
Acne-like Eruptions: Disease Features and Differential Diagnosis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Background
2. Acne-like Eruptions in the Adult Population
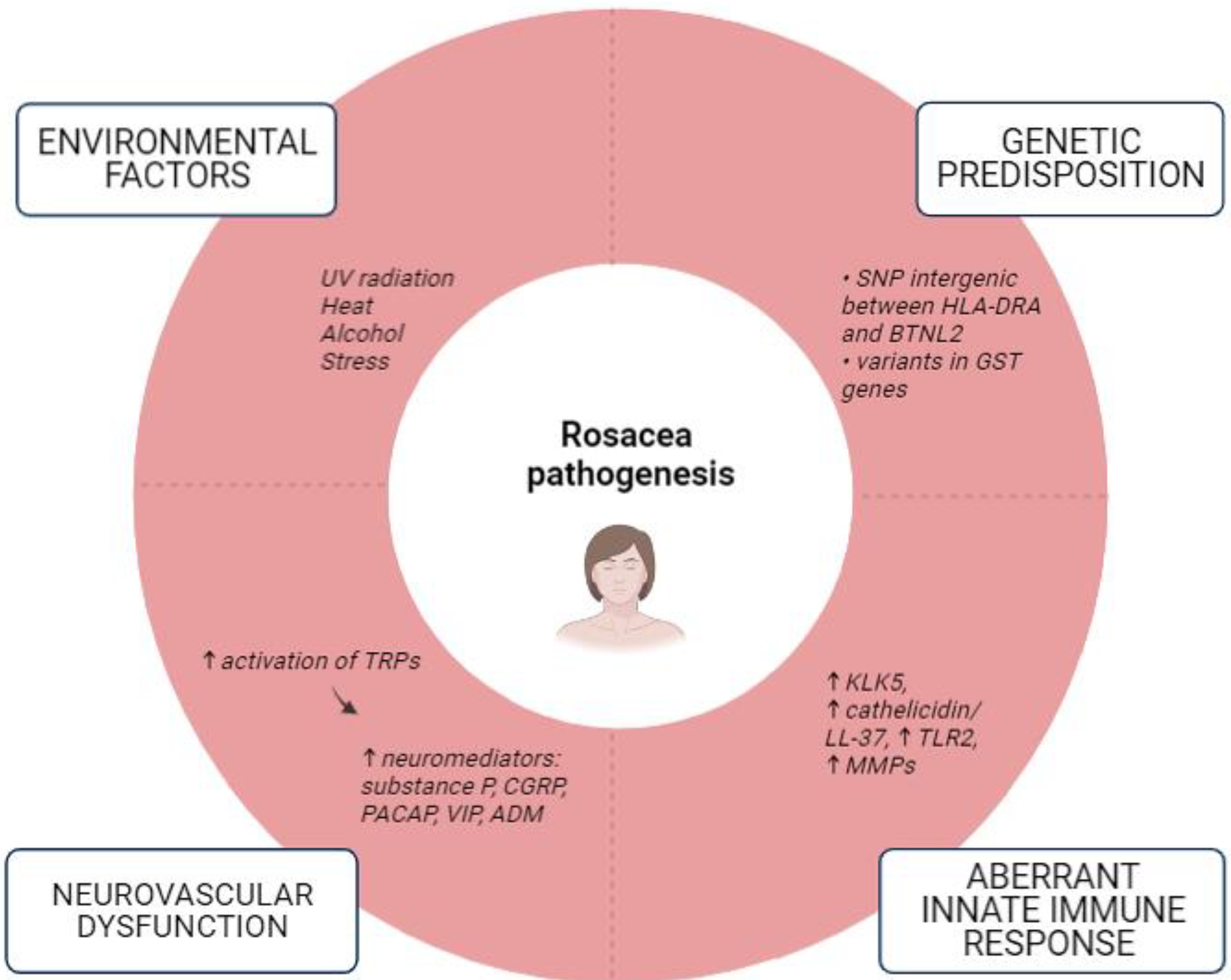
2.1. Rosacea
2.2. Demodicosis
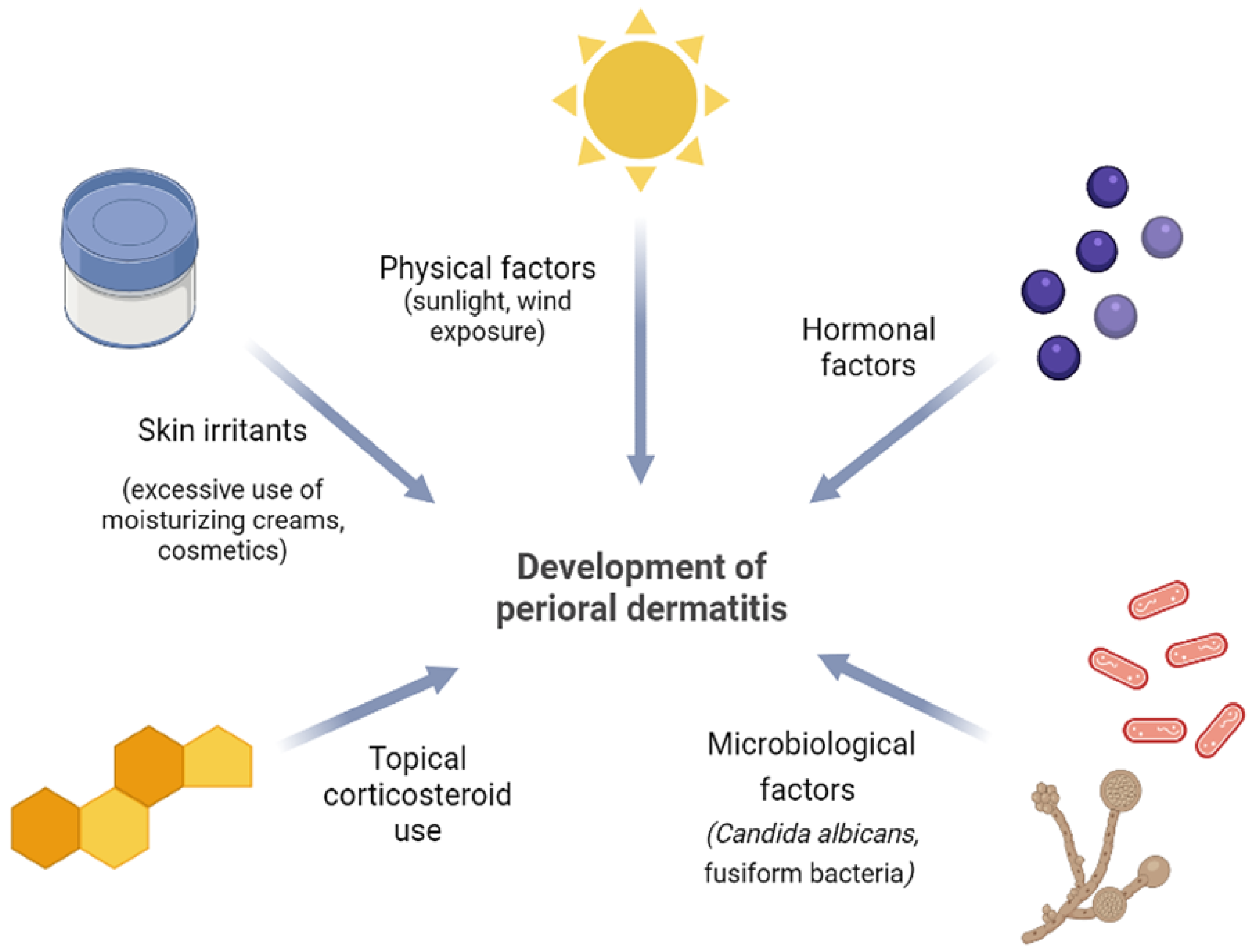
2.3. Perioral Dermatitis
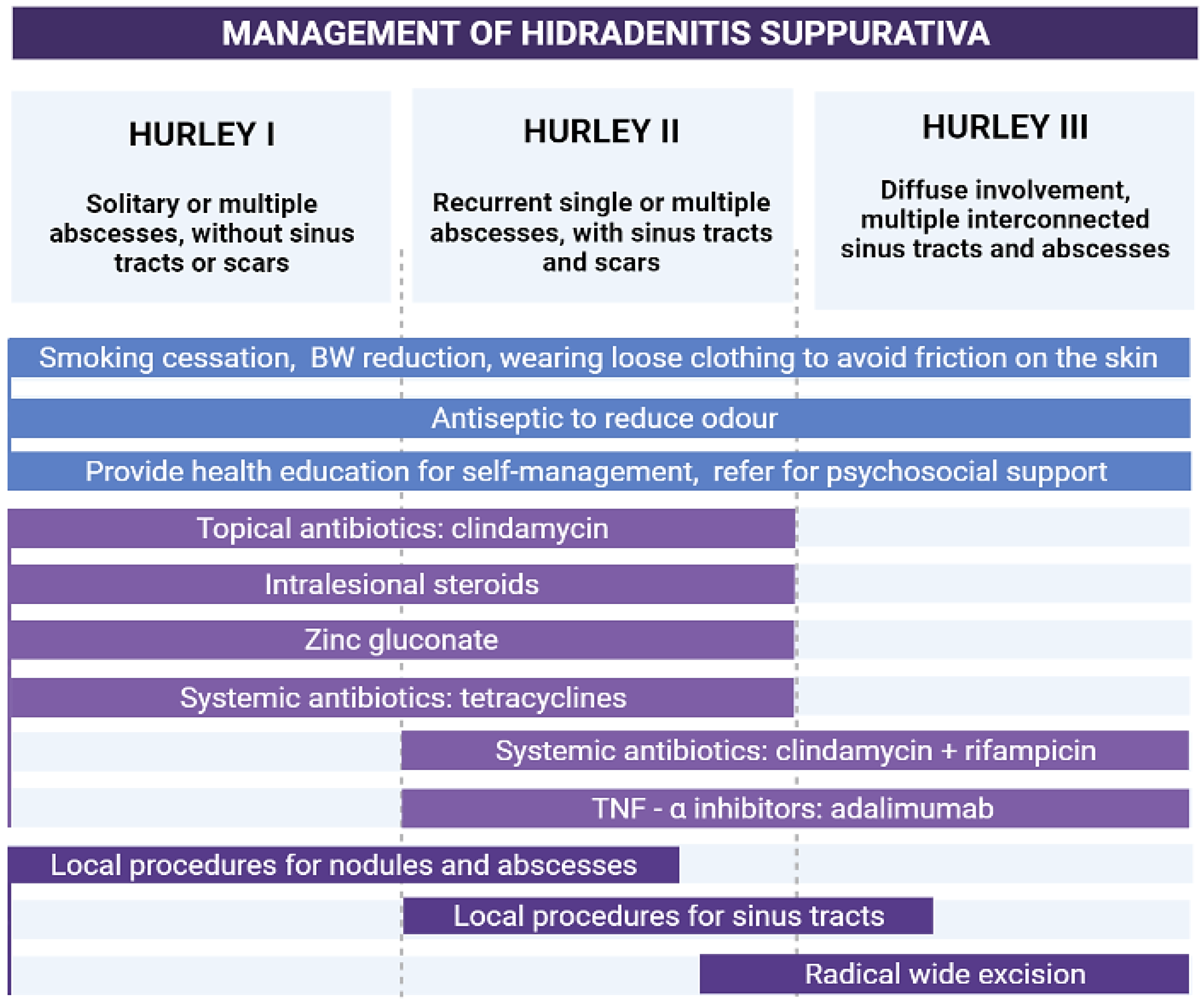
2.4. Hidradenitis Suppurativa
2.5. Pseudofolliculitis Barbae
2.6. Eosinophilic Pustular Folliculitis
2.7. Sarcoidosis
2.8. Papular Granuloma Annulare
2.9. Periorificial Granulomatous Dermatitis
3. Infectious Diseases Resembling Acne
3.1. Bacterial Folliculitis
3.2. Gram-Negative Folliculitis
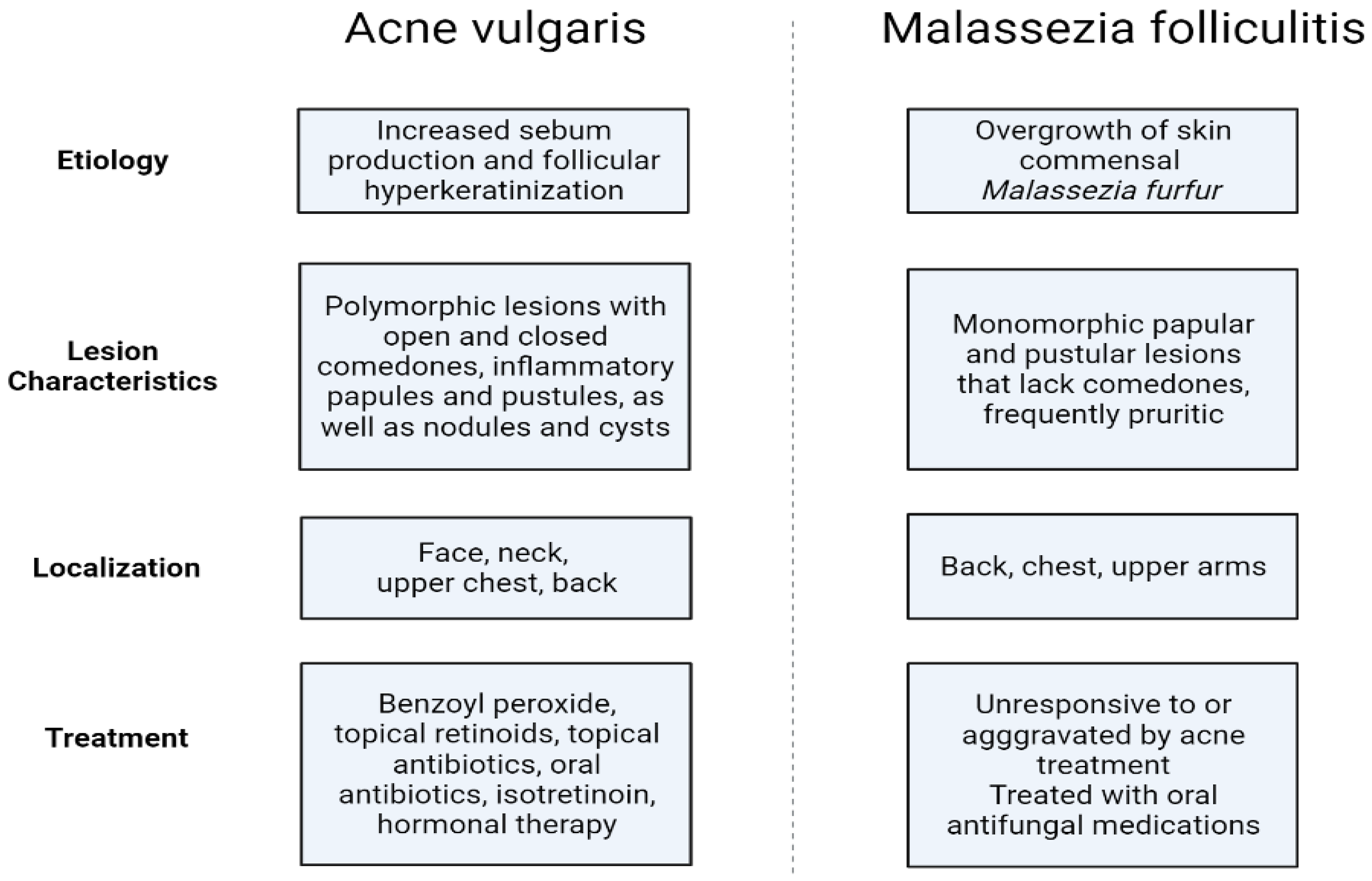
3.3. Malassezia Folliculitis
3.4. Hot Tub Folliculitis
3.5. Sporotrichosis
3.6. Cutaneous Coccidioidomycosis
3.7. Secondary Syphilis
4. Acne-like Eruptions Resulting from Exposure to Chemical and Physical Agents
4.1. Acne Aestivalis
4.2. Acne Mechanica
4.3. Acne Cosmetica
4.4. Radiation Acne
4.5. Chloracne
4.6. Oil Acne
4.7. Coal Tar Acne
4.8. Drug-Induced Acne-like Eruptions
4.8.1. Steroid Acne
4.8.2. Epidermal Growth Factor Receptor Inhibitors
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Layton, A.M.; Thiboutot, D.; Tan, J. Reviewing the Global Burden of Acne: How Could We Improve Care to Reduce the Burden? Br. J. Dermatol. 2020, 184, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Sutaria, A.H.; Masood, S.; Schlessinger, J. Acne Vulgaris. Available online: https://www.ncbi.nlm.nih.gov/books/NBK459173 (accessed on 9 April 2023).
- Ogé, L.K.; Broussard, A.; Marshall, M.D. Acne Vulgaris: Diagnosis and Treatment. Am. Fam. Physician 2019, 100, 475–484. [Google Scholar] [PubMed]
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef] [PubMed]
- Hay, R.J.; Johns, N.E.; Williams, H.C.; Bolliger, I.W.; Dellavalle, R.P.; Margolis, D.J.; Marks, R.; Naldi, L.; Weinstock, M.A.; Wulf, S.K.; et al. The Global Burden of Skin Disease in 2010: An Analysis of the Prevalence and Impact of Skin Conditions. J. Investig. Dermatol. 2014, 134, 1527–1534. [Google Scholar] [CrossRef] [Green Version]
- Melnik, B.; Wenchieh, C. Acne and Rosacea. In Braun-Falco’s Dermatology, 4th ed.; Plewig, G., French, L., Ruzicka, T., Kaufmann, R., Hertl, M., Eds.; Springer: Berlin/Heidelberg, Germany, 2022; pp. 1291–1324. [Google Scholar]
- MeSH Browser. Available online: https://meshb.nlm.nih.gov/record/ui?ui=D017486 (accessed on 10 April 2023).
- Cheung, M.J.; Taher, M.; Lauzon, G.J. Acneiform facial eruptions: A problem for young women. Can. Fam. Physician 2005, 51, 527–533. [Google Scholar]
- Kuflik, J.H. Acneiform Eruptions: Practice Essentials. Available online: https://emedicine.medscape.com/article/1072536-differential (accessed on 10 April 2023).
- Thiboutot, D.; Zaenglein, A.L. Pathogenesis, Clinical Manifestations, and Diagnosis of Acne Vulgaris. Available online: https://www.uptodate.com/contents/pathogenesis-clinical-manifestations-and-diagnosis-of-acne-vulgaris (accessed on 10 April 2023).
- Dessinioti, C.; Antoniou, C.; Katsambas, A. Acneiform Eruptions. Clin. Dermatol. 2014, 32, 24–34. [Google Scholar] [CrossRef]
- Alia, E.; Feng, H. Rosacea Pathogenesis, Common Triggers, and Dietary Role: The Cause, the Trigger, and the Positive Effects of Different Foods. Clin. Dermatol. 2021, 40, 122–127. [Google Scholar] [CrossRef]
- Marson, J.W.; Baldwin, H.E. Rosacea: A Wholistic Review and Update from Pathogenesis to Diagnosis and Therapy. Int. J. Dermatol. 2019, 59, e175–e182. [Google Scholar] [CrossRef]
- Ahn, C.S.; Huang, W.W. Rosacea Pathogenesis. Dermatol. Clin. 2018, 36, 81–86. [Google Scholar] [CrossRef]
- Kim, H.S. Microbiota in Rosacea. Am. J. Clin. Dermatol. 2020, 21 (Suppl. S1), 25–35. [Google Scholar] [CrossRef]
- Ferček, I.; Lugović-Mihić, L.; Tambić-Andrašević, A.; Ćesić, D.; Grginić, A.G.; Bešlić, I.; Mravak-Stipetić, M.; Mihatov-Štefanović, I.; Buntić, A.-M.; Čivljak, R. Features of the Skin Microbiota in Common Inflammatory Skin Diseases. Life 2021, 11, 962. [Google Scholar] [CrossRef] [PubMed]
- Picardo, M.; Eichenfield, L.F.; Tan, J. Acne and Rosacea. Dermatol. Ther. 2017, 7 (Suppl. S1), 43–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Tang, K.; Wang, Y.; Fang, R.; Sun, Q. Rosacea Treatment: Review and Update. Dermatol. Ther. 2021, 11, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Parać, E. Acneiform Eruptions. Diploma Thesis, University of Zagreb, School of Medicine, Zagreb, Croatia, 2022. Available online: https://urn.nsk.hr/urn:nbn:hr:105:662849 (accessed on 7 May 2023).
- Yun, C.H.; Yun, J.H.; Baek, J.O.; Roh, J.Y.; Lee, J.R. Demodex Mite Density Determinations by Standardized Skin Surface Biopsy and Direct Microscopic Examination and Their Relations with Clinical Types and Distribution Patterns. Ann. Dermatol. 2017, 29, 137–142. [Google Scholar] [CrossRef] [Green Version]
- Rather, P.; Hassan, I. Human Demodex Mite: The Versatile Mite of Dermatological Importance. Indian. J. Dermatol. 2014, 59, 60. [Google Scholar] [CrossRef]
- Yüksel, S.; Pancar Yüksel, E. Increased Demodex Density in Patients Hospitalized for Worsening Heart Failure. J. Pers. Med. 2020, 10, 39. [Google Scholar] [CrossRef]
- Bendezu-Quispe, G.; Rojas-Zevallos, J.; Rosales-Rimache, J. Type 2 Diabetes Mellitus and Demodex folliculorum Infestation: A Cross-Sectional Study in Peruvian Patients. Int. J. Environ. Res. Public Health 2022, 19, 13582. [Google Scholar] [CrossRef]
- Toka Özer, T.; Akyürek, Ö.; Durmaz, S. Association between Demodex folliculorum and Metabolic Syndrome. J. Cosmet. Dermatol. 2020, 19, 3145–3149. [Google Scholar] [CrossRef]
- Paichitrojjana, A. Demodex: The Worst Enemies Are the Ones That Used to Be Friends. Dermatol. Rep. 2022, 14, 9339. [Google Scholar] [CrossRef]
- Paichitrojjana, A. Demodicosis Imitating Acne Vulgaris: A Case Report. Clin. Cosmet. Investig. Dermatol. 2022, 15, 497–501. [Google Scholar] [CrossRef]
- Li, J.; Wei, E.; Reisinger, A.; French, L.E.; Clanner-Engelshofen, B.M.; Reinholz, M. Comparison of Different Anti-Demodex Strategies: A Systematic Review and Meta-Analysis. Dermatology 2023, 239, 12–31. [Google Scholar] [CrossRef] [PubMed]
- Mokos, Z.B.; Kummer, A.; Mosler, E.L.; Čeović, R.; Basta-Juzbašić, A. Perioral dermatitis: Still a therapeutic challenge. Acta Clin. Croat. 2015, 54, 179–185. [Google Scholar] [PubMed]
- Searle, T.; Ali, F.R.; Al-Niaimi, F. Perioral Dermatitis: Diagnosis, Proposed Etiologies, and Management. J. Cosmet. Dermatol. 2021, 20, 3839–3848. [Google Scholar] [CrossRef]
- Lugović-Mihić, L.; Špiljak, B.; Blagec, T.; Delaš Aždajić, M.; Franceschi, N.; Gašić, A.; Parać, E. Factors Participating in the Occurrence of Inflammation of the Lips (Cheilitis) and Perioral Skin. Cosmetics 2023, 10, 9. [Google Scholar] [CrossRef]
- Nikolakis, G.; Kokolakis, G.; Kaleta, K.; Wolk, K.; Hunger, R.; Sabat, R.; Zouboulis, C.C. Pathogenese der Hidradenitis Suppurativa/Acne Inversa. Hautarzt 2021, 72, 658–665. [Google Scholar] [CrossRef]
- Goldburg, S.R.; Strober, B.E.; Payette, M.J. Hidradenitis Suppurativa. J. Am. Acad. Dermatol. 2020, 82, 1045–1058. [Google Scholar] [CrossRef]
- Pescitelli, L.; Ricceri, F.; Prignano, F. Hidradenitis Suppurativa and Associated Diseases. G. Ital. Dermatol. Venereol. 2018, 153 (Suppl. S2), 8–17. [Google Scholar] [CrossRef] [PubMed]
- Frings, V.G.; Bauer, B.; Glöditzsch, M.; Goebeler, M.; Presser, D. Assessing the psychological burden of patients with hidradenitis suppurativa. Eur. J. Dermatol. 2019, 29, 294–301. [Google Scholar]
- Wieczorek, M.; Walecka, I. Hidradenitis Suppurativa—Known and Unknown Disease. Reumatologia 2018, 56, 337–339. [Google Scholar] [CrossRef] [Green Version]
- Seyed Jafari, S.M.; Hunger, R.E.; Schlapbach, C. Hidradenitis Suppurativa: Current Understanding of Pathogenic Mechanisms and Suggestion for Treatment Algorithm. Front. Med. 2020, 7, 68. [Google Scholar] [CrossRef] [Green Version]
- Ogunbiyi, A. Pseudofolliculitis Barbae; Current Treatment Options. Clin. Cosmet. Investig. Dermatol. 2019, 12, 241–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, B.G.; Goldstein, A.O. Pseudofolliculitis Barbae; Post, T.W., Ed.; UpToDate: Waltham, MA, USA, 2022. [Google Scholar]
- Kelly, A.P. Pseudofolliculitis Barbae and Acne Keloidalis Nuchae. Dermatol. Clin. 2003, 21, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Dalia, Y.; Khatib, J.; Odens, H.; Patel, T. A Review of Treatments of Pseudofolliculitis Barbae. Clin. Exp. Dermatol. 2023, 48, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Ribera, M.; Fernández-Chico, N.; Casals, M. Pseudofoliculitis de la barba [Pseudofolliculitis barbae]. Actas Dermo-Sifiliográficas 2010, 101, 749–757. [Google Scholar] [CrossRef]
- Katoh, M.; Nomura, T.; Miyachi, Y.; Kabashima, K. Eosinophilic Pustular Folliculitis: A Review of the Japanese Published Works. J. Dermatol. 2012, 40, 15–20. [Google Scholar] [CrossRef]
- Nomura, T.; Katoh, M.; Yamamoto, Y.; Miyachi, Y.; Kabashima, K. Eosinophilic Pustular Folliculitis: A Proposal of Diagnostic and Therapeutic Algorithms. J. Dermatol. 2016, 43, 1301–1306. [Google Scholar] [CrossRef] [Green Version]
- Nervi, S.J.; Schwartz, R.A.; Dmochowski, M. Eosinophilic Pustular Folliculitis: A 40 Year Retrospect. J. Am. Acad. Dermatol. 2006, 55, 285–289. [Google Scholar] [CrossRef]
- Sève, P.; Pacheco, Y.; Durupt, F.; Jamilloux, Y.; Gerfaud-Valentin, M.; Isaac, S.; Boussel, L.; Calender, A.; Androdias, G.; Valeyre, D.; et al. Sarcoidosis: A Clinical Overview from Symptoms to Diagnosis. Cells 2021, 10, 766. [Google Scholar] [CrossRef]
- Caplan, A.; Rosenbach, M.; Imadojemu, S. Cutaneous Sarcoidosis. Semin. Respir. Crit. Care Med. 2020, 41, 689–699. [Google Scholar] [CrossRef]
- Zeichner, J.A. Acneiform Eruptions in Dermatology: A Differential Diagnosis; Springer: New York, NY, USA, 2014. [Google Scholar]
- Schmieder, S.J.; Harper, C.D.; Schmieder, G.J. Granuloma Annulare. Available online: https://www.ncbi.nlm.nih.gov/books/NBK459377/ (accessed on 10 April 2023).
- Joshi, T.P.; Duvic, M. Granuloma Annulare: An Updated Review of Epidemiology, Pathogenesis, and Treatment Options. Am. J. Clin. Dermatol. 2021, 23, 37–50. [Google Scholar] [CrossRef]
- Smith, R. Papular Granuloma Annulare. In Acneiform Eruptions in Dermatology; Zeichner, J., Ed.; Springer: New York, NY, USA, 2014; pp. 375–379. [Google Scholar]
- Xue, J.; Lam, J.M. Granuloma Annulare. Paediatr. Child. Health 2019, 24, 366–367. [Google Scholar] [CrossRef] [PubMed]
- Rubin, C.B.; Rosenbach, M. Granuloma annulare: A retrospective series of 133 patients. Cutis 2019, 103, 102–106. [Google Scholar] [PubMed]
- Wang, J.; Khachemoune, A. Granuloma Annulare: A Focused Review of Therapeutic Options. Am. J. Clin. Dermatol. 2017, 19, 333–344. [Google Scholar] [CrossRef]
- Tambe, S.; Jerajani, H.; Pund, P. Granulomatous Periorificial Dermatitis Effectively Managed with Oral Isotretinoin. Indian Dermatol. Online J. 2018, 9, 68–70. [Google Scholar] [CrossRef]
- Al-Qassabi, A.-M.; Al-Busaidi, K.; Al Baccouche, K.; Al Ismaili, A. Granulomatous Periorificial Dermatitis in an Adult: A Case Report with Review of Literature. Sultan Qaboos Univ. Med. J. 2020, 20, 100–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chintagunta, S.R.; Manchala, S.; Arakkal, G. Granulomatous periorificial dermatitis in an adult: A rare case report. J. Dr. NTR Univ. Health Sci. 2018, 7, 143. [Google Scholar] [CrossRef]
- Fakih, A.; Makhoul, R.; Grozdev, I. Childhood Granulomatous Periorificial Dermatitis: Case Report and Review of the Literature. Dermatol. Online J. 2020, 26, 13030. [Google Scholar] [CrossRef]
- Rodriguez-Garijo, N.; Querol-Cisneros, E.; Tomas-Velazquez, A.; Estenaga, A.; Moreno-Artero, E.; Idoate, M.A.; Paricio, J.J.; España, A. Recalcitrant Granulomatous Periorificial Dermatitis with Good Response to Low-Dose Oral Isotretinoin. Pediatr. Dermatol. 2019, 36, 980–981. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.S.; Lin, P.T.; Tsai, Y.S.; Wang, S.H.; Chi, C.C. Interventions for bacterial folliculitis and boils (furuncles and carbuncles). Cochrane Database Syst. Rev. 2021, 2, CD013099. [Google Scholar] [CrossRef]
- Lugović-Mihić, L.; Barisić, F.; Bulat, V.; Buljan, M.; Situm, M.; Bradić, L.; Mihić, J. Differential diagnosis of the scalp hair folliculitis. Acta Clin. Croat 2011, 50, 395–402. [Google Scholar]
- Laureano, A.C.; Schwartz, R.A.; Cohen, P.J. Facial Bacterial Infections: Folliculitis. Clin. Dermatol. 2014, 32, 711–714. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, H.S.; Nopper, A.J. Superficial Bacterial Skin Infections and Cellulitis. In Principles and Practice of Pediatric Infectious Diseases, 5th ed.; Long, S.S., Prober, C.G., Fischer, M., Eds.; Elsevier—Health Sciences Division: Philadelphia, PA, USA, 2018; pp. 436–444. [Google Scholar]
- Plewig, G.; Jansen, T. Acneiform Dermatoses. Dermatology 1998, 196, 102–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Böni, R.; Nehrhoff, B. Treatment of Gram-Negative Folliculitis in Patients with Acne. Am. J. Clin. Dermatol. 2003, 4, 273–276. [Google Scholar] [PubMed]
- Vlachos, C.; Henning, M.A.S.; Gaitanis, G.; Faergemann, J.; Saunte, D.M. Critical Synthesis of Available Data in Malassezia Folliculitis and a Systematic Review of Treatments. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1672–1683. [Google Scholar] [CrossRef]
- Rubenstein, R.M.; Malerich, S.A. Malassezia (Pityrosporum) Folliculitis. J. Clin. Aesthetic Dermatol. 2014, 7, 37–41. [Google Scholar]
- Saunte, D.M.L.; Gaitanis, G.; Hay, R.J. Malassezia-Associated Skin Diseases, the Use of Diagnostics and Treatment. Front. Cell. Infect. 2020, 10, 112. [Google Scholar] [CrossRef]
- Malgotra, V.; Singh, H. Malassezia (Pityrosporum) Folliculitis Masquerading as Recalcitrant Acne. Cureus 2021, 13, e13534. [Google Scholar] [CrossRef]
- Spernovasilis, N.; Psichogiou, M.; Poulakou, G. Skin Manifestations of Pseudomonas aeruginosa Infections. Curr. Opin. Infect. Dis. 2021, 34, 72–79. [Google Scholar] [CrossRef]
- Ratnam, S.; Hogan, K.; March, S.B.; Butler, R.W. Whirlpool-Associated Folliculitis Caused by Pseudomonas aeruginosa: Report of an Outbreak and Review. J. Clin. Microbiol. 1986, 23, 655–659. [Google Scholar] [CrossRef] [Green Version]
- Toner, C.B. Pseudomonas Folliculitis; Elston, D.M., Ed.; Medscape: New York, NY, USA, 2020. [Google Scholar]
- Revanker, S.G. Sporotrichosis—Infectious Diseases. Available online: https://www.msdmanuals.com/professional/infectious-diseases/fungi/sporotrichosis (accessed on 10 April 2023).
- Sizar, O.; Talati, R. Sporotrichosis. Available online: https://www.ncbi.nlm.nih.gov/books/NBK532255 (accessed on 10 April 2023).
- Mahlberg, M.J.; Patel, R.; Rosenman, K.; Cheung, W.; Wang, N.; Sanchez, M. Fixed Cutaneous Sporotrichosis. Dermatol. Online J. 2009, 15, 5. [Google Scholar] [CrossRef]
- Kusuhara, M.; Hachisuka, H.; Sasai, Y. Statistical Survey of 150 Cases with Sporotrichosis. Mycopathologia 1988, 102, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Garcia, S.C.G.; Alanis, J.C.S.; Flores, M.G.; Gonzalez, S.E.G.; Cabrera, L.V.; Candiani, J.O. Coccidioidomycosis and the Skin: A Comprehensive Review. An. Bras. Dermatol. 2015, 90, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Ocampo-Garza, J.; Castrejón-Pérez, A.D.; Gonzalez-Saldivar, G.; Ocampo-Candiani, J. Cutaneous Coccidioidomycosis: A Great Mimicker. BMJ Case Rep. 2015, 2015, bcr2015211680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambert, W.C.; Bagley, M.P.; Khan, Y.; Schwartz, R.A. Pustular acneiform secondary syphilis. Cutis 1986, 37, 69–70. [Google Scholar] [PubMed]
- Harden, D. Papular and Nodular Lesions of the Scalp, Face, and Neck. Arch. Dermatol. 1997, 133, 1027. [Google Scholar] [CrossRef] [PubMed]
- Blaess, M.; Kaiser, L.; Sommerfeld, O.; Csuk, R.; Deigner, H.-P. Drug Triggered Pruritus, Rash, Papules, and Blisters—Is AGEP a Clash of an Altered Sphingolipid-Metabolism and Lysosomotropism of Drugs Accumulating in the Skin? Lipids Health Dis. 2021, 20, 156. [Google Scholar] [CrossRef] [PubMed]
- Hjorth, N.; Sjolin, K.E.; Sylvest, B.; Thomsen, K. Acne Aestivalis--Mallorca Acne. Acta Derm. Venereol. 1972, 52, 61–63. [Google Scholar] [CrossRef]
- Jones, C.; Bleehen, S.S. Acne Induced by PUVA Treatment. BMJ 1977, 2, 866. [Google Scholar] [CrossRef] [Green Version]
- Mazhar, M.; Simpson, M.; Marathe, K. Inner Thigh Friction as a Cause of Acne Mechanica. Pediatr. Dermatol. 2019, 36, 546–547. [Google Scholar] [CrossRef]
- Freiman, A. Sports Dermatology Part 1: Common Dermatoses. CMAJ 2004, 171, 851–853. [Google Scholar] [CrossRef] [Green Version]
- Kirkland, R.; Adams, B.B. Dermatological Problems in the Football Player. Int. J. Dermatol. 2006, 45, 927–932. [Google Scholar] [CrossRef] [PubMed]
- Knierim, C.; Goertz, W.; Reifenberger, J.; Homey, B.; Meller, S. Geigerknoten. Hautarzt 2013, 64, 724–726. [Google Scholar] [CrossRef]
- Kligman, A.M. Acne Cosmetica. Arch. Dermatol. 1972, 106, 843–850. [Google Scholar] [CrossRef] [PubMed]
- Plewig, G. Pomade Acne. Arch. Dermatol. 1970, 101, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Martin, W.M.C.; Bardsley, A.F. The Comedo Skin Reaction to Radiotherapy. Br. J. Radiol. 2002, 75, 478–481. [Google Scholar] [CrossRef] [PubMed]
- Hubiche, T.; Sibaud, V. Localized Acne Induced by Radiation Therapy. Dermatol. Online J. 2014, 20, 21545. [Google Scholar] [CrossRef]
- Paganelli, A.; Mandel, V.D.; Kaleci, S.; Pellacani, G.; Rossi, E. Favre–Racouchot Disease: Systematic Review and Possible Therapeutic Strategies. J. Eur. Acad. Dermatol. Venereol. 2018, 33, 32–41. [Google Scholar] [CrossRef] [Green Version]
- Sonthalia, S.; Arora, R.; Chhabra, N.; Khopkar, U. Favre-Racouchot Syndrome. Indian Dermatol. Online J. 2014, 5, 128. [Google Scholar] [CrossRef]
- Platsidaki, E.; Markantoni, V.; Balamoti, E.; Kouris, A.; Rigopoulos, D.; Kontochristopoulos, G. Combination of 30% Salicylic Acid Peels and Mechanical Comedo Extraction for the Treatment of Favre-Racouchot Syndrome. Acta Dermatovenerol. Croat. 2019, 27, 42–43. [Google Scholar]
- Schlessinger, D.I.; Robinson, C.A.; Schlessinger, J. Chloracne. Available online: https://www.ncbi.nlm.nih.gov/books/NBK459189/ (accessed on 10 April 2023).
- Dyall-Smith, D. Halogenoderma. Available online: https://dermnetnz.org/topics/halogenoderma (accessed on 18 May 2023).
- Ju, Q.; Zouboulis, C.C.; Xia, L. Environmental Pollution and Acne-Chloracne. Dermato-Endocrinology 2009, 1, 125–128. [Google Scholar] [CrossRef] [Green Version]
- Eskenazi, B.; Warner, M.; Brambilla, P.; Signorini, S.; Ames, J.; Mocarelli, P. The Seveso accident: A look at 40 years of health research and beyond. Environ. Int. 2018, 121 Pt 1, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Onozuka, D.; Nakamura, Y.; Tsuji, G.; Furue, M. Mortality in Yusho Patients Exposed to Polychlorinated Biphenyls and Polychlorinated Dibenzofurans: A 50-Year Retrospective Cohort Study. Environ. Health 2020, 19, 119. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, D.O. Polychlorinated Biphenyls (PCBs): Routes of Exposure and Effects on Human Health. Rev. Environ. Health 2006, 21, 1–24. [Google Scholar] [CrossRef]
- Pelclová, D.; Urban, P.; Preiss, J.; Lukáš, E.; Fenclová, Z.; Navrátil, T.; Dubská, Z.; Senholdová, Z. Adverse Health Effects in Humans Exposed to 2,3,7,8-Tetrachlorodibenzo-p-Dioxin (TCDD). Rev. Environ. Health 2006, 21, 119–138. [Google Scholar] [CrossRef] [PubMed]
- Demir, B.; Cicek, D. Occupational Acne. In Acne and Acneiform Eruptions; Kartal, S.P., Gönül, M., Eds.; IntechOpen: London, UK, 2017; pp. 53–67. [Google Scholar]
- Tindall, J.P. Chloracne and Chloracnegens. J. Am. Acad. Dermatol. 1985, 13, 539–558. [Google Scholar] [CrossRef]
- Panteleyev, A.A.; Bickers, D.R. Dioxin-Induced Chloracne—Reconstructing the Cellular and Molecular Mechanisms of a Classic Environmental Disease. Exp. Dermatol. 2006, 15, 705–730. [Google Scholar] [CrossRef] [PubMed]
- Kokelj, F. Occupational Acne. Clin. Dermatol. 1992, 10, 213–217. [Google Scholar] [CrossRef]
- Moustafa, G.-A.; Xanthopoulou, E.; Riza, E.; Linos, A. Skin Disease after Occupational Dermal Exposure to Coal Tar: A Review of the Scientific Literature. Int. J. Dermatol. 2015, 54, 868–879. [Google Scholar] [CrossRef]
- Zorba, E.; Karpouzis, A.; Zorbas, A.; Bazas, T.; Zorbas, S.; Alexopoulos, E.; Zorbas, I.; Kouskoukis, K.; Konstandinidis, T. Occupational Dermatoses by Type of Work in Greece. Saf. Health Work 2013, 4, 142–148. [Google Scholar] [CrossRef] [Green Version]
- Brunner, M.J.; Riddell, J.M., Jr.; Best, W.R. Cutaneous side effects of ACTH cortisone and pregnenolone therapy. J. Investig. Dermatol. 1951, 16, 205–210. [Google Scholar] [CrossRef] [Green Version]
- Hurwitz, R.M. Steroid acne. J. Am. Acad. Dermatol. 1989, 21, 1179–1181. [Google Scholar] [CrossRef] [PubMed]
- Gloor, M.; Mildenberger, K.H. On the influence of an external therapy with dexamethasone-21-sodium-m-sulfobenzoate on the amount of free fatty acids in the skin surface lipids. Arch. Dermatol. Res. 1978, 261, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Do, H.K.; Ezra, N.; Wolverton, S.E. Drug-Induced Acneiform Eruptions. In Acneiform Eruptions in Dermatology; Zeichner, J., Ed.; Springer: New York, NY, USA, 2014; pp. 389–404. [Google Scholar]
- Ayati, A.; Moghimi, S.; Salarinejad, S.; Safavi, M.; Pouramiri, B.; Foroumadi, A. A Review on Progression of Epidermal Growth Factor Receptor (EGFR) Inhibitors as an Efficient Approach in Cancer Targeted Therapy. Bioorg. Chem. 2020, 99, 103811. [Google Scholar] [CrossRef] [PubMed]
- Segaert, S.; Van Cutsem, E. Clinical Signs, Pathophysiology and Management of Skin Toxicity during Therapy with Epidermal Growth Factor Receptor Inhibitors. Ann. Oncol. 2005, 16, 1425–1433. [Google Scholar] [CrossRef]
- Fabbrocini, G.; Panariello, L.; Caro, G.; Cacciapuoti, S. Acneiform Rash Induced by EGFR Inhibitors: Review of the Literature and New Insights. Ski. Appendage Disord. 2015, 1, 31–37. [Google Scholar] [CrossRef] [Green Version]
- Gorji, M.; Joseph, J.; Pavlakis, N.; Smith, S.D. Prevention and Management of Acneiform Rash Associated with EGFR Inhibitor Therapy: A Systematic Review and Meta-Analysis. Asia-Pac. J. Clin. Oncol. 2022, 18, 526–539. [Google Scholar] [CrossRef]
- Potthoff, K.; Hofheinz, R.; Hassel, J.C.; Volkenandt, M.; Lordick, F.; Hartmann, J.T.; Karthaus, M.; Riess, H.; Lipp, H.P.; Hauschild, A.; et al. Interdisciplinary Management of EGFR-Inhibitor-Induced Skin Reactions: A German Expert Opinion. Ann. Oncol. 2011, 22, 524–535. [Google Scholar] [CrossRef]
- Beech, J.; Germetaki, T.; Judge, M.; Paton, N.; Collins, J.; Garbutt, A.; Braun, M.; Fenwick, J.; Saunders, M.P. Management and Grading of EGFR Inhibitor-Induced Cutaneous Toxicity. Future Oncol. 2018, 14, 2531–2541. [Google Scholar] [CrossRef] [Green Version]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parać, E.; Špiljak, B.; Lugović-Mihić, L.; Bukvić Mokos, Z. Acne-like Eruptions: Disease Features and Differential Diagnosis. Cosmetics 2023, 10, 89. https://doi.org/10.3390/cosmetics10030089
Parać E, Špiljak B, Lugović-Mihić L, Bukvić Mokos Z. Acne-like Eruptions: Disease Features and Differential Diagnosis. Cosmetics. 2023; 10(3):89. https://doi.org/10.3390/cosmetics10030089
Chicago/Turabian StyleParać, Ena, Bruno Špiljak, Liborija Lugović-Mihić, and Zrinka Bukvić Mokos. 2023. "Acne-like Eruptions: Disease Features and Differential Diagnosis" Cosmetics 10, no. 3: 89. https://doi.org/10.3390/cosmetics10030089