram et al. presented several machine learning algorithms to evaluate the MMSE-KC and CERAD-K datasets for the diagnosis of dementia. The MMSE-KC dataset was diagnosed as normal or abnormal, whereas the CERAD-K dataset was diagnosed as both dementia and mild cognitive impairment [
20]. Chen et al. introduced many machine learning algorithms and statistical methods for diagnosing people with dementia or no dementia; among these, Bayesian and SVM algorithms achieved the best performance [
21]. Joshi et al. applied machine learning and deep learning methods to diagnose dementia. The system achieved the best accuracy when collecting tests for both machine and deep learning [
22]. Cho et al. introduced a double-layer hierarchical architecture for the early diagnosis of dementia. The Bayesian algorithm runs at the top layer, whereas the FCM and PNN algorithms run at the base layer [
23]. Trambaiolli et al. presented an SVM algorithm to evaluate the electroencephalography (EEG) dataset to classify EEG signals as normal and Alzheimer’s images. The SVM algorithm achieved an accuracy of 87% [
24]. Shanklea et al. presented a machine learning algorithm to predict CDR; the Naive Bayes algorithm achieved the highest accuracy among all algorithms [
25]. Ekin et al. presented a 3D VGG convolutional neural network to preserve 3D MRI images while converting them to 2D through convolutional layers. The system was evaluated by using the ADNI and OASIS datasets, and the system achieved an accuracy of 73.4% for the ADNI dataset and an accuracy of 69.9% for the OASIS dataset [
26]. Pinaya et al. presented standardised module-based autoencoder models for a neuroimaging dataset for AD diagnosis and trained an independent dataset on autoencoder modules. Then, they monitored the deviation of each patient and identified the deviated brain regions based on the autoencoder units [
27]. Jorge et al. presented a spatio-temporal LME method based on Linear Mixed Effects (LME). The method exploits the spatial structure of MRI images to analyse measurements on the cortical surface. The method achieved good results [
28]. The main contributions to this study are as follows:
First, for the OASIS dataset:
Distribution of the converted class records to the non-demented and demented classes based on a feature value of CRD.
Representation of high-dimensional data in low-dimensional data space by the t-SNE algorithm.
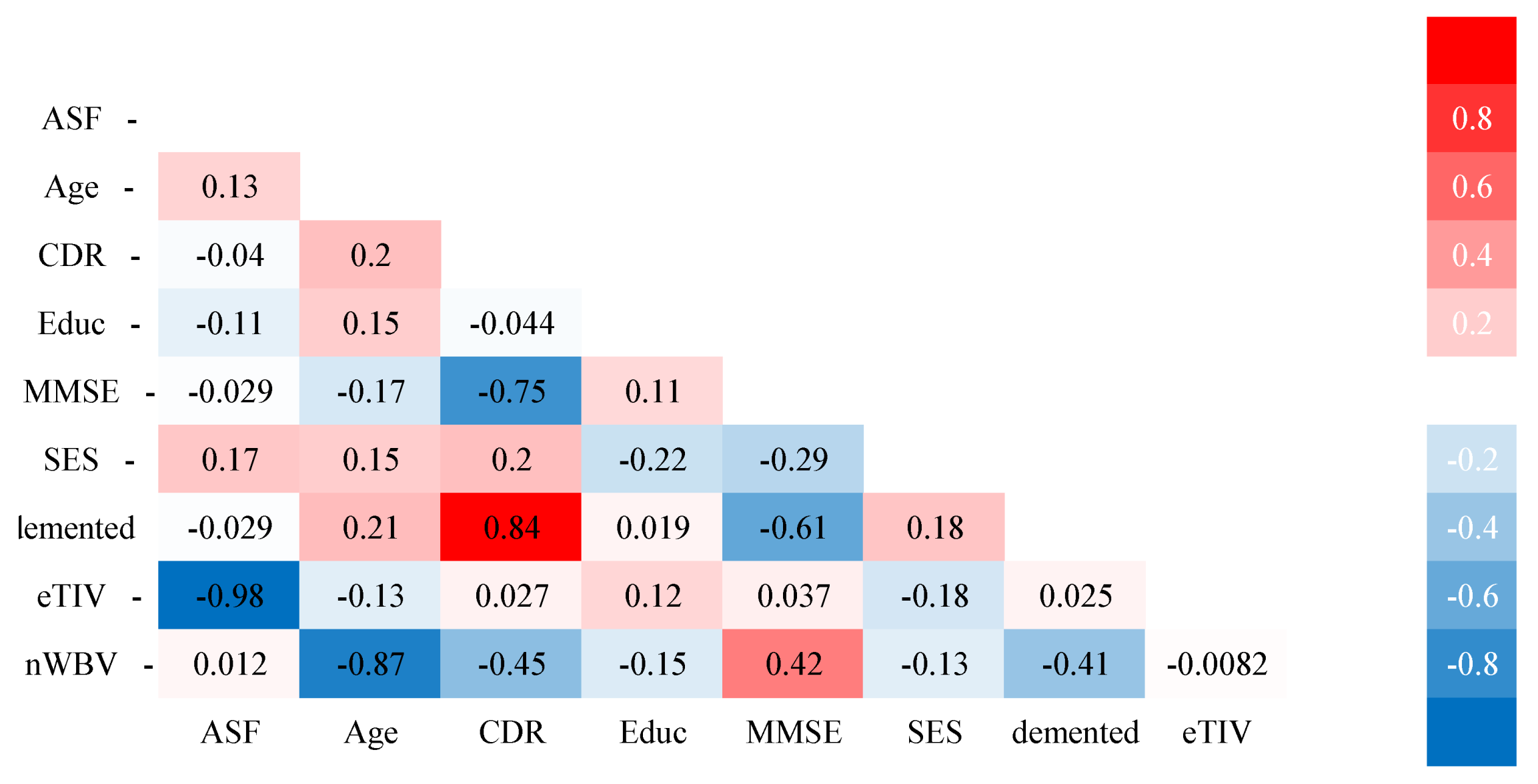
Representation of the correlation of each feature with the other and the correlation of each feature with the target feature.
Second, for the MRI dataset:
Balance the dataset by data augmentation technique to multiply the minority classes.
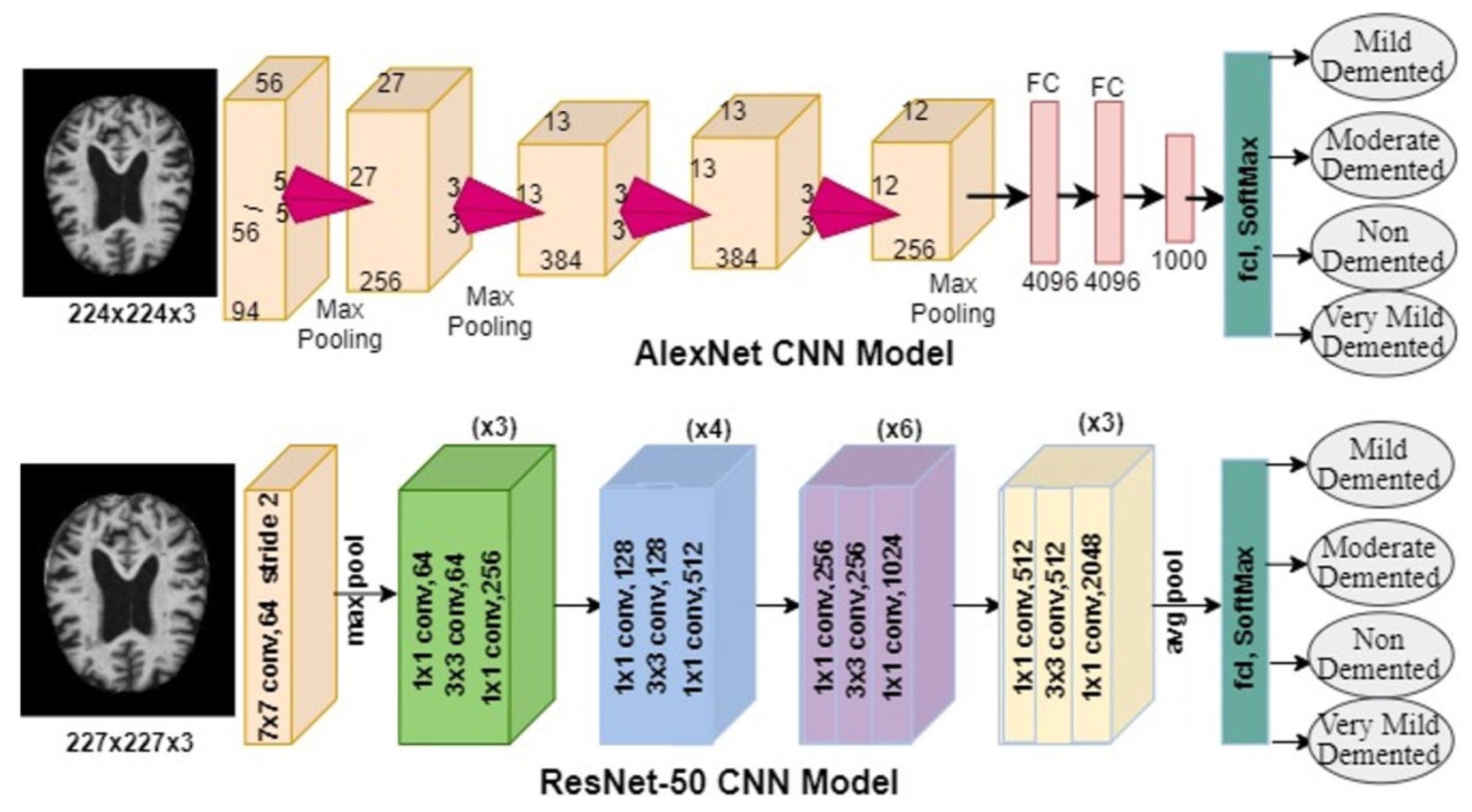
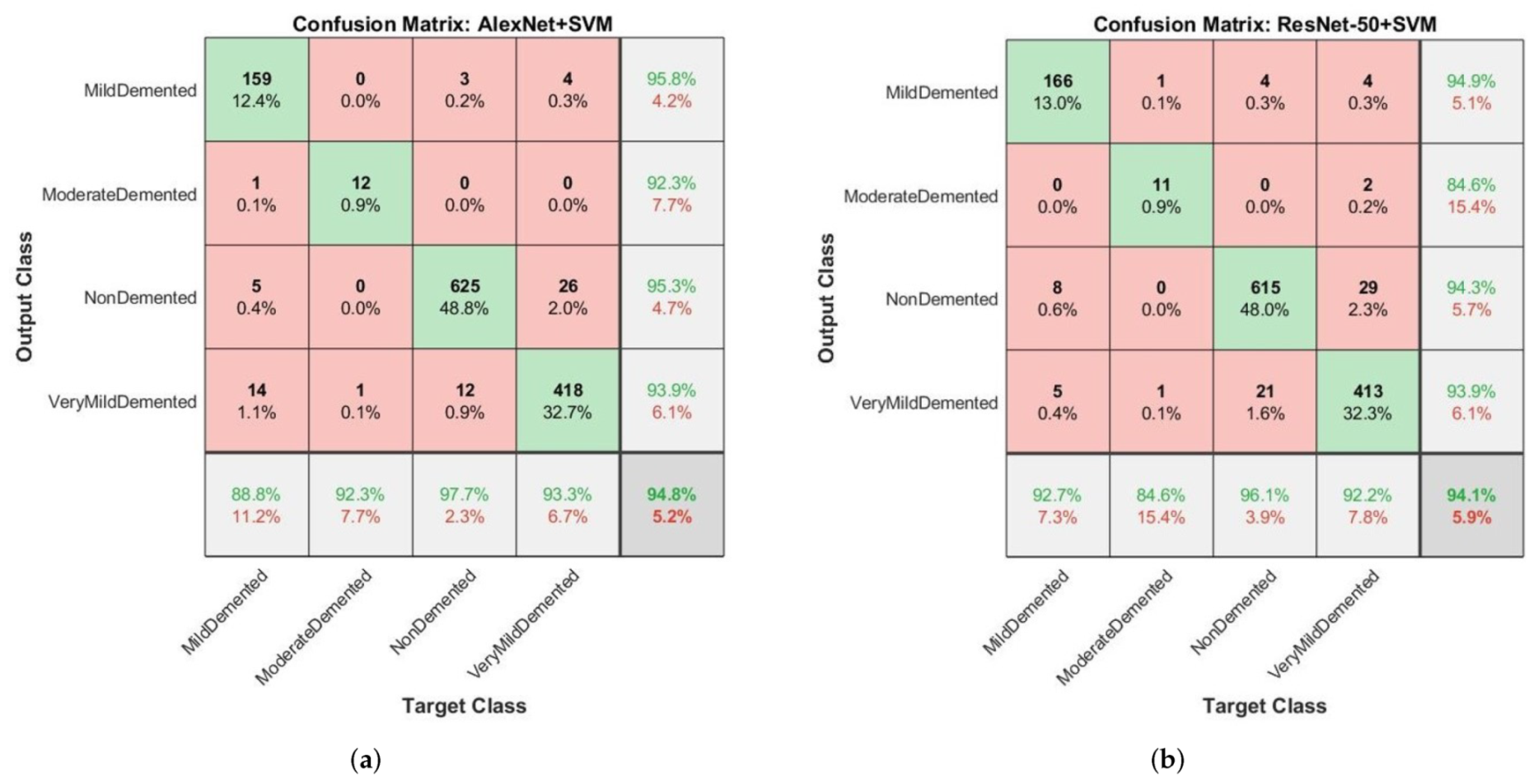
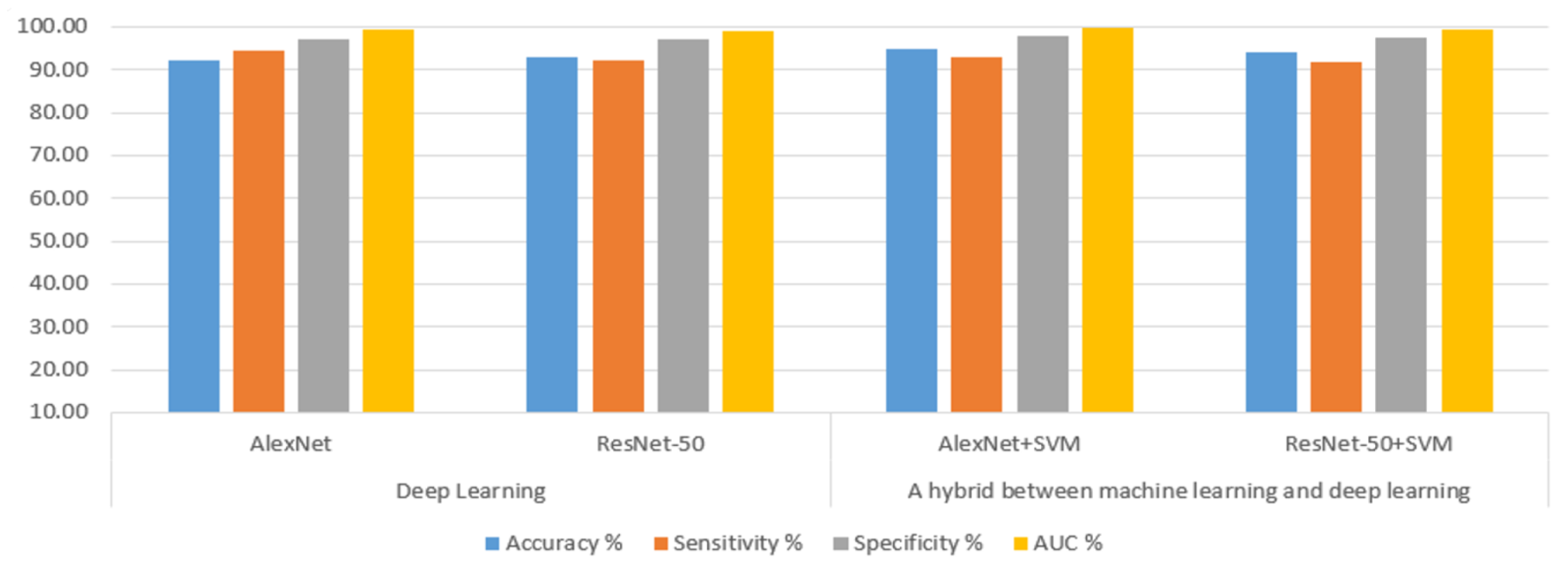
Apply hybrid techniques between deep learning based on AlexNet and ResNet-50 models and machine learning based on SVM classifier to produce hybrid AlexNet+SVM and ResNet-50+SVM models that achieve high performance and effective diagnosis of AD.
Machine learning, deep learning and hybrid techniques can be generalised with high efficiency to diagnose dementia and AD with the help of clinicians and experts and support their diagnostic decisions.
The remainder of the paper is organised as follows.
Section 2 describes materials and methods and contains subsections for describing the two datasets and processing features.
Section 3 reviews classification techniques.
Section 4 presents the results of the analysis and diagnosis.
Section 5 is the conclusion of the paper.
5. Conclusions
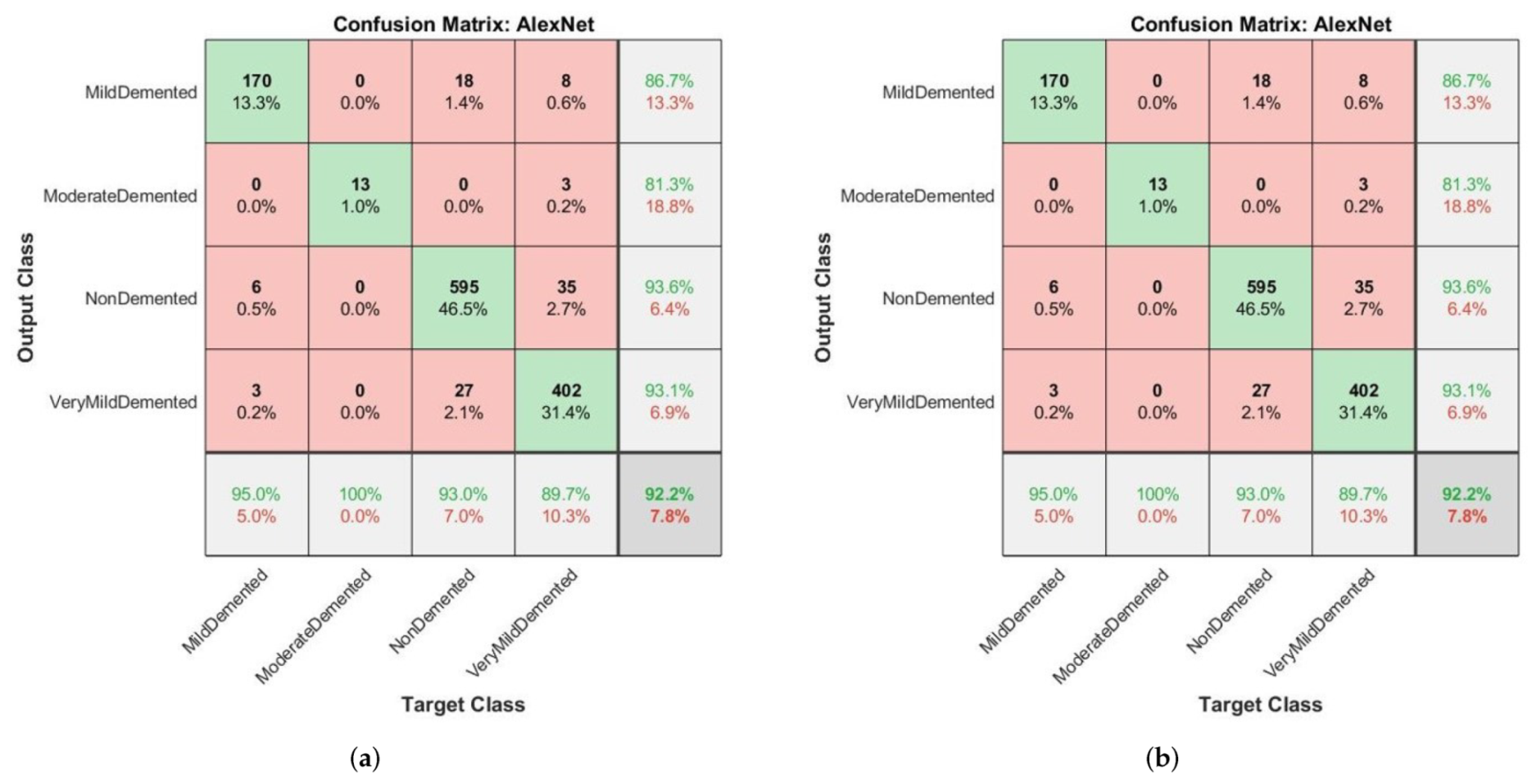
Dementia and AD are among the diseases that affect the elderly and their lives. Thus, an effective diagnosis of AD is an important factor in overcoming the disease. The volume of spending on AD and its economic impact amount to a trillion dollars. This indicates that the early diagnosis of dementia and AD is crucial. Considering the difficulty of manual diagnosis by doctors, artificial intelligence techniques have played an important role in the early diagnosis of dementia and AD. In this paper, we used two datasets. The first dataset was OASIS, which comprises medical records. SMOTE algorithm was applied to balance the dataset. The missing values were processed by replacing them using the median method. The relationship ratio between each feature and the target feature was found. The t-SNE algorithm was used to represent high-dimensional data in low-dimensional space. Finally, these features were diagnosed by four machine learning algorithms, namely, SVM, Decision Tree, Random Forest and KNN, and the dataset was divided into 80% for training and 20% for testing. All algorithms achieved effective results, the best of which was achieved by using the random forest classifier. It achieved an overall accuracy of 94% and precision, recall and F1 scores of 93%, 98% and 96%, respectively. The second dataset is MRI. All images were optimised to remove noise and artifacts through the average filter. Data augmentation method was used to balance the dataset and overcome the problem of overfitting. The dataset was divided into 80% for training and validation and 20% for testing. Deep feature maps were extracted through AlexNet and ResNet-50 models, where 9216 features were extracted for each image. Feature maps were fed to both fully connected layers. These maps were an extension of deep learning and the SVM algorithm and were the features of a hybrid method. The hybrid algorithm between machine learning and deep learning achieved better results than deep learning, with the AlexNet+SVM model achieving accuracy, sensitivity, specificity and AUC values of 94.8%, 93%, 97.75% and 99.7%, respectively.


 ,
, 










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}