Pathophysiology and Clinical Meaning of Ventilation-Perfusion Mismatch in the Acute Respiratory Distress Syndrome


Abstract
:Simple Summary
Abstract
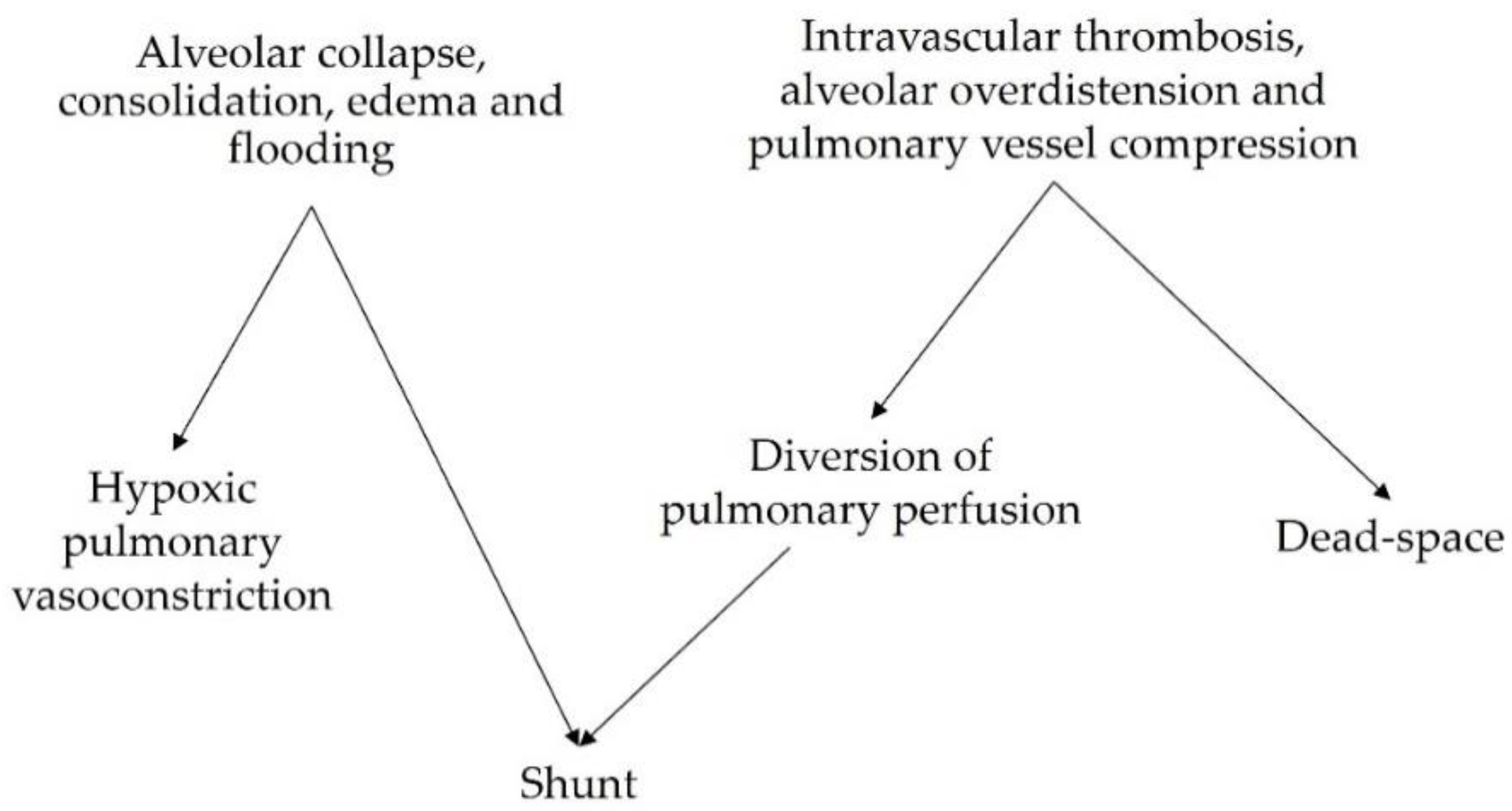
1. Genesis of Ventilation-Perfusion Mismatch in the Acute Respiratory Distress Syndrome
1.1. Non-Ventilated Perfused Units (Shunt)
1.2. Ventilated Non-Perfused Units (Dead-Space)
2. How to Assess V/Q Mismatch at the Bedside
2.1. Shunt at the Bedside
2.2. Dead-Space at the Bedside
2.3. Novel Techniques
3. V/Q Mismatch as a Marker of Severity in ARDS Patients
3.1. Intrapulmonary Shunt
3.2. Dead-Space
3.3. Assessment of V/Q Mismatch by EIT
4. Hypoxic Pulmonary Vasoconstriction and V/Q Mismatch as Mechanisms of VILI
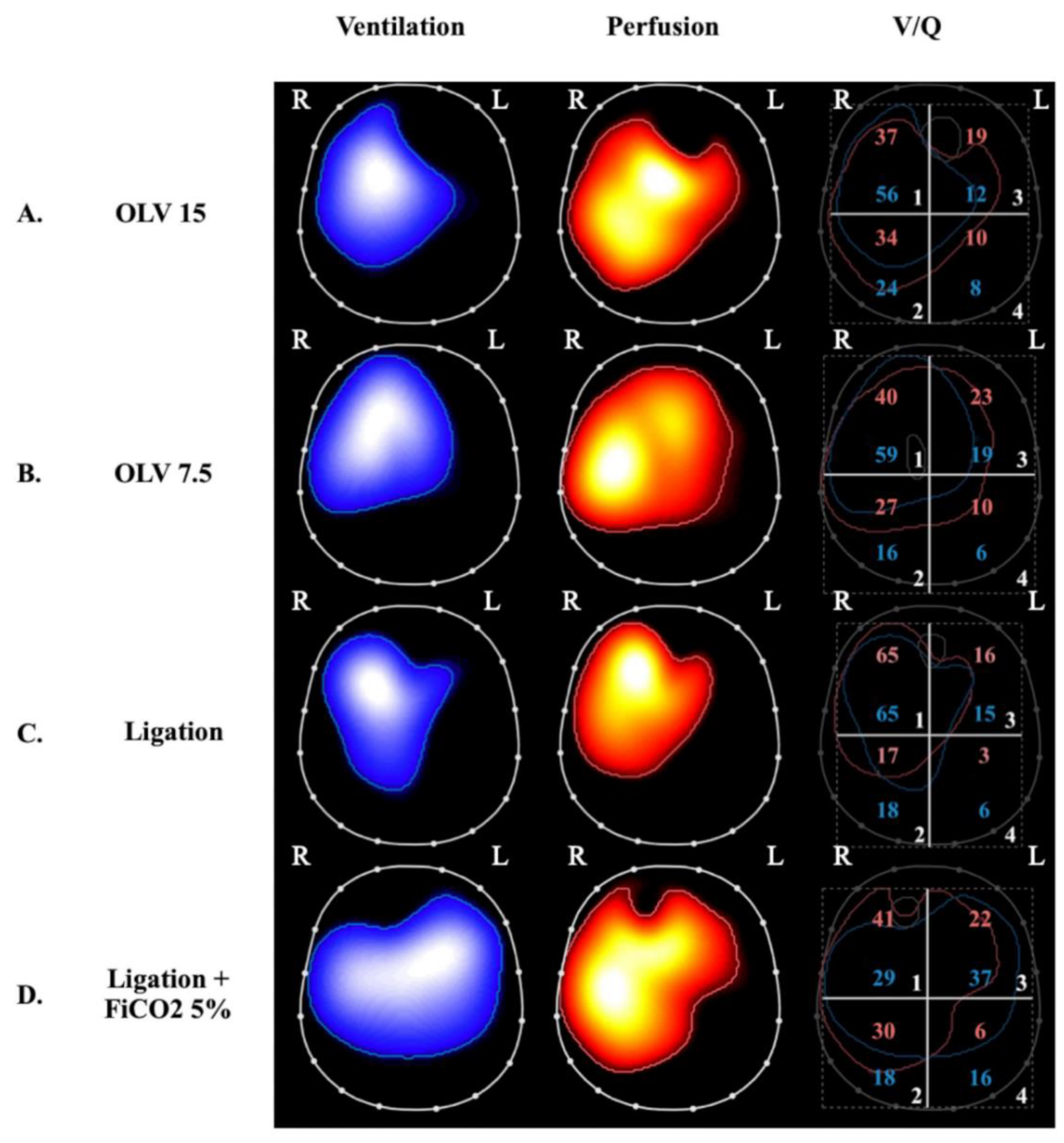
4.1. VILI Related to Perfused Non-Ventilated Lung Units
4.2. VILI Related to Ventilated Non-Perfused Lung Units
5. Strategies for Decreasing V/Q Mismatch in ARDS Patients
5.1. Vasoactive Drugs
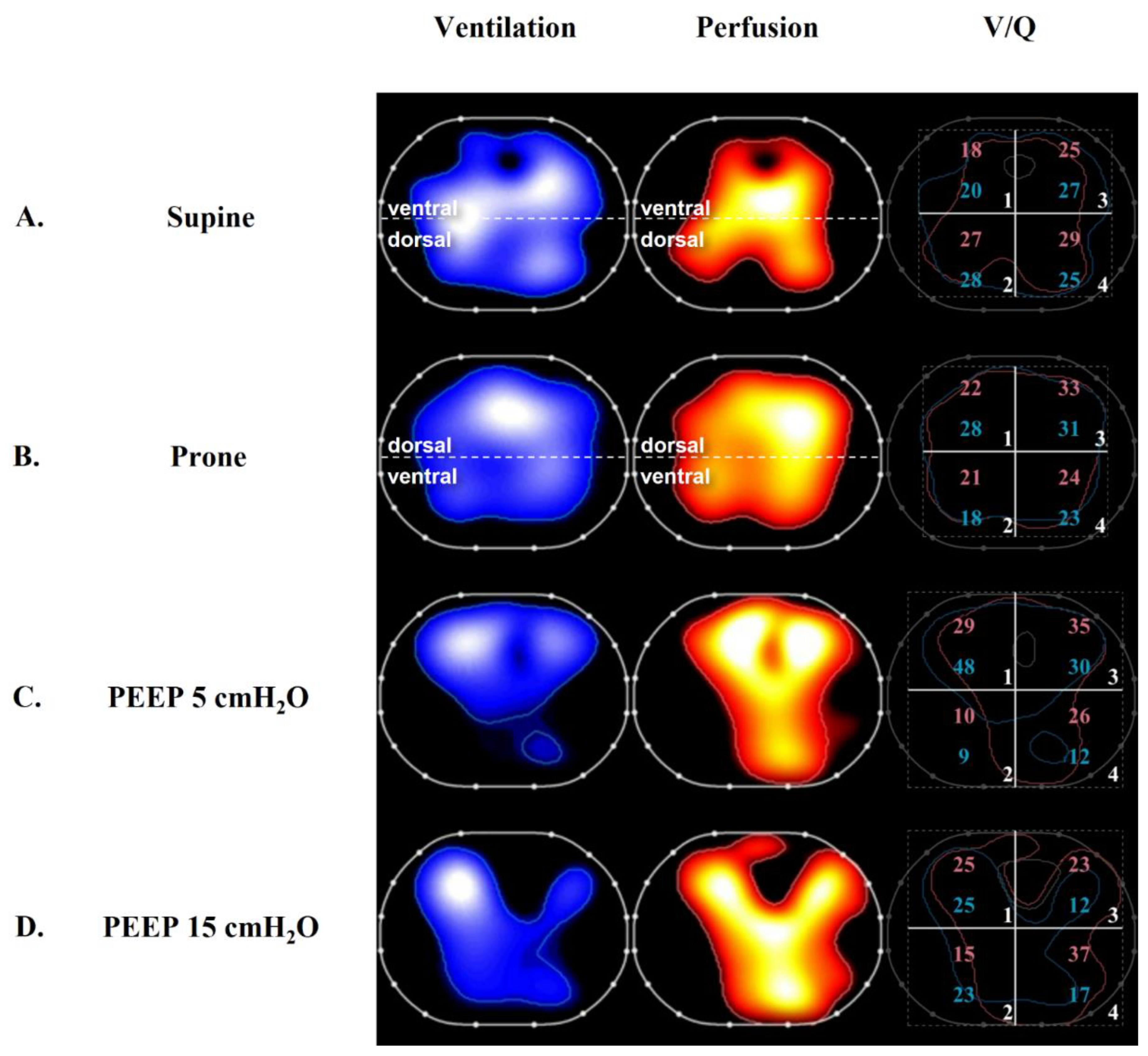
5.2. Positive End-Expiratory Pressure and Recruitment
5.3. Prone Positioning
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef] [PubMed]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [PubMed]
- Acute Respiratory Distress Syndrome Network; Brower, R.G.; Matthay, M.A.; Morris, A.; Schoenfeld, D.; Thompson, B.T.; Wheeler, A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar] [PubMed] [Green Version]
- Slutsky, A.S.; Ranieri, V.M. Ventilator-induced lung injury. N. Engl. J. Med. 2013, 369, 2126–2136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dantzker, D.R.; Brook, C.J.; Dehart, P.; Lynch, J.P.; Weg, J.G. Ventilation-perfusion distributions in the adult respiratory distress syndrome. Am. Rev. Respir. Dis. 1979, 120, 1039–1052. [Google Scholar]
- Pelosi, P.; D’Andrea, L.; Vitale, G.; Pesenti, A.; Gattinoni, L. Vertical gradient of regional lung inflation in adult respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 1994, 149, 8–13. [Google Scholar] [CrossRef]
- Cheng, I.W.; Ware, L.B.; Greene, K.E.; Nuckton, T.J.; Eisner, M.D.; Matthay, M.A. Prognostic value of surfactant proteins A and D in patients with acute lung injury. Crit. Care Med. 2003, 31, 20–27. [Google Scholar] [CrossRef]
- Tsangaris, I.; Lekka, M.E.; Kitsiouli, E.; Constantopoulos, S.; Nakos, G. Bronchoalveolar lavage alterations during prolonged ventilation of patients without acute lung injury. Eur. Respir. J. 2003, 21, 495–501. [Google Scholar] [CrossRef] [Green Version]
- Gattinoni, L.; Caironi, P.; Cressoni, M.; Chiumello, D.; Ranieri, V.M.; Quintel, M.; Russo, S.; Patroniti, N.; Cornejo, R.; Bugedo, G. Lung recruitment in patients with the acute respiratory distress syndrome. N. Engl. J. Med. 2006, 354, 1775–1786. [Google Scholar] [CrossRef]
- Bachofen, M.; Weibel, E.R. Alterations of the gas exchange apparatus in adult respiratory insufficiency associated with septicemia. Am. Rev. Respir. Dis. 1977, 116, 589–615. [Google Scholar] [CrossRef]
- Santos, C.; Ferrer, M.; Roca, J.; Torres, A.; Hernandez, C.; Rodriguez-Roisin, R. Pulmonary gas exchange response to oxygen breathing in acute lung injury. Am. J. Respir. Crit. Care Med. 2000, 161, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Suter, P.M.; Fairley, H.B.; Schlobohm, R.M. Shunt, lung volume and perfusion during short periods of ventilation with oxygen. Anesthesiology 1975, 43, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Theissen, J.L.; Loick, H.M.; Curry, B.B.; Traber, L.D.; Herndon, D.N.; Traber, D.L. Time course of hypoxic pulmonary vasoconstriction after endotoxin infusion in unanesthetized sheep. J. Appl. Physiol. 1991, 70, 2120–2125. [Google Scholar] [CrossRef] [PubMed]
- Hales, C.A.; Sonne, L.; Peterson, M.; Kong, D.; Miller, M.; Watkins, W.D. Role of thromboxane and prostacyclin in pulmonary vasomotor changes after endotoxin in dogs. J. Clin. Investig. 1981, 68, 497–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, T.; Morris, K.; McMurtry, I.F.; Zamora, M.; Tucker, A. Pulmonary and systemic vascular responsiveness to TNF-alpha in conscious rats. J. Appl. Physiol. 1993, 74, 1905–1910. [Google Scholar] [CrossRef] [PubMed]
- Boissier, F.; Razazi, K.; Thille, A.W.; Roche-Campo, F.; Leon, R.; Vivier, E.; Brochard, L.; Brun-Buisson, C.; Mekontso Dessap, A. Echocardiographic detection of transpulmonary bubble transit during acute respiratory distress syndrome. Ann. Intensive Care 2015, 5, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mekontso Dessap, A.; Boissier, F.; Leon, R.; Carreira, S.; Campo, F.R.; Lemaire, F.; Brochard, L. Prevalence and prognosis of shunting across patent foramen ovale during acute respiratory distress syndrome. Crit. Care Med. 2010, 38, 1786–1792. [Google Scholar] [CrossRef]
- Gattinoni, L.; Bombino, M.; Pelosi, P.; Lissoni, A.; Pesenti, A.; Fumagalli, R.; Tagliabue, M. Lung structure and function in different stages of severe adult respiratory distress syndrome. JAMA 1994, 271, 1772–1779. [Google Scholar] [CrossRef]
- Bein, T.; Reber, A.; Stjernstrom, H.; Metz, C.; Taeger, K.; Hedenstierna, G. Ventilation-perfusion ratio in patients with acute respiratory insufficiency. Anaesthesist 1996, 45, 337–342. [Google Scholar]
- Whitelaw, W.A.; Derenne, J.P.; Milic-Emili, J. Occlusion pressure as a measure of respiratory center output in conscious man. Respir. Physiol. 1975, 23, 181–199. [Google Scholar] [CrossRef]
- Greene, R.; Zapol, W.M.; Snider, M.T.; Reid, L.; Snow, R.; O’Connell, R.S.; Novelline, R.A. Early bedside detection of pulmonary vascular occlusion during acute respiratory failure. Am. Rev. Respir. Dis. 1981, 124, 593–601. [Google Scholar] [PubMed]
- Tomashefski, J.F., Jr.; Davies, P.; Boggis, C.; Greene, R.; Zapol, W.M.; Reid, L.M. The pulmonary vascular lesions of the adult respiratory distress syndrome. Am. J. Pathol. 1983, 112, 112–126. [Google Scholar] [PubMed]
- Nuckton, T.J.; Alonso, J.A.; Kallet, R.H.; Daniel, B.M.; Pittet, J.F.; Eisner, M.D.; Matthay, M.A. Pulmonary dead-space fraction as a risk factor for death in the acute respiratory distress syndrome. N. Engl. J. Med. 2002, 346, 1281–1286. [Google Scholar] [CrossRef] [PubMed]
- Sinha, P.; Calfee, C.S.; Beitler, J.R.; Soni, N.; Ho, K.; Matthay, M.A.; Kallet, R.H. Physiologic Analysis and Clinical Performance of the Ventilatory Ratio in Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2019, 199, 333–341. [Google Scholar] [CrossRef]
- Patel, B.V.; Arachchillage, D.J.; Ridge, C.A.; Bianchi, P.; Doyle, J.F.; Garfield, B.; Ledot, S.; Morgan, C.; Passariello, M.; Price, S.; et al. Pulmonary Angiopathy in Severe COVID-19: Physiologic, Imaging, and Hematologic Observations. Am. J. Respir. Crit. Care Med. 2020, 202, 690–699. [Google Scholar] [CrossRef]
- Kuwabara, S.; Duncalf, D. Effect of anatomic shunt on physiologic deadspace-to-tidal volume ratio—A new equation. Anesthesiology 1969, 31, 575–577. [Google Scholar] [CrossRef]
- Berggren, S.M. The Oxygen Deficit of Arterial Blood Caused by Non-Ventilating Parts of the Lung; Norstedt: Stockholm, Sweden, 1942. [Google Scholar]
- Riley, R.L.; Cournand, A. Ideal alveolar air and the analysis of ventilation-perfusion relationships in the lungs. J. Appl. Physiol. 1949, 1, 825–847. [Google Scholar] [CrossRef]
- Shapiro, B.A.; Cane, R.D.; Harrison, R.A.; Steiner, M.C. Changes in intrapulmonary shunting with administration of 100 percent oxygen. Chest 1980, 77, 138–141. [Google Scholar] [CrossRef]
- Reines, H.D.; Civetta, J.M. The inaccuracy of using 100% oxygen to determine intrapulmonary shunts in spite of PEEP. Crit. Care Med. 1979, 7, 301–303. [Google Scholar] [CrossRef]
- Ming, D.K.; Patel, M.S.; Hopkinson, N.S.; Ward, S.; Polkey, M.I. The ‘anatomic shunt test’ in clinical practice; contemporary description of test and in-service evaluation. Thorax 2014, 69, 773–775. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Zhong, M. Inhaled Nitric Oxide Improved Refractory Hypoxemia through Attenuation of Intrapulmonary Shunt. Am. J. Respir. Crit. Care Med. 2022, 205, 1114. [Google Scholar] [CrossRef] [PubMed]
- Rees, S.E.; Kjaergaard, S.; Perthorgaard, P.; Malczynski, J.; Toft, E.; Andreassen, S. The automatic lung parameter estimator (ALPE) system: Non-invasive estimation of pulmonary gas exchange parameters in 10–15 min. J. Clin. Monit. Comput. 2002, 17, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Andreassen, S.; Egeberg, J.; Schroter, M.P.; Andersen, P.T. Estimation of pulmonary diffusion resistance and shunt in an oxygen status model. Comput. Methods Programs Biomed. 1996, 51, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Andreassen, S.; Rees, S.E.; Kjaergaard, S.; Thorgaard, P.; Winter, S.M.; Morgan, C.J.; Alstrup, P.; Toft, E. Hypoxemia after coronary bypass surgery modeled by resistance to oxygen diffusion. Crit. Care Med. 1999, 27, 2445–2453. [Google Scholar] [CrossRef] [PubMed]
- Kreit, J.W. Volume Capnography in the Intensive Care Unit: Physiological Principles, Measurements, and Calculations. Ann. Am. Thorac. Soc. 2019, 16, 291–300. [Google Scholar] [CrossRef]
- Bohr, C. Ueber die Lungenathmung1. Skand. Arch. Physiol. 1891, 2, 236–268. [Google Scholar] [CrossRef] [Green Version]
- Enghoff, H. Volumen inefficax. Upsala Lakaref Forh 1938, 44, 191–218. [Google Scholar]
- Tang, Y.; Turner, M.J.; Baker, A.B. Effects of alveolar dead-space, shunt and V/Q distribution on respiratory dead-space measurements. Br. J. Anaesth. 2005, 95, 538–548. [Google Scholar] [CrossRef] [Green Version]
- Kreit, J.W. Volume Capnography in the Intensive Care Unit: Potential Clinical Applications. Ann. Am. Thorac. Soc. 2019, 16, 409–420. [Google Scholar] [CrossRef]
- Tusman, G.; Suarez-Sipmann, F.; Bohm, S.H.; Borges, J.B.; Hedenstierna, G. Capnography reflects ventilation/perfusion distribution in a model of acute lung injury. Acta Anaesthesiol. Scand. 2011, 55, 597–606. [Google Scholar] [CrossRef]
- Blanch, L.; Lucangelo, U.; Lopez-Aguilar, J.; Fernandez, R.; Romero, P.V. Volumetric capnography in patients with acute lung injury: Effects of positive end-expiratory pressure. Eur. Respir. J. 1999, 13, 1048–1054. [Google Scholar] [CrossRef] [PubMed]
- Tusman, G.; Scandurra, A.; Bohm, S.H.; Suarez-Sipmann, F.; Clara, F. Model fitting of volumetric capnograms improves calculations of airway dead space and slope of phase III. J. Clin. Monit. Comput. 2009, 23, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Beitler, J.R.; Thompson, B.T.; Matthay, M.A.; Talmor, D.; Liu, K.D.; Zhuo, H.; Hayden, D.; Spragg, R.G.; Malhotra, A. Estimating dead-space fraction for secondary analyses of acute respiratory distress syndrome clinical trials. Crit. Care Med. 2015, 43, 1026–1035. [Google Scholar] [CrossRef]
- Harris, J.A.; Benedict, F.G. A Biometric Study of Human Basal Metabolism. Proc. Natl. Acad. Sci. USA 1918, 4, 370–373. [Google Scholar] [CrossRef] [Green Version]
- Dianti, J.; Slutsky, A.S.; Goligher, E.C. Validity of Empirical Estimates of the Ratio of Dead Space to Tidal Volume in ARDS. Respir. Care 2021, 66, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Sinha, P.; Fauvel, N.J.; Singh, S.; Soni, N. Ventilatory ratio: A simple bedside measure of ventilation. Br. J. Anaesth. 2009, 102, 692–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinha, P.; Singh, S.; Hardman, J.G.; Bersten, A.D.; Soni, N.; Australia, New Zealand Intensive Care Society Clinical Trials Group. Evaluation of the physiological properties of ventilatory ratio in a computational cardiopulmonary model and its clinical application in an acute respiratory distress syndrome population. Br. J. Anaesth. 2014, 112, 96–101. [Google Scholar] [CrossRef] [Green Version]
- Sinha, P.; Sanders, R.D.; Soni, N.; Vukoja, M.K.; Gajic, O. Acute respiratory distress syndrome: The prognostic value of ventilatory ratio--a simple bedside tool to monitor ventilatory efficiency. Am. J. Respir. Crit. Care Med. 2013, 187, 1150–1153. [Google Scholar] [CrossRef]
- Gattinoni, L.; Chiumello, D.; Rossi, S. COVID-19 pneumonia: ARDS or not? Crit. Care 2020, 24, 154. [Google Scholar] [CrossRef] [Green Version]
- Bonifazi, M.; Romitti, F.; Busana, M.; Palumbo, M.M.; Steinberg, I.; Gattarello, S.; Palermo, P.; Saager, L.; Meissner, K.; Quintel, M.; et al. End-tidal to arterial PCO2 ratio: A bedside meter of the overall gas exchanger performance. Intensive Care Med. Exp. 2021, 9, 21. [Google Scholar] [CrossRef]
- Kallet, R.H.; Lipnick, M.S. End-Tidal-to-Arterial PCO2 Ratio as Signifier for Physiologic Dead-Space Ratio and Oxygenation Dysfunction in Acute Respiratory Distress Syndrome. Respir. Care 2021, 66, 263–268. [Google Scholar] [CrossRef]
- Frerichs, I.; Hahn, G.; Hellige, G. Thoracic electrical impedance tomographic measurements during volume controlled ventilation-effects of tidal volume and positive end-expiratory pressure. IEEE Trans. Med. Imaging 1999, 18, 764–773. [Google Scholar] [CrossRef]
- Brown, B.H.; Leathard, A.; Sinton, A.; McArdle, F.J.; Smith, R.W.; Barber, D.C. Blood flow imaging using electrical impedance tomography. Clin. Phys. Physiol. Meas. 1992, 13, 175–179. [Google Scholar] [CrossRef]
- Adler, A.; Arnold, J.H.; Bayford, R.; Borsic, A.; Brown, B.; Dixon, P.; Faes, T.J.; Frerichs, I.; Gagnon, H.; Garber, Y.; et al. GREIT: A unified approach to 2D linear EIT reconstruction of lung images. Physiol. Meas. 2009, 30, S35–S55. [Google Scholar] [CrossRef]
- Borges, J.B.; Suarez-Sipmann, F.; Bohm, S.H.; Tusman, G.; Melo, A.; Maripuu, E.; Sandstrom, M.; Park, M.; Costa, E.L.; Hedenstierna, G.; et al. Regional lung perfusion estimated by electrical impedance tomography in a piglet model of lung collapse. J. Appl. Physiol. 2012, 112, 225–236. [Google Scholar] [CrossRef] [Green Version]
- Kircher, M.; Elke, G.; Stender, B.; Hernandez Mesa, M.; Schuderer, F.; Dossel, O.; Fuld, M.K.; Halaweish, A.F.; Hoffman, E.A.; Weiler, N.; et al. Regional Lung Perfusion Analysis in Experimental ARDS by Electrical Impedance and Computed Tomography. IEEE Trans. Med. Imaging 2021, 40, 251–261. [Google Scholar] [CrossRef]
- Bluth, T.; Kiss, T.; Kircher, M.; Braune, A.; Bozsak, C.; Huhle, R.; Scharffenberg, M.; Herzog, M.; Roegner, J.; Herzog, P.; et al. Measurement of relative lung perfusion with electrical impedance and positron emission tomography: An experimental comparative study in pigs. Br. J. Anaesth. 2019, 123, 246–254. [Google Scholar] [CrossRef]
- Mauri, T.; Spinelli, E.; Scotti, E.; Colussi, G.; Basile, M.C.; Crotti, S.; Tubiolo, D.; Tagliabue, P.; Zanella, A.; Grasselli, G.; et al. Potential for Lung Recruitment and Ventilation-Perfusion Mismatch in Patients With the Acute Respiratory Distress Syndrome From Coronavirus Disease 2019. Crit. Care Med. 2020, 48, 1129–1134. [Google Scholar] [CrossRef]
- Fossali, T.; Pavlovsky, B.; Ottolina, D.; Colombo, R.; Basile, M.C.; Castelli, A.; Rech, R.; Borghi, B.; Ianniello, A.; Flor, N.; et al. Effects of Prone Position on Lung Recruitment and Ventilation-Perfusion Matching in Patients with COVID-19 Acute Respiratory Distress Syndrome: A Combined CT Scan/Electrical Impedance Tomography Study. Crit. Care Med. 2022, 50, 723–732. [Google Scholar] [CrossRef]
- Spinelli, E.; Kircher, M.; Stender, B.; Ottaviani, I.; Basile, M.C.; Marongiu, I.; Colussi, G.; Grasselli, G.; Pesenti, A.; Mauri, T. Unmatched ventilation and perfusion measured by electrical impedance tomography predicts the outcome of ARDS. Crit. Care 2021, 25, 192. [Google Scholar] [CrossRef]
- Rabbani, K.S.; Kabir, A.M. Studies on the effect of the third dimension on a two-dimensional electrical impedance tomography system. Clin. Phys. Physiol. Meas. 1991, 12, 393–402. [Google Scholar] [CrossRef]
- Pavlovsky, B.; Pesenti, A.; Spinelli, E.; Scaramuzzo, G.; Marongiu, I.; Tagliabue, P.; Spadaro, S.; Grasselli, G.; Mercat, A.; Mauri, T. Effects of PEEP on regional ventilation-perfusion mismatch in the acute respiratory distress syndrome. Crit. Care 2022, 26, 211. [Google Scholar] [CrossRef]
- Mountain, J.E.; Santer, P.; O’Neill, D.P.; Smith, N.M.J.; Ciaffoni, L.; Couper, J.H.; Ritchie, G.A.D.; Hancock, G.; Whiteley, J.P.; Robbins, P.A. Potential for noninvasive assessment of lung inhomogeneity using highly precise, highly time-resolved measurements of gas exchange. J. Appl. Physiol. 2018, 124, 615–631. [Google Scholar] [CrossRef]
- Laghi, F.; Siegel, J.H.; Rivkind, A.I.; Chiarla, C.; DeGaetano, A.; Blevins, S.; Stoklosa, J.C.; Borg, U.R.; Belzberg, H. Respiratory index/pulmonary shunt relationship: Quantification of severity and prognosis in the post-traumatic adult respiratory distress syndrome. Crit. Care Med. 1989, 17, 1121–1128. [Google Scholar] [CrossRef]
- Kallet, R.H.; Alonso, J.A.; Pittet, J.F.; Matthay, M.A. Prognostic value of the pulmonary dead-space fraction during the first 6 days of acute respiratory distress syndrome. Respir. Care 2004, 49, 1008–1014. [Google Scholar]
- Kallet, R.H.; Zhuo, H.; Liu, K.D.; Calfee, C.S.; Matthay, M.A.; National Heart Lung; Blood Institute ARDS Network Investigators. The association between physiologic dead-space fraction and mortality in subjects with ARDS enrolled in a prospective multi-center clinical trial. Respir. Care 2014, 59, 1611–1618. [Google Scholar] [CrossRef] [Green Version]
- Kallet, R.H.; Zhuo, H.; Ho, K.; Lipnick, M.S.; Gomez, A.; Matthay, M.A. Lung Injury Etiology and Other Factors Influencing the Relationship Between Dead-Space Fraction and Mortality in ARDS. Respir. Care 2017, 62, 1241–1248. [Google Scholar] [CrossRef] [Green Version]
- Graf, J.; Perez, R.; Lopez, R. Increased respiratory dead space could associate with coagulation activation and poor outcomes in COVID-19 ARDS. J. Crit. Care 2022, 71, 154095. [Google Scholar] [CrossRef]
- Siddiki, H.; Kojicic, M.; Li, G.; Yilmaz, M.; Thompson, T.B.; Hubmayr, R.D.; Gajic, O. Bedside quantification of dead-space fraction using routine clinical data in patients with acute lung injury: Secondary analysis of two prospective trials. Crit. Care 2010, 14, R141. [Google Scholar] [CrossRef] [Green Version]
- Morales-Quinteros, L.; Neto, A.S.; Artigas, A.; Blanch, L.; Botta, M.; Kaufman, D.A.; Schultz, M.J.; Tsonas, A.M.; Paulus, F.; Bos, L.D.; et al. Dead space estimates may not be independently associated with 28-day mortality in COVID-19 ARDS. Crit. Care 2021, 25, 171. [Google Scholar] [CrossRef]
- Morales-Quinteros, L.; Schultz, M.J.; Bringue, J.; Calfee, C.S.; Camprubi, M.; Cremer, O.L.; Horn, J.; van der Poll, T.; Sinha, P.; Artigas, A.; et al. Estimated dead space fraction and the ventilatory ratio are associated with mortality in early ARDS. Ann. Intensive Care 2019, 9, 128. [Google Scholar] [CrossRef]
- Siegel, E.R.; Zhuo, H.; Sinha, P.; Papolos, A.I.; Ni, S.A.; Vessel, K.; Belzer, A.; Minus, E.B.; Calfee, C.S.; Matthay, M.A.; et al. Ventilatory Ratio Is a Valuable Prognostic Indicator in an Observational Cohort of Patients With ARDS. Respir. Care 2022, 67, 1075–1081. [Google Scholar] [CrossRef]
- Monteiro, A.C.C.; Vangala, S.; Wick, K.D.; Delucchi, K.L.; Siegel, E.R.; Thompson, B.T.; Liu, K.D.; Sapru, A.; Sinha, P.; Matthay, M.A.; et al. The prognostic value of early measures of the ventilatory ratio in the ARDS ROSE trial. Crit. Care 2022, 26, 297. [Google Scholar] [CrossRef]
- Turzo, M.; Metzger, K.; Lasitschka, F.; Weigand, M.A.; Busch, C.J. Inhibition of overexpressed Kv3.4 augments HPV in endotoxemic mice. BMC Pulm. Med. 2020, 20, 260. [Google Scholar] [CrossRef]
- Leeman, M.; de Beyl, V.Z.; Biarent, D.; Maggiorini, M.; Melot, C.; Naeije, R. Inhibition of cyclooxygenase and nitric oxide synthase in hypoxic vasoconstriction and oleic acid-induced lung injury. Am. J. Respir. Crit. Care Med. 1999, 159 Pt 1, 1383–1390. [Google Scholar] [CrossRef] [Green Version]
- Johnston, W.E.; Vinten-Johansen, J.; Patel, A.; Tommasi, E. Hypoxic pulmonary vasoconstrictor response with asymmetric oleic acid injury in the dog. Crit. Care Med. 1989, 17, 647–651. [Google Scholar] [CrossRef]
- Adrie, C.; Holzmann, A.; Hirani, W.M.; Zapol, W.M.; Hurford, W.E. Effects of intravenous Zaprinast and inhaled nitric oxide on pulmonary hemodynamics and gas exchange in an ovine model of acute respiratory distress syndrome. Anesthesiology 2000, 93, 422–430. [Google Scholar] [CrossRef]
- Melot, C.; Naeije, R.; Mols, P.; Hallemans, R.; Lejeune, P.; Jaspar, N. Pulmonary vascular tone improves pulmonary gas exchange in the adult respiratory distress syndrome. Am. Rev. Respir. Dis. 1987, 136, 1232–1236. [Google Scholar] [CrossRef]
- Jing, L.; Konoeda, H.; Keshavjee, S.; Liu, M. Using nutrient-rich solutions and adding multiple cytoprotective agents as new strategies to develop lung preservation solutions. Am. J. Physiol. Lung Cell. Mol. Physiol. 2021, 320, L979–L989. [Google Scholar] [CrossRef]
- Tremblay, L.; Valenza, F.; Ribeiro, S.P.; Li, J.; Slutsky, A.S. Injurious ventilatory strategies increase cytokines and c-fos m-RNA expression in an isolated rat lung model. J. Clin. Investig. 1997, 99, 944–952. [Google Scholar] [CrossRef]
- Kozian, A.; Schilling, T.; Freden, F.; Maripuu, E.; Rocken, C.; Strang, C.; Hachenberg, T.; Hedenstierna, G. One-lung ventilation induces hyperperfusion and alveolar damage in the ventilated lung: An experimental study. Br. J. Anaesth. 2008, 100, 549–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spinelli, E.; Damia, A.; Damarco, F.; Mauri, T. Ventilator-Induced Lung Injury in the Excluded Lung during One-Lung Ventilation. In Pleural Pressure Working Group Online Meeting; 2022. [Google Scholar]
- Marongiu, I.; Spinelli, E.; Scotti, E.; Mazzucco, A.; Wang, Y.M.; Manesso, L.; Colussi, G.; Biancolilli, O.; Battistin, M.; Langer, T.; et al. Addition of 5% CO2 to Inspiratory Gas Prevents Lung Injury in an Experimental Model of Pulmonary Artery Ligation. Am. J. Respir. Crit. Care Med. 2021, 204, 933–942. [Google Scholar] [CrossRef] [PubMed]
- Tsang, J.Y.; Lamm, W.J.; Swenson, E.R. Regional CO2 tension quantitatively mediates homeostatic redistribution of ventilation following acute pulmonary thromboembolism in pigs. J. Appl. Physiol. 2009, 107, 755–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shepard, J.W., Jr.; Hauer, D.; Miyai, K.; Moser, K.M. Lamellar body depletion in dogs undergoing pulmonary artery occlusion. J. Clin. Investig. 1980, 66, 36–42. [Google Scholar] [CrossRef]
- Chinopoulos, C.; Adam-Vizi, V. Mitochondrial Ca2+ sequestration and precipitation revisited. FEBS J. 2010, 277, 3637–3651. [Google Scholar] [CrossRef] [PubMed]
- Ichimura, H.; Parthasarathi, K.; Lindert, J.; Bhattacharya, J. Lung surfactant secretion by interalveolar Ca2+ signaling. Am. J. Physiol. Lung. Cell Mol. Physiol. 2006, 291, L596–L601. [Google Scholar] [CrossRef] [Green Version]
- Kiefmann, M.; Tank, S.; Keller, P.; Bornchen, C.; Rinnenthal, J.L.; Tritt, M.O.; Schulte-Uentrop, L.; Olotu, C.; Goetz, A.E.; Kiefmann, R. IDH3 mediates apoptosis of alveolar epithelial cells type 2 due to mitochondrial Ca(2+) uptake during hypocapnia. Cell Death Dis. 2017, 8, e3005. [Google Scholar] [CrossRef] [Green Version]
- Thomas, H.M., 3rd; Garrett, R.C. Strength of hypoxic vasoconstriction determines shunt fraction in dogs with atelectasis. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1982, 53, 44–51. [Google Scholar] [CrossRef]
- Fox, G.A.; McCormack, D.G. The pulmonary physician and critical care. 4. A new look at the pulmonary circulation in acute lung injury. Thorax 1992, 47, 743–747. [Google Scholar] [CrossRef] [Green Version]
- Turzo, M.; Vaith, J.; Lasitschka, F.; Weigand, M.A.; Busch, C.J. Role of ATP-sensitive potassium channels on hypoxic pulmonary vasoconstriction in endotoxemia. Respir. Res. 2018, 19, 29. [Google Scholar] [CrossRef] [Green Version]
- Kiefmann, M.; Tank, S.; Tritt, M.O.; Keller, P.; Heckel, K.; Schulte-Uentrop, L.; Olotu, C.; Schrepfer, S.; Goetz, A.E.; Kiefmann, R. Dead space ventilation promotes alveolar hypocapnia reducing surfactant secretion by altering mitochondrial function. Thorax 2019, 74, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Laffey, J.G.; Engelberts, D.; Kavanagh, B.P. Injurious effects of hypocapnic alkalosis in the isolated lung. Am. J. Respir. Crit. Care Med. 2000, 162 Pt 1, 399–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ando, T.; Mikawa, K.; Nishina, K.; Misumi, T.; Obara, H. Hypocapnic alkalosis enhances oxidant-induced apoptosis of human alveolar epithelial type II cells. J. Int. Med. Res. 2007, 35, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Kolobow, T.; Spragg, R.G.; Pierce, J.E. Massive pulmonary infarction during total cardiopulmonary bypass in unanesthetized spontaneously breathing lambs. Int. J. Artif. Organs. 1981, 4, 76–81. [Google Scholar] [CrossRef]
- Langer, T.; Castagna, V.; Brusatori, S.; Santini, A.; Mauri, T.; Zanella, A.; Pesenti, A. Short-term Physiologic Consequences of Regional Pulmonary Vascular Occlusion in Pigs. Anesthesiology 2019, 131, 336–343. [Google Scholar] [CrossRef] [Green Version]
- Broccard, A.F.; Hotchkiss, J.R.; Vannay, C.; Markert, M.; Sauty, A.; Feihl, F.; Schaller, M.D. Protective effects of hypercapnic acidosis on ventilator-induced lung injury. Am. J. Respir. Crit. Care Med. 2001, 164, 802–806. [Google Scholar] [CrossRef]
- Sinclair, S.E.; Kregenow, D.A.; Lamm, W.J.; Starr, I.R.; Chi, E.Y.; Hlastala, M.P. Hypercapnic acidosis is protective in an in vivo model of ventilator-induced lung injury. Am. J. Respir. Crit. Care Med. 2002, 166, 403–408. [Google Scholar] [CrossRef]
- Mauri, T.; Spinelli, E.; Scotti, E.; Marongiu, I.; Mazzucco, A.; Wang, Y.-M.; Manesso, L.; Roma, F.; Biancolilli, O.; Battistin, M.; et al. Occlusion of the Left Pulmonary Artery Induces Bilateral Lung Injury in Healthy Swines. In American Thoracic Society International Conference; American Thoracic Society: New York, NY, USA, 2020. [Google Scholar]
- Esbenshade, A.M.; Newman, J.H.; Lams, P.M.; Jolles, H.; Brigham, K.L. Respiratory failure after endotoxin infusion in sheep: Lung mechanics and lung fluid balance. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1982, 53, 967–976. [Google Scholar] [CrossRef]
- Permpikul, C.; Wang, H.Y.; Kriett, J.; Konopka, R.G.; Moser, K.M.; Spragg, R.G. Reperfusion lung injury after unilateral pulmonary artery occlusion. Respirology 2000, 5, 133–140. [Google Scholar] [CrossRef]
- Broccard, A.F.; Hotchkiss, J.R.; Kuwayama, N.; Olson, D.A.; Jamal, S.; Wangensteen, D.O.; Marini, J.J. Consequences of vascular flow on lung injury induced by mechanical ventilation. Am. J. Respir. Crit. Care Med. 1998, 157 Pt 1, 1935–1942. [Google Scholar] [CrossRef] [Green Version]
- Edmunds, L.H., Jr.; Holm, J.C. Effect of inhaled CO2 on hemorrhagic consolidation due to unilateral pulmonary arterial ligation. J. Appl. Physiol. 1969, 26, 710–715. [Google Scholar] [CrossRef] [PubMed]
- Strand, M.; Ikegami, M.; Jobe, A.H. Effects of high PCO2 on ventilated preterm lamb lungs. Pediatr. Res. 2003, 53, 468–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spinelli, E.; Pesenti, A.; Lopez, G.; Damia, A.; Damarco, F.; Garbelli, E.; Dal Santo, G.; Caccioppola, A.; Giudici, G.; Figgiaconi, V.; et al. Inhaled CO2 vs. Hypercapnia Obtained by Low Tidal Volume or Instrumental Dead Space in Unilateral Pulmonary Artery Ligation: Any Difference for Lung Protection? Front. Med. 2022, 9, 901809. [Google Scholar] [CrossRef] [PubMed]
- Reyes, A.; Roca, J.; Rodriguez-Roisin, R.; Torres, A.; Ussetti, P.; Wagner, P.D. Effect of almitrine on ventilation-perfusion distribution in adult respiratory distress syndrome. Am. Rev. Respir. Dis. 1988, 137, 1062–1067. [Google Scholar] [CrossRef]
- Gallart, L.; Lu, Q.; Puybasset, L.; Umamaheswara Rao, G.S.; Coriat, P.; Rouby, J.J. Intravenous almitrine combined with inhaled nitric oxide for acute respiratory distress syndrome. The NO Almitrine Study Group. Am. J. Respir. Crit. Care Med. 1998, 158, 1770–1777. [Google Scholar] [CrossRef]
- Rossaint, R.; Falke, K.J.; Lopez, F.; Slama, K.; Pison, U.; Zapol, W.M. Inhaled nitric oxide for the adult respiratory distress syndrome. N. Engl. J. Med. 1993, 328, 399–405. [Google Scholar] [CrossRef]
- Bagate, F.; Tuffet, S.; Masi, P.; Perier, F.; Razazi, K.; de Prost, N.; Carteaux, G.; Payen, D.; Mekontso Dessap, A. Rescue therapy with inhaled nitric oxide and almitrine in COVID-19 patients with severe acute respiratory distress syndrome. Ann. Intensive Care 2020, 10, 151. [Google Scholar] [CrossRef]
- Taylor, R.W.; Zimmerman, J.L.; Dellinger, R.P.; Straube, R.C.; Criner, G.J.; Davis, J.; Kenneth Kelly, K.M.; Smith, T.C.; Small, R.J.; Group ftINOiAS. Low-Dose Inhaled Nitric Oxide in Patients With Acute Lung InjuryA Randomized Controlled Trial. JAMA 2004, 291, 1603–1609. [Google Scholar] [CrossRef]
- Hermle, G.; Mols, G.; Zugel, A.; Benzing, A.; Lichtwarck-Aschoff, M.; Geiger, K.; Guttmann, J. Intratidal compliance-volume curve as an alternative basis to adjust positive end-expiratory pressure: A study in isolated perfused rabbit lungs. Crit. Care Med. 2002, 30, 1589–1597. [Google Scholar] [CrossRef]
- Brower, R.G.; Lanken, P.N.; MacIntyre, N.; Matthay, M.A.; Morris, A.; Ancukiewicz, M.; Schoenfeld, D.; Thompson, B.T.; The National Heart; Lung, and Blood Institute ARDS Clinical Trials Network. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N. Engl. J. Med. 2004, 351, 327–336. [Google Scholar]
- Mercat, A.; Richard, J.C.; Vielle, B.; Jaber, S.; Osman, D.; Diehl, J.L.; Lefrant, J.Y.; Prat, G.; Richecoeur, J.; Nieszkowska, A.; et al. Positive end-expiratory pressure setting in adults with acute lung injury and acute respiratory distress syndrome: A randomized controlled trial. JAMA 2008, 299, 646–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meade, M.O.; Cook, D.J.; Guyatt, G.H.; Slutsky, A.S.; Arabi, Y.M.; Cooper, D.J.; Davies, A.R.; Hand, L.E.; Zhou, Q.; Thabane, L.; et al. Ventilation strategy using low tidal volumes, recruitment maneuvers, and high positive end-expiratory pressure for acute lung injury and acute respiratory distress syndrome: A randomized controlled trial. JAMA 2008, 299, 637–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beitler, J.R.; Sarge, T.; Banner-Goodspeed, V.M.; Gong, M.N.; Cook, D.; Novack, V.; Loring, S.H.; Talmor, D.; Group EP-S. Effect of Titrating Positive End-Expiratory Pressure (PEEP) With an Esophageal Pressure-Guided Strategy vs an Empirical High PEEP-Fio2 Strategy on Death and Days Free From Mechanical Ventilation Among Patients With Acute Respiratory Distress Syndrome: A Randomized Clinical Trial. JAMA 2019, 321, 846–857. [Google Scholar] [PubMed] [Green Version]
- Ralph, D.D.; Robertson, H.T.; Weaver, L.J.; Hlastala, M.P.; Carrico, C.J.; Hudson, L.D. Distribution of ventilation and perfusion during positive end-expiratory pressure in the adult respiratory distress syndrome. Am. Rev. Respir. Dis. 1985, 131, 54–60. [Google Scholar]
- Karbing, D.S.; Panigada, M.; Bottino, N.; Spinelli, E.; Protti, A.; Rees, S.E.; Gattinoni, L. Changes in shunt, ventilation/perfusion mismatch, and lung aeration with PEEP in patients with ARDS: A prospective single-arm interventional study. Crit. Care 2020, 24, 111. [Google Scholar] [CrossRef] [Green Version]
- Perier, F.; Tuffet, S.; Maraffi, T.; Alcala, G.; Victor, M.; Haudebourg, A.F.; De Prost, N.; Amato, M.; Carteaux, G.; Mekontso Dessap, A. Effect of Positive End-Expiratory Pressure and Proning on Ventilation and Perfusion in COVID-19 Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2020, 202, 1713–1717. [Google Scholar] [CrossRef]
- Guerin, C.; Reignier, J.; Richard, J.C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone positioning in severe acute respiratory distress syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef]
- Gattinoni, L.; Vagginelli, F.; Carlesso, E.; Taccone, P.; Conte, V.; Chiumello, D.; Valenza, F.; Caironi, P.; Pesenti, A.; Prone-Supine Study Group. Decrease in PaCO2 with prone position is predictive of improved outcome in acute respiratory distress syndrome. Crit. Care Med. 2003, 31, 2727–2733. [Google Scholar] [CrossRef]
- Pierrakos, C.; van der Ven, F.; Smit, M.R.; Hagens, L.A.; Paulus, F.; Schultz, M.J.; Bos, L.D.J. Prone Positioning Decreases Inhomogeneity and Improves Dorsal Compliance in Invasively Ventilated Spontaneously Breathing COVID-19 Patients-A Study Using Electrical Impedance Tomography. Diagnostics 2022, 12, 2281. [Google Scholar] [CrossRef]
- Slobod, D.; Spinelli, E.; Scaramuzzo, G.; Lissoni, A.; Grasselli, G.; Mauri, T. Redistribution of Perfusion by Prone Positioning Improves Shunt in a Patient with Unilateral Lung Injury. Am. J. Respir. Crit. Care Med. 2022, 206, e76–e78. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Mechanisms of Injury | Reference | |
|---|---|---|
| Shunt (perfused non-ventilated lung units) | Redistribution of perfusion due to hypoxic pulmonary vasoconstriction: hypo-perfused lung zones with locally decreased oxygen and nutrient delivery and lung ischemia. | [75] |
| Decreased size of aerated lung with increased risk of overdistension and barotrauma in the ventilated lung. | [76,77,78] | |
| Dead-space (ventilated non-perfused lung units) | Local alveolar hypocapnia: altered surfactant system, alveolar instability, apoptosis, and hemorrhagic infarction. | [79,80,81,82,83,84,85,86,87] |
| Local bronchoconstriction with diversion of ventilation to perfused lung zones resulting in hyperventilation and hyperperfusion in diverted zones. | [88,89] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Slobod, D.; Damia, A.; Leali, M.; Spinelli, E.; Mauri, T. Pathophysiology and Clinical Meaning of Ventilation-Perfusion Mismatch in the Acute Respiratory Distress Syndrome. Biology 2023, 12, 67. https://doi.org/10.3390/biology12010067
Slobod D, Damia A, Leali M, Spinelli E, Mauri T. Pathophysiology and Clinical Meaning of Ventilation-Perfusion Mismatch in the Acute Respiratory Distress Syndrome. Biology. 2023; 12(1):67. https://doi.org/10.3390/biology12010067
Chicago/Turabian StyleSlobod, Douglas, Anna Damia, Marco Leali, Elena Spinelli, and Tommaso Mauri. 2023. "Pathophysiology and Clinical Meaning of Ventilation-Perfusion Mismatch in the Acute Respiratory Distress Syndrome" Biology 12, no. 1: 67. https://doi.org/10.3390/biology12010067