
Maternal Cardiovascular Responses to Position Change in Pregnancy
 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Review of Physiological Assessments of Maternal and Fetal Impacts of Pregnancy and Position
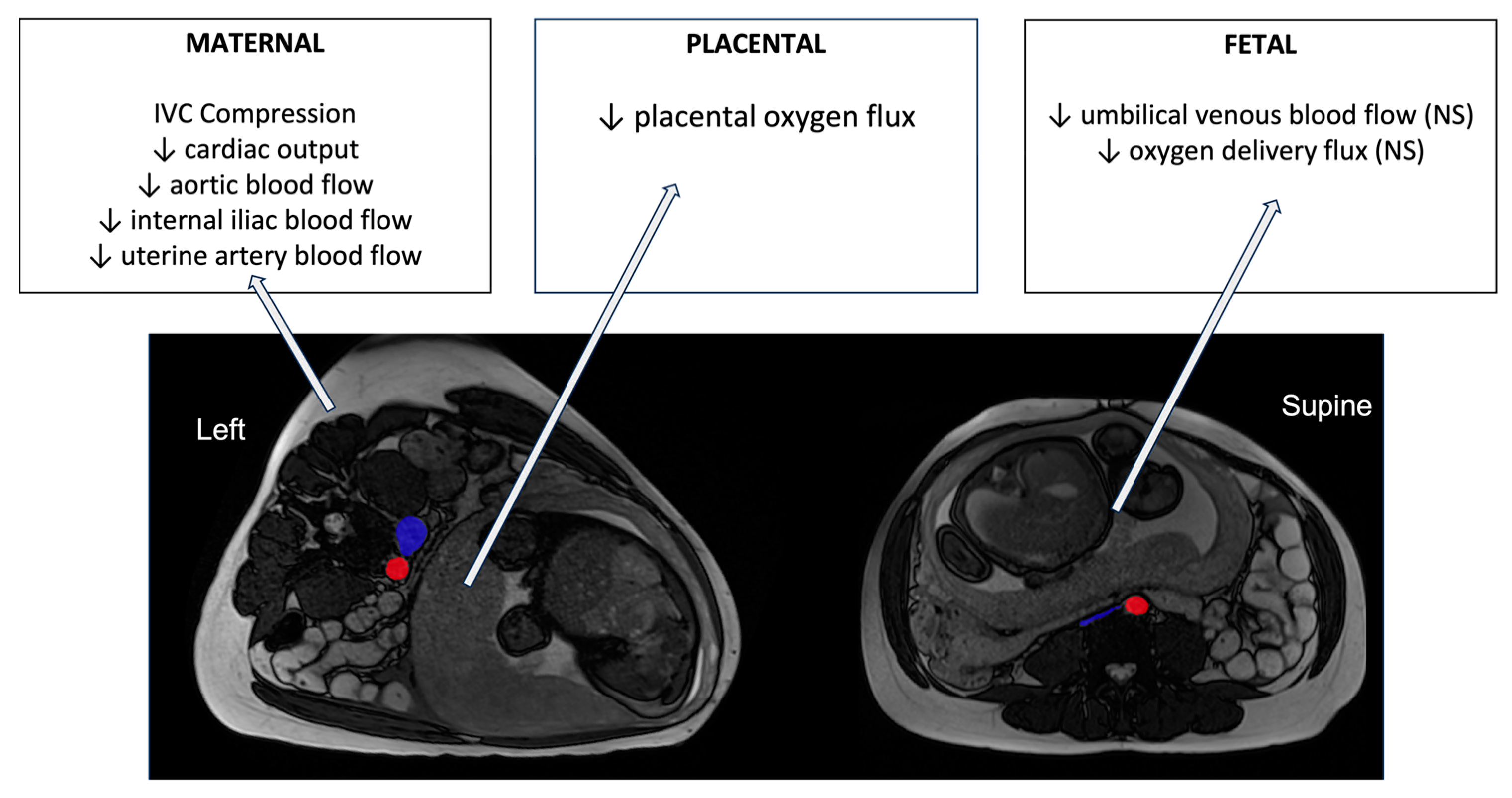
5.1. Maternal
5.2. Utero-Placental Adaption
5.3. Feto-Placental and Fetal Circulation
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hug, L.; You, D.; Blencowe, H.; Mishra, A.; Wang, Z.; Fix, M.J.; Wakefield, J.; Moran, A.C.; Gaigbe-Togbe, V.; Suzuki, E.; et al. Global, regional, and national estimates and trends in stillbirths from 2000 to 2019: A systematic assessment. Lancet 2021, 398, 772–785. [Google Scholar] [CrossRef] [PubMed]
- Heazell, A.E.P.; Siassakos, D.; Blencowe, H.; Burden, C.; Bhutta, Z.A.; Cacciatore, J.; Dang, N.; Das, J.; Flenady, V.; Gold, K.J.; et al. Stillbirths: Economic and psychosocial consequences. Lancet 2016, 387, 604–616. [Google Scholar] [CrossRef] [PubMed]
- King, V.J.; Bennet, L.; Stone, P.R.; Clark, A.; Gunn, A.J.; Dhillon, S.K. Fetal growth restriction and stillbirth: Biomarkers for identifying at risk fetuses. Front. Physiol. 2022, 13, 959750. [Google Scholar] [CrossRef] [PubMed]
- Redline, R.W.; Roberts, D.J.; Parast, M.M.; Ernst, L.M.; Morgan, T.K.; Greene, M.F.; Gyamfi-Bannerman, C.; Louis, J.M.; Maltepe, E.; Mestan, K.K.; et al. Placental pathology is necessary to understand common pregnancy complications and achieve an improved taxonomy of obstetrical disease. Am. J. Obs. Gynecol. 2023, 228, 187–202. [Google Scholar] [CrossRef]
- Ptacek, I.; Sebire, N.J.; Man, J.A.; Brownbill, P.; Heazell, A.E. Systematic review of placental pathology reported in association with stillbirth. Placenta 2014, 35, 552–562. [Google Scholar] [CrossRef]
- Gordijn, S.J.; Beune, I.M.; Thilaganathan, B.; Papageorghiou, A.; Baschat, A.A.; Baker, P.N.; Silver, R.M.; Wynia, K.; Ganzevoort, W. Consensus definition of fetal growth restriction: A Delphi procedure. Ultrasound Obs. Gynecol. 2016, 48, 333–339. [Google Scholar] [CrossRef]
- Cronin, R.S.; Li, M.; Thompson, J.M.D.; Gordon, A.; Raynes-Greenow, C.H.; Heazell, A.E.P.; Stacey, T.; Culling, V.M.; Bowring, V.; Anderson, N.H.; et al. An Individual Participant Data Meta-analysis of Maternal Going-to-Sleep Position, Interactions with Fetal Vulnerability, and the Risk of Late Stillbirth. EClinicalMedicine 2019, 10, 49–57. [Google Scholar] [CrossRef]
- Pacora, P.; Romero, R.; Jaiman, S.; Erez, O.; Bhatti, G.; Panaitescu, B.; Benshalom-Tirosh, N.; Jung, E.J.; Hsu, C.D.; Hassan, S.S.; et al. Mechanisms of death in structurally normal stillbirths. J. Perinat. Med. 2019, 47, 222–240. [Google Scholar] [CrossRef]
- Goldenberg, R.L.; Harrison, M.S.; McClure, E.M. Stillbirths: The Hidden Birth Asphyxia—US and Global Perspectives. Clin. Perinatol. 2016, 43, 439–453. [Google Scholar] [CrossRef]
- Burton, G.J.; Jauniaux, E. Pathophysiology of placental-derived fetal growth restriction. Am. J. Obstet. Gynecol. 2018, 218, S745–S761. [Google Scholar] [CrossRef]
- Brown, N.T.; Turner, J.M.; Kumar, S. The intrapartum and perinatal risks of sleep-disordered breathing in pregnancy: A systematic review and metaanalysis. Am. J. Obs. Gynecol. 2018, 219, 147–161.e141. [Google Scholar] [CrossRef] [PubMed]
- Warland, J.; McCutcheon, H.; Baghurst, P. Maternal blood pressure in pregnancy and stillbirth: A case-control study of third-trimester stillbirth. Am. J. Perinatol. 2008, 25, 311–317. [Google Scholar] [CrossRef]
- Friedman, E.A.; Neff, R.K. Hypertension-hypotension in pregnancy. Correlation with fetal outcome. JAMA 1978, 239, 2249–2251. [Google Scholar] [CrossRef] [PubMed]
- Humphries, A.; Mirjalili, S.A.; Tarr, G.P.; Thompson, J.M.D.; Stone, P. The effect of supine positioning on maternal hemodynamics during late pregnancy. J. Matern. Fetal Neonatal Med. 2019, 32, 3923–3930. [Google Scholar] [CrossRef] [PubMed]
- Stone, P.R.; Burgess, W.; McIntyre, J.P.; Gunn, A.J.; Lear, C.A.; Bennet, L.; Mitchell, E.A.; Thompson, J.M.; Maternal Sleep In Pregnancy Research Group, T.U.o.A. Effect of maternal position on fetal behavioural state and heart rate variability in healthy late gestation pregnancy. J. Physiol. 2017, 595, 1213–1221. [Google Scholar] [CrossRef] [PubMed]
- Howard, B.K.; Goodson, J.H.; Mengert, W.F. Supine hypotensive syndrome in late pregnancy. Obs. Gynecol. 1953, 1, 371–377. [Google Scholar]
- Rajendra Acharya, U.; Paul Joseph, K.; Kannathal, N.; Lim, C.M.; Suri, J.S. Heart rate variability: A review. Med. Biol. Eng. Comput. 2006, 44, 1031–1051. [Google Scholar] [CrossRef]
- Billman, G.E. Heart rate variability—A historical perspective. Front. Physiol. 2011, 2, 86. [Google Scholar] [CrossRef]
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef]
- Grossman, P.; Taylor, E.W. Toward understanding respiratory sinus arrhythmia: Relations to cardiac vagal tone, evolution and biobehavioral functions. Biol. Psychol. 2007, 74, 263–285. [Google Scholar] [CrossRef]
- Kinsella, S.M. Effect of blood pressure instrument and cuff side on blood pressure reading in pregnant women in the lateral recumbent position. Int. J. Obs. Anesth. 2006, 15, 290–293. [Google Scholar] [CrossRef] [PubMed]
- Wieling, W.; Karemaker, J. Measurement of heart rate and blood pressure to evaluate disturbances in neurocardiovascular control. In Autonomic Failure: A Textbook of Clinical Disorders of the Autonomic Nervous System, 5th ed.; Mathias, C., Bannister, R., Eds.; Oxford University Press: Oxford, UK, 2012; pp. 290–306. [Google Scholar]
- Shaffer, F.; McCraty, R.; Zerr, C.L. A healthy heart is not a metronome: An integrative review of the heart’s anatomy and heart rate variability. Front. Psychol. 2014, 5, 1040. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed]
- Sassi, R.; Cerutti, S.; Lombardi, F.; Malik, M.; Huikuri, H.V.; Peng, C.K.; Schmidt, G.; Yamamoto, Y. Advances in heart rate variability signal analysis: Joint position statement by the e-Cardiology ESC Working Group and the European Heart Rhythm Association co-endorsed by the Asia Pacific Heart Rhythm Society. Europace 2015, 17, 1341–1353. [Google Scholar] [CrossRef] [PubMed]
- Richman, J.S. Sample Entropy Statistics and Testing for Order in Complex Physiological Signals. Commun. Stat.—Theory Methods 2007, 36, 1005–1019. [Google Scholar] [CrossRef]
- Mahendru, A.A.; Everett, T.R.; Wilkinson, I.B.; Lees, C.C.; McEniery, C.M. A longitudinal study of maternal cardiovascular function from preconception to the postpartum period. J. Hypertens. 2014, 32, 849–856. [Google Scholar] [CrossRef]
- Chapman, A.B.; Abraham, W.T.; Zamudio, S.; Coffin, C.; Merouani, A.; Young, D.; Johnson, A.; Osorio, F.; Goldberg, C.; Moore, L.G.; et al. Temporal relationships between hormonal and hemodynamic changes in early human pregnancy. Kidney Int. 1998, 54, 2056–2063. [Google Scholar] [CrossRef]
- Spaanderman, M.E.; Willekes, C.; Hoeks, A.P.; Ekhart, T.H.; Peeters, L.L. The effect of pregnancy on the compliance of large arteries and veins in healthy parous control subjects and women with a history of preeclampsia. Am. J. Obs. Gynecol. 2000, 183, 1278–1286. [Google Scholar] [CrossRef]
- D’Souza, A.W.; Hissen, S.L.; Okada, Y.; Jarvis, S.S.; Washio, T.; Akins, J.D.; Nelson, D.B.; Fu, Q. Differential regulation of sympathetic neural burst frequency and amplitude throughout normal pregnancy: A longitudinal study. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2023, 324, R249–R259. [Google Scholar] [CrossRef]
- Schneider, K.T.; Bollinger, A.; Huch, A.; Huch, R. The oscillating ‘vena cava syndrome’ during quiet standing--an unexpected observation in late pregnancy. Br. J. Obs. Gynaecol. 1984, 91, 766–771. [Google Scholar] [CrossRef]
- Schneider, K.T.; Deckardt, R. The implication of upright posture on pregnancy. J. Perinat. Med. 1991, 19, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Fu, Q.; Witkowski, S.; Levine, B.D. Vasoconstrictor reserve and sympathetic neural control of orthostasis. Circulation 2004, 110, 2931–2937. [Google Scholar] [CrossRef] [PubMed]
- Hayano, J.; Sakakibara, Y.; Yamada, A.; Yamada, M.; Mukai, S.; Fujinami, T.; Yokoyama, K.; Watanabe, Y.; Takata, K. Accuracy of assessment of cardiac vagal tone by heart rate variability in normal subjects. Am. J. Cardiol. 1991, 67, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Perkiomaki, J.S.; Zareba, W.; Badilini, F.; Moss, A.J. Influence of atropine on fractal and complexity measures of heart rate variability. Ann. Noninvasive Electrocardiol. 2002, 7, 326–331. [Google Scholar] [CrossRef]
- Blake, M.J.; Martin, A.; Manktelow, B.N.; Armstrong, C.; Halligan, A.W.; Panerai, R.B.; Potter, J.F. Changes in baroreceptor sensitivity for heart rate during normotensive pregnancy and the puerperium. Clin. Sci. 2000, 98, 259–268. [Google Scholar] [CrossRef]
- Murphy, M.S.; Seaborn, G.E.; Redfearn, D.P.; Smith, G.N. Reduced Heart Rate Variability and Altered Cardiac Conduction after Pre-Eclampsia. PLoS ONE 2015, 10, e0138664. [Google Scholar] [CrossRef]
- Reyes, L.M.; Usselman, C.W.; Davenport, M.H.; Steinback, C.D. Sympathetic Nervous System Regulation in Human Normotensive and Hypertensive Pregnancies. Hypertension 2018, 71, 793–803. [Google Scholar] [CrossRef]
- Mongelli, M.; Benzie, R.; Condous, G. Average fetal weekly weight gain: A novel measure of fetal growth velocity. J. Matern. Fetal Neonatal Med. 2016, 29, 676–679. [Google Scholar] [CrossRef]
- Kerr, M.G.; Scott, D.B.; Samuel, E. Studies of the Inferior Vena Cava in Late Pregnancy. Br. Med. J. 1964, 1, 522, 524–533. [Google Scholar] [CrossRef]
- Scott, D.B. Inferior vena caval occlusion in late pregnancy and its importance in anaesthesia. Br. J. Anaesth. 1968, 40, 120–128. [Google Scholar] [CrossRef]
- Hughes, E.J.; Price, A.N.; McCabe, L.; Hiscocks, S.; Waite, L.; Green, E.; Hutter, J.; Pegoretti, K.; Cordero-Grande, L.; Edwards, A.D.; et al. The effect of maternal position on venous return for pregnant women during MRI. NMR Biomed. 2021, 34, e4475. [Google Scholar] [CrossRef] [PubMed]
- Fujita, N.; Higuchi, H.; Sakuma, S.; Takagi, S.; Latif, M.; Ozaki, M. Effect of Right-Lateral Versus Left-Lateral Tilt Position on Compression of the Inferior Vena Cava in Pregnant Women Determined by Magnetic Resonance Imaging. Anesth. Analg. 2019, 128, 1217–1222. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Cornette, J.; Johnson, M.R.; Karamermer, Y.; Springeling, T.; Opic, P.; Moelker, A.; Krestin, G.P.; Steegers, E.; Roos-Hesselink, J.; et al. Quantitative cardiovascular magnetic resonance in pregnant women: Cross-sectional analysis of physiological parameters throughout pregnancy and the impact of the supine position. J. Cardiovasc. Magn. Reson. 2011, 13, 31. [Google Scholar] [CrossRef] [PubMed]
- Humphries, A.; Mirjalili, S.A.; Tarr, G.P.; Thompson, J.M.D.; Stone, P. Hemodynamic changes in women with symptoms of supine hypotensive syndrome. Acta Obstet. Gynecol. Scand. 2020, 99, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Heldt, T.; Shim, E.B.; Kamm, R.D.; Mark, R.G. Computational modeling of cardiovascular response to orthostatic stress. J. Appl. Physiol. (1985) 2002, 92, 1239–1254. [Google Scholar] [CrossRef]
- Carson, J.; Warrander, L.; Johnstone, E.; van Loon, R. Personalising cardiovascular network models in pregnancy: A two-tiered parameter estimation approach. Int. J. Numer. Method. Biomed. Eng. 2021, 37, e3267. [Google Scholar] [CrossRef]
- Carson, J.; Lewis, M.; Rassi, D.; Van Loon, R. A data-driven model to study utero-ovarian blood flow physiology during pregnancy. Biomech. Model. Mechanobiol. 2019, 18, 1155–1176. [Google Scholar] [CrossRef]
- Assali, N.S.; Douglass, R.A., Jr.; Baird, W.W.; Nicholson, D.B.; Suyemoto, R. Measurement of uterine blood flow and uterine metabolism. IV. Results in normal pregnancy. Am. J. Obs. Gynecol. 1953, 66, 248–253. [Google Scholar] [CrossRef]
- James, J.L.; Chamley, L.W.; Clark, A.R. Feeding your baby in utero: How the uteroplacental circulation impacts pregnancy. Physiology 2017, 32, 234–245. [Google Scholar] [CrossRef]
- Roberts, V.H.J.; Morgan, T.K.; Bednarek, P.; Morita, M.; Burton, G.J.; Lo, J.O.; Frias, A.E. Early first trimester uteroplacental flow and the progressive disintegration of spiral artery plugs: New insights from contrast-enhanced ultrasound and tissue histopathology. Hum. Reprod. 2017, 32, 2382–2393. [Google Scholar] [CrossRef]
- Allerkamp, H.H.; Clark, A.R.; Lee, T.C.; Morgan, T.K.; Burton, G.J.; James, J.L. Something old, something new: Digital quantification of uterine vascular remodelling and trophoblast plugging in historical collections provides new insight into adaptation of the utero-placental circulation. Hum. Reprod. 2021, 36, 571–586. [Google Scholar] [CrossRef] [PubMed]
- Schaaps, J.-P.; Tsatsaris, V.; Goffin, F.; Brichant, J.-F.C.; Delbecque, K.; Tebache, M.; Collignon, L.; Retz, M.C.; Foidart, J.-M. Shunting the intervillous space: New concepts in human uteroplacental vascularization. Am. J. Obstet. Gynecol. 2005, 192, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Couper, S.; Clark, A.; Thompson, J.M.D.; Flouri, D.; Aughwane, R.; David, A.L.; Melbourne, A.; Mirjalili, A.; Stone, P.R. The effects of maternal position, in late gestation pregnancy, on placental blood flow and oxygenation: An MRI study. J. Physiol. 2021, 599, 1901–1915. [Google Scholar] [CrossRef]
- Sussman, D.; Saini, B.S.; Schneiderman, J.E.; Spitzer, R.; Seed, M.; Lye, S.J.; Wells, G.D. Uterine artery and umbilical vein blood flow are unaffected by moderate habitual physical activity during pregnancy. Prenat. Diagn. 2019, 39, 976–985. [Google Scholar] [CrossRef]
- Ducas, R.; Saini, B.S.; Yamamura, K.; Bhagra, C.; Marini, D.; Silversides, C.K.; Roche, S.L.; Colman, J.M.; Kingdom, J.C.; Sermer, M.; et al. Maternal and Fetal Hemodynamic Adaptations to Pregnancy and Clinical Outcomes in Maternal Cardiac Disease. Can. J. Cardiol. 2021, 37, 1942–1950. [Google Scholar] [CrossRef]
- Saini, B.S. Quantifying Placental Function Using Cardiovascular Magnetic Resonance Imaging. In Institute of Medical Science; University of Toronto: Toronto, ON, Cananda, 2021. [Google Scholar]
- Clark, A.R.; James, J.L.; Stevenson, G.N.; Collins, S.L. Understanding abnormal uterine artery Doppler waveforms: A novel computational model to explore potential causes within the utero-placental vasculature. Placenta 2018, 66, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Lear, C.A.; Westgate, J.A.; Ugwumadu, A.; Nijhuis, J.G.; Stone, P.R.; Georgieva, A.; Ikeda, T.; Wassink, G.; Bennet, L.; Gunn, A.J. Understanding Fetal Heart Rate Patterns That May Predict Antenatal and Intrapartum Neural Injury. Semin. Pediatr. Neurol. 2018, 28, 3–16. [Google Scholar] [CrossRef]
- Wilkening, R.B.; Meschia, G. Fetal oxygen uptake, oxygenation, and acid-base balance as a function of uterine blood flow. Am. J. Physiol.-Heart Circ. Physiol. 1983, 244, H749–H755. [Google Scholar] [CrossRef]
- Wilson, D.L.; Fung, A.M.; Skrzypek, H.; Pell, G.; Barnes, M.; Howard, M.E.; Walker, S.P. Maternal sleep behaviours preceding fetal heart rate events on cardiotocography. J. Physiol. 2022, 600, 1791–1806. [Google Scholar] [CrossRef]
- Melbourne, A.; Aughwane, R.; Sokolska, M.; Owen, D.; Kendall, G.; Flouri, D.; Bainbridge, A.; Atkinson, D.; Deprest, J.; Vercauteren, T.; et al. Separating fetal and maternal placenta circulations using multiparametric MRI. Magn. Reson. Med. 2019, 81, 350–361. [Google Scholar] [CrossRef]
- Giussani, D.A. The fetal brain sparing response to hypoxia: Physiological mechanisms. J. Physiol. 2016, 594, 1215–1230. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Control Group (n = 25) | Pregnant Group (n = 63) | ||||
|---|---|---|---|---|---|
| Mean | SD [Range] | Mean | SD [Range] | p-Value | |
| Age (years) | 28 | 4 [21–37] | 32 | 4 [24–41] | <0.001 |
| Height (cm) | 166 | 7 [148–180] | 167 | 8 [148–186] | 0.68 |
| Non-pregnant BMI (kg/m2) | 23 | 3 [17–30] | 23 | 3 [18–30] | 0.68 |
| Gestation at birth (days) | 277 | 7 [260–293] | n/a | ||
| Birthweight (g) | 3497 | 493 [2185–4450] | n/a | ||
| First Left Lateral Position | Nulligravid | Early Pregnancy | Mid-Pregnancy | Late-Pregnancy | Effect of Pregnancy | Effect of Gestation | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (N) | (T1) | (T2) | T3 | Mean Difference (95% CI) | Mean Difference (95% CI) | ||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | T1-N | p | T2-T1 | T3-T1 | p | |
| Heart rate and systolic blood pressure | |||||||||||||
| Mean heart rate (bpm) | 62 | 10 | 66 | 7 | 72 | 7 | 73 | 10 | 3 (−1, 7) | 0.18 | 6 (4, 7) | 8 (6, 9) | <0.001 |
| SBP (mmHg) | 107 | 15 | 99 | 10 | 97 | 11 | 99 | 11 | −8 (−15, −2) | 0.01 | −2 (−6, 1) | 0 (−4, 3) | 0.37 |
| Time domain measures of HRV | |||||||||||||
| RR mean (ms) | 993 | 170 | 921 | 104 | 842 | 80 | 837 | 127 | −63 (−129, 3) | 0.06 | −79 (−99, −59) | −88 (−111, −65) | <0.001 |
| SDNN (ms) | 75 | 38 | 55 | 26 | 46 | 18 | 46 | 25 | −18 (−34, 3) | 0.02 | −9 (−15, −4) | −11 (−16, −5) | 0.001 |
| RMSSD (ms) | 70 | 49 | 52 | 35 | 38 | 24 | 38 | 33 | −15 (−36, 6) | 0.16 | −13 (−22, −5) | −15 (−22, −8) | <0.001 |
| Frequency domain measures of HRV | |||||||||||||
| HF (ln, ms2) | 3.1 | 0.6 | 2.9 | 0.6 | 2.6 | 0.6 | 2.5 | 0.6 | −0.2 (−0.5, 0.1) | 0.19 | −0.3 (−0.4, −0.1) | −0.4 (−0.6, −0.3) | <0.001 |
| HF (nu) | 44 | 21 | 48 | 20 | 42 | 22 | 41 | 22 | 5 (−6, 15) | 0.36 | −4 (−9, 0) | −7 (−12, −2) | 0.02 |
| LF (ln, ms2) | 3 | 0.5 | 2.7 | 0.5 | 2.6 | 0.5 | 2.4 | 0.6 | −0.3 (−0.6, 0.0) | 0.03 | −0.2 (−0.3, −0.1) | −0.4 (−0.5, −0.2) | <0.001 |
| LF (nu) | 35 | 17 | 33 | 16 | 35 | 16 | 31 | 16 | −3 (−11, 6) | 0.55 | 0 (−4, 4) | −3 (−7, 0) | 0.1 |
| Non-linear measures of HRV | |||||||||||||
| Sample entropy | 1.55 | 0.3 | 1.55 | 0.28 | 1.41 | 0.38 | 1.47 | 0.37 | 0 (−0.15, 0.15) | 0.98 | −0.13 (−0.23, −0.02) | −0.07 (−0.16, 0.03) | 0.05 |
| α1 | 0.89 | 0.3 | 0.89 | 0.26 | 0.98 | 0.28 | 1 | 0.33 | 0 (−0.14, 0.14) | 0.99 | 0.08 (0.01, 0.14) | 0.1 (0.03, 0.17) | 0.02 |
| α2 | 0.86 | 0.23 | 0.79 | 0.2 | 0.85 | 0.24 | 0.91 | 0.22 | −0.08 (−0.19, 0.03) | 0.14 | 0.05 (−0.01, 0.11) | 0.13 (0.07, 0.19) | <0.001 |
| Spontaneous baroreflex sensitivity | |||||||||||||
| Spontaneous BRS | 0.41 | 0.29 | 0.32 | 0.24 | 0.27 | 0.22 | 0.36 | 0.38 | −0.08 (−0.23, 0.07) | 0.32 | −0.05 (−0.14, 0.04) | 0.06 (−0.08, 0.20) | 0.16 |
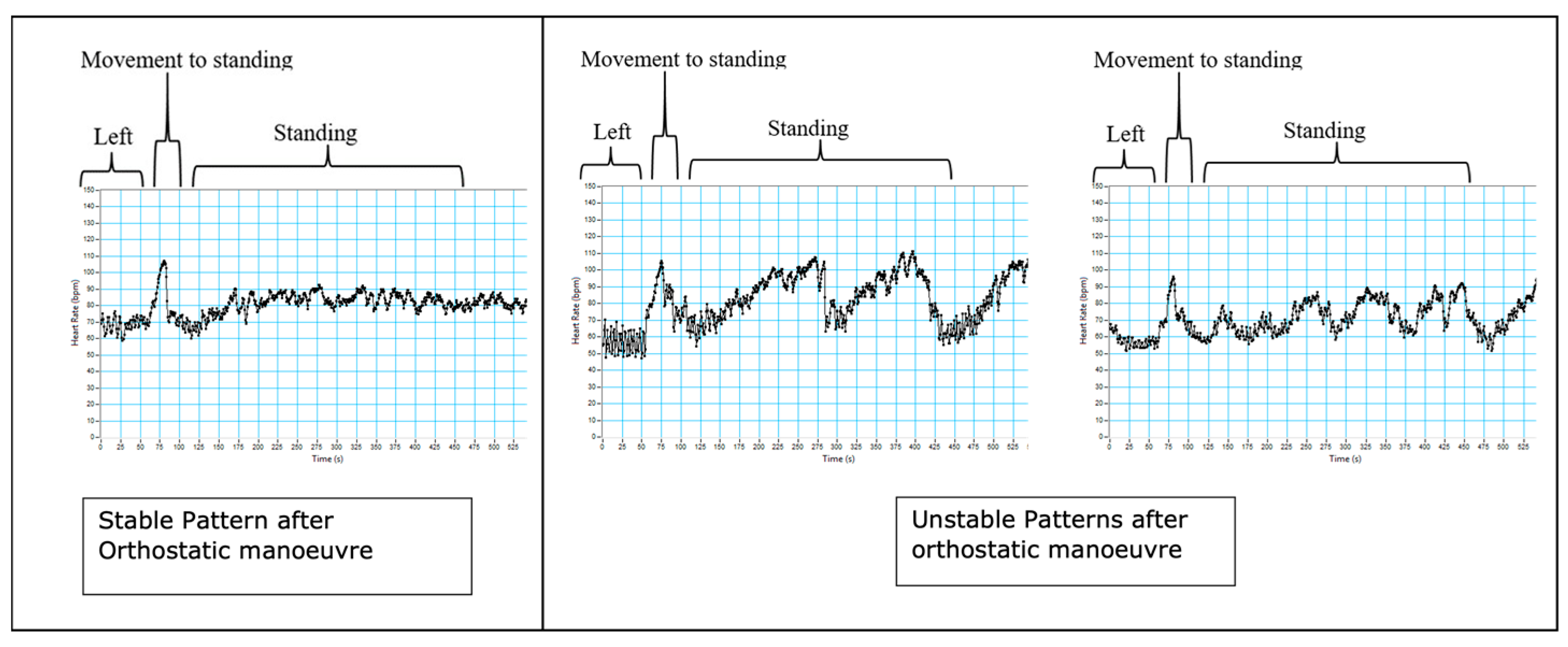
| Standing | Stable | Unstable | Mean Difference (95% CI) | |||
|---|---|---|---|---|---|---|
| (S) | (U) | |||||
| Mean | SD | Mean | SD | U-S | p | |
| Heart rate and systolic blood pressure | ||||||
| Mean heart rate (bpm) | 86 | 9 | 90 | 9 | 4 (−2, 9) | 0.18 |
| SBP (mmHg) | 117 | 16 | 112 | 11 | −5 (−12, 3) | 0.23 |
| Time domain measures of HRV | ||||||
| RR mean (ms) | 707 | 83 | 681 | 75 | −26 (−70, 19) | 0.25 |
| SDNN (ms) | 51 | 24 | 64 | 30 | 13 (−2, 29) | 0.1 |
| RMSSD (ms) | 32 | 39 | 27 | 21 | −5 (−22, 12) | 0.56 |
| Frequency domain measures of HRV | ||||||
| HF (ln, ms2) | 2.3 | 0.6 | 2.4 | 0.6 | 0.1 (−0.2, 0.4) | 0.57 |
| HF (nu) | 20 | 15 | 17 | 14 | −3 (−12, 5) | 0.44 |
| LF (ln, ms2) | 2.7 | 0.5 | 2.8 | 0.4 | 0.1 (−0.1, 0.4) | 0.4 |
| LF (nu) | 39 | 18 | 33 | 15 | −6 (−16, 3) | 0.19 |
| Non-linear measures of HRV | ||||||
| Sample entropy | 1.03 | 0.42 | 0.83 | 0.29 | −0.2 (−0.39, 0.00) | 0.05 |
| α1 | 1.25 | 0.37 | 1.36 | 0.3 | 0.11 (−0.07, 0.30) | 0.23 |
| α2 | 1.05 | 0.27 | 1.15 | 0.22 | 0.1 (−0.03, 0.24) | 0.14 |
| Spontaneous baroreflex sensitivity | ||||||
| Spontaneous BRS | 0.34 | 0.17 | 0.47 | 0.33 | 0.13 (−0.06, 0.31) | 0.12 |
| Position change reflexes | ||||||
| IIHR | 33 | 9 | 38 | 9 | 5 (0, 11) | 0.05 |
| max/min | 1.4 | 0.3 | 1.5 | 0.2 | 0.1 (−0.1, 0.2) | 0.37 |
| Effect of Gestation (St and L Data Combined) | Effect of Position | Effect of Gestation (S and L Data Combined) | Effect of Position | Effect of Gestation (R and L Data Combined) | Effect of Position | ||||
|---|---|---|---|---|---|---|---|---|---|
| T2-T1 | T3-T1 | St-L | T2-T1 | T3-T1 | S-L | T2-T1 | T3-T1 | R-L | |
| Heart rate and systolic blood pressure | |||||||||
| Mean heart rate (bpm) | * | * | * | ↑ | ↑ | - | ↑ | ↑ | ↑ |
| SBP (mmHg) | - | ↑ | ↑ | - | ↑ | ↑ | * | * | * |
| Time domain measures of HRV | |||||||||
| RR mean (ms) | * | * | * | ↓ | ↓ | - | ↓ | ↓ | ↓ |
| SDNN (ms) | * | * | * | ↓ | ↓ | - | ↓ | ↓ | - |
| RMSSD (ms) | * | * | * | * | * | * | ↓ | ↓ | - |
| Frequency domain measures of HRV | |||||||||
| HF (ln, ms2) | * | * | * | ↓ | ↓ | - | ↓ | ↓ | - |
| HF (nu) | * | * | * | * | * | * | ↓ | ↓ | - |
| LF (ln, ms2) | - | - | - | ↓ | ↓ | - | - | - | - |
| LF (nu) | * | * | * | - | - | - | * | * | * |
| Non-linear measures of HRV | |||||||||
| Sample entropy | - | ↓ | ↓ | * | * | * | ↓ | - | - |
| α1 | * | * | * | * | * | * | ↑ | ↑ | - |
| α2 | * | * | * | ↑ | ↑ | ↑ | - | ↑ | - |
| Spontaneous baroreflex sensitivity | |||||||||
| Spontaneous BRS | * | * | * | - | - | ↓ | - | - | ↓ |
| Position change reflexes | |||||||||
| IIHR | ↓ | ↓ | ↓ | ↓ | - | - | |||
| max/min | ↑ | - | - | - | ↓ | ↓ | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clark, A.R.; Fontinha, H.; Thompson, J.; Couper, S.; Jani, D.; Mirjalili, A.; Bennet, L.; Stone, P. Maternal Cardiovascular Responses to Position Change in Pregnancy. Biology 2023, 12, 1268. https://doi.org/10.3390/biology12091268
Clark AR, Fontinha H, Thompson J, Couper S, Jani D, Mirjalili A, Bennet L, Stone P. Maternal Cardiovascular Responses to Position Change in Pregnancy. Biology. 2023; 12(9):1268. https://doi.org/10.3390/biology12091268
Chicago/Turabian StyleClark, Alys R., Hanna Fontinha, John Thompson, Sophie Couper, Devanshi Jani, Ali Mirjalili, Laura Bennet, and Peter Stone. 2023. "Maternal Cardiovascular Responses to Position Change in Pregnancy" Biology 12, no. 9: 1268. https://doi.org/10.3390/biology12091268