
Trophism and Homeostasis of Liver Sinusoidal Endothelial Graft Cells during Preservation, with and without Hypothermic Oxygenated Perfusion

 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Donors’ Enrolment
- Allocation biopsy (A-Biopsy), performed at the stage of organ allocation for the assessment of graft suitability, as usually performed in our Institution [26];
- Post-perfusion biopsy (PP-Biopsy), performed for the purposes of the study after graft implant in the recipients. This biopsy was specifically performed for the study.
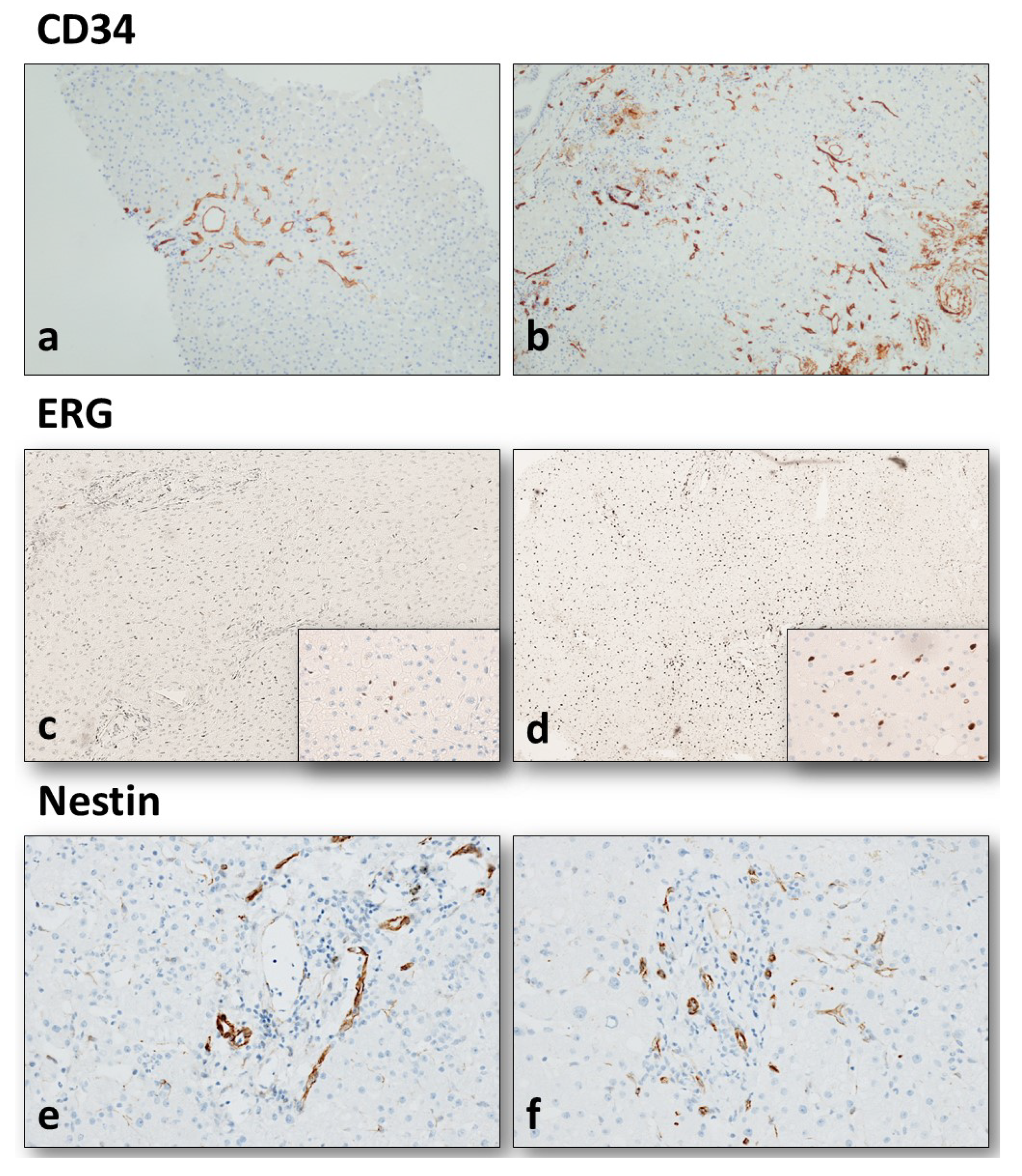
2.2. Histopathological Analysis and Immunohistochemistry
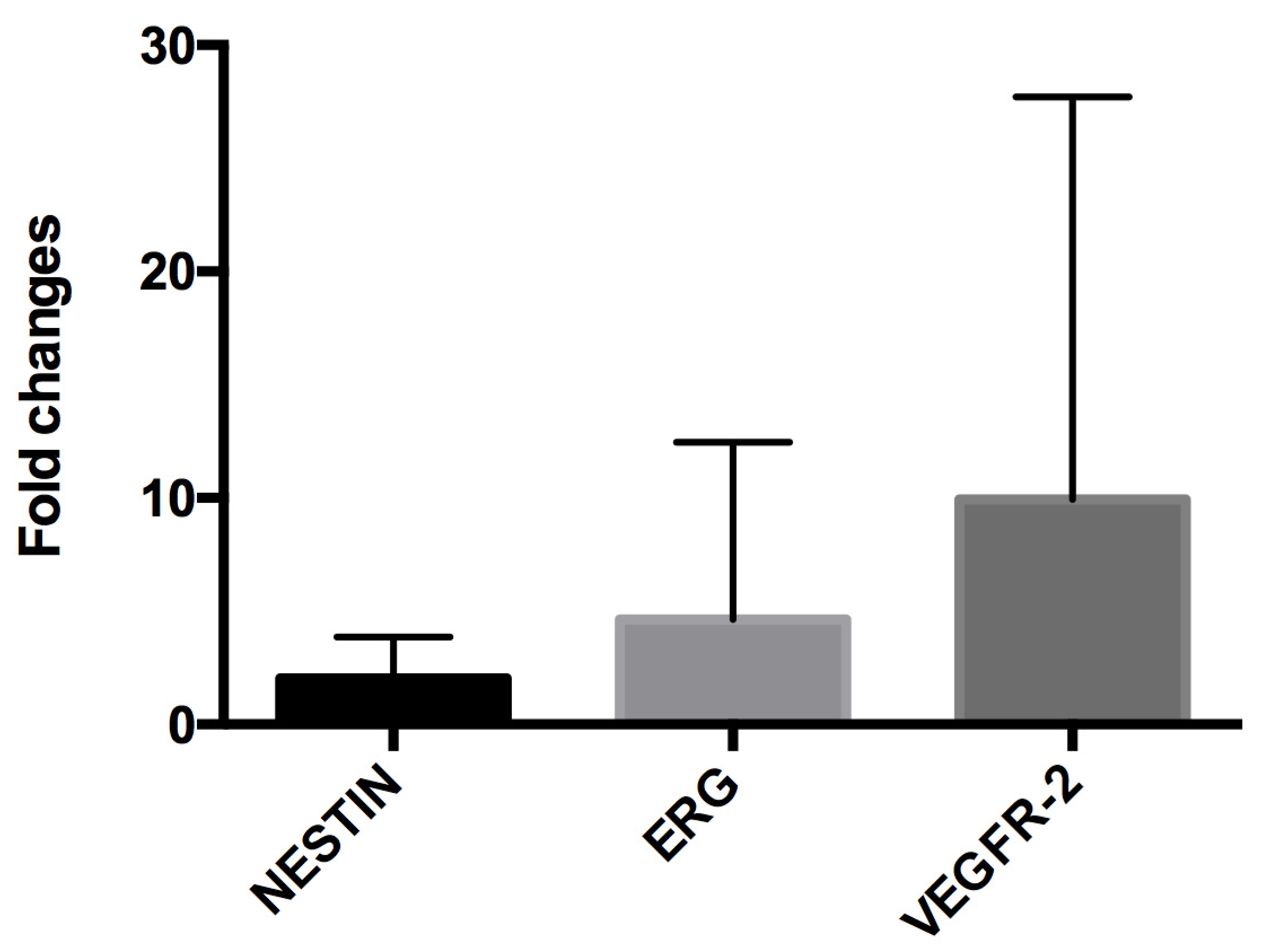
2.3. RNA Extraction and Reverse Transcriptase-Polymerase Chain Reaction (RT-PCR)
2.4. Statistical Analysis
3. Results
3.1. Donor and Graft Characteristics
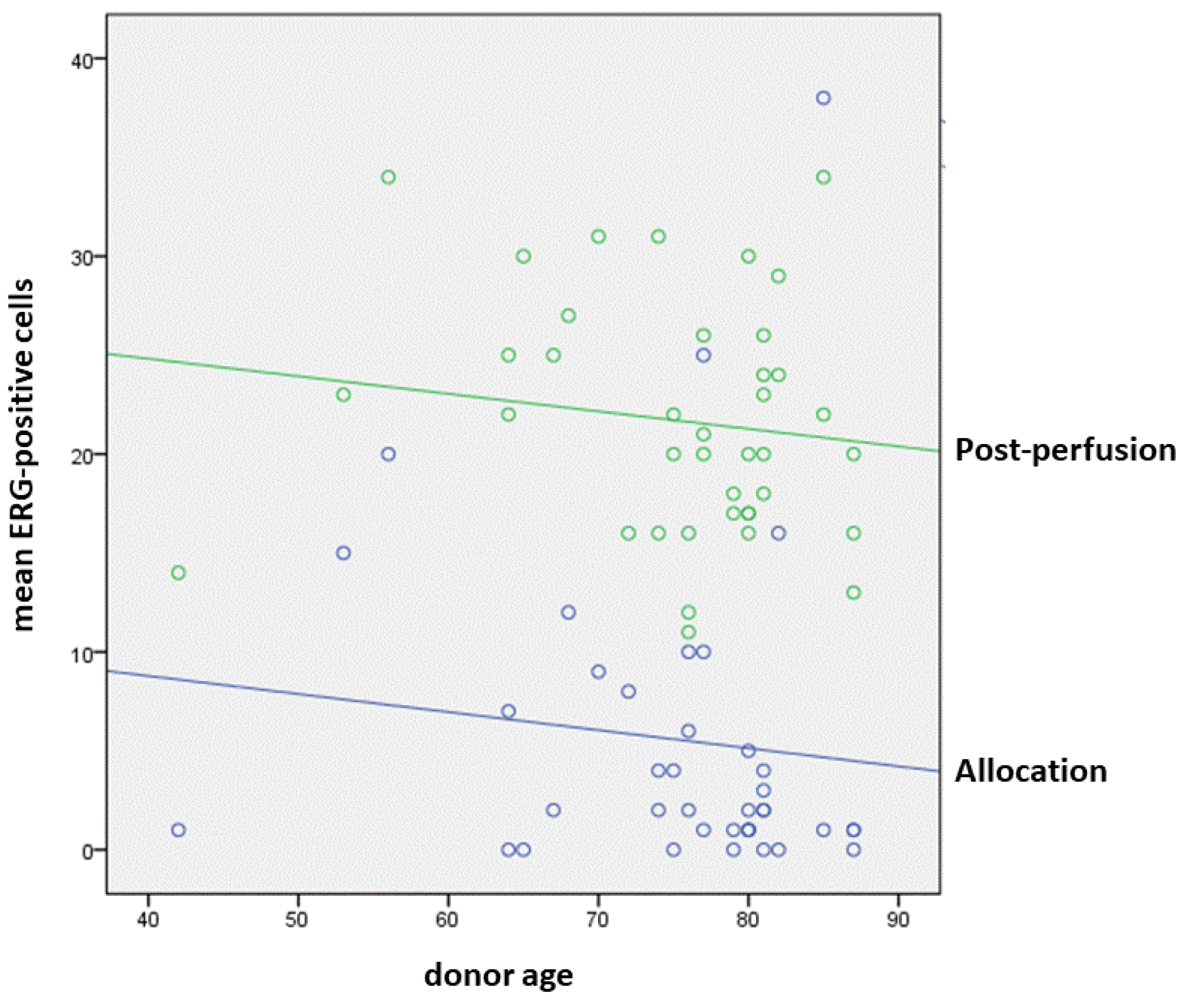
3.2. Modifications of Endothelial Trophism in Allocation and Post-Reperfusion Biopsies
3.3. Perfusion Characteristics Influencing Endothelial Trophism in Liver Grafts and Preliminary Follow-Up Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chiu, J.J.; Chien, S. Effects of disturbed blood flow on vascular endothelium: Pathophysiological basis and clinical perspectives. Physiol. Rev. 2011, 91, 327–387. [Google Scholar] [CrossRef] [PubMed]
- Poisson, J.; Lemoinne, S.; Boulanger, C.; Durand, F.; Moreau, R.; Valla, D.; Rautou, P.E. Liver sinusoidal endothelial cells: Physiology and role in live disease. J. Hepatol. 2017, 66, 212–227. [Google Scholar] [CrossRef] [PubMed]
- Schaffner, F.; Poper, H. Capillarization of hepatic sinusoids in man. Gastroenterology 1963, 44, 239–242. [Google Scholar] [CrossRef]
- Lalor, P.F.; Lai, W.K.; Curbishley, S.M.; Shetty, S.; Adams, D.M. Human hepatic sinusoidal endothelial cells can be distiguished by expression of phenotypic markers related to their specialised functions in vivo. World J. Gastroenterol. 2006, 12, 5429–5439. [Google Scholar] [CrossRef]
- Attia, M.; Silva, M.A.; Mirza, D.F. The marginal liver donor—An update. Transpl. Int. 2008, 21, 713–724. [Google Scholar] [CrossRef]
- Schlegel, A.; Rougemont, O.; de Graf, R.; Clavien, P.A.; Dutkowski, P. Protective mechanisms of end-ischemic cold machine perfusion in DCD liver grafts. J. Hepatol. 2013, 58, 278–286. [Google Scholar] [CrossRef]
- Feng, S.; Goodrich, N.P.; Bragg-Gresham, J.L.; Dykstra, D.M.; Punch, J.D.; DebRoy, M.A.; Greenstein, S.M.; Merion, R.M. Characteristics associated with liver graft failure: The concept of a donor risk index. Am. J. Transpl. 2006, 6, 783–790. [Google Scholar] [CrossRef]
- Schlegel, A.; Muller, X.; Dutkowski, P. Machine perfusion strategies in liver transplantation. HepatoBil. Surg. Nutr. 2019, 8, 490–501. [Google Scholar] [CrossRef]
- Ravaioli, M.; Germinario, G.; Dajti, G.; Sessa, M.; Vasuri, F.; Siniscalchi, A.; Morelli, M.C.; Serenari, M.; Del Gaudio, M.; Zanfi, C.; et al. Hypothermic Oxygenated Perfusion in Extended Criteria Donor Liver Transplantation—A Randomized Clinical Trial. Am. J. Transpl. Publ. Online 2022. Epub ahead of print. [Google Scholar] [CrossRef]
- Ravaioli, M.; de Pace, V.; Angeletti, A.; Comai, G.; Vasuri, F.; Baldassarre, M.; Maroni, L.; Odaldi, F.; Fallani, G.; Caraceni, P.; et al. Hypothermic Oxygenated New Machine Perfusion System in Liver and Kidney Transplantation of Extended Criteria Donors:First Italian Clinical Trial. Sci. Rep. 2020, 10, 6063. [Google Scholar] [CrossRef] [Green Version]
- Schlegel, A.; Muller, X.; Dutkowski, P. Hypothermic Machine Preservation of the Liver: State of the Art. Curr. Transplant. Rep. 2018, 5, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Schlegel, A.; Porte, R.; Dutkowski, P. Protective mechanisms and current clinical evidence of hypothermic oxygenated machine perfusion (HOPE) in preventing post-transplant cholangiopathy. J. Hepatol. 2022, 76, 1330–1347. [Google Scholar] [CrossRef] [PubMed]
- Parmar, K.M.; Larman, H.B.; Dai, G.; Zhang, Y.; Wang, E.T.; Moorthy, S.N.; Kratz, J.R.; Lin, Z.; Jain, M.K.; Gimbrone, M.A., Jr.; et al. Integration of flow-dependent endothelial phenotypes by Kruppel-like factor 2. J. Clin. Investig. 2006, 116, 49–58. [Google Scholar] [CrossRef]
- Czigany, Z.; Lurje, I.; Tolba, R.H.; Neumann, U.P.; Tacke, F.; Lurje, G. Machine perfusion for liver transplantation in the era of marginal organs-New kids on the block. Liver. Int. 2019, 39, 228–249. [Google Scholar] [CrossRef]
- Fernández, L.; Heredia, N.; Grande, L.; Gómez, G.; Rimola, A.; Marco, A.; Gelpí, E.; Roselló-Catafau, J.; Peralta, C. Preconditioning protects liver and lung damage in rat liver transplantation: Role of xanthine/xanthine oxidase. Hepatology 2002, 36, 562–572. [Google Scholar] [CrossRef]
- Peralta, C.; Jiménez-Castro, M.B.; Gracia-Sancho, J. Hepatic ischemia and reperfusion injury: Effects on the liver sinusoidal milieu. J. Hepatol. 2013, 59, 1094–1106. [Google Scholar] [CrossRef]
- Shah, A.V.; Birdsey, G.M.; Randi, A.M. Regulation of endothelial homeostasis, vascular development and angiogenesis by the transcription factor ERG. Vasc. Pharmacol. 2016, 86, 3–13. [Google Scholar] [CrossRef]
- Birdsey, G.M.; Dryden, N.H.; Amsellem, V.; Gebhardt, F.; Sahnan, K.; Haskard, D.O.; Dejana, E.; Mason, J.C.; Randi, A.M. Transcription factor Erg regulates angiogenesis and endothelial apoptosis through VE-cadherin. Blood 2008, 111, 3498–3506. [Google Scholar] [CrossRef]
- McLaughlin, F.; Ludbrook, V.J.; Cox, J.; von Carlowitz, I.; Brown, S.; Randi, A.M. Combined genomic and antisense analysis reveals that the transcription factor Erg is implicated in endothelial cell differentiation. Blood 2001, 98, 3332–3339. [Google Scholar] [CrossRef]
- Laumonnier, Y.; Nadaud, S.; Agrapart, M.; Soubrier, F. Characterization of an upstream enhancer region in the promoter of the human endothelial nitric-oxide synthase gene. J. Biol. Chem. 2000, 275, 40732–40741. [Google Scholar] [CrossRef] [Green Version]
- Sperone, A.; Dryden, N.H.; Birdsey, G.M.; Madden, L.; Johns, M.; Evans, P.C.; Mason, J.C.; Haskard, D.O.; Boyle, J.J.; Paleolog, E.M.; et al. The transcription factor Erg inhibits vascular inflammation by repressing NF-kappaB activation and proinflammatory gene expression in endothelial cells. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Michalczyk, K.; Ziman, M. Nestin structure and predicted function in cellular cytoskeletal organisation. Histol. Histopathol. 2005, 20, 665–671. [Google Scholar] [PubMed]
- Vasuri, F.; Fittipaldi, S.; Giunchi, F.; Monica, M.; Ravaioli, M.; Degiovanni, A.; Bonora, S.; Golfieri, R.; Bolondi, L.; Grigioni, W.F.; et al. Facing the enigma of the vascular network in hepatocellular carcinomas in cirrhotic and non-cirrhotic livers. J. Clin. Pathol. 2016, 69, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Malvi, D.; de Biase, D.; Fittipaldi, S.; Grillini, M.; Visani, M.; Pession, A.; D’Errico, A.; Vasuri, F. Immunomorphology and molecular biology of mixed primary liver cancers: Is Nestin a marker of intermediate-cell carcinoma? Histopathology 2020, 76, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Ravaioli, M.; Maroni, L.; Angeletti, A.; Fallani, G.; de Pace, V.; Germinario, G.; Odaldi, F.; Corradetti, V.; Caraceni, P.; Baldassarre, M.; et al. Hypothermic Oxygenated Perfusion Versus Static Cold Storage for Expanded Criteria Donors in Liver and Kidney Transplantation: Protocol for a Single-Center Randomized Controlled Trial. JMIR. Res. Protoc. 2020, 9, e13922. [Google Scholar] [CrossRef]
- D’Errico, A.; Riefolo, M.; Serenari, M.; de Pace, V.; Santandrea, G.; Monica, M.; de Cillia, C.; Ravaioli, M.; Cescon, M.; Vasuri, F. The histological assessment of liver fibrosis in grafts from extended criteria donors predicts the outcome after liver transplantation: A retrospective study. Dig. Liver. Dis. 2020, 52, 185–189. [Google Scholar] [CrossRef]
- Ishak, K.; Baptista, A.; Bianchi, L.; Callea, F.; de Groote, J.; Gudat, F.; Denk, H.; Desmet, V.; Korb, G.; MacSween, R.N.; et al. Histological grading and staging of chronic hepatitis. J. Hepatol. 1995, 22, 696–699. [Google Scholar] [CrossRef]
- Fiorentino, M.; Vasuri, F.; Ravaioli, M.; Ridolfi, L.; Grigioni, W.F.; Pinna, A.D.; D’Errico-Grigioni, A. Predictive value of frozen-section analysis in the histological assessment of steatosis before liver transplantation. Liver Transplant. 2009, 15, 1821–1825. [Google Scholar] [CrossRef]
- Ruan, B.; Duan, J.L.; Xu, H.; Tao, K.S.; Han, H.; Dou, G.R.; Wang, L. Capillarized Liver Sinusoidal Endothelial Cells Undergo Partial Endothelial-Mesenchymal Transition to Actively Deposit Sinusoidal ECM in Liver Fibrosis. Front. Cell. Dev. Biol. 2021, 9, 671081. [Google Scholar] [CrossRef]
- Hong, L.; Du, X.; Li, W.; Mao, Y.; Sun, L.; Li, X. EndMT: A promising and controversial field. Eur. J. Cell. Biol. 2018, 97, 493–500. [Google Scholar] [CrossRef]
- Birdsey, G.M.; Shah, A.V.; Dufton, N.; Reynolds, L.E.; Almagro, L.O.; Yang, Y.; Aspalter, I.M.; Khan, S.T.; Mason, J.C.; Dejana, E.; et al. The endothelial transcription factor ERG promotes vascular stability and growth through Wnt/β-catenin signaling. Dev. Cell. 2015, 32, 82–96. [Google Scholar] [CrossRef] [PubMed]
- Peghaire, C.; Dufton, N.P.; Lang, M.; Salles-Crawley, I.I.; Ahnström, J.; Kalna, V.; Raimondi, C.; Pericleous, C.; Inuabasi, L.; Kiseleva, R.; et al. The transcription factor ERG regulates a low shear stress-induced anti-thrombotic pathway in the microvasculature. Nat. Commun. 2019, 10, 5014. [Google Scholar] [CrossRef] [PubMed]
- Dufton, N.P.; Peghaire, C.R.; Osuna-Almagro, L.; Raimondi, C.; Kalna, V.; Chauhan, A.; Webb, G.; Yang, Y.; Birdsey, G.M.; Lalor, P.; et al. Dynamic regulation of canonical TGFβ signalling by endothelial transcription factor ERG protects from liver fibrogenesis. Nat. Commun. 2017, 8, 895. [Google Scholar] [CrossRef]
- Ginsberg, M.; James, D.; Ding, B.S.; Nolan, D.; Geng, F.; Butler, J.M.; Schachterle, W.; Pulijaal, V.R.; Mathew, S.; Chasen, S.T.; et al. Efficient direct reprogramming of mature amniotic cells into endothelial cells by ETS factors and TGFβ suppression. Cell 2012, 151, 559–575. [Google Scholar] [CrossRef]
- Wilkinson, A.L.; Qurashi, M.; Shetty, S. The Role of Sinusoidal Endothelial Cells in the Axis of Inflammation and Cancer Within the Liver. Front. Physiol. 2020, 11, 990. [Google Scholar] [CrossRef]
- Maeso-Díaz, R.; Ortega-Ribera, M.; Fernández-Iglesias, A.; Hide, D.; Muñoz, L.; Hessheimer, A.J.; Vila, S.; Francés, R.; Fondevila, C.; Albillos, A.; et al. Effects of aging on liver microcirculatory function and sinusoidal phenotype. Aging Cell 2018, 17, e12829. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Histopathological Variable | No. (Percentage) |
|---|---|
| Portal Fibrosis (Ishak’s stage) 0 1 2 3 | 3 (6.4%) 19 (40.4%) 23 (48.9%) 2 (4.3%) |
| Lobular Fibrosis Absent Mild/focal Severe/diffuse | 31 (66.0%) 12 (25.5%) 4 (8.5%) |
| Portal Inflammation Absent Mild Moderate-to-severe | 7 (14.9%) 35 (75.5%) 5 (10.6%) |
| Myointimal Thickening Absent/mild Moderate Severe | 22 (46.8%) 17 (36.2%) 8 (17.0%) |
| Biliocyte/bile duct regression Absent Mild Severe | 5 (10.6%) 38 (80.9%) 4 (8.5%) |
| Lobular Inflammation Absent Mild Moderate-to-severe | 30 (63.8%) 15 (31.9%) 2 (4.3%) |
| Lobular NecrosisAbsent Mild Moderate-to-severe | 33 (70.2%) 11 (23.4%) 3 (6.4%) |
| Cholestasis Absent Mild | 36 (76.6%) 11 (23.4%) |
| Microvesicular steatosis (mean) | 6.5 ± 6.7% (0–20%) |
| Macrovesicular steatosis (mean) | 4.2 ± 6.1% (0–25%) |
| HOPE (n = 34) | SCS (n = 13) | Sig. | |
|---|---|---|---|
| Mean Age | 73.7 years | 78.8 years | n.s. |
| Sex (male) | 17 (50%) | 5 (38.5%) | n.s. |
| MELD score | 14.4 | 23.0 | n.s |
| Cold ischemia time (min) | 411.2 | 361.8 | n.s. |
| Post-perfusion CD34 (diffuse endothelization) | 14 (41.2%) | 7 (53.8%) | n.s. |
| Post-perfusion mean Nestin-positive capillaries | 7.3 | 7.5 | n.s. |
| Post-perfusion mean ERG-positive sinusoids | 21.6 | 23.2 | n.s. |
| Early allograft dysfunction | 3 (8.8%) | 4 (30.1%) | p = 0.064 * |
| Primary non-function | 0 | 0 | n.s. |
| Graft failure (retransplantation) | 0 | 1 | n.s. |
| Recipients’ death | 1 | 1 | n.s |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vasuri, F.; Germinario, G.; Ciavarella, C.; Carroli, M.; Motta, I.; Valente, S.; Cescon, M.; D’Errico, A.; Pasquinelli, G.; Ravaioli, M. Trophism and Homeostasis of Liver Sinusoidal Endothelial Graft Cells during Preservation, with and without Hypothermic Oxygenated Perfusion. Biology 2022, 11, 1329. https://doi.org/10.3390/biology11091329
Vasuri F, Germinario G, Ciavarella C, Carroli M, Motta I, Valente S, Cescon M, D’Errico A, Pasquinelli G, Ravaioli M. Trophism and Homeostasis of Liver Sinusoidal Endothelial Graft Cells during Preservation, with and without Hypothermic Oxygenated Perfusion. Biology. 2022; 11(9):1329. https://doi.org/10.3390/biology11091329
Chicago/Turabian StyleVasuri, Francesco, Giuliana Germinario, Carmen Ciavarella, Michele Carroli, Ilenia Motta, Sabrina Valente, Matteo Cescon, Antonia D’Errico, Gianandrea Pasquinelli, and Matteo Ravaioli. 2022. "Trophism and Homeostasis of Liver Sinusoidal Endothelial Graft Cells during Preservation, with and without Hypothermic Oxygenated Perfusion" Biology 11, no. 9: 1329. https://doi.org/10.3390/biology11091329