
COVID-19 Severity and Androgen Receptor Polymorphism

 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
- -
- Any correlation between the length of CAG polymorphism in the androgen receptor and COVID-19 disease severity;
- -
- Any correlation between serum LH and total testosterone levels and COVID-19 disease severity.
2. Materials and Methods
2.1. Patients
- -
- Nasopharyngeal swab, positive for SARS-CoV-2 between July 2020 and January 2021;
- -
- Age between 18–70 years;
- -
- Andrological and/or systemic diseases that were capable of interfering with the gonadal hormone axis (autoimmune diseases, cardiovascular diseases, diabetes, etc.);
- -
- Genetic diseases;
- -
- Previous and/or current oncological disease and previous chemotherapy and/or radiotherapy treatments.
2.2. Genetic Analysis of Androgen Receptor Polymorphism
2.3. Hormone Evaluation
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scully, E.P.; Haverfield, J.; Ursin, R.L.; Tannenbaum, C.; Klein, S.L. Considering how biological sex impacts immune responses and COVID-19 outcomes. Nat. Rev. Immunol. 2020, 20, 442–447. [Google Scholar] [CrossRef]
- WHO. Coronavirus Disease 2019 (COVID-19): Situation Report, 72; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- Schurz, H.; Salie, M.; Tromp, G.; Hoal, E.G.; Kinnear, C.J.; Möller, M. The X chromosome and sex-specific effects in infectious disease susceptibility. Hum. Genom. 2019, 13, 2. [Google Scholar] [CrossRef] [Green Version]
- Tramontana, F.; Battisti, S.; Napoli, N.; Strollo, R. Immuno-Endocrinology of COVID-19: The Key Role of Sex Hormones. Front. Endocrinol. 2021, 12, 726696. [Google Scholar] [CrossRef]
- Trigunaite, A.; Dimo, J.; Jørgensen, T.N. Suppressive effects of androgens on the immune system. Cell. Immunol. 2015, 294, 87–94. [Google Scholar] [CrossRef]
- Lucas, J.M.; Heinlein, C.; Kim, T.; Hernandez, S.A.; Malik, M.S.; True, L.D.; Morrissey, C.; Corey, E.; Montgomery, B.; Mostaghel, E.; et al. The Androgen-Regulated Protease TMPRSS2 Activates a Proteolytic Cascade Involving Components of the Tumor Microenvironment and Promotes Prostate Cancer Metastasis. Cancer Discov. 2014, 4, 1310–1325. [Google Scholar] [CrossRef] [Green Version]
- Salciccia, S.; Del Giudice, F.; Gentile, V.; Mastroianni, C.M.; Pasculli, P.; Di Lascio, G.; Ciardi, M.R.; Sperduti, I.; Maggi, M.; De Berardinis, E.; et al. Interplay between male testosterone levels and the risk for subsequent invasive respiratory assistance among COVID-19 patients at hospital admission. Endocrine 2020, 70, 206–210. [Google Scholar] [CrossRef]
- Camici, M.; Zuppi, P.; Lorenzini, P.; Scarnecchia, L.; Pinnetti, C.; Cicalini, S.; Nicastri, E.; Petrosillo, N.; Palmieri, F.; D’Offizi, G.; et al. Role of testosterone in SARS-CoV-2 infection: A key pathogenic factor and a biomarker for severe pneumonia. Int. J. Infect. Dis. 2021, 108, 244–251. [Google Scholar] [CrossRef]
- Salonia, A.; Pontillo, M.; Capogrosso, P.; Gregori, S.; Tassara, M.; Boeri, L.; Carenzi, C.; Abbate, C.; Cignoli, D.; Ferrara, A.M.; et al. Severely low testosterone in males with COVID-19: A case-control study. Andrology 2021, 9, 1043–1052. [Google Scholar] [CrossRef]
- Cinislioglu, A.E.; Cinislioglu, N.; Demirdogen, S.O.; Sam, E.; Akkas, F.; Altay, M.S.; Utlu, M.; Sen, I.A.; Yildirim, F.; Kartal, S.; et al. The relationship of serum testosterone levels with the clinical course and prognosis of COVID-19 disease in male patients: A prospective study. Andrology 2021, 10, 24–33. [Google Scholar] [CrossRef]
- Rastrelli, G.; Di Stasi, V.; Inglese, F.; Beccaria, M.; Garuti, M.; Di Costanzo, D.; Spreafico, F.; Greco, G.F.; Cervi, G.; Pecoriello, A.; et al. Low testosterone levels predict clinical adverse outcomes in SARS-CoV-2 pneumonia patients. Andrology 2020, 9, 88–98. [Google Scholar] [CrossRef]
- Tan, M.H.E.; Li, J.; Xu, H.E.; Melcher, K.; Yong, E.-L. Androgen receptor: Structure, role in prostate cancer and drug discovery. Acta Pharmacol. Sin. 2015, 36, 3–23. [Google Scholar] [CrossRef] [Green Version]
- Davey, R.A.; Grossmann, M. Androgen Receptor Structure, Function and Biology: From Bench to Bedside. Clin. Biochem. Rev. 2016, 37, 3–15. [Google Scholar]
- Grassetti, D.; Giannandrea, F.; Paoli, D.; Masciandaro, P.; Figura, V.; Carlini, T.; Rizzo, F.; Lombardo, F.; Lenzi, A.; Gandini, L. Androgen receptor polymorphisms and testicular cancer risk. Andrology 2014, 3, 27–33. [Google Scholar] [CrossRef] [Green Version]
- Ferlin, A.; Bartoloni, L.; Rizzo, G.; Roverato, A.; Garolla, A.; Foresta, C. Androgen receptor gene CAG and GGC repeat lengths in idiopathic male infertility. Mol. Hum. Reprod. 2004, 10, 417–421. [Google Scholar] [CrossRef] [Green Version]
- Esteban, E.; Rodon, N.; Via, M.; González-Pérez, E.; Santamaria, J.; Dugoujon, J.-M.; El Chennawi, F.; Melhaoui, M.; Cherkaoui, M.; Vona, G.; et al. Androgen receptor CAG and GGC polymorphisms in Mediterraneans: Repeat dynamics and population relationships. J. Hum. Genet. 2005, 51, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Chamberlain, N.L.; Driver, E.D.; Miesfeld, R.L. The length and location of CAG trinucleotide repeats in the androgen receptor N-terminal domain affect transactivation function. Nucleic Acids Res. 1994, 22, 3181–3186. [Google Scholar] [CrossRef] [Green Version]
- Choong, C.S.; Kemppainen, J.A.; Zhou, Z.X.; Wilson, E.M. Reduced androgen receptor gene expression with first exon CAG repeat expansion. Mol. Endocrinol. 1996, 10, 1527–1535. [Google Scholar] [CrossRef] [Green Version]
- Afar, D.E.; Vivanco, I.; Hubert, R.S.; Kuo, J.; Chen, E.; Saffran, D.C.; Raitano, A.B.; Jakobovits, A. Catalytic cleavage of the androgen-regulated TMPRSS2 protease results in its secretion by prostate and prostate cancer epithelia. Cancer Res. 2001, 61, 1686–1692. [Google Scholar]
- Gu, J.; Han, B.; Wang, J. COVID-19: Gastrointestinal Manifestations and Potential Fecal–Oral Transmission. Gastroenterology 2020, 158, 1518–1519. [Google Scholar] [CrossRef]
- Mohamed, M.S.; Moulin, T.C.; Schiöth, H.B. Sex differences in COVID-19: The role of androgens in disease severity and progression. Endocrine 2021, 71, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Baldassarri, M.; Picchiotti, N.; Fava, F.; Fallerini, C.; Benetti, E.; Daga, S.; Valentino, F.; Doddato, G.; Furini, S.; Giliberti, A.; et al. Shorter androgen receptor polyQ alleles protect against life-threatening COVID-19 disease in European males. eBioMedicine 2021, 65, 103246. [Google Scholar] [CrossRef] [PubMed]
- McCoy, J.; Wambier, C.G.; Herrera, S.; Vaño-Galván, S.; Gioia, F.; Comeche, B.; Ron, R.; Serrano-Villar, S.; Iwasiow, R.M.; Tayeb, M.; et al. Androgen receptor genetic variant predicts COVID-19 disease severity: A prospective longitudinal study of hospitalized COVID-19 male patients. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e15–e17, Erratum in J. Eur. Acad. Dermatol. Venereol. 2021, 35, 1595. [Google Scholar] [CrossRef] [PubMed]
- WHO. COVID-19 Clinical Management Living Guidance 25 January 2021; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Pallotti, F.; Senofonte, G.; Pelloni, M.; Cargnelutti, F.; Carlini, T.; Radicioni, A.F.; Rossi, A.; Lenzi, A.; Paoli, D.; Lombardo, F. Androgenetic alopecia: Effects of oral finasteride on hormone profile, reproduction and sexual function. Endocrine 2020, 68, 688–694. [Google Scholar] [CrossRef]
- McCoy, J.; Wambier, C.; Vano-Galvan, S.; Shapiro, J.; Sinclair, R.; Ramos, P.; Washenik, K.; Andrade, M.; Herrera, S.; Goren, A. Racial variations in COVID-19 deaths may be due to androgen receptor genetic variants associated with prostate cancer and androgenetic alopecia. Are anti-androgens a potential treatment for COVID-19? J. Cosmet. Dermatol. 2020, 19, 1542–1543. [Google Scholar] [CrossRef]
- Ma, L.; Xie, W.; Li, D.; Shi, L.; Ye, G.; Mao, Y.; Xiong, Y.; Sun, H.; Zheng, F.; Chen, Z.; et al. Evaluation of sex-related hormones and semen characteristics in reproductive-aged male COVID-19 patients. J. Med. Virol. 2020, 93, 456–462. [Google Scholar] [CrossRef]
- Kaufman, J.-M.; Lapauw, B.; Mahmoud, A.; T’Sjoen, G.; Huhtaniemi, I.T. Aging and the Male Reproductive System. Endocr. Rev. 2019, 40, 906–972. [Google Scholar] [CrossRef]
- García-Rojo, E.; Manfredi, C.; Santos-Pérez-De-La-Blanca, R.; Tejido-Sánchez, Á.; García-Gómez, B.; Aliaga-Benítez, M.; Romero-Otero, J.; Rodriguez-Antolín, A. Impact of COVID-19 outbreak on urology surgical waiting lists and waiting lists prioritization strategies in the Post-COVID-19 era. Actas Urol. Esp. 2021, 45, 207–214. [Google Scholar] [CrossRef]
- Motlagh, R.S.; Abufaraj, M.; Karakiewicz, P.I.; Rajwa, P.; Mori, K.; Mun, D.-H.; Shariat, S.F. Association between SARS-CoV-2 infection and disease severity among prostate cancer patients on androgen deprivation therapy: A systematic review and meta-analysis. World J. Urol. 2021, 40, 907–914. [Google Scholar] [CrossRef]
- Welén, K.; Rosendal, E.; Gisslén, M.; Lenman, A.; Freyhult, E.; Fonseca-Rodríguez, O.; Bremell, D.; Stranne, J.; Balkhed, Å.Ö.; Niward, K.; et al. A Phase 2 Trial of the Effect of Antiandrogen Therapy on COVID-19 Outcome: No Evidence of Benefit, Supported by Epidemiology and In Vitro Data. Eur. Urol. 2021, 81, 285–293. [Google Scholar] [CrossRef]
- Meng, J.; Ge, Q.; Li, J.; Lu, X.; Chen, Y.; Wang, H.; Zhang, M.; Du, J.; Zhang, L.; Hao, Z.; et al. Protective trend of anti-androgen therapy during the COVID-19 pandemic: A meta-analysis. J. Infect. 2022, 84, 834–872. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
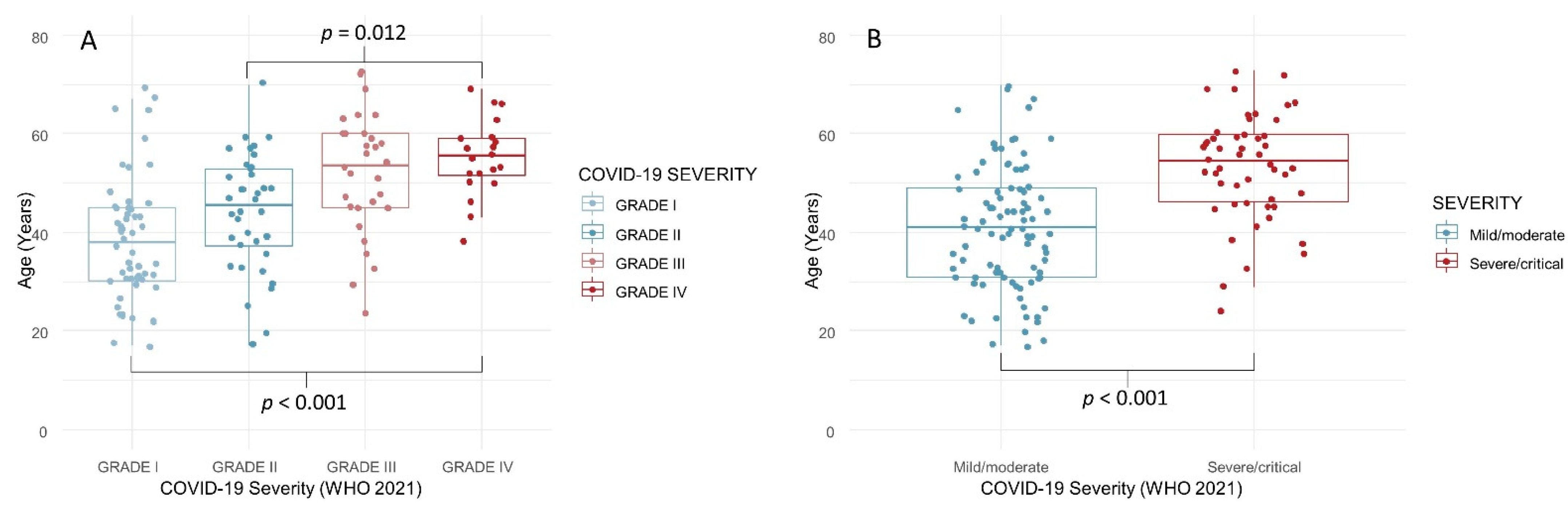
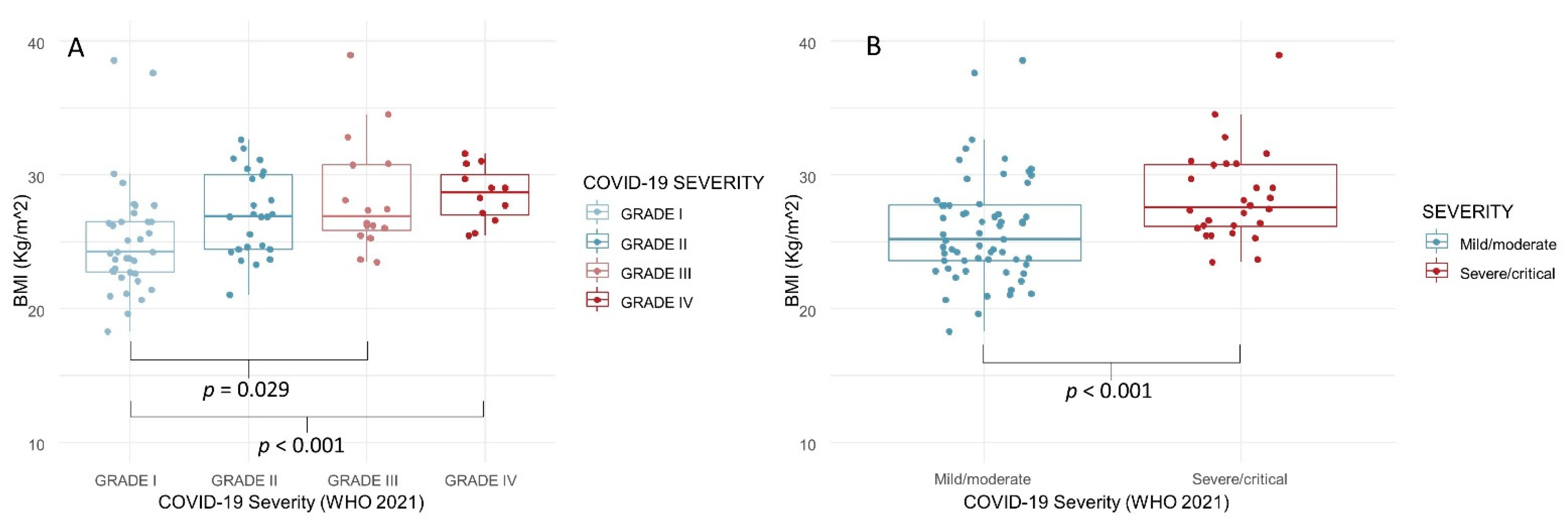
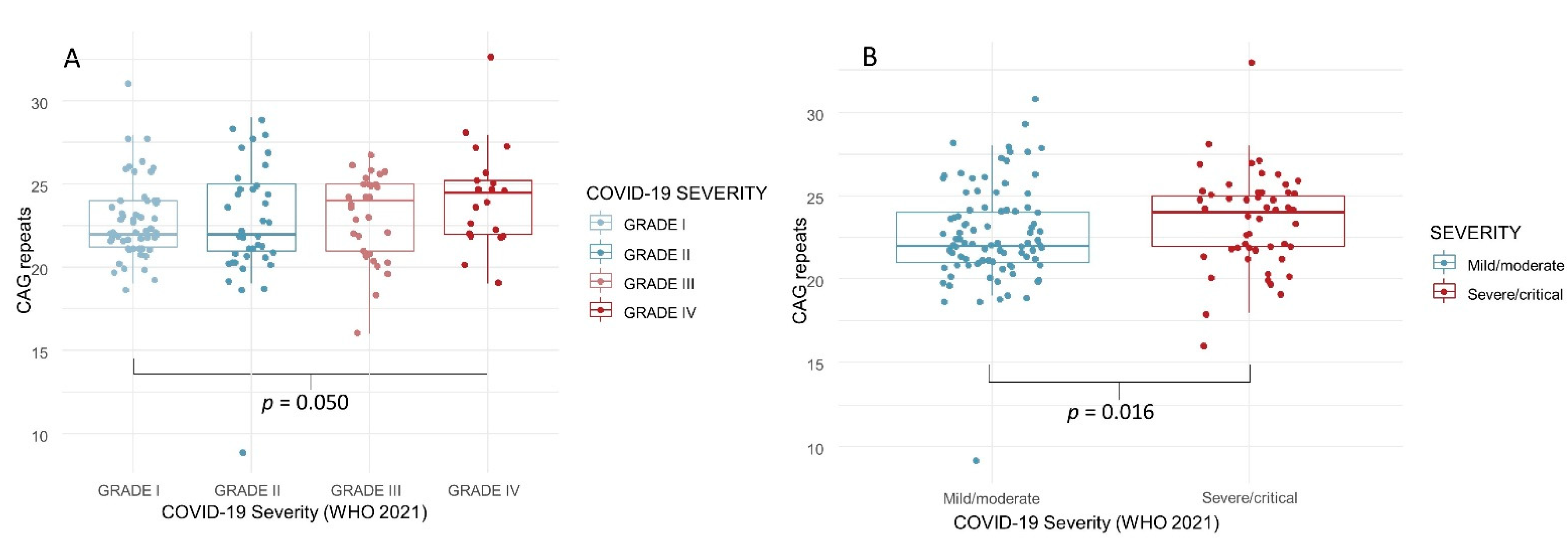
| Age (Years) | BMI (Kg/m2) | CAG Repeats | LH (mIU/mL) | Total Testosterone (nmol/L) | LH/TT Ratio | |
|---|---|---|---|---|---|---|
| Grade I | 38.4 ± 12.5 | 25.1 ± 4.2 | 22.8 ± 2.3 | 4.1 ± 1.9 | 19.0 ± 7.1 | 0.25 ± 0.14 |
| 38.0 | 24.2 | 22.0 | 4.0 | 18.2 | 0.22 | |
| (30.0–45.0) | (22.7–26.5) | (21.0–24.0) | (3.0–5.1) | (14.1–22.5) | (0.14–0.33) | |
| Grade II | 44.2 ± 11.7 | 27.1 ± 3.1 | 22.6 ± 3.6 | 3.4 ± 3.2 | 19.5 ± 8.4 | 0.18 ± 0.11 |
| 45.5 | 26.9 | 22.0 | 3.0 | 16.8 | 0.16 | |
| (37.0–53.0) | (24.4–30.0) | (21.0–25.0) | (1.9–3.9) | (13.8–24.4) | (0.10–0.19) | |
| Grade III | 52.0 ± 12.3 | 28.3 ± 4.2 | 23.0 ± 2.7 | 4.5 ± 3.4 | 16.1 ± 7.3 | 0.32 ± 0.25 |
| 53.5 | 26.9 | 24.0 | 3.5 | 15.0 | 0.24 | |
| (45.0–60.0) | (25.7–30.8) | (21.0–25.0) | (2.6–5.4) | (10.5–19.0) | (0.16–0.39) | |
| Grade IV | 55.1 ± 7.8 | 30.3 ± 5.0 | 24.3 ± 3.1 | 3.9 ± 2.6 | 16.1 ± 6.0 | 0.26 ± 0.14 |
| 55.0 | 29.0 | 24.5 | 3.1 | 14.3 | 0.15 | |
| (51.0–59.0) | (27.2–31.0) | (22.0–25.5) | (2.3–4.6) | (11.4–19.6) | (0.21–0.34) | |
| p-value | <0.001 | 0.002 | 0.050 | 0.055 | 0.435 | 0.156 |
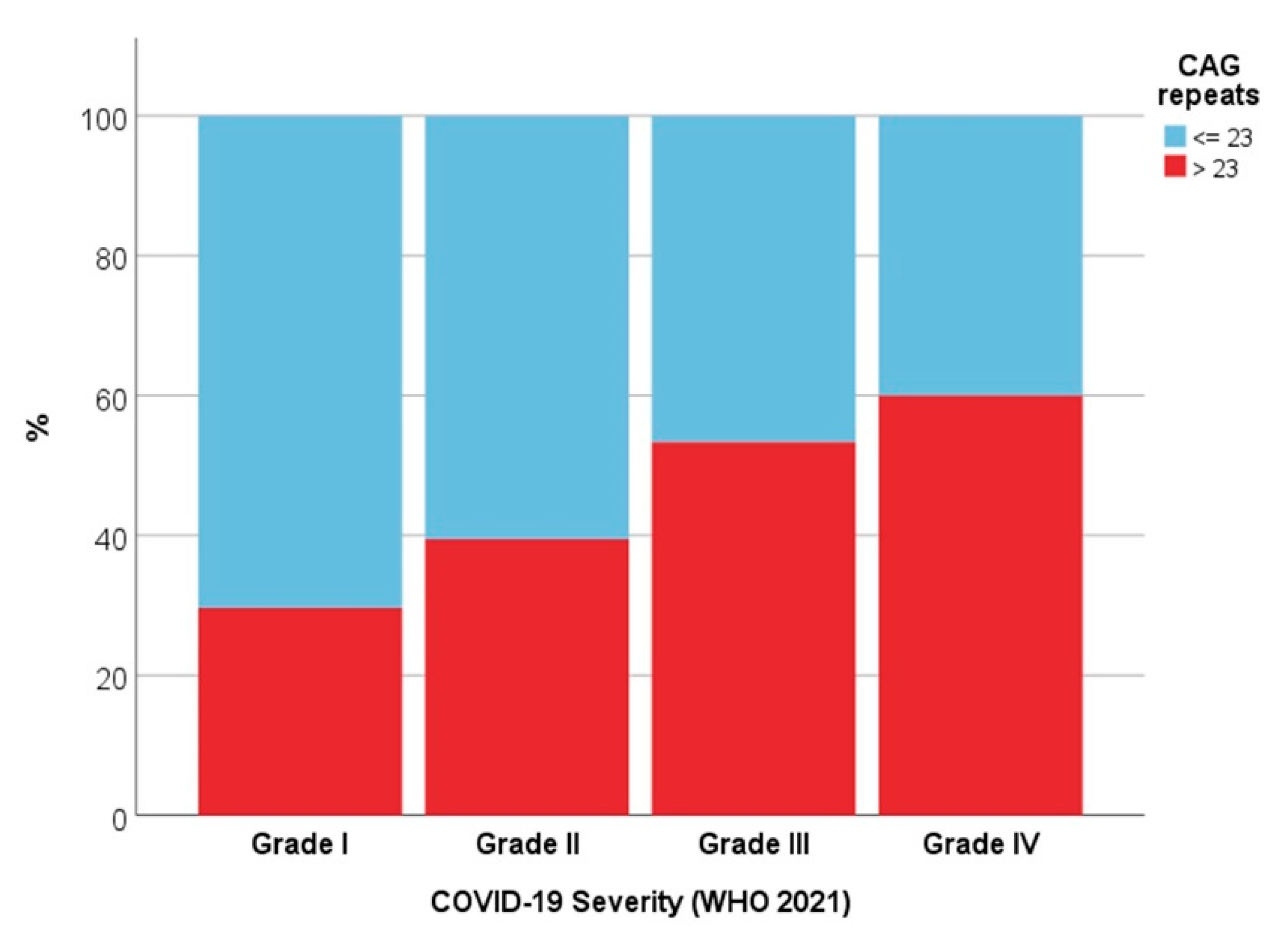
| OR | 95% CI | p Value | ||
|---|---|---|---|---|
| Grade I | CAG repeats ≤ 23 | 3.56 | 1.22–10.37 | 0.020 |
| Grade II | CAG repeats ≤ 23 | 2.30 | 0.76–6.95 | 0.140 |
| Grade III | CAG repeats ≤ 23 | 1.31 | 0.42–4.13 | 0.642 |
| Grade IV * | CAG repeats ≤ 23 | // | // | // |
| Papers | COVID-19 Severity | N. AR CAG Repeats |
|---|---|---|
| McCoy et al., 2021 | Severe | ≥22 |
| Baldassarri et al., 2021 | Severe | ≥23 |
| Present study, 2022 | Severe | >23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buonacquisto, A.; Conflitti, A.C.; Pallotti, F.; Anzuini, A.; Bianchini, S.; Caponecchia, L.; Carraro, A.; Ciardi, M.R.; Faja, F.; Fiori, C.; et al. COVID-19 Severity and Androgen Receptor Polymorphism. Biology 2022, 11, 974. https://doi.org/10.3390/biology11070974
Buonacquisto A, Conflitti AC, Pallotti F, Anzuini A, Bianchini S, Caponecchia L, Carraro A, Ciardi MR, Faja F, Fiori C, et al. COVID-19 Severity and Androgen Receptor Polymorphism. Biology. 2022; 11(7):974. https://doi.org/10.3390/biology11070974
Chicago/Turabian StyleBuonacquisto, Alessandra, Anna Chiara Conflitti, Francesco Pallotti, Antonella Anzuini, Serena Bianchini, Luisa Caponecchia, Anna Carraro, Maria Rosa Ciardi, Fabiana Faja, Cristina Fiori, and et al. 2022. "COVID-19 Severity and Androgen Receptor Polymorphism" Biology 11, no. 7: 974. https://doi.org/10.3390/biology11070974