
Tensiomyography Allows to Discriminate between Injured and Non-Injured Biceps Femoris Muscle


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Measurement Procedures
2.3. Experimental Design
2.4. Variables
2.5. Statistical Analysis
3. Results
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Verrall, G.; Dolman, B. Deducing a mechanism of all musculoskeletal injuries. Muscles Ligaments Tendons J. 2019, 6, 174. [Google Scholar] [CrossRef]
- Valle, X.; Alentorn-Geli, E.; Tol, J.L.; Hamilton, B.; Garrett, W.; Pruna, R.; Til, L.; Gutierrez, J.A.; Alomar, X.; Balius, R.; et al. Muscle injuries in sports: A new evidence-informed and expert consensus-based classification with clinical application. Sports Med. 2016, 47, 1241–1253. [Google Scholar] [CrossRef] [Green Version]
- Lundblad, M.; Waldén, M.; Magnusson, H.; Karlsson, J.; Ekstrand, J. The UEFA injury study: 11-year data concerning 346 MCL injuries and time to return to play. Br. J. Sports Med. 2013, 47, 759–762. [Google Scholar] [CrossRef]
- Petersen, J. Evidence based prevention of hamstring injuries in sport. Br. J. Sports Med. 2005, 39, 319–323. [Google Scholar] [CrossRef]
- Askling, C.M.; Tengvar, M.; Saartok, T.; Thorstensson, A. Acute First-Time hamstring strains during High-Speed running. Am. J. Sports Med. 2007, 35, 197–206. [Google Scholar] [CrossRef]
- Ekstrand, J.; Healy, J.C.; Waldén, M.; Lee, J.C.; English, B.; Hägglund, M. Hamstring muscle injuries in professional football: The correlation of MRI findings with return to play. Br. J. Sport. Med. 2011, 46, 112–117. [Google Scholar] [CrossRef] [Green Version]
- Fyfe, J.J.; Opar, D.A.; Williams, M.D.; Shield, A.J. The role of neuromuscular inhibition in hamstring strain injury recurrence. J. Electromyogr. Kinesiol. 2013, 23, 523–530. [Google Scholar] [CrossRef] [Green Version]
- Opar, D.A.; Williams, M.D.; Shield, A.J. Hamstring strain injuries. Sports Med. 2012, 42, 209–226. [Google Scholar] [CrossRef]
- Silder, A.; Heiderscheit, B.C.; Thelen, D.G.; Enright, T.; Tuite, M.J. MR observations of long-term musculotendon remodeling following a hamstring strain injury. Skelet. Radiol. 2008, 37, 1101–1109. [Google Scholar] [CrossRef] [Green Version]
- Schache, A.G.; Dorn, T.W.; Blanch, P.D.; Brown, N.A.T.; Pandy, M.G. Mechanics of the human hamstring muscles during sprinting. Med. Sci. Sport Exerc. 2012, 44, 647–658. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, B.; Valle, X.; Rodas, G.; Til, L.; Grive, R.P.; Gutierrez Rincon, J.A.; Tol, J.L. Classification and grading of muscle injuries: A narrative review. Br. J. Sports Med. 2015, 49, 306. [Google Scholar] [CrossRef] [Green Version]
- Maffulli, N.; Del Buono, A.; Oliva, F.; Giai Via, A.; Frizziero, A.; Barazzuol, M.; Brancaccio, P.; Freschi, M.; Galletti, S.; Lisitano, G.; et al. Muscle injuries: A brief guide to classification and management. Transl. Med. UniSa 2015, 12, 14–18. [Google Scholar]
- Pollock, N.; James, S.L.J.; Lee, J.C.; Chakraverty, R. British athletics muscle injury classification: A new grading system. Br. J. Sports Med. 2014, 48, 1347–1351. [Google Scholar] [CrossRef] [Green Version]
- Wangensteen, A.; Almusa, E.; Boukarroum, S.; Farooq, A.; Hamilton, B.; Whiteley, R.; Bahr, R.; Tol, J.L. MRI does not add value over and above patient history and clinical examination in predicting time to return to sport after acute hamstring injuries: A prospective cohort of 180 male athletes. Br. J. Sports Med. 2015, 49, 1579–1587. [Google Scholar] [CrossRef]
- Dolman, B.; Verrall, G.; Reid, I. Physical principles demonstrate that the biceps femoris muscle relative to the other hamstring muscles exerts the most force: Implications for hamstring muscle strain injuries. Muscles Ligaments Tendons J. 2014, 4, 371–377. [Google Scholar] [CrossRef]
- Hallén, A.; Ekstrand, J. Return to play following muscle injuries in professional footballers. J. Sports Sci. 2014, 32, 1229–1236. [Google Scholar] [CrossRef]
- Opar, D.A.; Williams, M.D.; Timmins, R.G.; Hickey, J.; Duhig, S.J.; Shield, A.J. Eccentric hamstring strength and hamstring injury risk in Australian footballers. Med. Sci. Sports Exerc. 2015, 47, 857–865. [Google Scholar] [CrossRef] [Green Version]
- Moen, M.H.; Reurink, G.; Weir, A.; Tol, J.L.; Maas, M.; Goudswaard, G.J. Predicting return to play after hamstring injuries. Br. J. Sports Med. 2014, 48, 1358–1363. [Google Scholar] [CrossRef] [Green Version]
- Tol, J.L.; Hamilton, B.; Eirale, C.; Muxart, P.; Jacobsen, P.; Whiteley, R. At return to play following hamstring injury the majority of professional football players have residual isokinetic deficits. Br. J. Sports Med. 2014, 48, 1364–1369. [Google Scholar] [CrossRef]
- Askling, C.M.; Tengvar, M.; Tarassova, O.; Thorstensson, A. Acute hamstring injuries in Swedish elite sprinters and jumpers: A prospective randomised controlled clinical trial comparing two rehabilitation protocols. Br. J. Sports Med. 2014, 48, 532–539. [Google Scholar] [CrossRef]
- Barry, D. Acoustic signals from frog skeletal muscle. Biophys. J. 1987, 51, 769–773. [Google Scholar] [CrossRef] [Green Version]
- Cè, E.; Rampichini, S.; Venturelli, M.; Limonta, E.; Veicsteinas, A.; Esposito, F. Electromechanical delay components during relaxation after voluntary contraction: Reliability and effects of fatigue. Muscle Nerve 2015, 51, 907–915. [Google Scholar] [CrossRef]
- Cè, E.; Rampichini, S.; Esposito, F. Novel insights into skeletal muscle function by mechanomyography: From the laboratory to the field. Sport Sci. Health 2015, 11, 1–28. [Google Scholar] [CrossRef]
- Cole, N.; Barry, D. Muscle sound frequencies of the frog are modulated by skeletal muscle tension. Biophys. J. 1994, 66, 1104–1114. [Google Scholar] [CrossRef] [Green Version]
- Hatta, I.; Sugi, H.; Tamura, Y. Stiffness changes in frog skeletal muscle during contraction recorded using ultrasonic waves. J. Physiol. 1988, 403, 193–209. [Google Scholar] [CrossRef]
- Orizio, C.; Baratta, R.V.; Zhou, B.H.; Solomonow, M.; Veicsteinas, A. Force and surface mechanomyogram frequency responses in cat gastrocnemius. J. Biomech. 2000, 33, 427–433. [Google Scholar] [CrossRef]
- Orizio, C.; Perini, R.; Veicsteinas, A. Muscular sound and force relationship during isometric contraction in man. Eur. J. Appl. Physiol. Occup. Physiol. 1989, 58, 528–533. [Google Scholar] [CrossRef]
- Oster, G.; Jaffe, J. Low frequency sounds from sustained contraction of human skeletal muscle. Biophys. J. 1980, 30, 119–127. [Google Scholar] [CrossRef] [Green Version]
- Ibitoye, M.O.; Hamzaid, N.A.; Zuniga, J.M.; Wahab, A.K.A. Mechanomyography and muscle function assessment: A review of current state and prospects. Clin. Biomech. 2014, 29, 691–704. [Google Scholar] [CrossRef]
- Islam, M.A.; Sundaraj, K.; Ahmad, R.B.; Ahamed, N.U. Mechanomyogram for muscle function assessment: A Review. PLoS ONE 2013, 8, e58902. [Google Scholar] [CrossRef]
- Orizio, C.; Liberati, D.; Locatelli, C.; Grandis, D.D.; Veicsteinas, A. Surface mechanomyogram reflects muscle fibers twitches summation. J. Biomech. 1996, 29, 475–481. [Google Scholar] [CrossRef]
- Dahmane, R.; Djordjevič, S.; Šimunič, B.; Valenčič, V. Spatial fiber type distribution in normal human muscle. J. Biomech. 2005, 38, 2451–2459. [Google Scholar] [CrossRef]
- Dahmane, R.; Valenčič, V.; Knez, N.; Eržen, I. Evaluation of the ability to make non-invasive estimation of muscle contractile properties on the basis of the muscle belly response. Med. Biol. Eng. Comput. 2001, 39, 51–55. [Google Scholar] [CrossRef]
- Morales-Artacho, A.J.; Padial, P.; Rodríguez-Matoso, D.; Rodríguez-Ruiz, D.; García-Ramos, A.; García-Manso, J.M.; Calderón, C.; Feriche, B. Assessment of muscle contractile properties at acute moderate altitude through tensiomyography. High Alt. Med. Biol. 2015, 16, 343–349. [Google Scholar] [CrossRef]
- Šimunič, B.; Degens, H.; Rittweger, J.; Narici, M.; Mekjavić, I.B.; Pišot, R. Noninvasive estimation of myosin heavy chain composition in human skeletal muscle. Med. Sci. Sport Exerc. 2011, 43, 1619–1625. [Google Scholar] [CrossRef] [Green Version]
- Valenčič, V.; Knez, N. Measuring of skeletal muscles dynamic properties. Artif. Organs 1997, 21, 240–242. [Google Scholar] [CrossRef]
- Ditroilo, M.; Smith, I.J.; Fairweather, M.M.; Hunter, A.M. Long-term stability of tensiomyography measured under different muscle conditions. J. Electromyogr. Kinesiol. 2013, 23, 558–563. [Google Scholar] [CrossRef]
- Šimunič, B. Between-day reliability of a method for non-invasive estimation of muscle composition. J. Electromyogr. Kinesiol. 2012, 22, 527–530. [Google Scholar] [CrossRef]
- Tous-Fajardo, J.; Moras, G.; Rodríguez-Jiménez, S.; Usach, R.; Doutres, D.M.; Maffiuletti, N.A. Inter-rater reliability of muscle contractile property measurements using non-invasive tensiomyography. J. Electromyogr. Kinesiol. 2010, 20, 761–766. [Google Scholar] [CrossRef]
- Martín-Rodríguez, S.; Loturco, I.; Hunter, A.M.; Rodríguez-Ruiz, D.; Munguia-Izquierdo, D. Reliability and measurement error of tensiomyography to assess mechanical muscle function. J. Strength. Cond. Res. 2017, 31, 3524–3536. [Google Scholar] [CrossRef]
- Lohra, C.; Schmidt, T.; Medina-Porquerese, I.; Braumanna, K.-M.; Reera, R.; Porthun, J. Diagnostic accuracy, validity, and reliability of Tensiomyography to assess muscle function and exercise-induced fatigue in healthy participants. A systematic review with meta-analysis. J. Electromyogr. Kinesiol. 2019, 47, 65–87. [Google Scholar] [CrossRef] [PubMed]
- Hanley, J.A.; McNeil, B.J. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology 1983, 148, 839–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delong, E.R.; Delong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated Receiver Operating Characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.I.C. The effect of class imbalance on Precision-Recall Curves. Neural Comput. 2021, 33, 853–857. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Hedo, R.; Rivera, A.; Rull, R.; Richardson, S.; Tu, X.M. Post hoc power analysis: Is it an informative and meaningful analysis? General Psychiatry 2019, 32, e100069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lieber, R.L.; Fridén, J. Mechanisms of muscle injury gleaned from animal models. Am. J. Phys. Med. Rehab. 2002, 81, S70–S79. [Google Scholar] [CrossRef]
- Kujala, U.M.; Orava, S.; Järvinen, M. Hamstring injuries. Sports Med. 1997, 23, 397–404. [Google Scholar] [CrossRef]
- Ekstrand, J.; Hagglund, M.; Walden, M. Epidemiology of muscle injuries in professional football (soccer). Am. J. Sports Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef] [Green Version]
- Huygaerts, S.; Cos, F.; Cohen, D.D.; Calleja-González, J.; Guitart, M.; Blazevich, A.J.; Alcaraz, P.E. Mechanisms of hamstring strain injury: Interactions between fatigue, muscle activation and function. Sports 2020, 8, 65. [Google Scholar] [CrossRef]
- Marshall, P.W.; Lovell, R.; Jeppesen, G.K.; Andersen, K.; Siegler, J.C. Hamstring muscle fatigue and central motor output during a simulated soccer match. PLoS ONE 2014, 9, e102753. [Google Scholar] [CrossRef] [Green Version]
- Timmins, R.G.; Opar, D.A.; Williams, M.D.; Schache, A.G.; Dear, N.M.; Shield, A.J. Reduced biceps femoris myoelectrical activity influences eccentric knee flexor weakness after repeat sprint running. Scand. J. Med. Sci. Sports 2014, 24, e299–e305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friden, J.; Lieber, R.L. Structural and mechanical basis of exercise-induced muscle injury. Med. Sci. Sports Exerc. 1992, 24, 521–530. [Google Scholar] [CrossRef] [PubMed]
- Mori, T.; Agata, N.; Itoh, Y.; Miyazu-Inoue, M.; Sokabe, M.; Taguchi, T.; Kawakami, K. Stretch speed-dependent myofiber damage and functional deficits in rat skeletal muscle induced by lengthening contraction. Physiol. Rep. 2014, 2, e12213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, S.J. Differential susceptibility on myosin heavy chain isoform following eccentric-induced muscle damage. J. Exerc. Rehabil. 2014, 10, 344–348. [Google Scholar] [CrossRef] [Green Version]
- Mendez-Villanueva, A.; Nuñez, F.J.; Lazaro-Ramirez, J.L.; Rodriguez-Sanchez, P.; Guitart, M.; Rodas, G.; Martin-Garetxana, I.; Lekue, J.; Di Salvo, V.; Suarez-Arrones, L. Knee flexor eccentric strength, hamstring muscle volume and sprinting in elite professional soccer players with a prior strained hamstring. Biology 2022, 11, 69. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Female Non-Injured | ||||||||
|---|---|---|---|---|---|---|---|---|
| Td L (ms) | Td R (ms) | p-Value | Tc L (ms) | Tc R (ms) | p-Value | Dm L (mm) | Dm R (mm) | p-Value |
| 23.1 ± 2.7 | 22.9 ± 2.1 | 0.466 | 23.9 ± 4.6 | 23.7 ± 3.7 | 0.736 | 4.1 ± 1.3 | 4.2 ± 1.2 | 0.327 |
| Male Non-injured | ||||||||
| 22.6 ± 2.2 | 22.7 ± 2.1 | 0.608 | 24.9 ± 4.8 | 25.0 ± 5.1 | 0.897 | 5.0 ± 2.0 | 5.1 ± 1.9 | 0.411 |
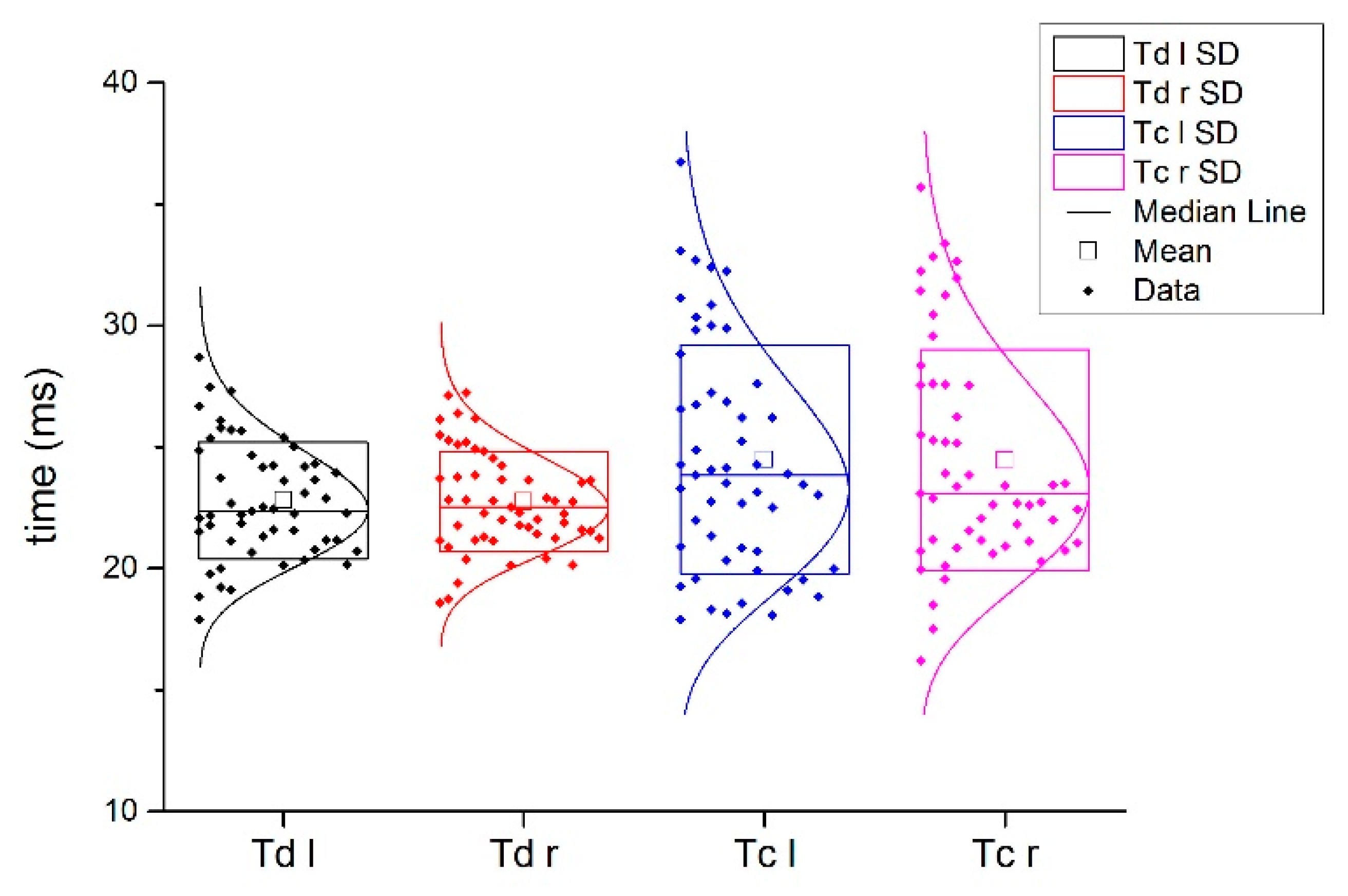
| Injured subjects | Non-injured subjects | |||||||
| Td ni (ms) | Td in (ms) | p-value | Td L (ms) | Td R (ms) | p-value | |||
| 23.1 ± 2.3 | 25.0 ± 3.6 | <0.001 | 22.8 ± 2.4 | 22.8 ± 2.1 | 0.819 | |||
| Tc ni (ms) | Tc in (ms) | p-value | Tc L (ms) | Tc R (ms) | p-value | |||
| 24.6 ± 5.1 | 32.9 ± 8.5 | <0.001 | 24.5 ± 4.7 | 24.5 ± 4.5 | 0.882 | |||
| Dm ni (mm) | Dm in (mm) | p-value | Dm L (mm) | Dm R (mm) | p-value | |||
| 4.9 ± 1.8 | 5.0 ± 1.9 | 0.683 | 4.6 ± 1.8 | 4.8 ± 1.7 | 0.227 | |||
| fTd ni (ms) | mTd ni (ms) | p-value | fTd L (ms) | mTd R (ms) | p-value | |||
| 25.4 ± 3.8 | 24.8 ± 3.6 | 0.514 | 23.1 ± 2.9 | 23.1 ± 1.7 | 0.995 | |||
| fTc ni (ms) | mTc ni (ms) | p-value | fTc L (ms) | mTc R (ms) | p-value | |||
| 31.5 ± 7.6 | 33.9 ± 9.0 | 0.303 | 25.1 ± 5.9 | 24.2 ± 4.4 | 0.534 | |||
| fDm ni (mm) | mDm ni (mm) | p-value | fDm L (mm) | mDm R (mm) | p-value | |||
| 4.5 ± 2.0 | 5.4 ± 1.8 | 0.085 | 4.5 ± 1.9 | 5.2 ± 1.7 | 0.156 | |||
| Non-injured group Female vs. Male | ||||||||
| fTd-L-ni | mTd-L-ni | p-value | fTc-L-ni | mTc-L-ni | p-value | fDm-L-ni | mDm-L-ni | p-value |
| 23.1 ± 2.8 | 22.6 ± 2.2 | 0.464 | 23.9 ± 4.6 | 24.9 ± 4.8 | 0.406 | 4.1 ± 1.3 | 5.0 ± 2.0 | 0.049 |
| fTd-R-ni | mTd-R-ni | data | fTc-R-ni | mTc-R-ni | data | fDm-R-ni | mDm-R-ni | data |
| 22.9 ± 2.1 | 22.7 ± 2.1 | 0.746 | 23.7 ± 3.7 | 25.0 ± 5.1 | 0.298 | 4.2 ± 1.2 | 5.1 ± 1.9 | 0.035 |
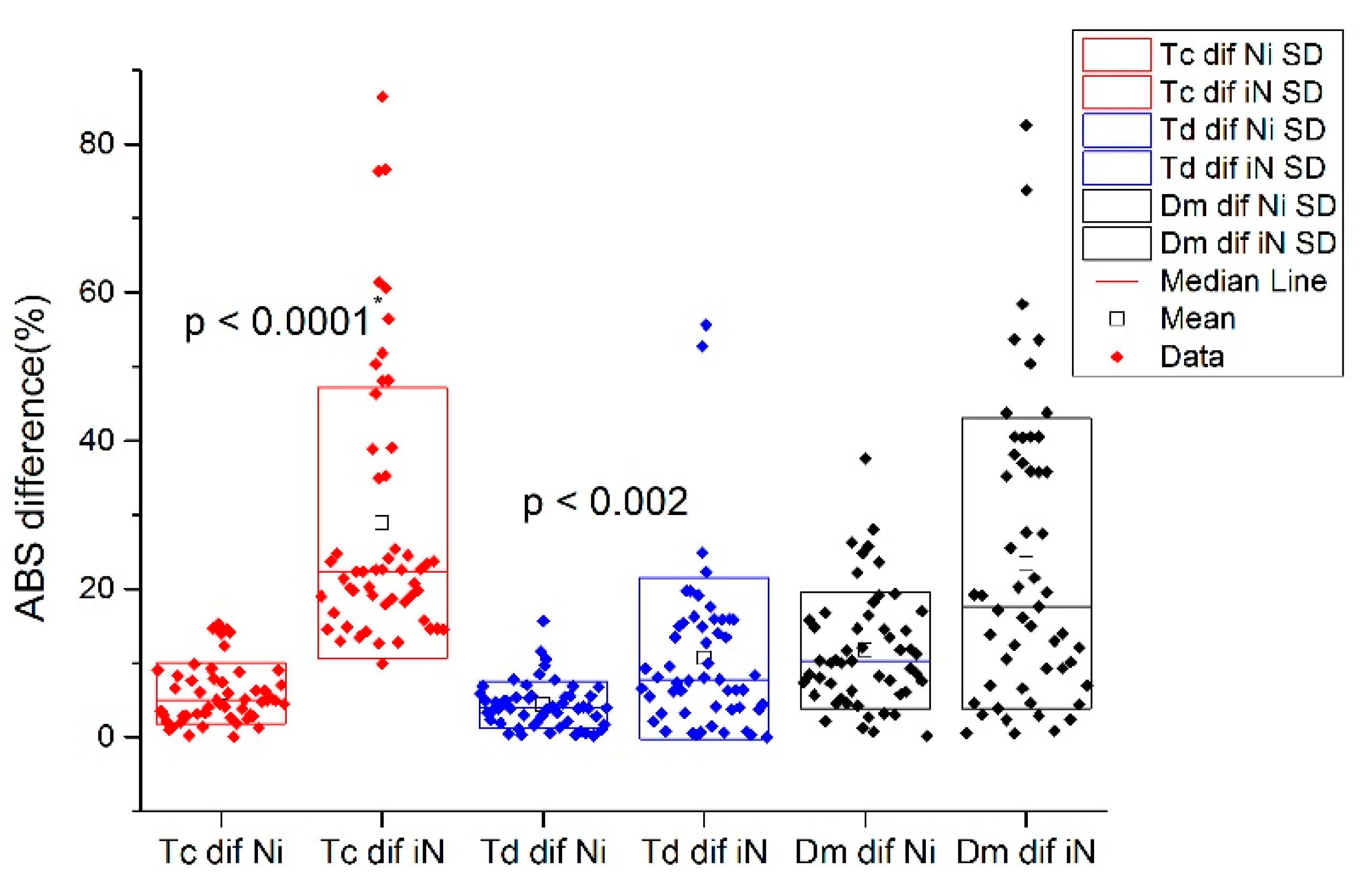
| Absolute Differences between Injured vs. Non-Injured BF | ||||
|---|---|---|---|---|
| Variables | in (%) | ni (%) | χ2 | p-Value |
| Td diff | 7.80 | 3.93 | 14.21 | <0.001 |
| Tc diff | 22.37 | 5.05 | 72.93 | <0.001 |
| Dm diff | 17.63 | 10.27 | 8.58 | <0.001 |
| Absolute Differences Between Injured vs. Non-injured BF in Males | ||||
| mTd diff | 6.35 | 3.93 | 9.12 | <0.001 |
| mTc diff | 23.43 | 4.96 | 43.69 | <0.001 |
| mDm diff | 14.02 | 10.33 | 1.81 | 0.179 |
| Absolute Differences Between Injured vs. Non-injured BF in Females | ||||
| fTd diff | 11.37 | 3.98 | 5.52 | 0.019 |
| fTc diff | 21.32 | 5.09 | 28.39 | <0.001 |
| fDm diff | 19.91 | 10.18 | 8.34 | <0.001 |
| Injury Differences in Female vs. Male Subgroups | ||||
| F in | M in | χ2 | p-value | |
| Td diff | 11.37 | 6.35 | 1.02 | 0.312 |
| Tc diff | 21.32 | 23.43 | 2.76 | 0.097 |
| Dm diff | 19.91 | 14.02 | 1.42 | 0.233 |
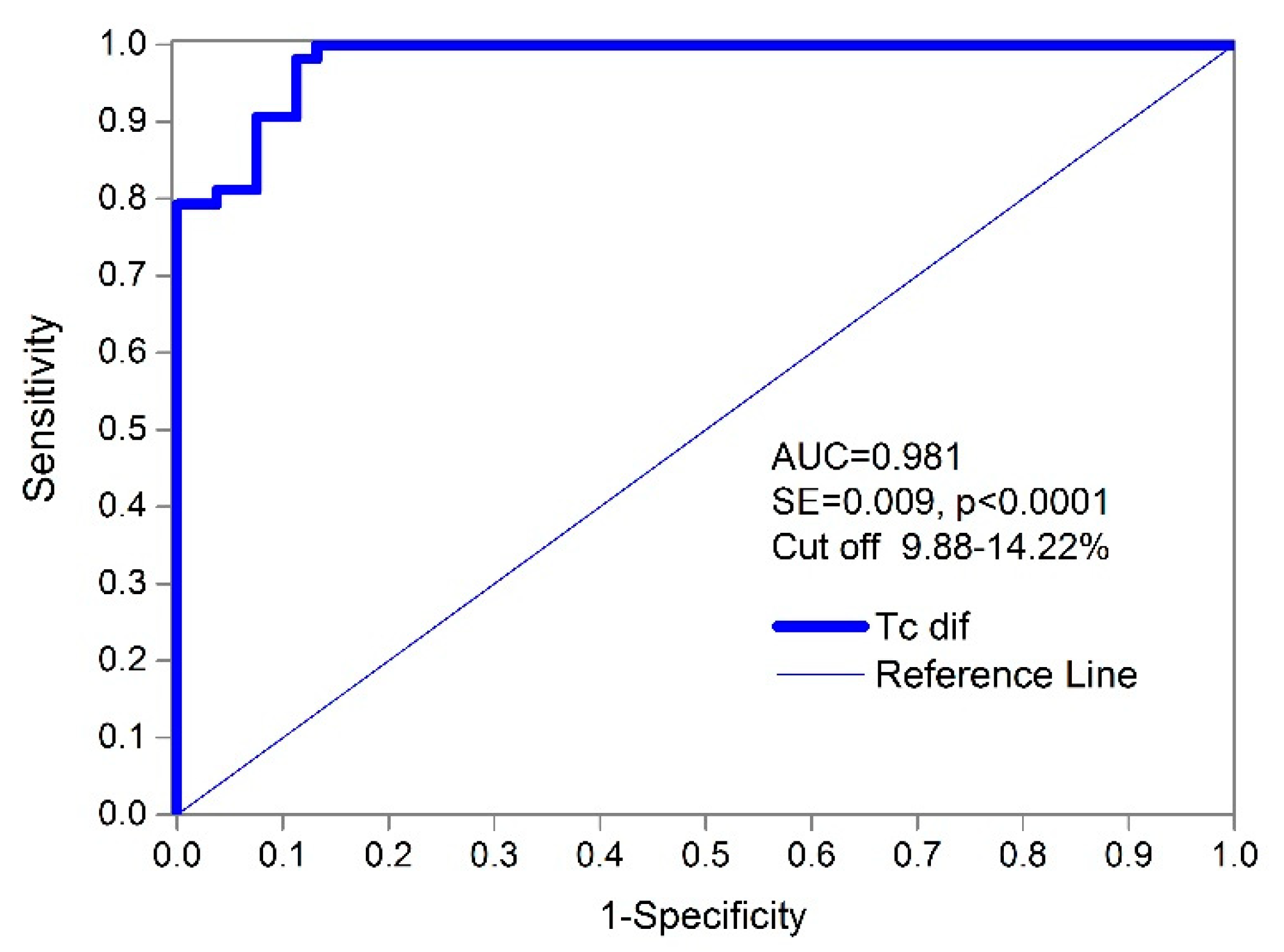
| Females—Injured vs. Non-Injured | Males—Injured vs. Non-Injured | Summarized F + M | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | Dm | Tc | Td | Dm | Tc | Td | Dm | Tc | Td |
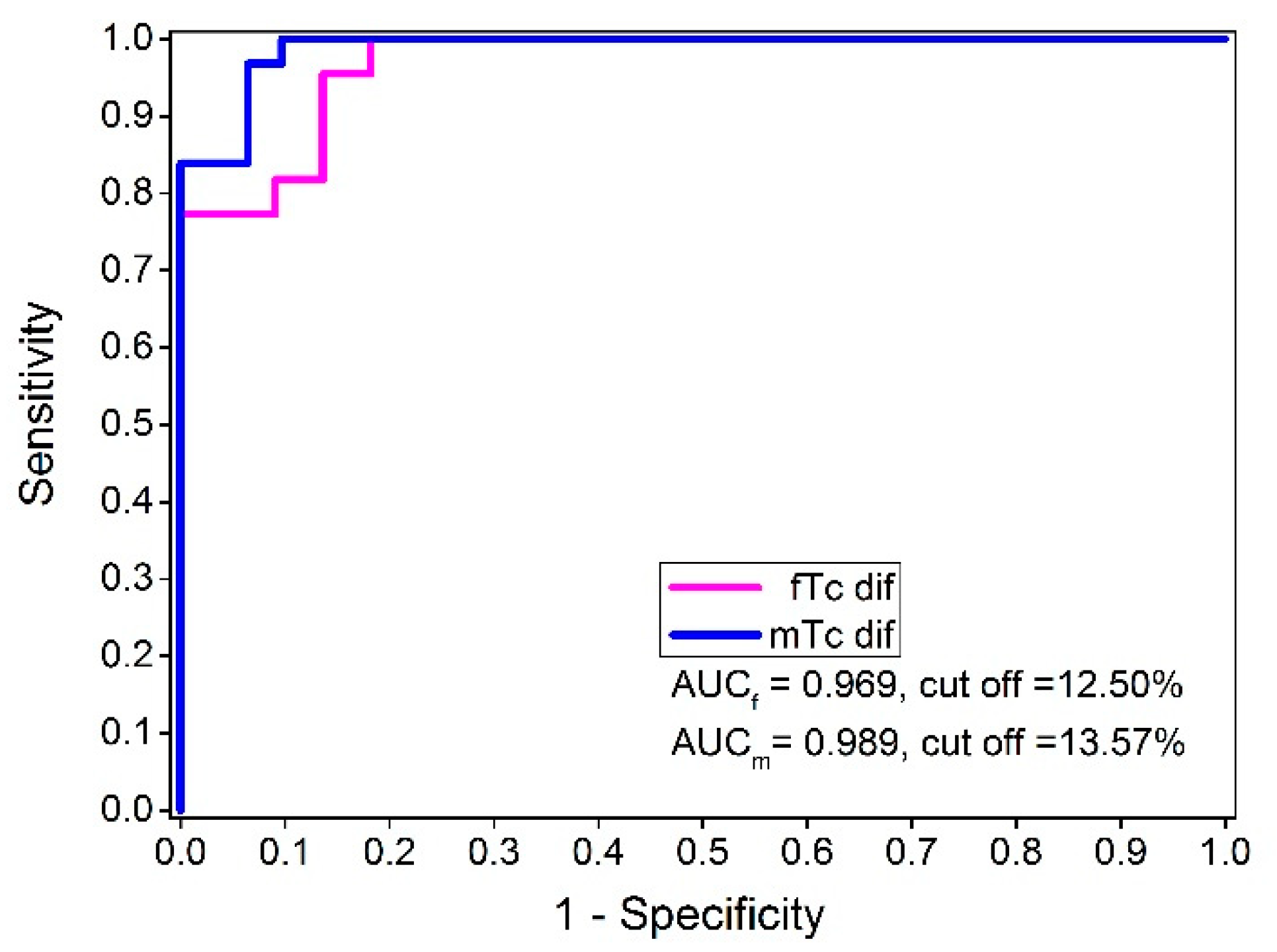
| AUC | 0.754 | 0.969 | 0.707 | 0.599 | 0.989 | 0.723 | 0.665 | 0.981 | 0.712 |
| St. Err. | 0.076 | 0.021 | 0.086 | 0.076 | 0.009 | 0.068 | 0.055 | 0.009 | 0.052 |
| 95% CI | 0.60–0.87 | 0.87–0.98 | 0.55–0.83 | 0.47–0.72 | 0.92–1.00 | 0.59–0.83 | 0.57–0.75 | 0.93–0.99 | 0.62–0.80 |
| p value | 0.001 | <0.001 | 0.016 | 0.192 | <0.001 | <0.001 | 0.003 | <0.001 | <0.001 |
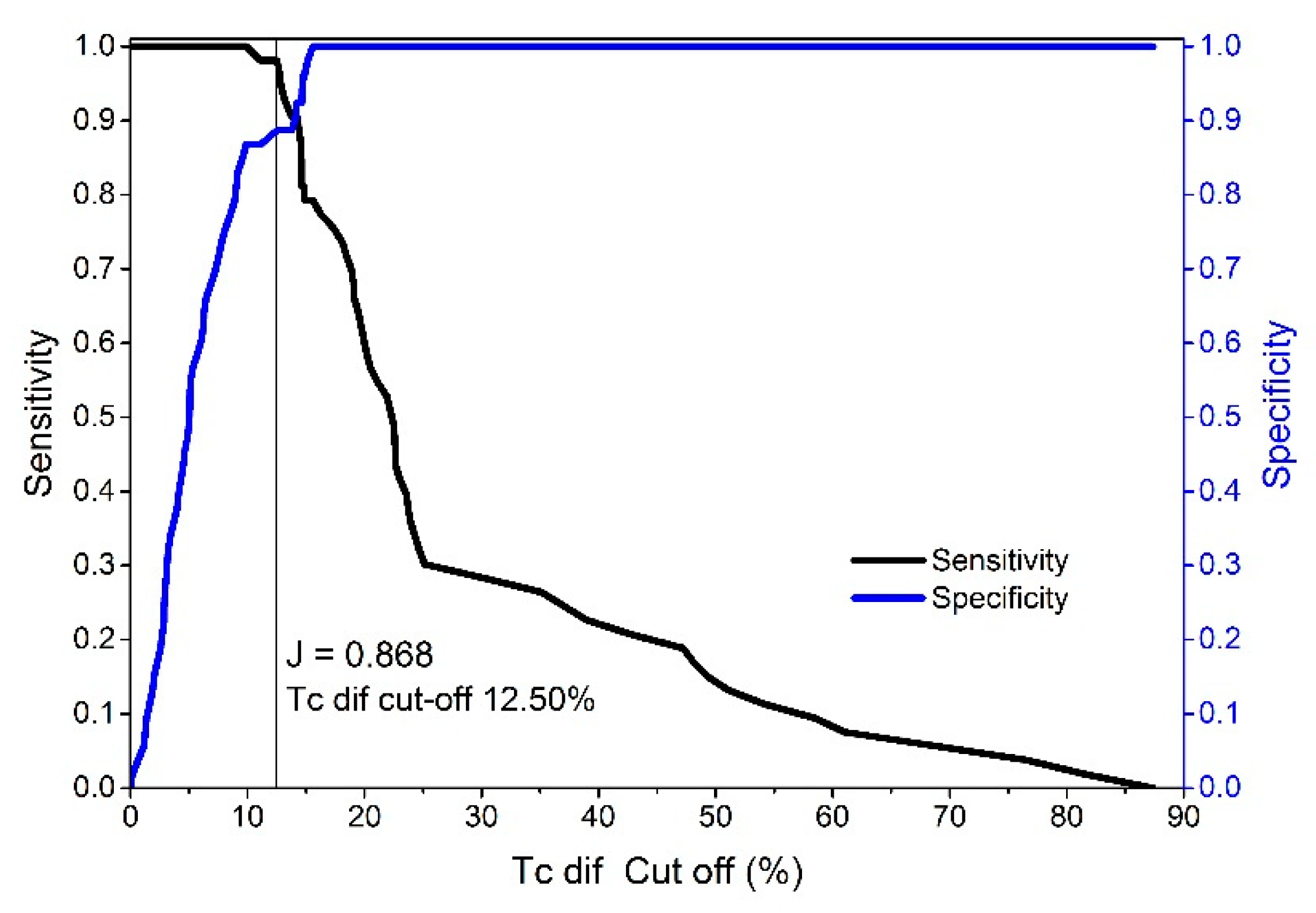
| YI index | 0.455 | 0.818 | 0.455 | 0.290 | 0.903 | 0.484 | 0.340 | 0.868 | 0.453 |
| 95% CI | 0.23–0.59 | 0.64–0.91 | 0.23–0.64 | 0.13–0.39 | 0.74–0.97 | 0.26–0.65 | 0.17–0.45 | 0.75–0.93 | 0.28–0.59 |
| Cut-Off | >25.81% | >9.25% | >7.76% | >17.00% | >9.87% | >5.91% | >17.0% | >9.87% | >5.91% |
| 95% CI | 19.14–25.81 | 6.14–15.36 | 1.51–15.71 | 6.98–37.64 | 7.76–14.63 | 5.52–10.53 | 10.10–28.04 | 8.82–14.18 | 5.52–11.59 |
| Sensitivity | 45.45 | 100.0 | 63.64 | 48.39 | 100.0 | 64.52 | 52.83 | 100.0 | 66.04 |
| Specificity | 100 | 81.82 | 81.82 | 80.65 | 90.32 | 83.87 | 81.13 | 86.79 | 79.25 |
| Females—Injured vs. Non-Injured | Males—Injured vs. Non-Injured | Summarized F + M | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | Dm | Tc | Td | Dm | Tc | Td | Dm | Tc | Td |
| AUPRC | 0.815 | 0.970 | 0.794 | 0.689 | 0.988 | 0.786 | 0.744 | 0.981 | 0.780 |
| F1max | 0.714 | 0.917 | 0.714 | 0.674 | 0.954 | 0.714 | 0.671 | 0.938 | 0.707 |
| Association Criteria | >14.67 | >9.25 | >7.07 | >0.19 | >9.87 | >5.91 | >0.19 | >9.87 | >5.91 |
| PPV | 1.00 | 1.00 | 0.52 | 0.48 | 1.00 | 0.84 | 0.52 | 1.00 | 0.62 |
| TPR | 0.91 | 0.84 | 0.73 | 0.71 | 0.91 | 0.96 | 0.71 | 0.88 | 0.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Đorđević, S.; Rozman, S.; Zupet, P.; Dopsaj, M.; Maffulli, N. Tensiomyography Allows to Discriminate between Injured and Non-Injured Biceps Femoris Muscle. Biology 2022, 11, 746. https://doi.org/10.3390/biology11050746
Đorđević S, Rozman S, Zupet P, Dopsaj M, Maffulli N. Tensiomyography Allows to Discriminate between Injured and Non-Injured Biceps Femoris Muscle. Biology. 2022; 11(5):746. https://doi.org/10.3390/biology11050746
Chicago/Turabian StyleĐorđević, Srđan, Sergej Rozman, Petra Zupet, Milivoj Dopsaj, and Nicola Maffulli. 2022. "Tensiomyography Allows to Discriminate between Injured and Non-Injured Biceps Femoris Muscle" Biology 11, no. 5: 746. https://doi.org/10.3390/biology11050746